
Generation of Multi-Party Dialogues among Embodied
Conversational Agents to Promote Active Living and Healthy Diet for
Subjects Suffering from Type 2 Diabetes
Kuthethur Sneha Jagannath Das
1,2
, Tessa Beinema
2
, Harm op den Akker
2
and Hermie Hermens
1
1
Biomedical Signals and Systems, University of Twente, 7522NB, Enschede, The Netherlands
2
Telemedicine Group, Roessingh Research and Development,7522 AH, Enschede, The Netherlands
Keywords: Virtual Coaching, Embodied Conversational Agents, Behaviour Change, Type 2 Diabetes Mellitus.
Abstract: Diabetes Mellitus is a chronic condition that is highly prevalent in the geriatric population. Self-management
plays a key role in the management of this condition. Leading an active lifestyle and having a healthy meal
are cornerstones in managing this condition. Now with the advancement in Information and Communication
Technology (ICT), continuous and proactive care from the affected individual’s side is possible. A change in
the individual’s behaviour would be beneficial in pursuing physical activity and adopting a healthy diet. This
paper focuses on providing a dialogue based virtual health coaching through multiple Embodied
Conversational Agents (ECAs), using strategies such as Motivational Interviewing (MI), Theories of
Behaviour Change and Behaviour Change Techniques (BCTs). The dialogues are constructed to induce a
behaviour change and promote motivation in the affected subjects to work on improving their physical activity
and diet plan.
1 INTRODUCTION
With the advancement in medicine and technology,
the life span of individuals has increased (Maresca et
al., 2018). In many of the European Union countries,
the ageing index has increased significantly. Statistics
reveal that the average life expectancy would increase
from 72 to 81 years (Silva et al., 2018). In such a
situation, there is a need for explicit geriatric
rehabilitation because the longer life span of the
individual needs to be balanced with a good Quality
of Life (QoL) as well (Maresca et al., 2018; Backman
et al., 2018).
One of the new strategies that have been designed
for geriatric care is telemedicine technology (Maresca
et al., 2018). Telemedicine is based on ICT. The
common forms of telemedicine include
telemonitoring and teleconsultation. These forms of
telemedicine have proven to be beneficial for the
geriatric population (Maresca et al.,2018; Gokalp and
Clarke., 2013).
One of the main challenges faced by the elderly
population is the suffering of a chronic condition.
Some of the commonly prevalent chronic conditions
are diabetes, cardiovascular diseases and chronic
obstructive pulmonary disorder (COPD) (Silva et al,
2018). Using mobile health (m-health), for dealing
with chronic conditions have proven to be beneficial
(Silva et al., 2018). m-health has been useful in the
aspects of personalizing the care provided, engaging
the users and enabling them to manage their own
condition. Some key features of m-health are
nutrition management, planning of exercise,
scheduling an appointment and, tracking of
medicines (Silva et al., 2018; Karageorgos et al,
2018).
Diabetes Mellitus is a chronic condition related
to the deficiency of insulin or resistance to insulin and
high blood glucose levels (Inzucchi and Sherwin,
2011). Type 2 Diabetes Mellitus (T2DM), formerly
known as adult-onset diabetes is characterized by the
ineffective use of insulin (Inzucchi and Sherwin,
2011). People suffering from T2DM, are at risk of
developing cardiovascular conditions, stroke,
blindness, gangrene in the foot which could lead to
foot amputation and kidney failure to name a few
(Pardhan et al., 2018; Backholer et al., 2012).
Physical activity (PA) and a healthy diet have proven
to be beneficial in the management of T2DM
(Inzucchi and Sherwin,2011; Di Loreto et al., 2003).
Das, K., Beinema, T., Akker, H. and Hermens, H.
Generation of Multi-Party Dialogues among Embodied Conversational Agents to Promote Active Living and Healthy Diet for Subjects Suffering from Type 2 Diabetes.
DOI: 10.5220/0007750602970304
In Proceedings of the 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2019), pages 297-304
ISBN: 978-989-758-368-1
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
297

The treatment of diabetes can be enhanced through
self-management by the affected individual. This can
be achieved through monitoring and education (Sina
et al., 2018).
Health coaching provided to the affected
individuals could aid in the self-management (Gupta
et al., 2018). In this type of coaching, poor health
habits are targeted and worked upon by setting
adaptable and personalized goals, monitoring
progress, providing encouraging feedback and
suggestions for further improvement. Health
coaching aims to bring about a behaviour change in
the individual (Snaith et al., 2018). With the
advancements in the digital healthcare, the health
coaching can be provided virtually through the form
of virtual coaches. These virtual coaches could be the
ECAs. ECAs can be seen as a part of a system that
conveys messages to humans through facial
expressions, hand gestures and voice (Shaked, 2017).
In this paper, the focus lies on developing
dialogues for a panel of ECAs and a human user,
where the human user is suffering from T2DM. The
dialogues aim to provide education and awareness
about T2DM and, motivate the users to adopt PA and
a healthy diet. The dialogues are constructed using the
theories of behaviour change and behaviour change
techniques (BCT).
2 BACKGROUND
In the management of diabetes, Web of Things (WoT)
is being applied. Websites provide information,
problem-solving aids, social support and awareness.
Higher end versions in WoT enable tailored feedback,
self-monitoring of the condition and self-care in
terms of medication, exercise and diet (Al-Taee et al.,
2013). These developments are being made by using
the principle of behaviour change (Al-Taee et al.,
2013). Studies reveal that people suffering from
chronic conditions have to go through behaviour
changes in order to cope with the condition (Aujoulat
et al., 2007). WoT and ICT based systems are being
developed that take into account the feedback
provided to the affected individual. Reminders in the
form of text messages to take medications on time,
electronic diary entries for tracking the diet and
exercise pursued, education and tips to manage the
condition and goals set are sent to the users (Nieto-
Chaupis et al., 2017; Fioravanti et al., 2011).
Digital technology has enabled the creation of
context-aware technology. These technologies
contribute to virtual coaching from the confines of a
home setting (Albaina et al., 2009). Many virtual
coaching systems aid in the pursuit of PA. One such
system is Flowie which has been developed using the
strategies of goal setting, self-monitoring and
intrinsic motivation to make the elderly people walk
more (Albaina et al., 2009).
Virtual coaching using ECAs is being explored
for the purpose of telehealth and behaviour change
(Lisetti et al., 2011). MI is being used to create health
behaviour change interventions. MI is a client-
oriented counselling approach whose main goal is to
resolve discrepancies between the current behaviour
of the patients and their set goals (Lisetti et al., 2011).
Emp-ODVIHC has developed an ECA based
virtual coaching system based on MI. It includes
strategies such as feedback (Amini et al., 2013).
`Most of the times ECAs have a human-like
appearance with the ability to process natural
language and non-verbal communication. ECAs are
being tried to be integrated into a medical platform
(Ravenet et al., 2018). The ECAs being
anthropomorphic in nature has proven to be
beneficial in inducing motivation based on self-
efficacy, interest and attitude (Baylor, 2009).
Adoption of ECAs have been explored in the health
domain for children with autism and for adults with
cognitive impairments (Tanaka et al., 2017; Wargnier
et al., 2015).
Providing telemedicine-based services in terms of
self-monitoring and education has proven to be
beneficial in improving the individual’s diet intake
and PA (van Doorn-van Atten et al., 2018).
3 METHODS
The focus of this paper lies in creating dialogues
among the panel of ECAs and a subject with the
chronic condition of T2DM. The dialogues need to be
able to motivate the subject to adopt healthy
behaviour changes in terms of PA and diet since these
are the cornerstones in the self-management of
T2DM.
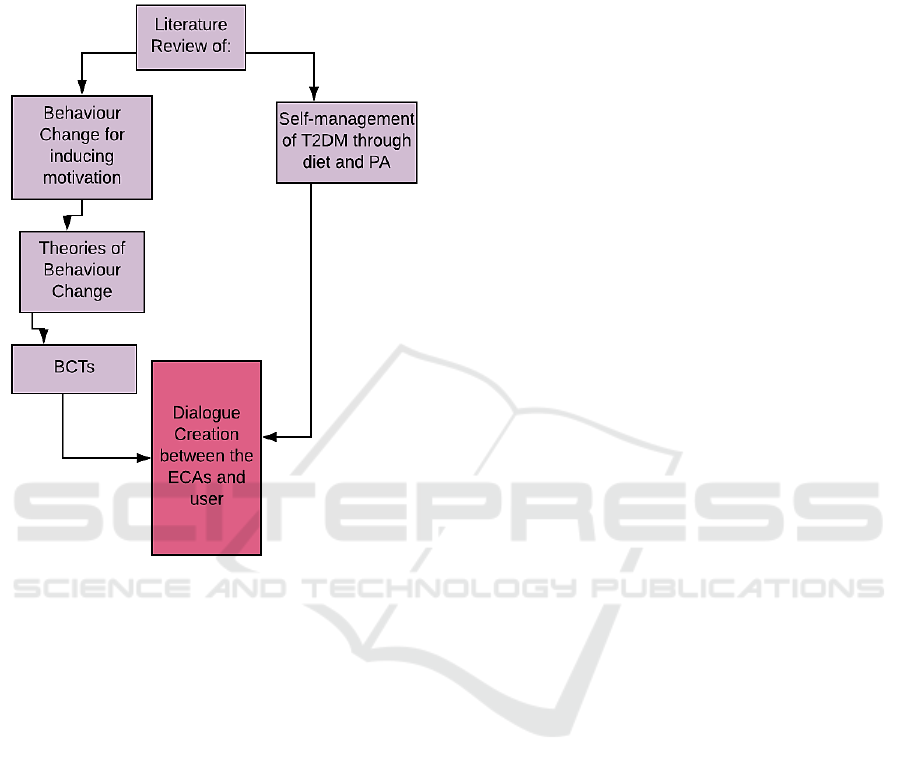
Since behaviour change is the key factor here, it
was decided that the dialogues would be written
based on the theories of behaviour change and BCTs.
Hence a thorough literature review as shown in
Figure 1, was implemented using keywords such as
motivation, behaviour change, intrinsic motivation,
goal setting in health care, virtual coaching, self-
management of T2DM, avatar-based coaching, health
coaching and PA monitoring to name a few.
At the end of the literature review, the theories of
behaviour change that could be used in the dialogue
creation and relevant BCTs were chosen. Along with
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
298
this, the types of exercise that could be performed and
the components of a healthy diet that would be
beneficial for people with T2DM were found out.
Based on these points the dialogues were created.
Figure 1: Method adopted in dialogue generation.
4 RESULTS
From the Methodology adopted, there are four main
results obtained and they are discussed in this section.
4.1 Theories of Behaviour Change
At the end of the literature review of psychological
theories related to behaviour change, the five theories
discussed below were chosen to write the dialogues
for the self-management of T2DM.
4.1.1 Goal Setting Theory
This theory focuses on the transition from the set
goals to the actual performance. Two core factors are
involved in this theory: difficulty and specificity of
the set goals. Moderators on the effect of the goals are
self-efficacy, feedback and commitment (Locke and
Latham, 2002). Goals need to be realistically set and
followed up. In T2DM management, we focus on the
pursuit of PA and a healthy diet. Hence, dialogues are
needed that would focus on helping the user to set
achievable goals that would have a positive effect on
their T2DM control.
4.1.2 Social Cognitive Theory
This theory focuses on human behaviour that is
motivated and regulated through self-regulation.
According to the theory, self-regulation occurs
through three sub-processes: self-monitoring, self-
judgement and self-reaction (Bandura, 1991). The
concept of self-efficacy is introduced through this
theory. In keeping T2DM under control, self-
management plays a crucial role. Monitoring the
insulin and glucose levels and keeping track of the
food intake and the levels of PA is needed for T2DM
management. Hence, dialogues that focus on
improving the user’s self-regulation and self-efficacy
are needed.
4.1.3 Protection Motivation Theory
This health psychology theory was developed as a
framework to understand the impact of fear appeals
on an individual. This theory is governed by two
processes: 1. Threat appraisal 2. Coping appraisal.
The cognitive predictors of this framework include
severity, vulnerability, response efficacy which is
based on the recommendations given and self-
efficacy (Rogers, 1983). In the case of T2DM,
through the threat appraisal and coping appraisal, a
self- protection behaviour can be induced in the
subject. For instance, if the user comes to know about,
developing cardiovascular issues due to poor
management of T2DM, out of fear and the need to
protect himself from incurring the issue, he would be
willing to let go of the sedentary lifestyle and quit
eating junk food. The dialogues can be created based
on this theory.
4.1.4 Information-Motivation Behavioural
Skills Model
This model is developed based on three factors. They
are the availability of information and knowledge in
the particular health topic, motivation to change
behaviour and the availability of behavioural skills to
do the specific acts required to tackle the health
condition (Fisher and Fisher, 1992). According to this
model, information and motivation influence each
other. In the case of T2DM, if the subject has the
knowledge that he needs to adopt more PA to manage
the condition, he would be motivated to take the stairs
instead of an elevator. Similarly, if he is motivated to
Generation of Multi-Party Dialogues among Embodied Conversational Agents to Promote Active Living and Healthy Diet for Subjects
Suffering from Type 2 Diabetes
299

manage T2DM, he would take the effort to gather
information about the same. For instance, he would
consult a nutritionist about a healthy diet plan.
4.1.5 Health Belief Model
This model tries to predict and explain when an
individual would adopt actions pertaining to his
health. According to this model, an individual would
be ready to adopt healthy behaviours if he
understands the susceptibility and severity of the
health condition and would adopt the changes when
the cues to action are provided (Janz and Becker,
1984). This model can be incorporated in the
dialogues. For instance, if the subject is made to
understand that eating too many sweets can worsen
T2DM and hence the person is more likely to develop
gangrene in the foot, he would understand that he is
susceptible to it and the severity of the condition as
well. Cues such as reminders by the virtual coaches
that sweets shouldn’t be eaten often can be provided.
4.2 Behaviour Change Techniques
Based on the theories selected in the previous section
and taking into account that the subjects need to adopt
a change in behaviour in terms of an active lifestyle
and diet, from the latest BCT taxonomy, the relevant
BCTs were chosen (Hankonen et al., 2014; Michie et
al., 2013).
The BCTs chosen belong to the cluster of goals
and planning, feedback and monitoring, social
support, shaping knowledge, natural consequences,
repetition and substitution and self-belief (Michie et
al., 2013).
For instance, BCTs belonging to the cluster of
goals and planning can be used in the improvement of
PA. This could be in terms of achieving a required
step count. The feedback and monitoring cluster
would help the individual to follow up his set goals
and his physiological parameters such as the glucose
level. Similarly, through the BCT clusters of shaping
knowledge and natural consequence, awareness
would be created in the subject about T2DM
management and keep the subject informed about the
negative conditions that could occur if T2DM is not
under control. BCTs of repetition and substitution
cluster is useful in the formation of healthy habits
such as cycling to the grocery store instead of using
the car. These kinds of suggestions can be given via
the virtual coaches through the dialogues. By using
the BCTs from self-belief, the subject can be given
the confidence that he could achieve the set goals. For
instance, by reflecting on the subject’s past success of
achieving good PA levels, the subject can be inspired
to achieve higher levels of PA.
4.3 Physical Activity and Diet in T2DM
Literature review on the role of PA and diet in T2DM
management revealed the type of exercises and
components of a healthy diet that could be adopted by
the subject. With regards to the PA, four groups of
exercises were considered to be optimal for T2DM
management. The groups are endurance, passive,
resistance and aerobic types of exercise. These
exercises can alter the body metabolism associated
with T2DM by improving insulin sensitivity, blood
glucose level and glycemic control. This is especially
the case with resistance and aerobic type of exercises.
Hence activities such as walking, running,
swimming, cycling, rowing, skipping and exercises
performed against resistance such as weight lifting
are recommended for subjects with T2DM (Thent et
al., 2013).
With regards to the diet, it was found that the diet
adopted has an explicit effect on obesity and glucose
level regulation. Hence it is highly imperative that a
person with T2DM avoids food with excessive sugar
content, oil and the intake of alcohol as well. Meals
with low-calorie content are recommended for people
with T2DM since it can prevent further progression
of the condition because of insulin sensitivity
improvement and reduction in weight. The ideal meal
should have a balance between the contents of
carbohydrates and high fibre (Lagerros and Rössner,
2013).
4.4 The Dialogues
The results of section 4.1, 4.2 and 4.3 are combined
to generate the dialogues. The below dialogue set is a
result of this combination. Three ECAs have been
chosen for the virtual coaching panel. These coaches
focus on motivating the user to adopt PA and a
healthy diet. A brief persona description of the
coaches and the user is discussed in the following
paragraph (Le Rouge et al, 2013).
Bob: Exercise trainer (Male- 38 years)
Kim: Nutritionist (Female- 30 years)
Emma: Volunteer (Female- 57 years)
Dora: Subject (Female-55 years)
Six months ago, the subject Dora was diagnosed
with T2DM and she is not happy with the way her
condition is progressing. Hence, she has scheduled
her first meeting to meet this virtual team of coaches.
The coaches are Bob whose expertise lies in fitness
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
300

training through exercises, for elderly people since
the last 10 years and Kim who has a Master’s degree
in nutrition sciences and specializes in coming up
with a healthy diet plan for people with T2DM and
cardiovascular conditions. In the panel, Emma a
volunteer who has been suffering from T2DM but is
successfully coping with it for the last 3 years is also
present.
Bob and Kim are amiable kinds of personalities.
Bob says his suggestions right away and is more
authoritative whereas Kim likes to understand her
subject and then give the required suggestions in a
milder manner. Emma is a part of the panel since she
feels that she would be able to relate to the subject’s
worries because she herself has gone through it in the
past and by sharing her experiences she wants to
boost the confidence of the subject. Dora has been
recently diagnosed with T2DM and she is worried
about her condition and wants to take the necessary
steps to control it but she is confused about how to
proceed with it. Hence, she has come to meet the
coaches.
Below is a brief illustration of the dialogues that
could take place between the panel and the user.
Dora: Hello. For the last 6 months, I have been
suffering from Diabetes and with the medicines
prescribed, I tried to take care of the condition. But I
guess it is not working.
Bob: Hello! Don’t worry. A lot of people who have
come to us have been in the same state as you and are
now doing much better. Isn’t it so, Kim?
Kim: Yes. Of course Bob!
Emma: Yes Dora. Even, I faced a similar situation
around 3 years back and with a good exercise and diet
plan, I am able to manage the condition really well.
(BCT: Social Support(unspecified), Information
about Health Consequences)
Dora: Okay. This sounds promising. From where
should I start?
Bob: Dora, to keep Diabetes under check, you need
to follow both a good exercise plan and diet. Only
then would your insulin and glucose levels be under
control. (BCT: Goal Setting(outcome), Goal
Setting (Behaviour), Problem Solving,
Information about Health Consequences)
Emma: Bob is right. Could you tell us a little bit
about your comfort with performing exercises?
Dora: I am not a very athletic person nor do I go to
the gym. Once a while I go for walks but most of the
time, I drive around.
Bob: Hmm. Okay. Maybe you could start with a
45minutes to 1-hour walk every morning. You can
follow this time period for 10 days and then gradually
increase the duration by about half an hour or so.
(BCT- Action planning, Graded Tasks, Habit
Formation, Instruction on how to perform a
Behaviour, Goal Setting (Behaviour))
Emma: You need to focus on your PA levels. If it is
not up to the mark, then you would land up in a
problem. I have been through that phase! (BCT:
Information about Health Consequences,
Information about Antecedents)
Bob: Regarding your diet, the first step is to
completely cut down on junk food. This means that
you should cut down on sugary and oily foods. Work
on this for the next three weeks starting from today.
(BCT: Goal setting (Behaviour), Habit Reversal)
Kim: Yes. We can see how this goes.
Dora: okay. I am not very confident about this but I
will try my best to stick to this plan.
Kim: I think you can do it! Find a friend who would
be your teammate in this for a few days. (BCT: Social
Support (unspecified)
Emma: Yes! I think you will be fine as well. I would
also suggest that you use a diary to write down about
all this on a daily basis. It has helped me to stay
motivated and get things back on track. (BCT-Self-
monitoring (behaviour), Self -monitoring
(outcome), Information about Antecedents)
Dora: Okay. Would you also suggest that I weigh my
weight every week and check for the sugar level?
Kim: Yes. That’s a good idea and it will help in
getting a thorough feedback. (BCT-Bio-feedback,
focus on past success, self-monitoring, feedback
from others, Information about Antecedents)
Dora: Okay. See you!
Kim: Good luck!
Dialogues based on the BCTs such as Goal
Setting(outcome) and Goal Setting (behaviour)
follow from the Goal Setting Theory (Locke and
Latham, 2002). Dialogues that use the BCTs
belonging to the self-monitoring cluster are derived
from the Social Cognitive theory which focuses on
self-efficacy (Bandura, 1991). Overall, the
information provided to the user in the dialogue is
based on the Protection Motivation Theory,
Information- Motivation Behavioural Skills Model
and Health Belief Model. The dialogues provide
information about how the PA should be pursued and
the nature of diet and also focus on what could go
wrong with the subject’s health if the behaviour is not
followed (Rogers,1983; Fisher and Fisher, 1992; Janz
and Becker, 1984). The coaching strategies
incorporated through these dialogues are MI,
Motivational Enhancement Therapy (ME) and
diabetes specific coaching (Lisetti et al., 2011; Miller,
1995; Sherifali, 2017).
Generation of Multi-Party Dialogues among Embodied Conversational Agents to Promote Active Living and Healthy Diet for Subjects
Suffering from Type 2 Diabetes
301

5 DISCUSSION
A dialogue set between a panel of ECAs and a subject
with T2DM has been created for the purpose of
virtual coaching. The dialogues are created using the
psychological theories of behaviour change and
BCTs. Predominantly in the dialogue set, the
coaching strategies of MI and ME along with diabetes
specific management is adopted.
MI and ME are useful in trying to induce an
intrinsic motivation in the subject (Lisetti et al., 2011;
Miller, 1995). Theories and BCTs on which the
dialogues are constructed have been adopted in
coaching systems related to the pursuit of PA and
healthy diet (Hankonen et al., 2014). Goal Setting
Theory, Social Cognitive Theory and Information
Motivation Behavioural Skills model are used
commonly in health psychology and are known for
inducing intrinsic motivation (Van Doorn-van Atten
et al., 2018; Locke and Latham, 2002; Fisher and
Fisher, 1992; Miller, 1995). Goal setting is a very
integral part of health coaching in order to induce a
behaviour change (Snaith et al, 2018). The goals set
need to be understood and agreed upon by the subject
and through the dialogues, the concept of
commitment in pursuing the set goal is being aimed
for (Snaith et al., 2018).
The BCTs chosen focus on inducing an intrinsic
motivation since this type of motivation would help
the subject on a long- term basis (Seifert et al., 2012).
This is the reason why the BCTs are chosen from the
clusters mention in Section 4.2 and BCTs belonging
to the cluster such as rewards have not been included
(Michie et al., 2013). BCTs such as satiation or
exposure is not used in this dialogue set because of
the possibility that it would lead to poor management
of T2DM. For instance, in satiation, the subject could
be asked to eat a lot of chocolates in order to let go of
the habit of eating sugary stuff but it might not go well
with T2DM management (Michie et al., 2013). The
BCTs focus on creating awareness about T2DM and
its self-management. It tries to motivate the subject
by giving her the confidence that she can do it.
In the coaching panel, three ECAs are present who
have expertise in T2DM management. According to
the literature, a positive effect in health coaching is
possible through a multi-virtual coach system
(Kantharaju et al., 2018; op den Akker et al., 2018).
Persuasiveness from the coach’s side also adds more
value to the health coaching. Studies indicate that a
coach with an authoritative personality can be more
successful in inducing a behaviour change (Prochaska
et al., 1994). Hence, Bob’s character is shown to be
authoritative. Cross-gender interaction has also been
recommended in this type of coaching (Kantharaju et
al., 2018).
As a part of the future work, a user evaluation
needs to be conducted to test the competency of the
dialogues delivered by this multi-party ECAs. The
persuasiveness of the dialogues and whether the users
would be intrinsically motivated to adopt an active
living and a healthy diet needs to be evaluated.
Parameters such as how quickly the changes can be
seen, that is whether and when they would move to
the action phase in the five stages of change model
needs to be looked into (Prochaska et al., 1994). For
the virtual coaching to have maximal efficiency, the
ECAs which comprise the heart of the coaching
system need to be fully aware and updated with the
overall health and behaviour of the subject (op den
Akker et al., 2018). For instance, if Dora is attending
the second session with the panel and if there is an
improvement in PA, then the coach needs to be
automatically able to say it during the session. This
could be implemented for instance through a Heart
Rate (HR) sensor worn by Dora, where the HR values
are indicated in prior to the system of coaches. This
way, the system can be tailored and adapted in
specific to each user. Similarly, to improve the
adaptability and smartness of the system, the coaches
need to be able to predict the stage of change of the
user, this could be done through a short questionnaire
that could be filled by the user before the session
starts and based on the questionnaire results, the
ECAs can provide a tailored coaching to the user.
In conclusion, a dialogue set was created between
a set of virtual coaches and a geriatric subject
suffering from T2DM using the theories of behaviour
change, BCTs and coaching strategies such as MI and
ME in order to make the subject adopt better lifestyle
changes in terms of PA and diet.
REFERENCES
Al-Taee, M. A., Sungoor, A. H., Abood, S. N. and Philip,
N. Y., 2013, December. Web-of-Things inspired e-
Health platform for integrated diabetes care
management. In Applied Electrical Engineering and
Computing Technologies (AEECT), 2013 IEEE Jordan
Conference on (pp. 1-6). IEEE.
Albaina, I. M., Visser, T., Van Der Mast, C. A. and
Vastenburg, M. H., 2009, April. Flowie: A persuasive
virtual coach to motivate elderly individuals to walk. In
Pervasive Computing Technologies for Healthcare,
2009. PervasiveHealth 2009. 3rd International
Conference on (pp. 1-7). IEEE.
Amini, R., Lisetti, C., Yasavur, U. and Rishe, N., 2013,
September. On-demand virtual health counselor for
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
302

delivering behavior-change health interventions.
In Healthcare Informatics (ICHI), 2013 IEEE
International Conference on (pp. 46-55). IEEE.
Aujoulat, I., d’Hoore, W. and Deccache, A., 2007. Patient
empowerment in theory and practice: polysemy or
cacophony?. Patient education and counseling, 66(1),
pp.13-20.
Backholer, K., Chen, L. and Shaw, J., 2012. Screening for
diabetes. Pathology, 44(2), pp.110-114.
Backman, C., Harley, A., Peyton, L., Kuziemsky, C.,
Mercer, J., Monahan, M. A., Schmidt, S., Singh, H. and
Gravelle, D., 2018. Development of a Path to Home
Mobile App for the Geriatric Rehabilitation Program at
Bruyère Continuing Care: Protocol for User-Centered
Design and Feasibility Testing Studies. JMIR research
protocols, 7(9).
Bandura, A., 1991. Social cognitive theory of self-regulation.
Organizational behavior and human decision processes,
50(2), pp.248-287.
Baylor, A. L., 2009. Promoting motivation with virtual
agents and avatars: role of visual presence and
appearance. Philosophical Transactions of the Royal
Society B: Biological Sciences, 364(1535), pp.3559-
3565.
Di Loreto, C., Fanelli, C., Lucidi, P., Murdolo, G., De
Cicco, A., Parlanti, N., Santeusanio, F., Brunetti, P. and
De Feo, P., 2003. Validation of a counseling strategy to
promote the adoption and the maintenance of physical
activity by type 2 diabetic subjects. Diabetes care,
26(2), pp.404-408.
Fioravanti, A., Fico, G., Arredondo, M. T. and Leuteritz, J.
P., 2011, August. A mobile feedback system for
integrated E-health platforms to improve self-care and
compliance of diabetes mellitus patients. In 2011
Annual International Conference of the IEEE
Engineering in Medicine and Biology Society (pp.
3550-3553). IEEE.
Fisher, J. D. and Fisher, W. A., 1992. Changing AIDS-risk
behavior. Psychological bulletin, 111(3), p.455.
Gokalp, H. and Clarke, M., 2013. Monitoring activities of
daily living of the elderly and the potential for its use in
telecare and telehealth: a review. TELEMEDICINE and
e-HEALTH, 19(12), pp.910-923.
Gupta, I., Di Eugenio, B., Ziebart, B., Liu, B., Gerber, B.,
Sharp, L., Davis, R. and Baiju, A., 2018, June. Towards
Building a Virtual Assistant Health Coach. In 2018
IEEE International Conference on Healthcare
Informatics (ICHI) (pp. 419-421). IEEE.
Hankonen, N., Sutton, S., Prevost, A. T., Simmons, R. K.,
Griffin, S. J., Kinmonth, A. L. and Hardeman, W.,
2014. Which behavior change techniques are associated
with changes in physical activity, diet and body mass
index in people with recently diagnosed diabetes?.
Annals of Behavioral Medicine, 49(1), pp.7-17.
Inzucchi, S. E. and Sherwin, R. S., 2011. Type 2 diabetes
mellitus. Cecil Medicine. 24th ed. Philadelphia, Pa:
Saunders Elsevier.
Janz, N. K. and Becker, M. H., 1984. The health belief model:
A decade later. Health education quarterly, 11(1), pp.1-
47.
Kantharaju, R. B., De Franco, D., Pease, A. and Pelachaud,
C., 2018, November. Is Two Better than One?: Effects
of Multiple Agents on User Persuasion. In Proceedings
of the 18th International Conference on Intelligent
Virtual Agents (pp. 255-262). ACM.
Karageorgos, G., Andreadis, I., Psychas, K., Mourkousis,
G., Kiourti, A., Lazzi, G. and Nikita, K. S., 2018. The
Promise of Mobile Technologies for the Health Care
System in the Developing World: A Systematic
Review. IEEE reviews in biomedical engineering.
Lagerros, Y. T. and Rössner, S., 2013. Obesity management:
what brings success?. Therapeutic advances in
gastroenterology, 6(1), pp.77-88.
LeRouge, C., Ma, J., Sneha, S. and Tolle, K., 2013. User
profiles and personas in the design and development of
consumer health technologies. International journal of
medical informatics, 82(11), pp.e251-e268.
Lisetti, C.L., Yasavur, U., Visser, U. and Rishe, N., 2011,
May. Toward conducting motivational interviewing
with an on-demand clinician avatar for tailored health
behavior change interventions. In Pervasive Computing
Technologies for Healthcare (PervasiveHealth), 2011
5th International Conference on (pp. 246-249). IEEE.
Locke, E. A. and Latham, G. P., 2002. Building a practically
useful theory of goal setting and task motivation: A 35-
year odyssey. American psychologist, 57(9), p.705.
Maresca, G., De Cola, M. C., Caliri, S., De Luca, R.,
Manuli, A., Scarcella, I., Silvestri, G., Bramanti, P.,
Torrisi, M., Calabrò, R. S. and Bramanti, A., 2018.
Moving towards novel multidisciplinary approaches for
improving elderly quality of life: The emerging role of
telemedicine in Sicily. Journal of telemedicine and
telecare, p.1357633X17753057.
Michie, S., Richardson, M., Johnston, M., Abraham, C.,
Francis, J., Hardeman, W., Eccles, M. P., Cane, J. and
Wood, C. E., 2013. The behavior change technique
taxonomy (v1) of 93 hierarchically clustered
techniques: building an international consensus for the
reporting of behavior change interventions. Annals of
behavioral medicine, 46(1), pp.81-95.
Miller, W. R., 1995. Motivational enhancement therapy
manual: A clinical research guide for therapists
treating individuals with alcohol abuse and
dependence. DIANE Publishing.
Nieto-Chaupis, H., Matta-Sólis, H., Asencios, B. B., Perez-
Siguas, R., Talledo, R. A., Moreno, T. E. and Sifuentes,
V. N., 2017, October. Proposal of a telecare system for
monitoring glucose anomalous behavior in type-2
diabetes patients. In Electrical, Electronics
Engineering, Information and Communication
Technologies (CHILECON), 2017 CHILEAN
Conference on (pp. 1-6). IEEE.
op den Akker, H., op den Akker, R., Beinema, T., Baños,
O., Heylen, D., Bedsted, B., Pease, A., Pelachaud, C.,
Salcedo, V. T., Kyriazakos, S. A. and Hermens, H.,
2018, March. Council of Coaches-A Novel Holistic
Behavior Change Coaching Approach. In ICT4AWE
(pp. 219-226).
Pardhan, S., Nakafero, G., Raman, R. and Sapkota, R.,
2018. Barriers to diabetes awareness and self-help are
Generation of Multi-Party Dialogues among Embodied Conversational Agents to Promote Active Living and Healthy Diet for Subjects
Suffering from Type 2 Diabetes
303

influenced by people's demographics: perspectives of
South Asians with type 2 diabetes. Ethnicity & health,
pp.1-19.
Prochaska, J. O., Velicer, W. F., Rossi, J. S., Goldstein, M.
G., Marcus, B. H., Rakowski, W., Fiore, C., Harlow, L.
L., Redding, C. A., Rosenbloom, D. and Rossi, S. R.,
1994. Stages of change and decisional balance for 12
problem behaviors. Health psychology, 13(1), p.39.
Ravenet, B., Pelachaud, C., Clavel, C. and Marsella, S.,
2018. Automating the production of communicative
gestures in embodied characters. Frontiers in
psychology, 9.
Rogers, R. W., 1983. Cognitive and psychological processes
in fear appeals and attitude change: A revised theory of
protection motivation. Social psychophysiology: A
sourcebook, pp.153-176.
Seifert, C. M., Chapman, L. S., Hart, J. K. and Perez, P.,
2012. Enhancing intrinsic motivation in health
promotion and wellness. American Journal of Health
Promotion, 26(3), pp.1-12.
Shaked, N. A., 2017. Avatars and virtual agents–relationship
interfaces for the elderly. Healthcare technology letters,
4(3), pp.83-87.
Sherifali, D. (2017). Diabetes coaching for individuals with
type 2 diabetes: A state-of-the-science review and
rationale for a coaching model. Journal of Diabetes,
9(6), 547-554.
Sina, M., Graffy, J. and Simmons, D., 2018. Associations
between barriers to self-care and diabetes complications
among patients with type 2 diabetes. Diabetes research
and clinical practice, 141, pp.126-131.
Silva, S., Felgueiras, R. and Oliveira, I. C., 2018. Geriatric
Helper: An mHealth Application to Support
Comprehensive Geriatric Assessment. Sensors (Basel,
Switzerland), 18(4).
Snaith, M., De Franco, D., Beinema, T., Op Den Akker, H.
And Pease, A., 2018. A dialogue game for multi-party
goal-setting in health coaching. In Proceedings of the
Seventh International Conference on Computational
Models of Argument (COMMA 2018), IOS Press,
accepted for publication.
Tanaka, H., Negoro, H., Iwasaka, H. and Nakamura, S.,
2017. Embodied conversational agents for multimodal
automated social skills training in people with autism
spectrum disorders. PloS one, 12(8), p.e0182151.
Thent, Z. C., Das, S. and Henry, L. J., 2013. Role of
exercise in the management of diabetes mellitus: the
global scenario. PloS one, 8(11), p.e80436.
van Doorn-van Atten, M., de Groot, L., de Vries, J. and
Haveman-Nies, A., 2018. Determinants of Behaviour
Change in a Multi-Component Telemonitoring
Intervention for Community-Dwelling Older Adults.
Nutrients, 10(8), p.1062.
Wargnier, P., Malaisé, A., Jacquemot, J., Benveniste, S.,
Jouvelot, P., Pino, M. and Rigaud, A. S., 2015, March.
Towards attention monitoring of older adults with
cognitive impairment during interaction with an
embodied conversational agent. In Virtual and
Augmented Assistive Technology (VAAT), 2015 3rd
IEEE VR International Workshop on (pp. 23-28). IEEE.
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
304
