
Empathize with the CAPTAIN Stakeholders’ Community towards
Understanding Older Adults’ Daily Needs and How They Cope with
Them
Despoina Petsani
1
, Evdokimos I. Konstantinidis
1,2 a
, Antonis Billis
1b
, Maria Nikolaidou
1c
,
Nikolaos Kiriakidis
1
, Vassiliki Zilidou
1d
, Despoina Mantziari
1
, Michalis Timoleon
1
and Panagiotis D. Bamidis
1e
1
Lab of Medical Physics, Medical School, Aristotle University of Thessaloniki, Thessaloniki, Greece
2
Nively Sas, Nice, France
vickyzilidou@gmail.com, mantziad@gmail.com, mtimoleon@auth.gr, bamidis@med.auth.gr
Keywords: Older Adults, Active and Health Ageing, Smart Homes, Design Thinking.
Abstract: This paper presents the results of the first part of the design thinking approach that was utilized within the
CAPTAIN H2020 funded project. CAPTAIN aims at developing a new technology to help older adults living
at home, by designing new technology that turns the home of older adults into a ubiquitous assistant. Six
personas were selected for the empathize session which was conducted through plenary face–to-face open
discussion meeting. 33 older adults and caregivers participated. The goal of this study was to identify the
everyday difficulties that older adults face and clarify the means they are currently using to address these
problems. The paper presents the approach, the design of the first session and the results from the Greek pilot
site.
1 INTRODUCTION
According to a Center for Disease Control study by
the State of Aging and Health in America (Centers for
Disease Control and Prevention, 2013), 64% of
surveyed American older adults want to live in their
own homes. These figures are consistent with the
preferences of the European population. However,
they often need to be institutionalized due to age-
related problems. This might have negative impact on
different aspects of person’s life such as depression,
lower quality of life, social isolation and has also been
linked with high mortality rates (Yang and Ornstein,
2015).
The use of technology has demonstrated
compelling evidence as a means of supporting aging
at home (Reeder et al., 2013). A wide range of
technologies for homecare scenarios for older adults
have been developed including but not limited to
a
https://orcid.org/0000-0002-5522-9553
b
https://orcid.org/0000-0002-1854-7560
c
https://orcid.org/0000-0003-1307-3252
d
https://orcid.org/0000-0002-4859-6996
e
https://orcid.org/0000-0002-9936-5805
enhancing self-management of chronic conditions
(García-Lizana and Sarría-Santamera, 2007),
objective frailty assessment (Schwenk et al., 2015),
fall detection and prevention (Chaudhuri, Thompson
and Demiris, 2014) and assistance in overcoming
social isolation (Chen and Schulz, 2016).
In this context, the H2020 funded project,
CAPTAIN (Coach Assistant via Projected and
Tangible Interface, [www.captain-eu.org]), aims at
developing a new technology to help older adults
living at home. CAPTAIN will develop a new
technology designed to turn the home of older adults
into a ubiquitous assistant. The produced system
makes use of projected augmented reality and real-
time 3D sensing technologies to monitor and
“comprehend” the user and the indoor space in order
to provide contextualized and personalized coaching
and instructions. Solutions will be designed for non-
invasive user and environmental sensing including
Petsani, D., Konstantinidis, E., Billis, A., Nikolaidou, M., Kiriakidis, N., Zilidou, V., Mantziari, D., Timoleon, M. and Bamidis, P.
Empathize with the CAPTAIN Stakeholders’ Community towards Understanding Older Adults’ Daily Needs and How They Cope with Them.
DOI: 10.5220/0007766303110318
In Proceedings of the 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2019), pages 311-318
ISBN: 978-989-758-368-1
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
311

emotional and behavioral recognition, indoor location
and gait analysis, physical and cognitive training
progress monitoring. Exploiting this information,
CAPTAIN will develop behaviour and AI algorithms
which will allow the system to provide personalised
advice, guidance and follow-up for key age-related
issues in daily life which impact the person's ability
to remain active and independent at their home. This
will include risk avoidance, nutrition guidance,
physical activity and cognitive training follow-up,
guidance for lifestyle and social participation. One of
the research question CAPTAIN is expected to
answer is how effectively can machine learning
techniques predict older adult’s profile and provide
behavioral guidance.
CAPTAIN has to deal also with the system’s
usability and acceptability. To this end, CAPTAIN
consortium has built an engagement and
dissemination plan in order to create a community of
stakeholders with strong support bonds to stay active
throughout the whole project. The so called
CAPTAIN community is the only official source of
requirements. While the multidisciplinary team of
CAPTAIN will suggest requirements, it will be up to
the active stakeholders’ network to decide their
adoption or not. The question raised is how to build
and maintain a network of stakeholders while gather
information that will assist on enhancing system’s
usability and acceptability.
CAPTAIN has adopted a fully user-centered,
participatory design approach based on agile
principles for technology development. Throughout
the project a combination of Design Thinking, Lean
Startup and Agile methods is applied. Design
Thinking (Plattner, Meinel and Leifer, 2011)is a
highly approved method for exploring the so called
wicked problems, which are complex problems not
adequately defined. Designers using the Design
Thinking method are also willing to redefine the
problem and investigate the frame that guides to the
solution. The Lean Startup method (Ries,
2011)allows the design team to rapidly define and
build the right things. The Build–Measure–Learn
loop encapsulates the core idea of the Lean Startup
methodology and emphasizes speed as a critical
ingredient to development. Based on the output of the
Design Thinking the team defines what they are going
to Build, followed by measuring the end-users
reactions and behaviors against the delivered system
and Learn from that in order to start Building again.
The Agile method aims to define how to build the
things right. In systems like CAPTAIN that are
complex, innovative and last for about 3 years, the
traditional software development methods are not
effective. Stable plans and accurate definition of the
components at the beginning are hard to get and might
not be needed. Agile development is based on an
iterative definition and implementation of small
functional parts of the whole system. At the end of
every iteration a working increment of the system and
validate its value.
In this work we explore the engagement of end-
users in the design process at an early stage of the
system. It is mostly an exploratory work on older
adults every day habits and problems.
2 RELATED WORK
CAPTAIN’s goal is to address a new participatory
design (PD) process to the field of funded EU projects
for providing technological solutions to older adults
and create a protocol that can lead to innovative
solutions. The idea of user-driven innovation
introduced by von Hippel (Hippel, 2005) seems to have
a higher appeal in the general marketplace. The
diversity of participatory design schemas (Halskov and
Hansen, 2015) and the particularities of EU funded
projects raise the need to find new design practices.
In (Kanstrup, 2012), Kanstrup presents the maXi-
project in which designers has worked with 17
families with one or more diabetic aiming to create an
interactive system to support everyday life with
diabetes. In the COGKNOW project (Mulvenna et
al., 2007) the design team iterates the development
three times and the goal of each cycle is to improve
the final system engaging also end users through
workshops and field trials. (Zouganeli et al., 2017)
support that the users should be involved all the way
in the design. Their work aims at involving people
with mild cognitive impairment, dementia and their
caregivers and family in the design of a technological
approach providing support in various aspects of the
everyday life.
CAPTAIN tries to go beyond that approaches by
defining a protocol of user-driven innovation
approach based on business innovation model
(Design Thinking, Lean Startup and Agile) and
responsible research and innovation (RRI).
3 MATERIALS AND METHODS
This work presents the methodology and results of the
1
st
session of the Design Thinking process for
CAPTAIN project for the Greek pilot site hosted by
the Thessaloniki Active and Healthy Ageing Living
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
312
Lab (Thess-AHALL). The first phase of the Design
Thinking session, the Empathize, was carried out in a
single session with the participation of primary (older
adults) and secondary (formal and informal
caregivers) end-users followed by the Define phase
which was carried out by the CAPTAIN team.
3.1 Material Preparation
The method selected for the Empathize session was
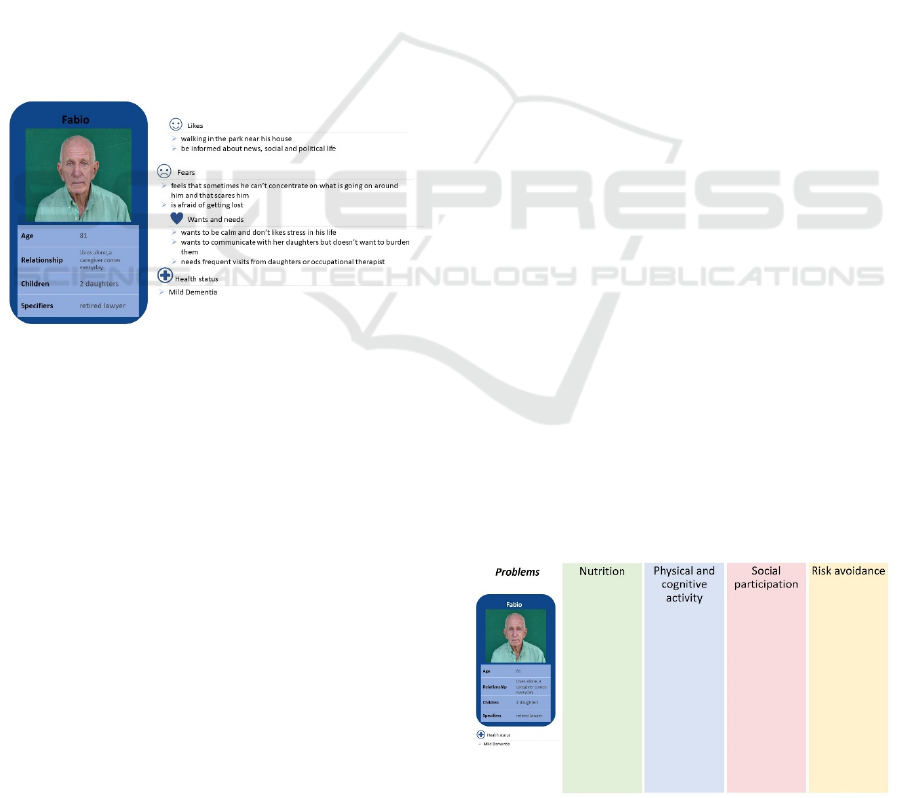
based on the use of personas. Six personas were
created that adequately depict CAPTAIN’s main
targeted end-users.
Figure 1 presents the personas
created for the session. For the preparation of the
personas the whole multidisciplinary CAPTAIN
consortium provided insights during a plenary face–
to-face meeting open discussion. Also, 6 end-users (2
older adults, 2 caregivers, 2 facilitators) were
involved in order to distinguish issues about
presentation and content. After integrating their
feedback, the personas concluded in their current
version presented in the next session.
Figure 1: Example of CAPTAIN persona.
The main goal of this session was to define the
problems that older adults face in their everyday lives
at home based on 4 main axis: nutrition, physical and
cognitive activity, social participation and risk
avoidance, and then recognize how they currently
solve these problems. As older adults are defined
people of age greater than 60 years old (World Health
Organization, 2010). The protocol for the session was
initially drafted and tested with 2 older adults in
Thess-AHALL in order to detect any issues that may
arise and improve the whole procedure.
3.2 Personas
The personas’ role is twofold: on one hand they help
partners to gain deeper understanding of the system’s
end-users and on the other hand they are created to
aid participants develop empathy and initiate
discussion about their own lives, too.
3.3 World Café
A World Café is a structured process that enables
conversation and knowledge sharing in which groups
of people discuss a topic at several tables. The
participants are switching tables periodically (one or
more times) and getting introduced to the previous
discussion at their new table by a "table facilitator"
(Brown, J. Isaacs, 2010). The methodology followed
in this work adopted the World Café conversational
framework in order to enable the participants to hear
about different user personas and increase the
empathy that they feel without limiting their opinion.
The procedure was managed and moderated by 5
table facilitators, one moderator and two assistant
personnel. Each table facilitator was in charge of a
single persona and for moderating a group of 5-6
people. At the beginning of the session the
participants were all sitting together and they attend a
small presentation of the CAPTAIN project and the
aim of the session. Subsequently, the participants
were divided randomly into 5 groups of 5-6 people.
Each group was seated in a different round table with
one facilitator. One persona was excluded from the
Greek session due to the number of participants.
After the participants have been divided into
groups and were sited in different tables, the table
facilitators presented the persona to their tables. The
personas were presented orally to the participants by
the table facilitator and were also placed in the table
in a printed version (Figure 2) .The facilitator
presented the basic information about the personas
(age, relationship, children, health status and likes)
and explained the purpose of the exercise: ‘Imagine,
define and describe the problems that this specific
persona faces in his/her everyday life”. Facilitators
avoided sketching more details on their personas than
the ones shown in the printed paper (Figure 2).
Additional information was available only for the
table facilitator (Figure 1) while other details or
questions remain unspecified, by replying for
example “We do not have this information about X”.
Figure 2: Canvas for problem definition.
Empathize with the CAPTAIN Stakeholders’ Community towards Understanding Older Adults’ Daily Needs and How They Cope with
Them
313

The facilitator encouraged the participants to
answer the following question “Which do you think
are this persona’s problems regarding the 4 main axes
(Figure 2)?”, participating also in the discussion and
helping the participants to write down their ideas. The
facilitators’ incumbent was to moderate the
conversation and make sure that it does not diverge
from the target. Each problem was written in a
separate post-it as an one short, clear phrase. The
discussion lasted for 30 minutes and was followed by
a short break to avoid straining the participants.
Afterwards, the participants switched tables so
that everyone had a new table facilitator. Each table
facilitator kept the same persona which explained to
the newcomers. Then every problem was presented
separately, inviting the participants to provide
solutions. The main objective of this round was to
find out how people are dealing with the problems
defined in the previous round. The facilitators were
encouraging the participants to talk about their own
experiences or from their environment on how they
handle similar problems (Fitzpatrick, 2014). The
team suggested a couple of solutions for each
problem and wrote them on another post-it paper
using short, clear phrases. This discussion lasted 30
minutes too.
3.4 Participation Satisfaction
Evaluation
At the end each participant was asked to answer a
short questionnaire regarding his/her satisfaction and
approval of the procedure.
The questionnaires were designed to be short
enough, to not burden the participants but include
some critical questions.
The first question was about the overall
satisfaction of the current meeting. The answers were
given in a 5-point Likert scale: 1 (Very Unsatisfied),
2 (Unsatisfied), 3 (Neutral), 4 (Satisfied), 5 (Very
Satisfied).
The second question was about the willingness to
keep attending the CAPTAIN community meetings.
This question is an indication of how interesting they
found the session and the value they find in being part
of the community.
The third question was based on Net Promoter
Score (NPS) (Promoter, 2017). NPS is a management
tool for measuring the willingness of a customer (in
our case participant) to propose a product or service.
It is an indicator of the customer’s loyalty and overall
satisfaction. It can also measure the word of mouth
accountability. Regarding CAPTAIN session, NPS
score is used as an indication of satisfaction and can
also provide an insight of the possibility to broaden
the CAPTAIN community. To calculate NPS, the
participants are divided into three categories based on
their answers.
1. Detractors are the participants that gave score
lower or equal to 6 and are more likely to
damage session’s reputation by negative word
of mouth
2. Passives that gave score 7 or 8. They most
probably enjoyed their participation but they
are not that enthusiastic to actually promote it.
3. Promoters that answered 9 or 10 who are the
most probable to encourage other people to join
too.
3.5 Participants
Thirty three Participants were recruited using
voluntary sampling (O’Leary, 2004) and were older
adults (n=26) (above the age of 60), as well as formal
and informal caregivers (n=7). As formal caregivers
are considered all types of professionals, e.g. doctors,
nurses, psychologists and physical therapists while
informal caregivers include both family members
living or not with the elderly and paid healthcare
workers, not necessarily undergoing qualified
training, who provide day-to-day help/assistance to
elderly people.
4 RESULTS
At the end of the session each facilitator gathered the
post-its that were describing the problems and the
solutions defined in the session for each persona.
These, along with the facilitator’s personal notes was
digitalized and categorized based on the objective and
not the persona. Same problems, even those defined
with different words, were consolidated in one. For
each problem various solutions were presented.
4.1 Session Output
In the following section, the problems and solutions
defined by participants of the session are presented.
4.1.1 Nutrition
In the nutrition category are included all problems
related to eating disorders, difficulties in food
preparation and consumption that may lead to eating
disorders and mental health problems that can limit
the ability of organizing food routines and eating. The
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
314

problems gathered are summarized in the following
four categories.
1. Problems in food preparation (e.g. confuse
food ingredients, burn food, do not know how
to function some devices)
2. Problems with food that are stemming from
memory issues (skip some meals, dehydration,
poor nutrition, poisoning, forget what is
permitted to eat)
3. Gain/lose weight (not balanced diet due to lack
of information, used to not healthy diet,
sensitivity in food consumption, not scheduled
meals)
4.1.2 Physical and Cognitive Activity
All the problems concerning the physical and
cognitive difficulties that an older adult might face
when dealing with everyday life activities are
included in this category. By physical activity we
mean all the activities requiring body movement and
physical strength and by cognitive all the activities
that require complicated reasoning and logic.
1. Memory issues (forget medication, forgets
where he/she stored things)
2. Decrease of body strength (lack of physical
activity, balance difficulties, fear of getting
hurt/injured, fear of falling, aches in different
body parts)
3. Psychological issues (difficulty when he/she
needs to ask for help, lack of confidence, stress,
anxiety, sadness)
4. Loss of personal capacities (sleep problems,
lose ability of solving problems, problems in
reading books/the news, problems with
personal hygiene, problem with organizing
outings, use of toilet, difficulties with
shopping)
4.1.3 Social Participation
This category focus on defining the main parameters
and variables for lifestyle and social participation.
The difficulties that came out in social inclusion and
maintain an active social life as the people age was
the main purpose of this category. This category
includes also issues that have as an impact the
possibility to lose or reduce social contacts.
1. Reluctance for group gatherings (reduced
ability to talk and communicate, trouble in
expressing/managing emotions, fear about
forgetting important things about
friends/family)
2. Change in social activities due to loss of
personal capacities (difficulties in mobility,
lack of personal time due to health
deterioration, forgets important meetings, loss
of ability to drive)
3. Change in social activities due to psychological
issues (depressive symptoms, sadness, lack of
self-esteem, fear of being a burden)
4. Unawareness (not able to find information
about local events, not familiar with
technology)
4.1.4 Everyday Risks
The scope of this category was to define everyday
issues that may lead to dangerous situation and what
older adults do in order to avoid or prevent these
situations.
1. Risks stemming from memory issues (forget to
turn off an electrical device, take wrong
medication, food poisoning, forget to lock the
front door)
2. Risks associated with physical capacity (risk of
falling, slip over cables, carpets, scattered
objects in the physical environment, dizziness
when climbing stairs, when picking something
up)
3. Risk of being deceived (abusive phone calls
and visits e.g. sales, mistakes when dealing
with money)
4.1.5 Solutions
Regardless the objective, all solutions were grouped
in four categories:
1. Reminders/Alarms, including solutions for
creating various reminders and notifications
2. List/calendars/instructions, including proposed
solutions for scheduled events, information and
lists for events or people
3. Role of relatives/friends/experts in providing
assistance or solutions to various problems.
Their role could be advisory, motivational or
educational
4. Personal motivation, concerning solutions that
require self-stimulation without the aid of
external factors. These solutions also include
behavior change.
The solutions that came up from the
discussion are presented in Table 1, Table 2, Table 3
and Table 4.
Empathize with the CAPTAIN Stakeholders’ Community towards Understanding Older Adults’ Daily Needs and How They Cope with
Them
315
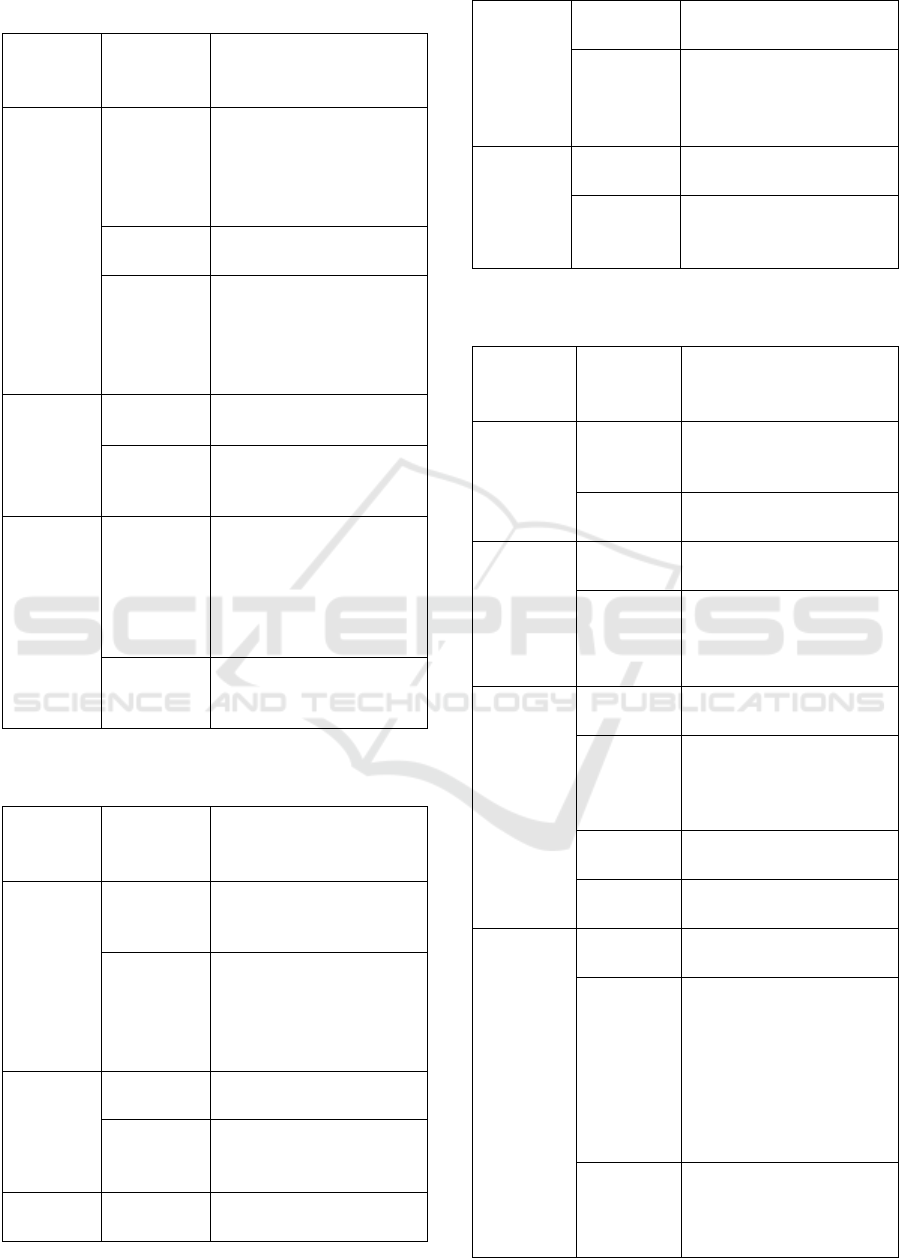
Table 1: Solutions for the problems defined for nutrition.
Problem Solution
Type
Description
Gain/lose
weight
Lists
Calendars
Instructions
- set specific hours for
meals
- friends or relatives take
care of his/her diet
- psychoeducation
Relatives
Experts
- advice from nutritionist
Personal
motivation
- exercising
- information from internet
about herbs and healthy
diet
- step by step change
Memory
issues
Reminders
Alarms
- to drink water
- to eat meals
Lists
Calendars
Instructions
- list with diet in the fridge
- list with permitted foods
Food
preparation
Relatives
Experts
- simple guidelines
- pictures on cupboards
with ingredients
- gather all the ingredients
in the table before starting
to cook
Personal
motivation
- direction from relatives on
how to use electrical
devices
Table 2: Solutions for the problems defined for physical and
cognitive activity.
Problems Solution
Type
Description
Loss of
personal
capacities
Lists
Calendars
Instructions
- create routines (time
going to bed)
Personal
motivation
- organize personal space
(place of things, furniture)
- use audio books to read
-change routines (not lifting
weight)
Psychologic
al issues
Relatives
Experts
- help from professional for
confidence issues
Personal
motivation
- Strategy games for
problem solving
- breathing exercise
Reminders
Alarms
-reminders to go walking
Decrease
of body
strength
Relatives
Experts
- help from friends/relatives
in household
Personal
motivation
- exercising
- walking, yoga, pilates
- household as a form of
exercise
Memory
issues
Reminders
Alarms
- reminders for medication
Lists
Calendars
Instructions
- pillbox to organize
medicine
- signs and labels in things
Table 3: Solutions for the problems defined for social
participation.
Problem Solution
Type
Description
Unawarene
ss
Lists/calend
ars/instructi
ons
- learn to search for local
events on the internet
Relatives
Experts
- friends/family to inform
him/her about local events
Change in
social
activities
due to
psychologic
al issues
Relatives
Experts
- meet friends through
groups and activities
Personal
motivation
- entertainment activities
- reading, writing thoughts
in a diary
- traveling
Change in
social
activities
due to loss
of personal
capacities
Reminders
Alarms
- reminders to call
relatives/friends
Lists
Calendars
Instructions
- simple instructions on
how to use technology to
communicate
- speed dial
Relatives
Experts
- friends/ relatives help in
transportation
Personal
motivation
- new hobbies (e.g. reading
group, local social group)
Reluctance
for group
gatherings
Reminders
Alarms
- reminders to meet/visit
friends
Relatives
Experts
- "dementia-awareness"
training for family and
friends to improve
knowledge of condition
- scheduled meetings with
relatives/friends
- friends to motivate to go
out/socialize
Personal
motivation
- education about the
benefit of social life
- visits in his/her former job
environment
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
316
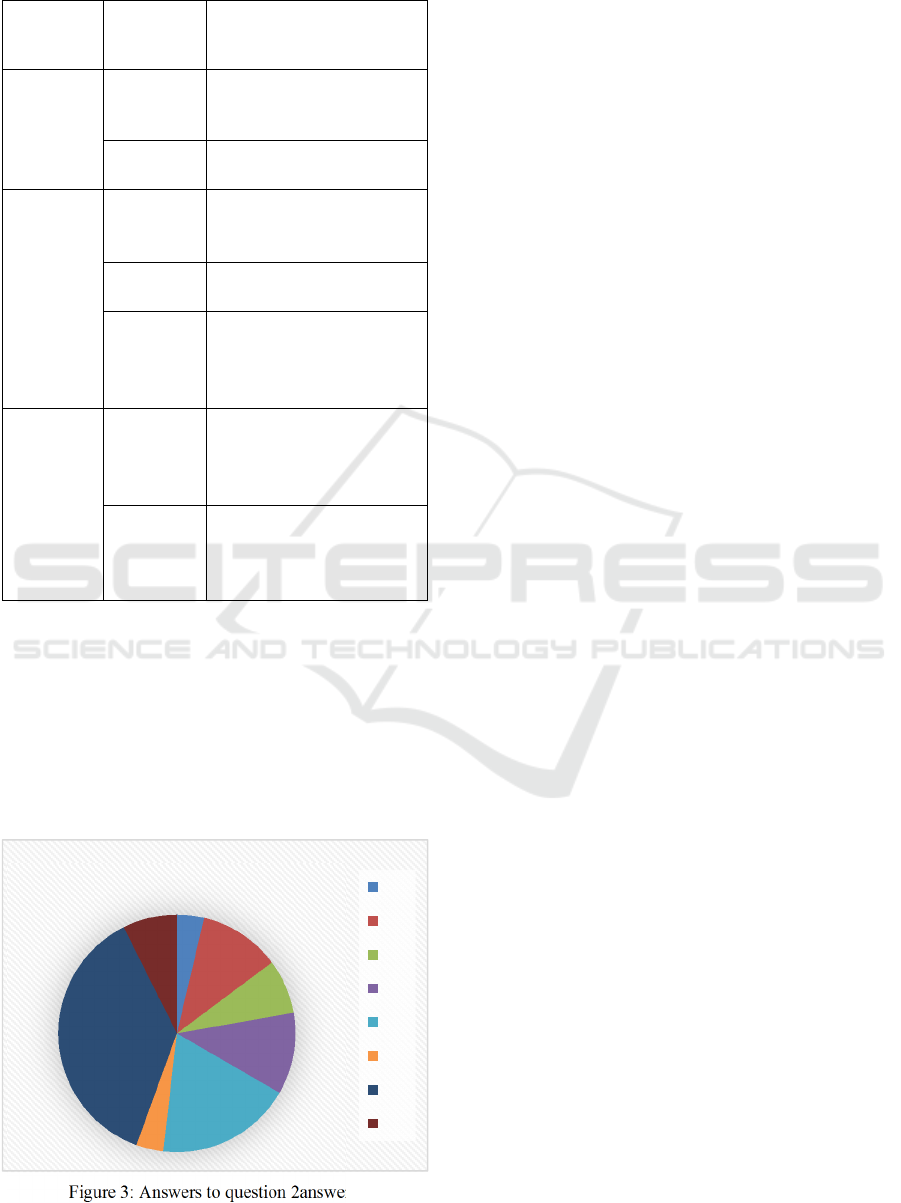
Table 4: Solutions for the problems defined for everyday
risks.
Problem Solution
Type
Description
Risk of
being
deceived
Lists/calend
ars/instructi
ons
- note down money
transactions
Personal
motivation
- not having a lot of money
at home
Risks
associated
with
physical
capacity
Reminders
Alarms
- emergency button
- automatic fall detection
system
Relatives
Experts
- help from relatives/friends
in households
Personal
motivation
- ergonomics
- avoid households that
he/she cannot do
- place useful items lower
Risks
stemming
from
memory
issues
Reminders
Alarms
- reminders to lock doors
- reminders to turn off
devices
- sign on the door to lock
Lists
Calendars
Instructions
- instructions on how to use
devices
- easily accessible list with
emergency phones
4.2 Questionnaires
As far as the participation satisfaction questionnaires
are concerned, 32 out of the 33 participants (97%)
express the will to keep attending the CAPTAIN
community meetings. The Net Promoter Score (NPS),
determined by subtracting the percentage of parti-
cipants who are detractors from the percentage who are
promoters, was NPS= 41%-22%=19 (Figure 3).
Figure 3: Answers to question 2answers.
Last but not least, there was an open question
about possible suggestions for the next session. The
participants mentioned:
“Very useful, helpful for development of
technological solutions as well as everyday practical
actions because the session makes you think deep in
problems”
“I really enjoyed it, congratulations to the
coordinators. I would like this to be repeated again
and again”
However, most of the participants did not write
any comment or recommendation.
5 DISCUSSION
This paper presents the 1
st
Design Thinking session of
the Greek pilot site of the CAPTAIN community. The
CAPTAIN consortium adopting a user-centred, agile
methodology will carry out a number of meetings
with the end-users in which participants and the
CAPTAIN team will co-design the system that older
adults would like to use.
This session’s goal was to identify the everyday
difficulties that older adults face and clarify the
means they are currently using to address these
problems. At this stage of the design, the input
gathered did not concerned technological issues. It is
very important to understand older adults’
preferences and routines and create a system that
facilitates and assists them, not a system that uses the
most innovative technology but nobody wants to use.
Some very interesting outcomes came out from
the discussion with CAPTAIN’s end-users. The fact
that a classification of solution in four main
categories was noticeable, rises the research interest
of investigating technological solution in that four
directions. Furthermore, it is clear that social life and
communication have a prominent role in older adults’
everyday lives. To this extend, a technological
solution should support their social inclusion and
interaction with other people and not try to substitute
human presence.
However, the results did not deviate from the
existing literature regarding older adults’ everyday
needs. A detailed comparison of the existing
literature, which has already been studied among the
CARTAIN consortium and the results from the
Design Thinking session is the next step.
Another important outcome of this session was
the satisfaction of involvement depicted on the
questionnaires. The goal is to create and maintain a
community throughout the project and the first step
was this session.
4%
11%
7%
11%
19%
4%
37%
7%
2
5
6
7
8
9
10
n/a
Empathize with the CAPTAIN Stakeholders’ Community towards Understanding Older Adults’ Daily Needs and How They Cope with
Them
317

ACKNOWLEDGEMENTS
This project has received funding from the European
Union’s Horizon 2020 research and innovation
programme under the Grant Agreement No. 769830.
REFERENCES
Brown, J. Isaacs, D. (2010) ‘Improvisation the World Cafe:
Shaping our futures through conversations that matter’,
Journal of Religious Leadership, 9, pp. 120–123.
Centers for Disease Control and Prevention (2013) The
state of aging & health in America 2013, Centers for
Disease Control and Prevention US Dept of Health and
Human Services. doi: 10.2217/1745509X.3.2.139.
Chaudhuri, S., Thompson, H. and Demiris, G. (2014) ‘Fall
detection devices and their use with older adults: A
systematic review’, Journal of Geriatric Physical
Therapy, pp. 178–196. doi: 10.1519/JPT.0b013e3182a
be779.
Chen, Y. R. R. and Schulz, P. J. (2016) ‘The Effect of
Information Communication Technology Interventions
on Reducing Social Isolation in the Elderly: A
Systematic Review’, Journal of medical Internet
research, p. e18. doi: 10.2196/jmir.4596.
Fitzpatrick, R. (2014) ‘The Mom Test’, Igarss 2014, (1),
pp. 1–5. doi: 10.1007/s13398-014-0173-7.2.
García-Lizana, F. and Sarría-Santamera, A. (2007) ‘New
technologies for chronic disease management and
control: A systematic review’, Journal of Telemedicine
and Telecare, 13(2), pp. 62–68. doi: 10.1258/1357
63307780096140.
Halskov, K. and Hansen, N. B. (2015) ‘The diversity of
participatory design research practice at PDC 2002-
2012’, International Journal of Human Computer
Studies, 74, pp. 81–92. doi: 10.1016/j.ijhcs.2014.09.
003.
Hippel, E. von (2005) Democratizing innovation, The
evolving phenomenon of user innovation. doi:
10.1111/j.1540-5885.2006.00192_2.x.
Kanstrup, A. M. (2012) ‘A small matter of design’, in, p.
109. doi: 10.1145/2347635.2347651.
Mulvenna, M. et al. (2007) ‘COGKNOW : Translating
Research Innovation into Products and Services’,
Expanding the Knowledge Economy, Issues,
Applications, Case Studies, pp. 575–583.
O’Leary, Z. (2004) ‘Volunteer Sampling’, in The Essential
Guide To Doing Research, p. 110. doi:
10.4135/9780857020116.n223.
Plattner, H., Meinel, C. and Leifer, L. (2011) Design
Thinking Research - Understanding Innovation, Design
Thinking: Understand, Improve, Apply. doi:
10.1016/B978-0-12-387667-6.00013-0.
Promoter, N. (2017) ‘Net Promoter Score ® Calculation’,
Inside Learning Technologies & Skills, 135, pp. 1–5.
Reeder, B. et al. (2013) ‘Framing the evidence for health
smart homes and home-based consumer health
technologies as a public health intervention for
independent aging: A systematic review’, International
Journal of Medical Informatics, pp. 565–579. doi:
10.1016/j.ijmedinf.2013.03.007.
Ries, E. (2011) The Lean Startup, Journal of Chemical
Information and Modeling. doi: 23.
Schwenk, M. et al. (2015) ‘Wearable sensor-based in-home
assessment of gait, balance, and physical activity for
discrimination of frailty status: Baseline results of the
Arizona frailty cohort study’, Gerontology, 61(3), pp.
258–267. doi: 10.1159/000369095.
World Health Organization (2010) Definition of an older or
elderly person, Geneva, Switzerland: WHO. Available
at: http://www.who.int/healthinfo/survey/ageingdefn
older/en/index.html.
Yang, N. and Ornstein, K. (2015) ‘The impact of symptom
burden on hospitalization, nursing home placement and
death among homebound older adults’, Journal of the
American Geriatrics Society, 63(SUPPL. 1), p. S134.
doi: http://dx.doi.org/10.1111/jgs.13439.
Zouganeli, E. et al. (2017) ‘Responsible Development of
Self-learning Assisted Living Technology for Older
Adults with Mild Cognitive Impairment or Dementia’,
in 3rd International Conference on Information and
Communication Technologies for Ageing Well and e-
Health Volume 1: ICT4AWE, ISBN 978-989-758-251-
6, pp. 204–209. doi: 10.5220/0006367702040209.
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
318
