
Methods of Increasing Statokinetic Stability in Racers using
Normobaric Hypoxia and Neck Muscle Training
Alexander Bolotin
1
, Vladislav Bakayev
1
and Leonid Buynov
2
1
Institute of Physical Education, Sports and Tourism, Peter the Great St. Petersburg Polytechnic University,
St. Petersburg, Russian Federation
2
The Herzen State Pedagogical University of Russia, St. Petersburg, Russian Federation
Keywords: Racers, Statokinetic Resistance, Normobaric Hypoxia, Neck Muscle Training.
Abstract: In recent years, against the background of a significant improvement in the equipment of pilots,
improvement of technical characteristics of cars, a significant increase in the speed of movement of race
drivers on the highway has been noted. At the same time, the psychophysiological capabilities of athletes
remained virtually unchanged. This discrepancy, in turn, led to the fact that when the dynamic factors of the
race and the speed of movement on the track are excessively affected, the athlete's body is affected by forces
that impair not only its functional state, but also negatively affect competitive activity. To improve
statokinetic stability of the experimental group subjects, a within a month normobaric hypoxia training
course in combination with cervical muscle exercises was used. The control group subjects were given
“fake” normobaric hypoxia courses and performed no dedicated cervical muscle exercise. The results of the
study showed that the experimental group subjects who received normobaric hypoxia in combination with
cervical muscle exercise demonstrated a reliably improved continuous cumulation of Coriolis acceleration
(CCCA) tolerance time (versus initial measurements). Besides, there was a decrease in the manifestation
degree of vestibulosensory, vestibulovegetative, and vestibulosomatic reactions, which generally indicates
improvement of CCCA tolerance in this group of subjects. athletes.
1 INTRODUCTION
Currently, the most important conditions for
achieving high results in the world of big sports is
the presence of a sufficient amount of psycho-
physiological reserves, a good functional state and a
high level of performance in an athlete.
Especially important is the presence of the
optimal state of the above-mentioned psycho-
physiological characteristics for athletes-racers,
whose competitive activity is associated with high
voltage psycho-physiological functions of the body
during movement on the track at high speeds.
During the competition race car drivers Formula 1
speed of movement on the highway exceeds 300 km
per hour. Pilots have great overloads and, against
this background, they must make the right decisions
for the minimum amount of time during a
competitive fight. Such activities place high
demands on the psycho-physiological systems of the
pilot's body.
Researches of some scientists provides evidence
that excessive exposure to dynamic loads negatively
influences the bioelectric cerebral cortex activity and
conditioned reflexes, memory and attention,
emotional responses and orientation in space.
Meanwhile, the time on the race track, as well as the
number of mistakes, including gross mistakes,
affecting the safety of the athlete’s racers movement,
increases.
This circumstance dictates the need to search for
new effective means and methods for training of
race drivers directed at improvement of their
functional state and the level of their physical
performance (Bakaev et al., 2015, Bolotin &
Bakayev, 2016, Dong, 2016, Malcata & Hopkins,
2014, Wrigley, 2015, Bolotin & Bakayev, 2017,
Bolotin & Bakayev, 2018, Gorshova, et al., 2017,
Ivashchenko, et al., 2017, Bakaev, et al., 2016, Bakaev,
et al., 2018). This is related to a high degree of
manifestation of sensory, vegetative and somatic
components of statokinetic reactions in race drivers.
The physiologic methods currently used for
improvement of the functional state and physical
performance of athletes, as a rule, directly influence
various physiologic systems of race drivers. Such
Bolotin, A., Bakayev, V. and Buynov, L.
Methods of Increasing Statokinetic Stability in Racers using Normobaric Hypoxia and Neck Muscle Training.
DOI: 10.5220/0008198001670172
In Proceedings of the 7th International Conference on Sport Sciences Research and Technology Support (icSPORTS 2019), pages 167-172
ISBN: 978-989-758-383-4
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
167

methods include, inter alia, the method of
normobaric hypoxia training which, apart from
improving athletes’ tolerance to a lack of oxygen, is
used to enhance their bodies’ resistive and adaptive
capability to adverse effects of a number of other
agents (Mao, et al., 2014, Mekjavic, et al., 2016,
Gonggalanzi, et al., 2017, Naeije, 2014).
Currently, despite availability of a detailed
description of mechanisms of negative impact of
hypoxia on organs and tissues, in certain conditions
it can also be regarded as a driver of expansion of
physiologic ranges of functional systems and
facilitate improvement of athletes’
psychophysiologic capabilities. The use of
normobaric hypoxic training in combination with the
training of individual muscle groups can lead to an
optimization of the functional state of athletes and
an increase in their working capacity (Bolotin, &
Bakayev, 2017a, Bolotin, & Bakayev, 2017b,
Bolotin, & Bakayev, 2017c).
The aim of this research was to develop a
methodology for the use of normobaric hypoxia in
combination with special training of the neck
muscles, with race drivers, to increase their
statokinetic resistance to competitive activity.
2 ORGANIZATION AND
METHODS
The research was performed at the Department of
Medical and Valeological Specialties in Herzen
State Pedagogical University of Russia and the
Institute of Physical Culture, Sports and Tourism in
Peter the Great St. Petersburg Polytechnic
University. Its subjects were race drivers aged 18–20
in whom the continuous cumulation of Coriolis
acceleration (hereinafter “CCCA”) test tolerance
time amounted to less than two minutes.
At the initial stage of the experiment, all the
subjects were introduced to the plan and procedure
of the forthcoming research, and the methods it
used. All subjects provided voluntary written
consent to participate in the experiment.
Next, random sampling was used to form two
groups of subjects: the experimental group (n-11)
and the control group (n-14). Subsequently the
experimental group subject were engaged in a within
one month course of normobaric hypoxia training
(hereinafter “NBHT”) in combination with dedicated
cervical muscle exercises (hereinafter “DCME”).
The control group subjects received “fake” courses
of NBHT and performed no DCME.
After a month-long experiment, all subjects were
re-examined in their original volume. Then the
survey in the original volume was repeated after one,
two and three months after the end of the
experiment.
In the course of the experiment, the CCCA test
tolerance time was determined using the procedure
and evaluation according to the traditional R. Barany
chair method.
The severity of sensory, vegetative, and somatic
components of statokinetic reactions was also
assessed. It was determined with the help of the
scoring system developed by us: 0 - no sensations; 1
- mild; 2 - strong sensations.
In the experimental group (EG) for the NBHT
we used the Bionova-Nova-204, AF system (Russia).
The NBHT was performed in a course of 14
sessions. Duration of each session was 30 minutes.
During the first session, the subjects were
administered hypoxic gas mix with 17.0% oxygen
content. During the following four sessions, oxygen
content was reduced to 1.0–2.0%. Starting from the
fifth session to the end of the NBHT course, oxygen
content in the hypoxic gas mix was maintained at the
level of 12.0–14.0%.
The DCME method included two exercises in the
supine position. In Exercise No.1, the subject was
supine on the gymnastic bench, with the head poised
(earphone helmet loaded with 500 g weight
prevented engagement of muscles adducting the
head to the chest). In Exercise No.2, a rubber band,
secured around the head with the loose end
protracting from the back of the head, was fixed 0.8
meters higher than the bench level, preventing
engagement of muscles extending the head. In both
exercises the subject evenly tilted the head upward
and downward, making one movement in two
seconds, with the tilt angle of 30.0°, duration of each
exercise 5 minutes, and break between exercises also
5 minutes.
Immediately after CCCA, the ST-02 stabilograph
was used for the subjects to perform a static
stabilometric test in the integrated functional
computer stabilography (hereinafter “SST IFCS”),
consisting of two tests: test No.1 was performed
with the eyes open and gaze of the subject fixed on
the remote (5 m) object; test No.2 was performed
with the eyes closed. The duration of tests amounted
to 20 seconds, with the break of 1 minute between
them. The following parameters were captured: the
average rate of increase of the statokinesiogram
length and area, oscillation amplitude (hereinafter
“OA”), coefficient of asymmetry (hereinafter “CA”)
of the projection of the common center of gravity
icSPORTS 2019 - 7th International Conference on Sport Sciences Research and Technology Support
168

(hereinafter “PCCG”) in the frontal and sagittal
planes and directions.
Statistical processing of the obtained data was
performed using Microsoft Excel software kit
according with accepted standards. For each sample
of parameters, numerical distribution characteristics
were calculated. The statistical significance of
difference between the compared samples was
evaluated using the parametric Student’s t-test.
3 RESULTS AND DISCUSSION
The results obtained in the course of the experiment
justify a conclusion that the monthly combined use
of NBHT and DCME reliably improved CCCA
tolerance in the subjects of the experimental group.
This was accompanied by a reduced degree of
manifestation of sensory, vegetative and somatic
components of statokinetic reactions (Table 1).
As seen from Table 1, in the open eyes test there
was a reliable decrease in the parameters descriptive
of the rate of increase in the length (by 11.3%) and
area (by 12.4%) of the statokinesiogram, OA PCCG
in the frontal (by 14.1%) and sagittal (by 12.7%)
planes, CA in the frontal (by 13.6%) and sagittal (by
11.9%) directions. At the same time, in the closed
eyes test there was no statistically significant
difference between the parameter values before and
after course use of NBHT and DCME.
In comparison with the initial measurements, the
CCCA test tolerance time was improved by 93.7%.
Moreover, there was a 42.8% reduction in
parameters descriptive of heat sensation, 43.7%
reduction in head heaviness sensation, 57.2%
reduction in vertigo sensations, and 53.7% reduction
in stomach discomfort. Besides, there was a
reduction in hypersalivation by 54.3%, hyperhidrosis
by 53.7%, manifestation degree of protective
movements by 47.9%, and time of post-rotation
nystagmus by 17.8%.
The observed positive dynamics in the above-
listed parameters indicates that the experimental
group test subjects could tolerate CCCA loads on the
R. Barany chair longer and easier.
The obtained dynamics is concordant with the
nature of change in parameters obtained during SST
IFCS which the subjects underwent after the CCCA
test (Table 2).
One of the tasks we intended to solve by the
experiment was to determine the duration of the
achieved effect from the monthly combined use of
NBHT and DCME. To this end, after the course
performance of NBHT and DCME, the subjects
were retested in one, two and three months.
The analysis of the obtained data shows that the
highest value of CCCA tolerance time in the
experimental group subjects was reached
immediately after course application of NBHT and
DCME; later its values started to gradually decrease
and were back to the initial level by the end of the
third month (Figure 1).
Simultaneously there was a reduction of basal
metabolism and more economical use of oxygen by
tissues. These changes helped expand reserve
capabilities of the body’s functional systems and
increase physical performance of athletes (Hackett,
& Rennie, 2016, Luks, et al., 2017).
Table 1: Tested Functional Parameters for Subjects “Before” and “After” monthly Use of NBHT in Combination with
DCME (X±δ).
Test
parameters
Experimental
group
Control
group
Before
After
Before
After
CCCA tolerance time (seconds)
109.7±5.7
213.4±9.7*
98.5±6.6
98.9±7.5
Heat sensation (points)
0.5±0.05
0.3±0.04*
0.4±0.06
0.4±0.05
Head heaviness sensation (points)
0.5±0.06
0.3±0.07*
0.5±0.06
0.5±0.07
Vertigo sensation (points)
0.4±0.06
0.2±0.05*
0.4±0.05
0.4±0.06
Stomach discomfort (points)
0.4±0.05
0.2±0.06*
0.4±0.07
0.4±0.08
Hypersalivation degree (points)
0.6±0.05
0.3±0.06*
0.5±0.07
0.5±0.08
Hyperhidrosis degree (points)
0.4±0.04
0.2±0.05
0.4±0.06
0.4±0.07
Protective movements (points)
0.7±0.08
0.4±0.06*
0.6±0.07
0.6±0.08
Nystagmus duration (seconds)
21.0±3.3
17.3±3.5*
20.1±3.5
20.0±3.7
Number of subjects
11
11
14
14
Note: - reliability of differences: * - p<0.05 versus initial parameter values.
Methods of Increasing Statokinetic Stability in Racers using Normobaric Hypoxia and Neck Muscle Training
169
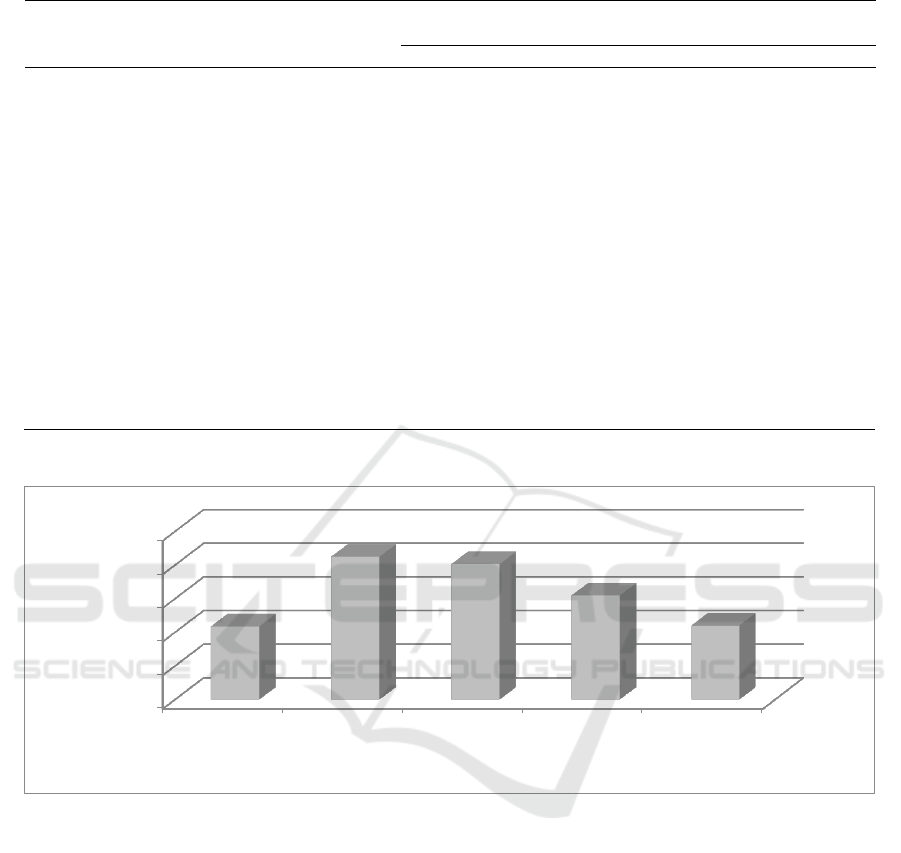
Table 2: SST IFCS Parameters for Subjects “Before” and “After” monthly use of NBHT in combination with DCME (X±δ).
Test
Parameters
Experimental
group
Control
Group
Before
After
Before
After
Open eyes test
Length increase rate (mm/s)
41.2±1.8
37.4±1.7*
38.5±2.3
39.0±2.0
Area increase rate (mm²/s)
68.4±3.4
61.3±3.3*
62.4±4.1
61.3±4.8
OA PCCG, frontal plane (mm)
6.8±0.4
5.9±0.3*
6.3±0.6
6.4±0.5
OA PCCG, sagittal plane (mm)
7.1±0.3
6.3±0.4*
6.4±0.7
6.6±0.8
CA, frontal direction (%)
7.4±0.4
6.4±0.5*
6.6±0.6
6.8±0.7
CA, sagittal direction (%)
7.6±0.3
6.7±0.4*
7.3±0.6
7.2±0.7
Closed eyes test
Length increase rate (mm/s)
46.2±4.5
44.3±4.6
44.4±5.1
43.6±4.9
Area increase rate (mm²/s)
64.3±5.5
62.0±4.8
69.8±5.4
60.1±5.0
OA PCCG, frontal plane (mm)
8.0±0.8
8.0±0.9
7.7±0.8
7.5±0.8
OA PCCG, sagittal plane (mm)
7.5±0.7
7.4±0.8
8.2±0.7
8.1±0.8
CA, frontal direction (%)
7.4±0.9
7.3±0.8
7.8±0.8
7.9±0.7
CA, sagittal direction (%)
7.2±0.8
7.1±0.9
8.1±0.9
8.0±0.8
Note: Reliability of differences: * p<0.05 versus initial parameter values.
Note: Reliability of differences: * - p<0,05 versus initial parameter values.
Figure 1: The CCCA test tolerance time in the experimental group subjects “Before”, “After”, and in 1, 2, and 3 months
following the course use of NBHT in combination with DCME (in seconds).
On the cellular level, the body responded by
enhancing the capacity of the energy supply system
due to the increase of mitochondria count and
activation of the respiratory chain ferments.
Therefore, improvement of non-specific
resistance of the body emerging as a result of
adaptation to normobaric hypoxia induces a whole
array of physiologic changes in race driver. These
changes play an important role in correction of the
athletes’ functional state and optimization of
capabilities of organs and systems in athletes
(Pieralisi, 2017, Mao, 2014).
Finally, this mechanism plays a role of a critical
link in the chain of adaptation changes and
ultimately facilitates improvement of tolerance to
statokinetic exposures and reduction of the
manifestation degree of sensory, vegetative and
somatic reactions (Gonggalanzi, et al., 2017,
Hopkins, et al., 2009, Luks, et al., 2017).
In their turn, physical exercises in the form of
regular and adequately selected types of loads assist
enhancement of the vascular tone, improve the
cardiovascular and external respiratory function.
They optimize gas exchange and redox processes,
thereby improving bioelectric activity and
reinforcing excitatory processes in the structures of
the central nervous system, facilitating overall
0
50
100
150
200
250
Before the
study
After research In one month After two
months
In three
months
*
*
*
icSPORTS 2019 - 7th International Conference on Sport Sciences Research and Technology Support
170

enhancement of the stamina and physical
performance of the body race drivers.
It has been established that the increase of
statokinetic stability under the influence of DCME is
caused by the change in the sensitivity threshold of
the vestibular, visual, interoceptive, tactile and
proprioceptive analyzers (Wrigley, 2015).
In turn, this improves tolerance to statokinetic
loads through faster and more adequate build-up of a
single statokinetic stability system in athletes.
4 CONCLUSIONS
1) The use of NBHT in combination with DCME
during the month of training significantly increases
the tolerance time of the CCCA test, while reducing
the severity of the sensory, vegetative and somatic
components of the statokinetic reactions of the race
drivers.
2) The highest value of the time of portability of
CCCA is noted immediately after the monthly use of
NBHT in combination with DCME. The achieved
effect lasts for two months, then gradually decreases
to baseline. This indicates the need for such training
with racers at the final stage of the preparatory
period for competitive activities.
REFERENCES
Bakaev, V.V., Bolotin, A.E., & Vasil'eva, V.S. (2015).
Factors determining sports specialization of cross
country skiers. Teoriya i Praktika Fizicheskoy Kultury,
(2), 40-41.
Bakaev, V.V.,Bolotin, A.E., & Aganov, S.S. (2016).
Physical training complex application technology to
prepare rescuers for highland operations. Teoriya i
Praktika Fizicheskoy Kultury, (6), pp.6-8.
Bakayev V., Vasilyeva V., Kalmykova S., & Razinkina E.
(2018). Theory of physical culture - a massive open
online course in educational process. Journal of
Physical Education and Sport, 18(1), pp.293-297.
DOI: 10.7752/jpes.2018.01039
Bolotin, A., & Bakayev, V. (2016). Factors that determine
high efficiency in developing speed and strength
abilities of female hurdlers. Journal of Physical
Education and Sport, 16(3), 910-913.
Bolotin A., & Bakayev V. (2017). Structure of the
parameters that define the preparedness of archers for
competitive struggle. Journal of Physical Education
and Sport, 17(3), pp.1177-1179. DOI:10.7752/
jpes.2017.03181
Bolotin, A, & Bakayev, V. (2017a). Peripheral circulation
indicators in veteran trail runners. Journal of Physical
Therapy Science, 29(8), 1092–1094.
Bolotin A., & Bakayev V. (2017b). Method for Training
of Long Distance Runners Taking into Account
Bioenergetic Types of Energy Provision for Muscular
Activity. In Proceedings of the 5th International
Congress on Sport Sciences Research and Technology
Support - icSPORTS, ISBN 978-989-758-269-1, pages
126-131. DOI: 10.5220/0006516101260131
Bolotin A., & Bakayev V. (2017c). The differences in
response of the respiratory system of long and middle-
distance runners and their influence on recovery rate.
Journal of Physical Education and Sport, 17(4),
pp.2443-2446. DOI: 10.7752/jpes.2017.04272
Bolotin, A., & Bakayev, V. (2018). Pedagogical practice
for development of coordination potential of MMA
fighters and estimation of its efficiency. Journal of
Human Sport and Exercise, 13(1), 72-88.
doi:https://doi.org/10.14198/jhse.2018.131.08
Dong, J. (2016). The role of heart rate variability in sports
physiology (Review). Experimental and Therapeutic
Medicine, 11, 1531-1536. doi.org/10.3892/etm.
2016.3104
Gorshova I., Bohuslavska V., Furman Y., Galan Y.,
Nakonechnyi I., & Pityn M. (2017). Improvement of
adolescents adaptation to the adverse meteorological
situationby means of physical education. Journal of
Physical Education and Sport, 17(2), 892-898.
DOI:10.7752/jpes.2017.02136
Ivashchenko O., Yarmak O., Galan Y., Nakonechnyi I., &
Zoriy Y. (2017). Leadership as a fundamental aspect
of the performance of student-athletes in university
men’s sports teams. Journal of Physical Education
and Sport, 17, Supplement issue 2, 472 – 480.
DOI:10.7752/jpes.2017.s2071
Gonggalanzi, Labasangzhu, Bjertness E, Wu T, Stigum H,
& Nafstad P. (2017). Acute mountain sickness, arterial
oxygen saturation and heart rate among Tibetan
students who reascend to Lhasa after 7 years at low
altitude: a prospective cohort study. BMJ Open, 7(7),
e016460. doi:10.1136/bmjopen-2017-016460.
Hackett, P. & Rennie, D. (2016). The incidence,
importance, and prophylaxis of acute mountain
sickness. Lancet, (7996), 1149–1155.
Hopkins, W., Marshall, S., Batterham, A., & Hanin, J.
(2009). Progressive statistics for studies in sports
medicine and exercise science. Medicine & Science in
Sports & Exercise, 41(1), 3-12.
Luks, A., Swenson, E., & Bärtsch, P. (2017). Acute high-
altitude sickness. Eur. Respir. Rev., 26(143):160096.
Malcata, R., & Hopkins, W. (2014). Variability of
competitive performance of elite athletes: a systematic
review. Sports Medicine, (44), 1763-1774.
Mao, Y. Chen, P., Li, L., & Huang, D. (2014). Virtual
reality training improves balance function. Neural
Regeneration Research, 9(17), 1628-1834.
Mekjavic, I. Amon, M., Kölegård, R. et.al. (2016). The
effect of normobaric hypoxic confinement on
metabolism, gut hormones, and body composition.
Frontiers in Physiology. (7), 202–214.
Methods of Increasing Statokinetic Stability in Racers using Normobaric Hypoxia and Neck Muscle Training
171

Naeije, R. (2014). High-altitude adaptation: where
Tibetans and Han Chinese agree. Exp. Physiol.,( 99),
1593–1604.
Pieralisi, M., et al. (2017). An Electromagnetic Sensor for
the Autonomous Running of Visually Impaired and
Blind Athletes (Part I: The Fixed Infrastructure),
Sensors, 17(2), 364.
Wrigley, A. (2015). Recent changes in hypoxia training at
the Royal Air Force Centre of Aviation Medicine. J. R.
Nav. Med. Serv., 101(2), 186–197.
icSPORTS 2019 - 7th International Conference on Sport Sciences Research and Technology Support
172
