
Blockchain or Distributed Ledger Technology
What Is in It for the Healthcare Industry?
Nabil Georges Badr
a
Higher Institute for Public Health, Saint Joseph University, Lebanon
Keywords: Blockchain, Patient Data, Distributed Ledger Technology, Privacy, Security, Electronic Health Records.
Abstract: Distributed ledger technology has seen its debut into communities of practice in healthcare where the reliance
on knowledge sharing between participants postulates the foundations of secure and distributed knowledge,
especially in some sensitive context, such as patient information. This knowledge is essential for the practice
of care from patient contact to research, pharmaceutical supply chain, medication adherence and management
of the plethora of bedside data into a collection of knowledge about the patient, essential to quality care. We
introduce different schools of thought and implementation contexts of the distributed ledger technology or
Blockchain. We provide an overview of Blockchain and Distributed Ledger Technology, focused on the
Healthcare industry, as an initial assessment of the validity of an application of Distributed Ledger
Technology in a specific knowledge management model to solve problems related to knowledge sharing in
medical knowledge management systems. The paper summarizes some instances of most likely and unlikely
uses of Blockchain in the healthcare setting. The paper also introduces a few use cases where some short-term
benefits from such implementation.
1 INTRODUCTION
The growth of data in healthcare has brought a
disruptive foray of new technologies to find, manage,
move and maintain digital information. Distributed
Ledger Technology (DLT) or Blockchain will likely
not revolutionize healthcare immediately, however,
may transform it forever.
Communities of practice in healthcare rely on
knowledge sharing between participants (Jørgensen
et al, 2019) with data that must meet the foundations
of secure and distributed knowledge (Li et al, 2018),
especially in some sensitive context, such as patient
information. Practitioners must make sense of all data
presented to them and leverage technology advances
for predictive modelling that has the premise to
integrate all data sources into a single ecosystem and
accelerate the visualization of the patient’s case in
order to provide accurate evidence based diagnoses
(Rakic, 2018). Therefore, in practicality,
Blockchains could be complementary to digital
medical records. DLT with its features of handling
and anonymizing data, will likely enter the healthcare
IT market subtly, making certain service areas of the
a
https://orcid.org/0000-0001-7110-3718
industry more efficient. Based on dynamic ontologies
of knowledge management, which may tie into
changing state of data, and status of practice
processes and workflows (Jurisica et al, 2004), DLT
could enable healthcare staff to get information in a
shorter timeframe without searches, paperwork,
signatures, etc. Similar to how electronic medical
records (EMR), MPI (Master Patient Index) systems,
and data analytics are slowly changing workflows by
increasing the capabilities of staff in healthcare
organizations (Le Nguyen, 2018).
Treatment of patient data is an essential
component to building knowledge management
systems for managing the quality of care and
improving patient outcome (Wang et al, 2018).
However, handling patient data will never be totally
risk-free.
Patient data has had three major concerns:
Who owns it?
Who has access to it?
If they have access to it, how they can use it?
These concerns are complicated by the plethora of
conditions of privacy, confidentiality and security.
This position paper attempts to address the data
concerns through the potential implementation of
Badr, N.
Blockchain or Distributed Ledger Technology What Is in It for the Healthcare Industry?.
DOI: 10.5220/0008348902770284
In Proceedings of the 11th International Joint Conference on Knowledge Discovery, Knowledge Engineering and Knowledge Management (IC3K 2019), pages 277-284
ISBN: 978-989-758-382-7
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
277

Blockchain or Distributed Ledger Technology.
Which begs the research question: Blockchain or
Distributed Ledger Technology - What is in it for the
Healthcare Industry?
2 DISTRIBUTED LEDGER
TECHNOLOGY OR
BLOCKCHAIN
Distributed ledger technology (DLT) is a digital
system for recording transaction of assets in which
the transactions and their details are registered in
multiple places at the same time. Unlike traditional
databases, distributed ledgers have no central data
store or administration functionality. Basically, “a
Blockchain is a distributed, transactional database.
Globally distributed nodes are linked by a peer-to-
peer (P2P) communication network with its own layer
of protocol messages for node communication and
peer discovery” (Glaser 2017, p. 1545).
Blockchain implementation can be public, open
to the public, where the only protection is provided
by encryption. As “everyone can see everything” on
a Blockchain network. In contrast, Private
Blockchains are Blockchains with organizational
level implementations where varying levels of control
of who can access data, who can modify data, and
who ultimately has authority in the system (Yip,
2016).
Some claim that new technology implementations
that involve a high volume of data collection, such as
the case of Internet of Things (IoT), lend themselves
well to novel Blockchain applications, as do networks
and machine visualization, public key cryptography,
web applications, certification schemes and the
secure storage of Personally Identifiable Information
(PII) (Taylor, et al, 2019).
While Blockchain may have significant potential
to improve data interoperability (Brodersen, et al,
2016), and address issue in security and privacy
(Esposito et al, 2018), it is important to note the
boundaries of the technology: Blockchain is not a
substitute for an enterprise database and are not
optimized for high volume data exchange necessary
for applications in an organization. Blockchain
solutions are designed to record specific
transactional data events that are meant to be shared
across a network of parties where transparency and
collaboration are mission critical (RJ Krawiec, et al,
2016). Each party on the Blockchain has access to the
whole database; no single party controls the
information. Communication is directly between
peers, each node stores and forwards information to
other nodes; transactions occur between Blockchain
addresses (pseudonyms); once the record is entered,
it cannot be altered (Iansiti and Lakhani, 2017).
Furthermore, though debatable, the literature has
touted the “transparency and trust” element of
Blockchain technology (Agbo et al, 2019). The
inherent data verifiability of Blockchain could add an
atmosphere of trust, however, trust is still a difficult
factor to establish as it relates to data quality, access,
security and other human factors.
2.1 Two Schools of Thought
There are two schools of thought on the use of DLT
for healthcare. One professes that a Blockchain could
unlock the true value of interoperability (Krawiec, et
al, 2016). Another, more centred on protecting data
privacy, recognizes the fundamental role of the
Blockchain as an access-control manager for health
records and data (Linn and Koo, 2016).
In broad terms, both directions support principles
of integration of healthcare information across a
range of uses and stakeholders. There are varying
levels of control of who can access the data, who can
modify the data, and who ultimately has authority in
the system.
With a distributed ledger technology, all
participants would have access to the distributed
ledger to maintain a secure exchange without
complex brokered trust. Thus, establishing a “Trust
Network” that would reduce the complexity of
sharing clinical information among different
healthcare information systems, as an intermediary to
establish point-to-point sharing and “book-keeping”
of what data is to be exchanged (RJ Krawiec, et al,
2016).
2.2 The Healthcare Context
In the healthcare context, research has concentrated
on applications using distributed ledger technology to
focus on integration, integrity and access control of
health records and related patient data (Dagher et al,
2018). However, other diverse and interesting
applications are emerging, addressing clinical trials
(Nugent et al, 2016), biomedical databases (Kleinaki
et al, 2018) and medical insurance (Zhou et al, 2018).
Some works have advanced architectures that aim at
protecting data and sense-making of data collected by
embedded devices, wearables (Brogan et al, 2018),
and sensors (Angeletti, 2017), designs to build
building tamper resistant M-health devices
(Ichikawa, 2017), in addition to proposals for
KMIS 2019 - 11th International Conference on Knowledge Management and Information Systems
278
extending the technology to manage medicines
supply chain (Tseng, et al, 2018),
Recently, this subject has occupied the forefront
of the biomedical research. Scholars have reported on
the potential of using DLT to maintain the integrity
and access control of data collected in clinical trial
records (Benchoufi, 2018) and presented use cases
where medical transaction records (Tseng, et al,
2018), consent forms (Benchoufi, 2018), and
financial records, have been managed by a form of
DLT implementation for features of traceability,
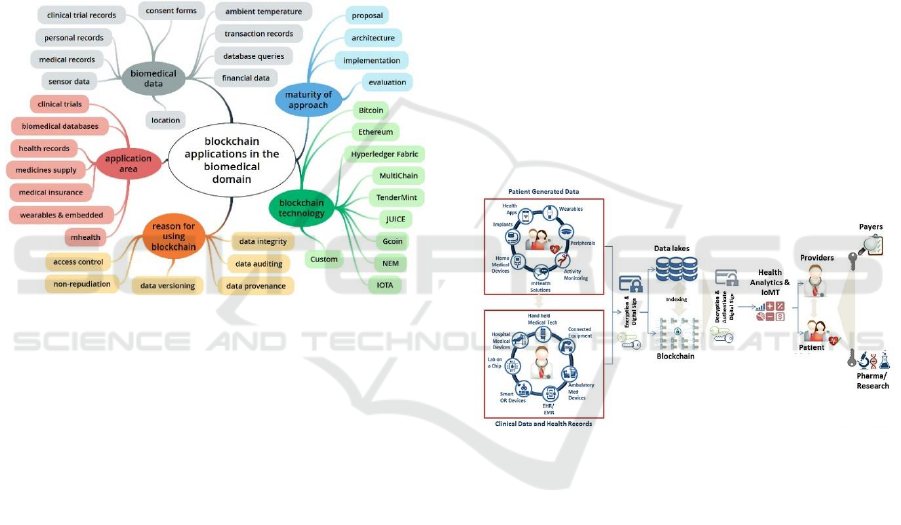
provenance, and non-repudiation. Drosatos and
Kaldoudi, 2019, for instance, summarize current
coverage of the literature on DLT in the biomedical
domain (Figure 1).
Figure 1: Blockchain application in the biomedical domain
(from Drosatos and Kaldoudi, 2019; Fig 7).
Similarly, practitioners have positioned DLT in
Healthcare IT implementations, to address Master
Patient Index (MPI) challenges that arise from the
need to synchronize multiple patient identifiers
between systems while securing patient privacy.
Distributed Ledger Technology could use private and
public identifiers secured through cryptography, to
create a singular, more secure method of protecting
patient identity. Varying data standards reduce
interoperability because records are not compatible
between systems. Distributed Ledger Technology
could enable near real-time updates across the
network to all parties. Other institutions, in
Population Health management, have identified a
benefit in Distributed Ledger Technology that could
enable secure access to patient longitudinal health
data across the distributed ledger. Blockchain
technology can provide the means to aggregate and
identify where data are – so that organizations can
access patient data on a large scale in an
interoperable, secure and traceable form. Distributed
Ledger Technology could therefore establish low
cost, near-real time, rule-based methods for accessing
patient data that can be permissioned to selected
health organizations.
Before initiating Blockchain projects, hospital IT
leaders and decision makers, should consider whether
the technology is suitable to the hospital’s needs. Not
all problems require a DLT solution. That said, DLT
promises to be truly effective when multiple parties
generate transactions that change information in a
shared repository where intermediaries are inefficient
or not trusted as arbiters of truth - If this condition is
not met, a shared database may be a more appropriate
solution.
3 PROMISING USES OF
BLOCKCHAIN FOR THE
HEALTHCARE INDUSTRY
Figure 2 below, published by Chartier-Rueg and
Zweifel (2017) shows an illustration for promising
uses of Blockchain for the healthcare industry.
Figure 2: Promising uses of Blockchain in healthcare
(simplified from Chartier-Rueg and Zweifel, 2017).
Patient generated data, clinical data and health
record data are maintained in what is referred to as a
data lake, a repository that holds a vast amount of raw
data [BigData] in its native format until it is needed.
A data lake architecture usually incorporates search
and analytics techniques for decision-making,
reporting, legislation and census. Blockchain
implementations in this context can provide a
complete index history of the patient’s unique
identifier and an encrypted link to health records.
Each record is time stamped. Providers use health
applications to access data, patients may use mobile
devices to assign access permission to data. The
patient has control over the permissions on whom to
share data with and what portions of the data.
Blockchain network consensus enables the
automation of claim processing through predefined
Blockchain or Distributed Ledger Technology What Is in It for the Healthcare Industry?
279

inherent Blockchain features referred to as Smart
Contracts [ensuring tokenization of the data and
anonymization].
3.1 Likely and Unlikely Uses of
Blockchain in the Healthcare
Setting
The dynamic nature of health data and its
expansiveness prohibits replicating all health records
to every member in the chain, as is in the case of
traditional Blockchains, this would prove bandwidth
intensive, wasteful on resources and cause serious
data throughput concerns (Linn and Koo, 2016).
In the immediate, for healthcare to realize benefits
from distributed ledger technology, the distributed
ledger technology would need to function, primarily,
as an access-control manager for health records and
data (Linn and Koo, 2016). That said, likely uses for
distributed ledger technology in Healthcare aim at
improving medical record management, enhancing
insurance claim process and accelerating
clinical/biomedical research (Kuo et al, 2017).
Distributed ledger technology may also prove
effective as provider and patient directories, and care
plans, as historical ledgers of patient care data, in
support of pharmaceutical research and supply (Agbo
et al, 2019) chain and medical research and in
hospitals as back office component for admission,
discharge, and transfer systems (ADT/ATD) (Yip,
2016).
Likely Uses:
Improved medical record management
Historical ledgers of patient care data
Provider directory
Patient directory and care plans
Enhance insurance claim Processing
Accelerate pharma/ medical research
ADT back office component
Unlikely Uses:
Full featured Electronic health record systems
Global patient ID software
Public Health Data Access
3.2 Improve Medical Record
Management
Implementation of Blockchain technology may clear
obstacles to patients acquiring copies of their
healthcare records or transferring them to another
healthcare provider (Patel, 2018). Records signed by
the source and added to the Blockchain allow
legitimacy of records to be verified. Data are stored
in the private Blockchain cloud. Blockchain may
guarantee unalterable patient records, as encrypted
data in the Blockchain can only be read with the
patient’s private key (Kuo et al, 2017), which would
empower patients to control access to their sensitive
data (Esposito et al, 2018), which is Consistent with
the European General Data Protection Regulation
(GDPR) and other healthcare security regulation
(HIPAA).
3.3 Enhance Insurance Claim
Processing
Implementation of Blockchain technology may
provide the ability to maintain verifiable claim
transactions to support healthcare financing tasks and
facilitate real-time claim adjudication by replacing
the health plan intermediation with transparent
Blockchain technologies. Blockchain’ s transparency,
immutability and auditability of records stored can be
of great value to payers and insurance providers
(Boulos et al, 2018). In addition to increased security
of patient medical insurance information, payers,
private and government insurers, and individual
payers have the benefits of audits facilitation and
better fraud detection based on Blockchain
immutability (Crawford, 2017).
3.4 Accelerate Clinical/Biomedical
Research
Several firms contemplate accelerating secondary use
of clinical data (ie, clinical and biomedical studies
and research) using Blockchain technology (Roman-
Belmonte et al, 2018). The decentralized but traceable
functionality of Blockchain may imply that, each
institution can keep full control of their own
computational resources, while collaborating with
other institutions for data sharing and analysis
without ceding control (Benchoufi and Ravaud,
2017). Clinical trial would have a solid dataset,
reducing the risk of underreporting and exclusion
(Shae and Tsai, 2017). Furthermore, the immutability
property of Blockchain would be useful to certify the
integrity of data collected through Blockchain for
clinical study.
Personal patient-generated health data may now
become available to researchers. If anonymized and
then tracked in the research process with a timestamp,
this secondary source of data would engage millions
of individuals, healthcare providers, healthcare
KMIS 2019 - 11th International Conference on Knowledge Management and Information Systems
280
entities and medical researchers to share vast amounts
of genetic, diet, lifestyle, environmental and health
data with guaranteed security and privacy protection
(Boulos et al, 2018).
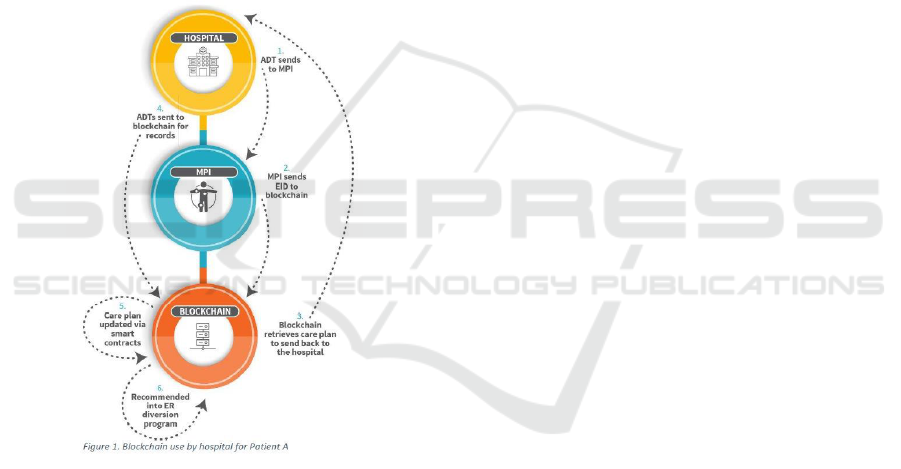
3.5 Illustrative Use Case: Back Office
Component for Admission,
Discharge, and Transfer Systems
(ADT).
Below is a description of how a hospital (or
healthcare organization) may likely adopt Blockchain
into its infrastructure (Yip, 2016).
Yip, 2016 proposed, as an illustration (Figure 3), a
use case of a network of public hospitals using
different and disconnected electronic medical record
systems (EMR).
Figure 3: Illustrative Use Case: Back Office Component for
Admission, Discharge, and Transfer Systems from (Yip,
2016, Fig 1).
The public hospitals, in lieu of normalizing their
systems, which can be a costly endeavour, with often
unsurmountable challenges, have implemented
Blockchain technology to identify patients going to
the hospital and clinics and determine whether were
part of the network. The hospital IT team has setup a
Blockchain with nodes at each of the hospitals and
clinics, plug-ins and interface engines were used to
connect the Blockchain with the different EMR
systems at each point of care setting. For our case, we
consider a patient who has moved from one city to
another and now seeks admission in the local clinic in
the public/national hospital network.
1. The patient’s ADT information is transmitted to
the MPI.
2. The MPI queries the Blockchain for patient
information. [If the MPI finds no record of the
patient, suggesting that the patient is a new
patient in this hospital. Noticing this, staff asks if
the patient wants to self-register and quickly
enrolls the patient through a web interface on the
intranet that connect to the Blockchain].
3. The patient directory information, with care plan
data, in the Blockchain, are returned to the ADT
system as a response.
4. ADT messages are sent during the admission
time and discharge time respectively to the
Blockchain.
5. After completion of the intervention, the patient
is now waiting to be discharged.
The clinical staff admit the patient for the
procedure or check-up. The Blockchain automatically
updates the patient records and care plan. [In this
hypothetical case, the Blockchain adds a
recommendation to put the patient into an ER
diversion program after noticing that the discharge
message was for a minor diagnoses and this has
marked three ER visits for minor diagnoses in the last
month].
Similarly, as reported by Yip, 2016, on the
payer’s side of the data interchange, each of the
hospitals and clinics used the interface engine to
connect their claims system and providers to the
Blockchain.
Payers were able to connect directly to the
national record for the patient and process insurance
claims and payments, while avoiding costly
processing workflows and delays in duplicate records
management.
Hospital management was able to make a
dashboard of cost vs. quality measures.
Patients received access to portals connected to
this Blockchain; they are able to view their medical
and financial records. The Blockchain was able to
provide information with a single source of truth.
4 CONCLUSION
Blockchain or distributed ledger technology (DLT)
has the potential to become the backbone for digital
health, incorporating data from patient-based
technologies and the electronic medical records to
provide a pool from which authorized users, such as
providers and patients, have access.
Blockchain or Distributed Ledger Technology What Is in It for the Healthcare Industry?
281

The paper has touched upon the initial research
question by demonstrating the potential of DLT
technology to address major concerns in data
ownership, access and use. All data are stored in a
decentralized manner, with no single entity storing or
having singular authority to access. This technology
has already made its impact in improved medical
record management, enhanced insurance claim
processes and accelerated clinical/biomedical
research. We conclude that DLT has a promising
proposition to define data ownership and access to
sensitive data; however, the jury can still be out on
controlling use.
Implementation of Blockchain for healthcare are
at their burgeoning stage: HealthChain, for instance,
is an EMR application that uses smart contracts, or
chain codes that are developed on IBM Blockchain’s
Hyperledger Fabric and deployed on Bluemix
(Ahram et al, 2017), to control authorizations and
access privileges.
4.1 A Winning Proposition
The growth of the distributed ledger technology and
its premise to fuel incremental innovations will
eventually become indispensable for proper data
stewardship for the proper use of patients, providers,
payers, pharma, medical researchers and public
health analysts while respecting the privacy,
confidentiality and integrity of the data asset.
For healthcare organizations that have decided to
initiate Blockchain projects, the next step is to design
the use cases. In this paper, we presented one
illustrative use case on the effectiveness of
Blockchain implementations in enhancing the
security, ensuring integrity of the system and
maintaining the originality of the data.
For MedTech, the use of embedded blockchain-
like technology can provide a real-time mechanism to
track data ownership, collection, usage and when it is
used and for what purposes. A value added
proposition for medical technology companies who
are looking to participate in the Internet of Medical
things ecosystem
1
. These companies can now
leverage the added privacy, security and data
protection, by design, which would improve enhance
practitioners’ and patients’ access to trusted
information, improve diagnosis, care and treatment,
thus advancing the vision of medicine that is
1
https://www2.deloitte.com/content/dam/Deloitte/global/
Documents/Life-Sciences-Health-Care/gx-lshc-medtech-
iomt-brochure.pdf
predictive, preventive, personalized and participatory
(‘P4’) (Hood et al, 2012).
However, essentially, it seems like, until more
rigor is placed on managing public keys and
protecting against data loss due to hacks or otherwise,
issues related to transparency and confidentiality may
prohibit the use of DLT for public healthcare data.
Whereas, private Blockchain implementations, with
some level of control over access, would likely be the
norm in healthcare settings (Dagher et al, 2018).
4.2 A Position Paper
Blockchain is among the top health technologies
touted to streamline healthcare operations, lower
costs and enhance quality of care. Artificial
intelligence (AI), voice search, chat-bots and virtual
reality (VR) are also among the list most promising
health technologies in 2019
2
.
Our position paper is an attempt to socialize the
enigmatic distributed ledger technology and highlight
its potential value in the healthcare setting. We invite
researchers and practitioners to use to start the
practical discussion of the technology. At this stage,
a set of questions that remain without answer:
How far could public Blockchains be useful at a
larger scale for public healthcare?
What will the advantages be in public health and
epidemic management?
Can DLT be useful at the service of the consumer
through integration with Consumer Heath
Informatics?
How resilient can this technology be in correcting
user errors introduced by practitioners?
How scalable could DLT become in order to
integrated data and analytics from the ever-increasing
integration of medical devices; scaling to accept
internet of things (IoT) big data storage levels?
Can clinical researchers and practitioners obtain
authorized access to clinical trials before a major drug
announcement? or, to report certain reactions by their
patients, then have that information be joined with
other decision support criteria for drug interaction
management? This would inevitably be a step in the
right direction as medical trials expand into real time
field data capture. Etc.
2
https://healthcareweekly.com/health-technologies/
KMIS 2019 - 11th International Conference on Knowledge Management and Information Systems
282

REFERENCES
Agbo, C. C., Mahmoud, Q. H., Eklund, J. M. 2019, June.
Blockchain Technology in Healthcare: A Systematic
Review. In Healthcare (Vol. 7, No. 2, p. 56).
Multidisciplinary Digital Publishing Institute.
Ahram, T.; Sargolzaei, A.; Sargolzaei, S.; Daniels, J.;
Amaba, B., 2017. Blockchain Technology Innovations.
In Proceedings of the 2017 IEEE Technology &
Engineering Management Conference (TEMSCON),
Santa Clara, CA, USA, 8–10 June 2017; pp. 137–141
Angeletti F, Chatzigiannakis I, Vitaletti A. 2017. The role
of blockchain and IoT in recruiting participants for
digital clinical trials. 25th international conference on
software, telecommunications and computer networks
(SoftCOM); 2017. p. 1–5.
Benchoufi M, Porcher R, Ravaud P. 2018. Blockchain
protocols in clinical trials: Transparency and
traceability of consent. F1000 Research 2018; 6:66.
Benchoufi, M.; Ravaud, P. 2017 Blockchain Technology
for Improving Clinical Research Quality. Trials 2017,
18, 335
Boulos, M.N.K.; Wilson, J.T.; Clauson, K.A. 2018
Geospatial blockchain: Promises, challenges, and
scenarios in health and healthcare. Int. J. Health Geogr.
2018, 17, 25.
Brodersen, C., Kalis, B., Leong, C., Mitchell, E., Pupo, E.,
Truscott, A., Accenture, L. 2016. Blockchain: Securing
a New Health Interoperability Experience. Accenture
LLP.
Brogan J, Baskaran I, Ramachandran N. 2018.
Authenticating health activity data using distributed
ledger technologies. Comput Struct Biotechnol J 2018;
16:257–66.
Chartier-Rueg, T. C., Zweifel, T. D. 2017. Blockchain,
Leadership and Management: Business as Usual or
Radical Disruption. Eureka: Social and Humanities,
(4), 76-110.
Crawford, M. 2017. The insurance implications of
blockchain. Risk Management, 64(2), 24.
Dagher, G.G.; Mohler, J.; Milojkovic, M.; Marella, P.B.;
Marella, B., 2018. Ancile: Privacy-Preserving
Framework for Access Control and Interoperability of
Electronic Health Records Using Blockchain
Technology. Sustain. Cities Soc. 2018, 39, 283–297.
Drosatos, G., & Kaldoudi, E. (2019). Blockchain
applications in the biomedical domain: a scoping
review. Computational and structural biotechnology
journal.
Esposito, C., De Santis, A., Tortora, G., Chang, H., & Choo,
K. K. R., 2018. Blockchain: A panacea for healthcare
cloud-based data security and privacy? IEEE Cloud
Computing, 5(1), 31-37.
Gcoin blockchain. Int J Environ Res Public Health 2018;
15(6):1055.
Glaser, F. 2017. Pervasive decentralisation of digital
infrastructures: a framework for blockchain enabled
system and use case analysis. Proceedings of the 50th
Hawaii International Conference on System Sciences |
2017
Hood, L., Balling, R., & Auffray, C. (2012).
Revolutionizing medicine in the 21st century through
systems approaches. Biotechnology journal, 7(8), 992-
1001.
Iansiti, M., & Lakhani, K. R. 2017. The truth about
blockchain. Harvard Business Review, 95(1), 118-127.
Ichikawa D, Kashiyama M, Ueno T. Tamper-resistant
mobile health using blockchain technology. JMIR
Mhealth Uhealth 2017;5(7):e111.
Jørgensen, R., Scarso, E., Edwards, K., Ipsen, C. 2019.
Communities of practice in healthcare: A framework
for managing knowledge sharing in operations.
Knowledge and Process Management. 2019
Jurisica, I., Mylopoulos, J., Yu, E. 2004. Ontologies for
knowledge management: an information systems
perspective. Knowledge and Information systems, 6(4),
380-401.
Kleinaki A-S, Mytis-Gkometh P, Drosatos G, Efraimidis
PS, Kaldoudi E. 2018 A blockchain based notarization
service for biomedical knowledge retrieval. Comput
Struct Biotechnol J 2018; 16:288–97.
Kuo, T. T., Kim, H. E., Ohno-Machado, L. 2017.
Blockchain distributed ledger technologies for
biomedical and health care applications. JAMIA, 24(6),
1211-1220.
Le Nguyen, T. 2018, August. Blockchain in Healthcare: A
New Technology Benefit for Both Patients and
Doctors. In 2018 Portland International Conference on
Management of Engineering and Technology
(PICMET) (pp. 1-6). IEEE.
Li, Z., Wang, W. M., Liu, G., Liu, L., He, J., Huang, G. Q.
2018. Toward open manufacturing: A cross-enterprises
knowledge and services exchange framework based on
blockchain and edge computing. Industrial
Management & Data Systems, 118(1), 303-320.
Linn, L. A., & Koo, M. B. 2016. Blockchain for health data
and its potential use in health it and health care related
research. In ONC/NIST Use of Blockchain for
Healthcare and Research Workshop. Gaithersburg,
Maryland, United States: ONC/NIST.
Nugent T, Upton D, Cimpoesu M. 2016 Improving data
transparency in clinical trials using blockchain smart
contracts. F1000Research 2016; 5:2541.
Patel, V. A, 2018. Framework for Secure and Decentralized
Sharing of Medical Imaging Data via Blockchain
Consensus. Health Inform. J. 2018.
Rakic, D. (2018, March). Blockchain Technology in
Healthcare. In ICT4AWE (pp. 13-20).
RJ Krawiec, et al, 2016. Blockchain: Opportunities for
Health Care. CP Transaction. Deloitte.
Roman-Belmonte, J.M.; De la Corte-Rodriguez, H.;
Rodriguez-Merchan, E.C.C.; la Corte-Rodriguez, H.;
Carlos Rodriguez-Merchan, E. 2018 How Blockchain
Technology Can Change Medicine. Postgrad. Med.
2018, 130, 420–427
Shae, Z.; Tsai, J.J. On the Design of a Blockchain Platform
for Clinical Trial and Precision Medicine. In
Proceedings of the 2017 IEEE 37th International
Conference on Distributed Computing Systems
Blockchain or Distributed Ledger Technology What Is in It for the Healthcare Industry?
283

(ICDCS), Atlanta, GA, USA, 5–8 June 2017; pp. 1972–
1980.
Taylor, P. J., Dargahi, T., Dehghantanha, A., Parizi, R. M.,
& Choo, K. K. R. 2019. A systematic literature review
of blockchain cyber security. Digital Communications
and Networks.
Tseng J-H, Liao Y-C, Chong B, Liao S-W. 2018.
Governance on the drug supply chain via
Wang, Y., Kung, L., Wang, W. Y. C., Cegielski, C. G.
2018. An integrated big data analytics-enabled
transformation model: Application to health care.
Information & Management, 55(1), 64-79.
Yip, K, 2016. Blockchain and Alternative Payment Models.
A Look at where Blockchain can be Implemented to
Further APM Goals. healthit.gov.
Zhou L, Wang L, Sun Y. MIStore: a blockchain-based
medical insurance storage system. J Med Syst 2018;
42(8):149.
KMIS 2019 - 11th International Conference on Knowledge Management and Information Systems
284
