
HEALTH CARE PROCESS BASED ON THE ABC MODEL
THROUGH A META-STRUCTURED INFORMATION SYSTEM
Christine Verdier
LIRIS, INSA of Lyon, bat. B. Pascal, 7 av. J. Capelle, 69621 Villeurbanne Cedex
Gérard Cluze
IAE, University Lyon 3, 15 quai Claude Bernard, 69007 Lyon
Keywords: Medical information system, UML packages, ABC method, care process
Abstract: We propose in this article to define a system which generates a generic care process based on the ABC
method. For this purpose, we adapt dynamically the medical information system with UML packages in
order to generate some semantic and syntactic links between the different packages that represent the
“business objects” of a hospital. These packages contain all the information related to a specific problem for
all the patients. So we are able to extract the particular data concerning a criteria (diagnosis, IP number, etc.)
and a patient and, in that manner, to re-build the care process. The ABC method gives the skeleton of the
care process and allows the definition of costs on a particular care process (e.g. the care process of the
patient “John” concerning the disease “kidney failure” in the hospital H).
1 INTRODUCTION
A serious problem is always noticed in hospitals; the
great difficulty to coordinate medical information
systems and management ones. So the financial
evaluation of a care process is really difficult to do.
It implies the extraction of the good data in the
different information systems, the ability to re-build
the patient care process and to evaluate the cost of
this process. The data used to create the care process
exists but its semantic and syntactic concatenations
are very hard to make. So to couple an information
system with a method which is able to identify the
costs objects can be interesting to 1) build a generic
care process, 2) define a particular care process and
3) propose a result-cost for this care process. The
Activity-Based Costing method allows us to have a
better understanding of the organisation
management
We propose in a first paragraph to briefly
co
nsider the related works. We will continue with
our approach and finish with an experimental study.
2 RELATED WORKS
2.1 ABC in medical areas
The ABC method was recently developed, in France
(less than ten years old). Generally, we attribute it to
(Kaplan, 1984). The authors initiated the criticism of
traditional cost accountancy and proposed the ABC
method. This method has been developed by several
authors (Cooper, 1990), (Turney, 1991) and
(Brimson, 1991).
All these authors share the same observations:
the structures
of the organisations transform
themselves, the concept of the product is
significantly modified, the logics of management are
no longer the same. They concluded that the system
of costing is no longer relevant.
ABC appears to be more coherent. It is based on
a detailed analysis of processes and perm
its a
diagnosis of quality, delay and cost of the different
activities and finally facilitates the identification of
factors which hinder the performance of activities
and therefore of the organisation.
The inherent logic of ABC can also be presented
as fo
llows: Activities identification, activities
149
Verdier C. and Cluze G. (2004).
HEALTH CARE PROCESS BASED ON THE ABC MODEL THROUGH A META-STRUCTURED INFORMATION SYSTEM.
In Proceedings of the Sixth International Conference on Enterprise Information Systems, pages 149-154
DOI: 10.5220/0002622301490154
Copyright
c
SciTePress

analysis, process construction, cost identification,
activities cost description, costs calculation.
This technique is rarely used in the service sector
and practically never introduced into health care
centres (the rare French attempts to introduce it
concerned the industrial activities of hospitals). This
confers an experimental character on our work.
ABC presents besides, characteristics which, for
us, seem particularly well adapted to the specificity
of the production of health care. And thus the
absence of a production function, the difficulty
seizing the nature of the product, the confusion
between the customer and the patient, the non
standardisation of the processes of health care, the
development of care networks, the environmental
complexity, etc. are features which seem, from our
point of view, linked with the concepts of transverse
process and flexibility which are the bases of ABC.
Added to that, the ABC method can be used both
for the health costs management in hospitals and to
help find a financial solution when the resources
decrease. The first experience in hospital is quite
new (Baker, 1998). It was followed by several ABC
applications in different countries: Germany, Great
Britain, Spain and Australia (Abernethy, 1995). In
France, despite of an increasing interest in ABC
applications in hospitals, there is no real application.
In Strasbourg (Biron, 1998])an ABC experiment was
created in hospital but only concerning the medico-
technique activities.
2.2 Treatment chain
The enormous possibilities within diagnosis and
therapy lead to an extreme specialization of medical
tasks. So, it becomes difficult to identify the
treatment chain within a same medical organization.
The problem is increased when we consider several
health places; in that case, the treatment chain
evaluation requires a coordination of the different
information systems, the management of missing
data, the interoperability of the systems, etc.
But, the requirements of the justified medical
costs lead the researchers and the practitioners to
discard a unit-centered approach (to care and to
evaluate) in aid of treatment chain value.
The successful projects match static and dynamic
models (especially UML tools) with activity
diagrams or workflow procedures. Two main
difficulties have to be affronted beyond: the accurate
aggregation of the patient medical data and the
dynamic links between these data.
In (Ammenwerth, 2000), the authors consider 5
views of the treatment process (roles and activity
profiles, documentation, business processes,
communication and cooperation). They mix the
different tools related to every view and propose a
solution to catch the treatment process.
In (Dadam, 2000), the authors develop a
workflow tool called Adept which considers in
conjunction all the aspects of the workflow process :
robustness, security and flexibility.
In (Yousfi, 1996) and (Bricon-Souf, 1998), the
authors develop a computer-based system supporting
cooperative planning in critical care environment
called Placo. They particularly develop structured
and unstructured messages that are generated firstly
by the system and secondly by the users.
Some researches work upstream in order to offer
gathered data, explored in syntactic and semantic
ways. We can cite works concerning visual approach
for browsing huge amount of data (Tanin, 2000).
Some other researches concern the design of specific
interface in order to display all the dispatched data
(wherever their health places creation). We can cite
for example (Ouziri, 2002).
These approaches essentially deal with a real and
complex problem that is the capture and retrieval of
the right information in the right place in order to
improve the medical follow-up of the patient.
3 OUR APPROACH
Our approach is a bit different. We propose a system
that couple together evaluation techniques (ABC
method) and information systems.
The main question is how to reconcile the
necessity to have a justified medical health cost of
patient cares and the difficulty to semantically and
syntactically gather distributed medical data. Our
system proposes to create a generic care process that
can be instantiated according to every patient or
every criteria from the existing information systems.
Then we build an ABC system. The system model is
a necessary stage, the theory is useless in practise
without the system. The ABC system permits the
application of the model into the health care sector.
The system is enriched by successive experiments of
the ABC, the progress of the research and our
experiment in practice. After the organisation
analysis, we conceived the idea of the « flow of
patients » and the cost of this flow. We linked the
concept of the « flow of patients » with the concept
of procedures : we think that this idea is completely
original in the domain of management and
economics in France. To create that system, we
propose three steps.
Three main parts can be identified :
ICEIS 2004 - DATABASES AND INFORMATION SYSTEMS INTEGRATION
150
The meta-structuring of the medical business-
object
The definition of the generic care process
The instantiation of a patient care process with a
concrete example.
3.1 Meta-structuring of the medical
business-objects
To represent the whole activities of a hospital, we
use the UML package notation to factorize
homogeneous parts of models (that is to say
elements of model getting the same « semantics »
according to one criterion). A package can be
defined as the following: a package is a grouping of
model elements or packages. Packages themselves
may be nested within other packages. All kinds of
UML model elements and diagrams can be
organized into packages. Packages own model
elements and model fragments and are the basis for
configuration control, storage and access control
(UML, 1997). That definition supposes that (1) a
package is homogeneous according to a criterion, (2)
that it can be derived according to the goals and
tools of the organization and (3) that the links
structuring itself can be defined as needed.
3.1.1 Description of the business objects
package
The packages in our approach are declined
according to the criterion business-objects that are,
specifically in our study, the only way to catch all
the « businesses » of a hospital.
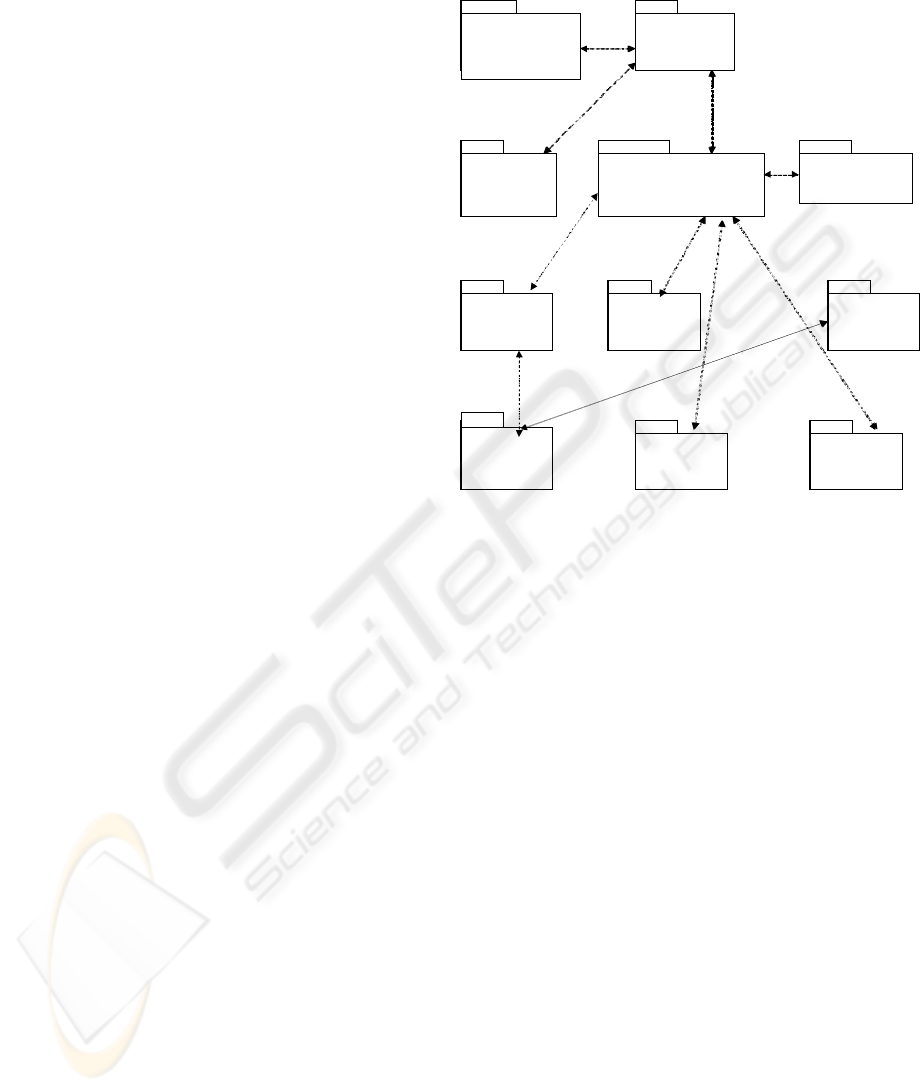
The different « business-objects » of the hospital
are the following : to welcome (the patient in the
hospital or in a particular service area), to diagnose
(diagnostic procedures that help to know the
patient's disease), to care (therapeutic procedure that
helps to increase the health of the patient), to operate
on (techniques and resources used to operate on a
patient), to control (medical control procedures), to
train (traditional training or continuing education), to
feed (the patient during his stay), to clean (cleaning
of the surgical/medical instruments and premises), to
transport (outside or inside the hospital), to manage
(resources allocation to succeed in the care process),
and to accomodate (beds management). The
different packages corresponding to each business-
object of the hospital are described in figure 1.
NB : The packages contain some activities that
can be divided into tasks.
3.1.2 Contents of the packages
Welcome
+ Patient Identifying Form
+ Administrative staff
+ Medical staff
Diagnose
+ Medical record
+ Medical history
+ Investigation examination
+ Medical staff
train
+ Type of training
(medical, emergency,
investigation equipment)
+ Staff
Control
+ Medical supervision
+ Medico-economics
indicators
operate on
+Preoperative examination
+ Technical tools
Put up
+ Type of rooms
+ Beds equipment
Clean
+ Premises
+ Medical instruments
Manage
+ Financial charts
+ Material resources
+ Non-material resources
Feed
+ Type of food
+ Food time
+ Type of diet
transport
+ Type of transport
+ Destination transport
Welcome/
Outcome
+ Patient Identifying Form
+ Administrative staff
+ Medical staff
Diagnose
+ Medical record
+ Medical history
+ Investigation examination
+ Medical staff
train
+ Type of training
(medical, emergency,
investigation equipment)
+ Staff
Control
+ Medical supervision
+ Medico-economics
indicators
Care/ Relationship
+ Drugs
+ Non-drug therapeutic care
+ Type of cares
(curative/preventive/palliative)
operate on
+Preoperative examination
+ Technical tools
A
ccomodate
+ Type of rooms
+ Beds equipment
Clean
+ Premises
+ Medical instruments
General
management
+ Financial charts
+ Material resources
+ Non-material resources
Feed
+ Type of food
+ Food time
+ Type of diet
transport
+ Type of transport
+ Destination transport
Fi
g
ure 1: Descri
p
tion of the hos
p
ital activities with UML-
p
acka
g
es
Every package is independent from the others. It
implies that the information system can focus on one
part or another. The content of a package can be
declined as wished. More precisely, all the types of
models can be described in every package. In order
to design the static part of the information system,
we can use a class diagram. Every part of a
conceptual model (grouped into a package)
corresponds to a distinct part of the activities but it
can be linked to the rest of the model if needed. For
instance, we can show the description of the class
diagram of two packages: « welcome » and
« diagnose » (figure 2).
The class diagram of the package « welcome »
contains three classes: the patient identifying form,
the hospital staff and the administrative staff. The
class administrative staff inherits (like the class
medical staff in the package « diagnose ») from the
class « hospital staff ». The only difference between
them is the nature of the occupation, so it is better to
factorize properties and methods in the class
« hospital staff ».
HEALTH CARE PROCESS BASED ON THE ABC MODEL THROUGH A META-STRUCTURED INFORMATION
SYSTEM
151
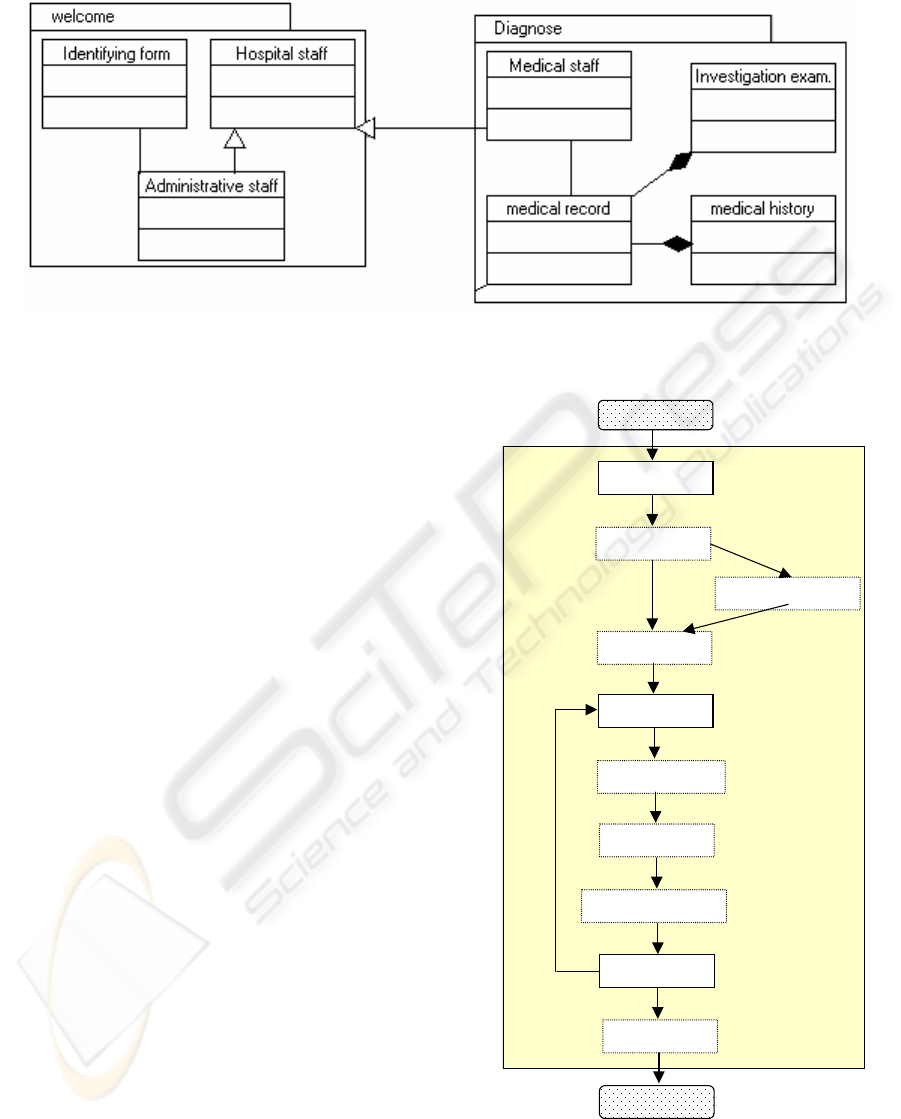
Figure 2: Class diagram in two packages
In the other package, four classes are present: the
medical staff linked throughout the package to the
class hospital staff, the medical record which is
composed of the class Investigation examination and
Medical history. Every package has to be filled like
the two others and the association links between
them must be created. We precise that the
description of the class diagram in the different
packages consists in the static design of the whole
information system. One of the advantage is that the
design of the IS is totally modular and every part can
be created after each other without disrupting the
existing running. Another advantage consists in the
ability for the organization to reuse the part of
existing applications with the restriction of the
linkage between them and the IS.
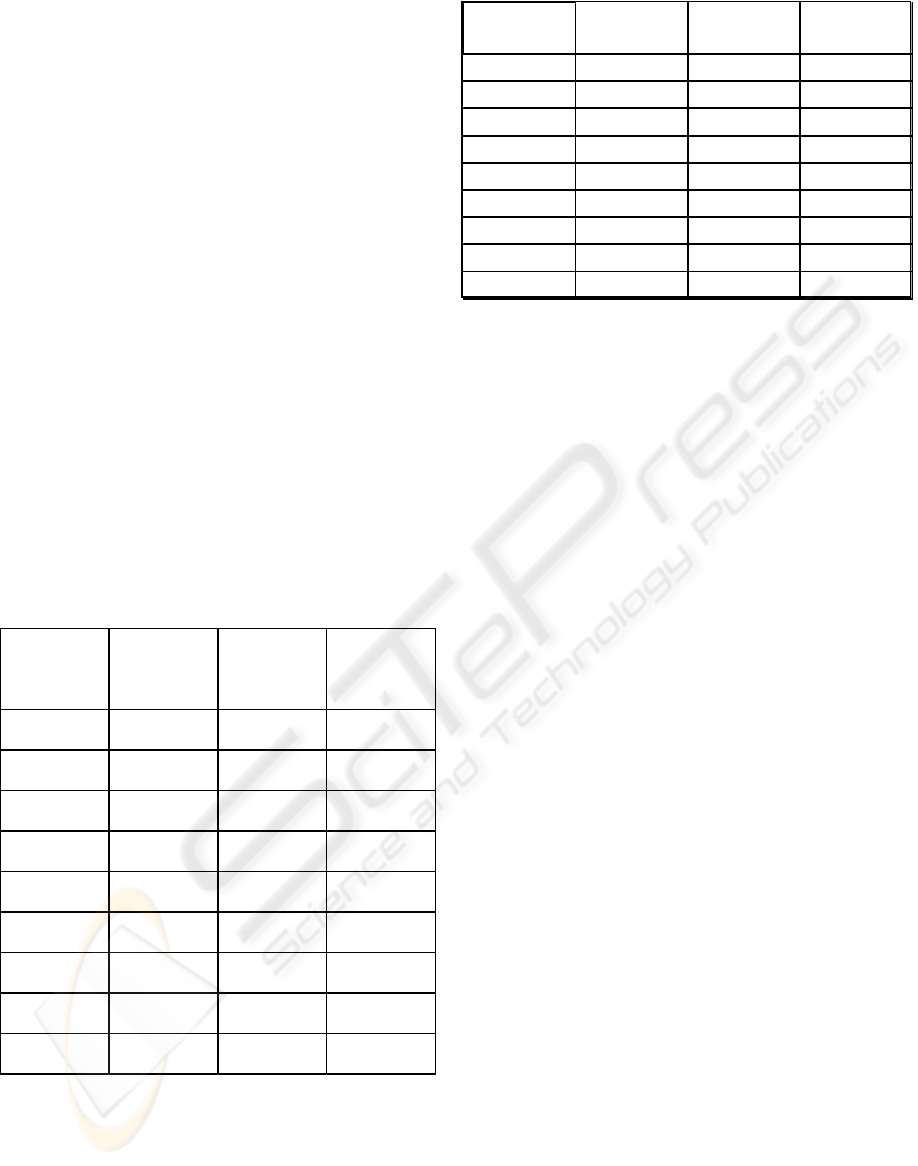
PATIENT
Welcome
Consultation
Investigation exam
Type of Care
Feed
Following Care
Leisure
Medical supervision
Accomodate
Consultation
PATIENT
3.2 The generic care process
The package representation of the medical
information system makes easier the extraction of
the generic care process.
Every activity is linked to the other by a
syntactic link which role is to coordinate the data
through a criteria: the IPP number, the disease, etc.
To realise our objective, we cross examine the
ABC accountancy and the “package” information
system. Resources are attributed directly to business-
objects of the organisation. The activities are
regrouped into macro-activities which are shared
between cost items according to cost drivers. Doing
that, we notice that analytical accountancy centred
on activities induces a different view of information
systems.
Figure 3: Process Patient-Medicine Trajectory
This new approach requires to have a particular
information system, able to supply a multi-views of
the whole hospitals information systems.
ICEIS 2004 - DATABASES AND INFORMATION SYSTEMS INTEGRATION
152
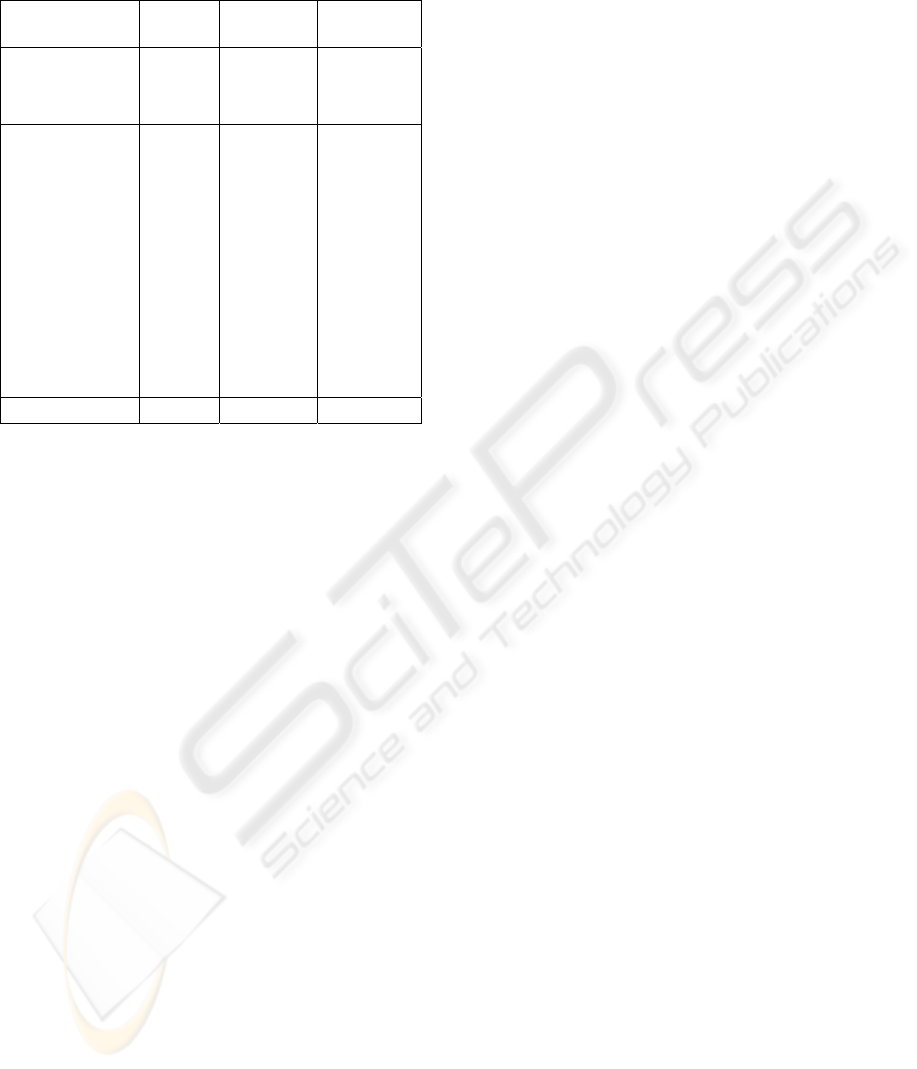
Global cost
(€)
Nb of drivers Unit cost (€)
MA
1
17486 470 37,2
MA
2
31434,9 470 66,88
MA
3
133072,7 5394 24,67
MA
4
83069,4 5394 15,4
MA
5
17455,4 470 37,14
MA
6
16403,5 5394 3,04
MA
7
114428,2 5394 21,2
MA
8
209861,3 5130 40,9
MA
9
16601,6 470 35,32
4 A FIRST EXPERIMENTAL
STUDY
4.1 Generic care process design
The experimentation lead in the Château de
Vernhes, a French private hospital, specialized in
obesity care. Like most hospitals (Saulquin 1995],
the accountancy is quite restricted and does not
permit to obtain a real image of the care process
cost. The experimentation was realized in a medical
unit, the medicine department. This department
contains 15 beds: this particularity is interesting to
get a better image of the cost reality. The process
used is the process medicine and the care process is
called patient-medicine trajectory.
Figure 5: Cost Drivers
The medical business-objects defined in the
packages represent the basis of the activities defined.
The activities can be retrieve from the packages,
some others can be added.
The care process is represented by the figure 3.
The activities, tasks and business-objects are
retrieved from the packages of the information
system. We said that the packages can be filled in as
wished. The parts (elements of models) of the
existing information systems are put together to be
used in a strategic way. In our application, some
activities or business-objects are used to define the
process described above. The dotted rectangle
concern the activities and the others, the business-
objects. Some activities are still in the package
model. Some other are not considered. The selection
of the activities concerning a generic process
represents the first step of the update of the dynamic
package creation. The modelling elements contained
in the packages necessary to catch the generic
process are gathered and processed as needed before
the step of process creation.
4.2 Representation of the activities
drivers
To calculate the costs, we use the following steps :
- step 1 : research the procedures and activities
(identification of the key factors, the process, the
activities, the cost drivers).
Main
activities
Re f e r e nce
package
activities
drivers
number of
activities
drivers in a
year
MA 1: Welcome Welcome
Number of
entrance
470
MA 2:
Expertise
Diagnose
Number of
patients
470
MA 3: Car e Ca r e
Number of
days
5394
MA 4:Catering Feed
Number of
days
5394
MA 5:
Relationship
Car e
Number of
patients
470
MA 6:
Accomodate
Put up
Number of
nights
5394
MA 7:
Management
General
management
Number of
days
5394
MA 8: Building
management
General
management
m² 5130
MA 9: Leaving Welcome
Number of
leavings
470
- step 2: linking costs to activities
The activities drivers are used to find a link
between ressources consumption and the real
production. The activities drivers have been defined
for each activity and for a reference year.
The activities drivers are represented in the
figure 4.
Every resource has been linked to the main
activities and permit to determine the cost drivers
(the costs of the activities drivers). The cost drivers
are represented in the figure 5.
Then, the resources are allocated in proportion of
the consumption.
The final cost of the process patient-medicine
trajectory is obtained by adding the resources
directly attributed to the cost object to the indirect
resources consumed by the activities used by the
cost object (here, the object cost is a particular
patient).
Figure 4: Activities Drivers
For a particular patient, the ABC cost is shown in
the figure 6. The patient stayed 7 days. The
additional costs were : 155,49 € for external lab
examinations and 148 € for blood products.
The global cost is so identified according to the
global care process (see figure 6) and is really equal
HEALTH CARE PROCESS BASED ON THE ABC MODEL THROUGH A META-STRUCTURED INFORMATION
SYSTEM
153
to the real costs engaged for the treatment of this
patient.
5 CONCLUSION
We try to show in this paper that we can couple the
economic and medical information in order to
measure a real cost of the care process. For that, we
build a re-organisation of the different information
systems with the packages and we adapt the ABC
method to generate the generic care process and
calculate the costs induced by a specific patient care
process.
REFERENCES
Abernethy, M.A., Stoelwinder, J.U., 1995. The role of
professional control in the management of complex
organisations, Accounting Organisations and Society,
vol 20, n°1, 1995:1-16
Ammenwerth, E. et ali, 2000. Analysis and modeling of
the treatment process characterizing the cooperation
within multi-professional treatment teams, MIE 2000,
IOS Press, A. Hasman et al (eds), 2000:57-61
Baker, J.J., 1998. Activity-based costing and activity-
based management for health care, Aspen Publishers,
Maryland, USA, 1998
Biron, N. et ali, 1998. L’utilisation de la méthode ABC
pour les activités de support médico-technique et
logistique, Gestion hospitalière, juin-juil 1998:425-29
Bricon-Souf, N., Renard J.M., Beuscart, R., 1998.
Dynamic workflow model for complex activity in
intensive care unit. Medinfo 1998, Seoul, Korea,
1998 :227-31
Resources
consumed
Quantity Unit cost (€)
Total
amount (€)
D
irect expenditure
Blood products
148
Lab exam
155,49
I
ndirect
expenditure
MA 1
1
37,2
37,2
MA 2
1
66,88
66,88
MA 3
7
24,67
172,69
MA 4
7
15,4
107,8
MA 5
7
37,14
259,98
MA 6
7
3,04
21,28
MA 7
7
21,2
148,4
MA 8
0,82
40,9
3,53
MA 9
1
35,32
35,32
Total amount
1156,57
Brimson, J.A., 1991. Activity Accounting: an activity-
based costing, Wiley & Sons, New York, 1991
Cooper, R., 1990 Cost classification in unit-based and
activity-based manufacturing cost systems. Journal of
cost management for the manufacturing industry, Fall
1990:4-14
Dadam, P., Reichert, M., 2000. Towards a new dimension
in clinical information processing. MIE 2000, IOS
Press, A. Hasman et al (eds), 2000:295-301
Kaplan, R.S., 1984. The Evolution of Management
Accounting. The Accounting Review, vol LIX, n°3,
1984.
Ouziri, M., Verdier, C., Flory, A., 2002. Utilisation des
TopicMaps pour l’interrogation et la visualisation du
dossier médical distribué. DVP 2002, Brest, juillet
2002.
Saulquin, J.Y., 1995. Le contrôle de gestion, une greffe
difficile des outils dans les cliniques privées. Revue du
CEREGE, IAE, Poitiers, n° 149, septembre 1995, pp.
1-21.
Figure 6 : Global costs
Tanin, E. et ali, 2000. Facilitating network data
exploration with query previews: a study of user
performance and preference. Behaviour and
Information Technology, vol. 19, n°6 (2000), pp 393-
403
Turney, P.B.B., 1991. Common cents, the ABC
performance breakthrough. Cost technology,
Hillsboro-Portland, Oregon, 1991
UML, 1997. UML notation guide, version 1.1., sept 1997,
Rational software corporation, http://rational.com/uml
Yousfi, F., Beuscart, R., Souf, N., 1996. A asynchronous
cooperative model for coordinating medical unit
activities. MIE 96, IOS Press, J. Brender et al (eds),
1996:858-62
ICEIS 2004 - DATABASES AND INFORMATION SYSTEMS INTEGRATION
154
