
SECURING A WEB-BASED EPR
An approach to secure a centralized EPR within a hospital
Ferreira A, Correia R, Costa-Pereira A
Department of Biostatistics and Medical Informatics, Faculty of Medicine, University of Porto
Al. Prof. Hernâni Monteiro 4200-319 Porto, Portugal
Keywords: Electronic Patient Record; Information Security
; Standards & Internet Technology;
Abstract: The introduction of new technologies such as the EPR stresses the importance of healthcare information
security
. The Biostatistics and Medical Informatics Department of Porto’s Faculty of Medicine is
developing a centralized Electronic Patient Record at Hospital S. João, in Portugal, the HSJ.ICU. The main
objective is to electronically integrate heterogeneous departmental information in a secure way, using
Internet technology. The methodology used takes into consideration user-driven security issues in terms of
confidentiality, integrity and availability of information. This was achieved using CEN/TC251
prestandards, Internet security protocols (e.g. TLS) and digital signature protocols. Having in mind the CIA
(Confidentiality, Integrity and Availability) structure helps organizing and in a way, separating concepts
that can be assessed in a more direct and efficient way. Security issues are already rooted and constitute a
good basis for any enhancements that will be made in the future.
1 INTRODUCTION
The Electronic Patient Record (EPR) is a
fundamental information system for healthcare
organizations, enabling a single point of entry and
access to patient-related, administrative and research
information (Shortliffe, 1999). It provides for easier
and faster access to patient information. Further, it
helps for the creation of a more complete and better
quality record (Hassey, 2001)(Stausberg, 2003).
The introduction of new technologies such is the
EPR also stresses
for the importance of healthcare
information security. New challenges (to face old
problems) need to be dealt with new measures, and
these must be evaluated for its effectiveness.
Several pressures during the development of IT
sol
utions often imply that security is an afterthought.
It is quite often overlooked so that the system can be
easier to work with (Godoy, 2002). This and other
factors make the integration of the EPR into medical
processes within large environments, such as
hospitals, very difficult
(Benson, 2002).
The Biostatistics and Medical Informatics
Depart
ment of Porto’s Faculty of Medicine has
started to develop and implement the HSJ.ICU
project, a centralized Electronic Patient Record
(EPR) at Hospital S. João, the second biggest
hospital in Portugal with about 1.350 beds. The main
objective is to electronically integrate heterogeneous
departmental information in a secure way, using
Internet technology. Many people and services, as
well as a complex infrastructure, are involved in this
process (Kurtz, 2003). There is the need to provide
for confidentiality (avoiding unauthorized access
(Salazar-Kish, 2000)), integrity (information needs
to be accurate, valid and complete (Bemmel, 1997))
and availability (Bemmel, 1997) of patient’s
information. That is why learning from previous
experiences, specifically in Portugal and in the same
hospital, can be very important and rewarding whilst
saving time and avoiding the most common mistakes
(Ferreira, 2002). In summary, information security is
fundamental for the success of the EPR.
This paper describes the methodology to assess
system
infrastructure, healthcare professionals’
attitudes and patient’s information workflow
affecting information security. It also presents some
results, analysis and procedures to be implemented
so that this project is successful.
2 METHODS
Prior to any action, it is important to assess the
infrastructure where the system HSJ.ICU is going to
54
A F., R C. and A C. (2004).
SECURING A WEB-BASED EPR - An approach to secure a centralized EPR within a hospital.
In Proceedings of the Sixth International Conference on Enterprise Information Systems, pages 54-59
DOI: 10.5220/0002655000540059
Copyright
c
SciTePress

Figure 1: HSJ.ICU Generic Infrastructure
be integrated. Figure 1 presents a generic
architecture of the EPR system to be implemented.
It shows the heterogeneity of the infrastructure that
supports the healthcare information flow within the
hospital. The departmental systems presented above
have different infrastructures and types of workflow.
In some of these departments, patient records are still
paper-based while others have a mixture of
procedures and technology that make the integration
of a common platform not straightforward.
Another important step is to assess what are the
main concerns of the healthcare professionals
involved. This is done with several meetings with
each department’s staff. Other contacts made
afterwards during the development of the project are
also taken into consideration.
In summary, security services will be
implemented so that information security (mainly
user-driven) can be effectively achieved whilst still
allowing for the proper use of the system. It follows
the description of the security services and problems
that need to be taken into consideration whilst
developing this project.
2.1 Confidentiality
In terms of user-driven security issues,
confidentiality can be provided by controlling access
to the system and make sure that only authorized
users access information. When this rule is breached,
unauthorized users’ actions along with their
identification should be recorded for further
responsibility and subsequent legal actions.
Also, this project involves the integration of
several physical places making it crucial that all
communication channels are protected. This will
provide for the secure information flow. Any breach
that may occur (e.g. eavesdropping) should not allow
for unauthorized access to sensitive information.
The following two sections will explain the
methodology used for both these issues (access
control and secure communications) in more detail.
2.1.1 Access Control
Controlling the access to sensitive information is
fundamental; moreover when that information relates
to healthcare patient sensitive information. The
heterogeneous environment, such is the healthcare
environment where different people and services are
required to interact, make it more difficult to control
and provide for its proper use. Nevertheless, there
are ways to provide for proper access control.
The main step is to make sure every user can be
uniquely identified so that his actions can be easily
traced. Usually, every healthcare professional within
the hospital has his reference number, which is
unique.
In order to provide for an efficient way for
identification and authentication, the development of
access control tools is based on a European
prestandard, ENV 12251 (CEN/TC251, 2000). This
allowed for a better understanding and definition of
some basic, standard rules pertaining to the use of
login and password.
For this purpose, the standard protocol LDAP
(IETF, 2003) was introduced. In this specific case,
due to institutional policy demands, the chosen tool
to provide for that protocol is the Microsoft Active
Directory (MSDN, 2003). Some results from this
implementation are described in section 3.
2.1.2 Secure Communications
The same issue about heterogeneity applies to this
section (Figure 1). Each departmental system is
positioned in a different physical location within the
hospital while the database server and file system are
placed somewhere else. It becomes very difficult to
both protect and monitor every part that comprises
the system. Internet technology is the most
appropriate in this case because several platforms
and processes need to be integrated (Correia, 2001).
This technology is cost-effective, easy to implement
and has standards that a wide number of people
nowadays is used to interact with.
However, it is very hard to protect this
infrastructure against eavesdropping, tampering or
message forgery, when all the wiring and equipment
is spread all over a big hospital. Means to prevent (or
SECURING A WEB-BASED EPR: AN APPROACH TO SECURE A CENTRALIZED EPR WITHIN A HOSPITAL
55

at least minimize) malicious and/or accidental
actions were implemented.
2.2 Integrity
One of the main security issues that healthcare
professionals specified (and is implicit) is the trust or
confidence put into the information withheld by the
patient’s reports they need to access. The alteration
or corruption of these reports needs to be avoided.
The healthcare environment, probably more than any
other environment, requires that information is valid,
correct and complete (e.g. provide for integrity).
In order to achieve this, the reports that are
automatically generated from the departmental
systems (Figure 1) are all digitally signed and
encrypted before being stored in the file system
server. More details about how this is done and some
performance tests are presented in section 3.
2.3 Availability
As was already mentioned, availability is a
fundamental part of information security but often
overlooked. Having user-driven security measures in
mind, availability issues need to focus on means to
provide for the continuous information availability
for authorized users of the HSJ.ICU.
It is then important to provide for equipment
redundancy, with the use of action-specific machines
and other redundant power equipment; the recording
of the most important actions and errors that may
occur during system’s usage (so that the system can
be always updated and corrected); and finally, there
is the need for backups so that information resources
can easily be replaced if anything damages them.
3 RESULTS
Each departmental system can generate several
reports daily (some up to 30 reports per minute).
These reports are collected by the EPR HSJ.ICU and
Figure 2: User Authentication to the HSJ.ICU
stored within a file system. Further information
about their location, date and time, exceptions, errors
and so on, are stored in a database system. This will
enhance and speed their retrieval.
Most healthcare professionals’ concerns assessed
by the project’s team relate with secure auditing for
further notification and responsibility of
unauthorized users’ access; the integrity and
reliability of the generated reports; and the provision
for the confidentiality of the sensitive information
involved within the whole process. These issues map
very well with what the project’s team assessed as
user-driven security problems. Also, apart from the
concerns mentioned above, there is also a main issue
not to be overlooked: availability (Barrows, 1996).
Some implementation tools, technologies and
performance tests will be now presented.
3.1 Confidentiality
3.1.1 Access Control
Figure 2 shows how the user authenticates to the
Microsoft Active Directory by presenting a login and
a password (Figure 3 presents the web page where
the user gives his credentials for authentication.).
These credentials are verified in the Active Directory
server to allow (or not) the access to the HSJ.ICU.
The main advantage for the use of Microsoft
Active Directory (Microsoft implementation for the
LDAP protocol) is the separation between access
control and access to the requested information
stored in the database. Using technologies dedicated
to specific services that can easily integrate among
each other improves performance and establishes
separation of concerns. Further, the Microsoft Active
Directory contains other tools that allow configuring
security policies in accordance to the ones specified
within the prestandard ENV 12251.
Table 1 (AD=Active Directory) shows the
requirements that were implemented from the
prestandard. Only two of the requirements are still
being implemented. It is also important to refer that
ICEIS 2004 - INFORMATION SYSTEMS ANALYSIS AND SPECIFICATION
56
all these tasks are quite transparent to the user when
he tries to authenticate himself to the system.
Other issues such as maintaining the identity of
active users, is achieved by creating and managing
sessions with PHP (PHP, 2003). This registers a
unique and temporary session for each user that
logs-on allowing the control of user’s activity. Also,
whenever each user logs to the system, a flag in the
Active Directory (e.g. isLoggedIn) is set to TRUE,
and the opposite when he logs out. Information
about date, time and user’s identity is also recorded
in the Oracle Database for future actions, if needed.
Table 1: Prestandard ENV 12251 requirements
Requirement Tools
Unique identification & authentication
(user reference number)
Y AD
Identification and Authentication prior to all
other interactions
Y
AD
Oracle
PHP
Associating unique identity with users (ref. no) Y AD
Maintaining the identity of active users
(flag isloggedin in AD)
Y
AD
PHP
Log-on message (Figure 3 – top left corner) Y HTML
Number of log-on trials (3 times) Y AD
Incorrectly performed log-on procedure Y AD
Display of log-on statistics Y AD
Password sharing Y AD
Password storage (one-way encryption tools) Y AD
Logging of passwords N
Password display suppression Y HTML
User-changeability of passwords Y AD
Default passwords N/a N/a
Initialised passwords Y AD
Temporary passwords Y AD
Password expiration (2 months) Y AD
Password expiration notification (before expires) Y AD
Password reuse N
Password Complexity Y AD
The only part of the process that breaches the access
control rules explained before is when an authorized
user (already logged-on to the system) wants to
access some resources he is not authorized to. In a
case like this (e.g. break the glass), he has the option
to proceed or not whilst all his actions are properly
recorded for future notification.
Figure 3: Form for user authentication to the HSJ.ICU
In summary, the access control is a security
service that was thought from the beginning and
simple rules were applied so that no extra effort
would be asked to the user. Still, its transparency
does not allow for security relaxation. There are a
series of procedures that provide and support for the
monitoring, notification and prevention of
unauthorized access and usage of the system.
3.1.2 Secure Communications
Encryption is a security mechanism that allows for
the transformation of plaintext information to a
sequence of non-understandable characters.
In order to provide for the encryption of all
information whilst in transit the system uses the TLS
authentication protocol (IETF, 1999). This protocol
is a standard and is widely used for client/server
secure transactions among the most common
browsers, using internet technology. It has a
selection of encryption algorithms to be chosen
according to the type of authentication (e.g.
mutual/unilateral) required.
3.2 Integrity
The process of digitally signing, along with
signature verification of the generated reports by the
departmental systems can be seen in Figure 4.
A digital signature, allied to a digital timestamp
(particularly helpful in enhancing the integrity of a
digital signature system) is applied before the reports
are stored. This means that if someone or something
tries to tamper with the report, that signature will not
be valid any more.
Without getting in too much detail, the
technology used for this process is the GnuPG
(GnuPG, 2003), an open source that is based on the
PGP standard email encryption software. It uses
SECURING A WEB-BASED EPR: AN APPROACH TO SECURE A CENTRALIZED EPR WITHIN A HOSPITAL
57
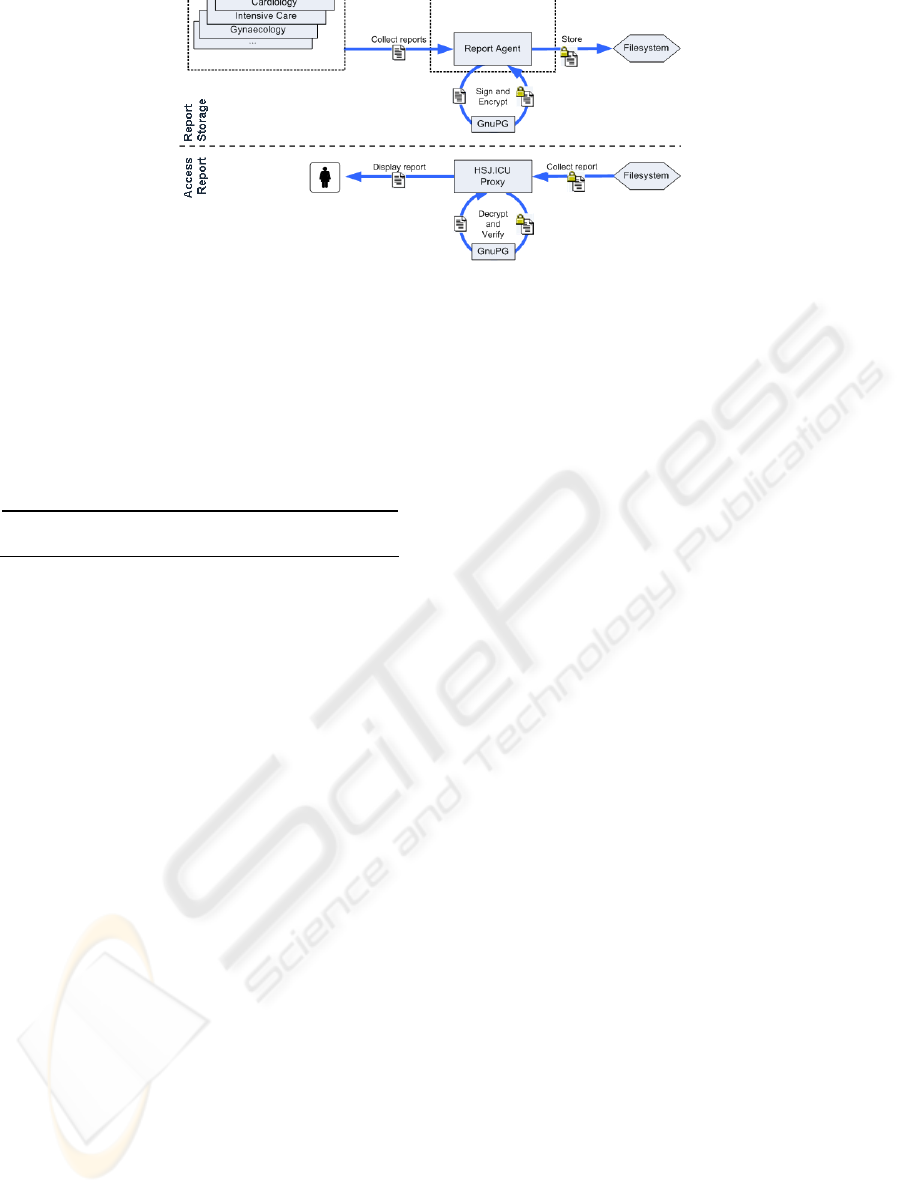
Figure 4: Report’s Digital Signature and Signature Verification process
public key DSA algorithm with key size 1024 bits,
impossible to break with today’s technology
(Silverman, 2000). Table 2 presents some
performance results to both apply and verify the
digital signature. It is important to mention that
different technologies are used for each of these
processes.
Table 2: Performance tests for a report’s digital signature
Process (Mean N=5) Without DS With DS
Store report 5 ms 33 ms
Access report 35 ms 48 ms
According to the results presented in Table 2, the
process of signing reports is generally slower than
the process of verifying their digital signatures.
Nevertheless, the process of signing and storing a
report is only done once, while the process of
accessing reports will be done numerous times.
Further, the digital signature and storage of the
reports is an automatic process and does not require
any user interaction. It is programmed to do it at the
least workload time.
In conclusion, the time difference registered
between both processes (signing and verification of
the digital signature) is not that relevant and does not
compromise system’s usability.
3.3 Availability
According to what was already mentioned about
availability, Figure 5 shows the generic hardware
architecture of the HSJ.ICU.
The extra equipment such is the load balancer,
allows for the balance of the work load to the
available web servers (two in this case). This will
enhance the availability of resources and will
provide access redundancy whilst increasing speed
retrieval of users’ requests.
All connections started directly or indirectly by
users are registered. Information about the user, date,
time and a unique session identifier are also
recorded. Apart from the usual file and database log
mechanisms supplied, user actions are recorded into
a file (at real time), ready to be inserted in a
structured way in the database system.
Other unsuccessful actions or errors generated by
the system are also registered because the HSJ.ICU
is still in the development stage and there is the need
to know what the weakest points are and what
problems still need to be corrected. Further, this will
allow following all important steps of the system’s
execution and guaranteeing that it does what is
supposed to do (or not).
Even more important than redundant equipment
is the need for data redundancy. Regular backups are
being made with database structure, data and file
system stored information so that it can be easily
replaced if anything corrupts or damages the original
information. This will allow minimizing the
unavailability time, and if possible, preventing any
outage of the system.
4 DISCUSSION
The development and implementation of the
HSJ.ICU project has been a very good learning
process for everyone involved in it. Although is still
work in progress, very important results were
already obtained.
One important conclusion is the fact that the
introduction of security from beginning as part of the
systems’ features and capabilities is essential. It
makes the process much simpler and transparent to
the normal user. Furthermore, having always in mind
the CIA (Confidentiality, Integrity and Availability)
structure helps organizing and in a way, separate
concepts that can be assessed in a more direct and
efficient way.
However, this is not enough. People (specially
future users) must be involved in the whole process.
Healthcare professionals have a higher sense for
providing for information security and patient
privacy. However, there is the need to make sure
security does not interfere with their work.
ICEIS 2004 - INFORMATION SYSTEMS ANALYSIS AND SPECIFICATION
58

Another important consideration is the use of
standards. This helps and speeds any project’s
implementation, whilst benefiting from the already
thought, tested and implemented procedures.
Another relevant aspect of this project’s
implementation is the use of cost-effective tools,
mainly web based, and the fact that it is still possible
to build security that works and is usable.
Finally, this project needs to be tested and
evaluated on a real environment. There is the need to
analyze some more performance and usability issues
that involve security. It is a project that will never be
completed as management support and updates will
be essential to apply. Nevertheless, security issues
are already rooted and constitute a good basis for
any enhancements that will be made in the future.
REFERENCES
Barrows, C., 1996. Barrows C, Clayton P. Privacy,
Confidentiality and electronic medical records.
JAMIA. 3:139-148.
Bemmel, V., 1997. Handbook of Medical Informatics. M.
A. Musen Editors. Springer.
Benson, T., 2002. Why general practitioners use
computers and hospital doctors do not-Part2:
scalability. BMJ. 325:1090-1093.
CEN/TC251, 2000. ENV 12251: Health Informatics -
Secure user identification for health care
management and security of authentication by
passwords.
Correia, R., 2001. Acquisition, processing and storage of
vital signals in an electronic patient record system.
Presented at Mednet 2001.
Ferreira, A., 2002. Electronic Patient Record Security.
Msc in Information Security. Information Security
Group. Royal Holloway, University of London.
GnuPG, 2003. Gnu Privacy Guard, Open PGP. Available
at:
http://www.gnupg.org
Figure 5: Generic HSJ.ICU hardware architecture
.
Godoy, C., 2002. A privacidade e o registro informatizado
na Faculdade de Medicina de Marília. Encontro
Paulista de Pesquisa em Ética Médica 2002.
Hassey, A., 2001. A survey of validity and utility of
electronic patient records in a general practice. BMJ.
322:1401-1405.
IETF, 1999. TLS – Transport Layer Security. RFC 2246.
Internet Engineering Task Force - IETF. Available
at:
ftp://ftp.rfc-editor.org/in-notes/rfc2246.txt.
IETF, 2003. LDAP – Lightweight Directory Access
Protocol . RFC 2251. Internet Engineering Task
Force - IETF. Available at:
http://www.ietf.org/internet-drafts/draft-ietf-ldapbis-
protocol-18.txt.
Kurtz, G., 2003. EMR confidentiality and information
security. Journal of Healthcare information
management. 17(3):41-48.
MSDN, 2003. Microsoft Active Directory. Available at:
http://msdn.microsoft.com/library/default.asp?url=/li
brary/en-us/netdir/ad/active_directory.asp.
PHP, 2003. PHP Hypertext Preprocessor. Available at:
http://www.php.net.
Salazar-Kish, J., 2000. Development of CPR Security
Using Impact Analysis. AMIA Annual Symposium.
Shortliffe, E., 1999. The Evolution of Electronic Medical
Records. Academic Medicine;74(4):414-419.
Silverman, R., 2000. A Cost-Based Security Analysis of
Symmetric and Asymmetric Key Lengths. RSA
Laboratories Bulletin, 13.
Stausberg, J., 2003. Comparing paper-based with
Electronic Patient Records: Lessons Learned during a
Study on Diagnosis and Procedure Codes. J Am Med
Inform Assoc. 10:470-477.
SECURING A WEB-BASED EPR: AN APPROACH TO SECURE A CENTRALIZED EPR WITHIN A HOSPITAL
59
