
An Empirical Study into Governance Requirements for
Autonomic E-Health Clinical Care Path Systems
Mr. Philip Miseldine
1
, Prof. Azzelarabe Taleb-Bendiab
1
1
Department of Computing and Mathematical Sciences, Liverpool John Moores University.
Abstract. Information technology has been widely recognized as a key build-
ing block to the Government modernization agenda for the NHS, and a vital
component to assisting continuous improvement in clinical practice, patient
safety and standard of care. Medicine is far from a static field, and this is espe-
cially true for research into the prevention and treatment of breast cancer,
which is thankfully ever changing and advancing towards more comprehensive
care and therapy for the condition. With such a fluid and fluctuating set of re-
quirements, software that aids in the delivery and prognosis of therapy faces
real challenges in its design so that it can adapt successfully as and when re-
quired to new requirements in the field. This paper will discuss the challenges
that designers of such software must solve, and highlights the issues facing cur-
rent state-of-the-art solutions in the domain of breast cancer prognosis. The pa-
per then introduces the notion of system self-governance to produce a rigid yet
highly dynamic system that is evaluated through a case study involving several
leading UK cancer hospitals. The paper concludes with analysis of how the
principals introduced in the paper can be applied to the wider domain of
eHealthcare.
Keywords: breast cancer prognosis, requirements engineering, ehealthcare, self
governance, adaptable system design
1 Introduction
Software engineering aims for the systematic, principled design and deployment of
applications that fulfil software’s original promise: applications that retain their full
malleability throughout their lifetime and that are as easy to modify when deployed as
they are on the drawing board [18].
Whilst significant advancement in the field has been made to meet these goals
through the development of high-level languages, structured design using object
orientated design, and software configuration abstraction through policy definition,
software remains fragile to changes in its environment and its perceived requirement.
Indeed, software that facilitates diagnosis in a field such as healthcare, where ad-
vances in research coupled with the wide-ranging and unpredictable requirements of
Miseldine M. and Taleb-Bendiab P. (2005).
An Empirical Study into Governance Requirements for Autonomic E-Health Clinical Care Path Systems.
In Proceedings of the 1st International Workshop on Requirements Engineering for Information Systems in Digital Economy, pages 89-100
DOI: 10.5220/0001423600890100
Copyright
c
SciTePress

patients and clinicians, has to adapt and react to requirement change to remain useful.
It is here where such fragility in design is all too apparent.
This paper discusses how the current design of information systems is ineffective
in its delivery of informatics in healthcare systems, focusing on the domain of breast
cancer care by evaluating current state-of-the-art prognosis systems against recog-
nized requirements. An approach to ease the deployment of adaptive decision proc-
esses that encapsulate requirements using distributed, highly adaptable system gov-
ernance is outlined and evaluated through a wide reaching case study involving sev-
eral leading cancer treatment hospitals. The paper concludes with discussion of em-
ploying the proposed programming model within different areas of eHealthcare, in-
cluding a description of a dental triage study.
2 Identification and Capture of Requirement
This section will explore the exact nature of the perceived requirements for modern
medical information systems and judge the suitability and effectiveness of current
state-of-the-art prognosis systems to represent these requirements.
2.1 Clinical Requirements in Medical Information Systems
In a report published by the National Coordination Office for Information Technol-
ogy Research and Development (NITRD) [19] it was recommended that information
systems play a critical role in assisting clinical decision as recommended by medical
institutions and government regulations. An evidence-based approach to the delivery
of clinical care has gained wide recognition within the healthcare community, advo-
cating that decision-making should use current knowledge and clinical evidence from
systematic research [23]. Medicine is far from a static field, and this is especially true
for research into the prevention and treatment of breast cancer, which is thankfully
ever changing and advancing towards more comprehensive care and therapy for the
condition. For software to successfully aid in the clinical decision process these initial
requirements imply that systems must adapt their decision process based on current,
often changing recommended knowledge.
As with much of scientific research, whilst there is general consensus on the iden-
tification of the problem domain, there is a wide range of variety in proposed solu-
tions and best-practice recommendations. In the medical field this variety is encapsu-
lated within published guidelines from different institutes, which clinicians adhere to
based on internal preference, or through the recommendation of a governmental body.
For example Christie Hospital, Manchester [2] and the Linda McCartney Cancer
Research Centre, Liverpool [12], use their own internally developed set of guidelines
based on the knowledge of their own respective clinicians and specialists. Any guide-
lines used by NHS centres (such as Christie) must also adhere to the governments
own guidelines set by NICE [17].
With the wide range of requirements based on conformance to guidelines for care,
there is no recognized standard method to support clinicians' decision-making proc-
esses as to how and when to include new evidence, or other models and practices
90

from elsewhere. This means that there is no standard way to ensure that clinicians are
following accepted guidelines or deviating from them.
The variety in the decision process, and the requirement for conformance to set
guidelines makes coordination a central pillar in any solution to the NITRD propos-
als. Changes to guidelines must be reflected as soon as possible within a decision
system so that conformance is maintained, and to keep the system as up to date with
current knowledge as possible. As software diversity leads to data variety [9], to
successfully represent variety within a guideline decision model, any system must
also provide coordination in its formulation and representation so change is effec-
tively propagated from requirement definition to actual inclusion within the system.
This is particularly relevant when individual clinician concerns are considered.
Static modelling through a static system oftentimes will yield an updated decision
process for an individual clinician, rather than for the organisation or institution as a
whole. It is up to the responsibility of the clinician to distribute the change or new
requirement, and then for this to be reintroduced into the institutions system. Some
adaptation or requirement alteration might not be considered appropriate for general
use within the organisation, however might be appropriate to a subset of clinicians
within the institution. Again, within a static system the complexity of tracking which
models have evolved for which clinicians makes this coordination impractical. This
complexity is compounded by the fact that research shows uptake of guidelines by
clinicians in practice is generally poor [4].
Indeed, these issues can be extended outside the scope of the medical domain. Any
organisation that distribute decision processes through their systems to their mem-
bers, and that require adaptation based on the position of a member within the organi-
sation, or the personal requirement of the member, face the same issues of coordina-
tion and lack of support within statically defined information systems.
2.2 Patient Requirement and Requirement Priority
Clinical and clinician concerns are not the only dynamic requirements that a medi-
cal information system should consider, however. A strategic report for the Depart-
ment of Health in particular notes that “the involvement of patients in decisions about
individual care and policies - including R&D priorities - is widely advocated but little
information exists about its impact or value” [8] and advocates that the involvement
of the patient into the decision process is “the most cost effective way to provide in-
formation to meet the needs of patients, their families, healthcare professionals and
the public”. In addition, research [21] indicates that software implementations of
guidelines (SIGs) are more likely to be used by clinicians if they provide patient spe-
cific advice during consultations.
Such requirements are particularly important in cancer care where proposed treat-
ment is often invasive or can cause irreversible damage to the patient, both physically
and mentally. Thus, patient consultation, and respecting their requirements for treat-
ment are essential for successful treatment.
91

2.3 Computer Based Prognosis Systems and SIGs
Two complementary forms of system are used to provide computer-based prognosis
in deployment. The first type of system is an all-encompassing solution that provides
a service-based approach to prognosis, by assisting the clinician or patient during
consultation. In general, these systems are web-based and distributed and maintained
by an Application Service Provider (ASP). A notable example of an ASP delivered
service in breast cancer prognosis is the AdjuvantOnline service [1] which is widely
used by clinicians in the UK. Clinicians enter patient data into a predefined interface
and retrieve a graphical report of prognosis and possible treatment plans. Clinicians
enter the system “blind”, that is, the system stores no information regarding their
historical usage or preferences, and the same experience is repeated to any user of the
system, without personalization. This is typical of ASP based prognosis, including the
implementations Finprog [6], and OncoDoc [20]. As such, their effectiveness to deal
with the issues highlighted in the previous discussion are highly limited.
The second system type is a multi-stage solution with a SIG implementation under-
lying a user interface that acts as an interface to query the SIG. The interface layer of
these applications can fall into the first form of system, where an ASP provides the
interface and the SIG is maintained externally. By controlling development of the
underlying decision process encoded within a SIG, a better model for adaptation and
coordination can hoped to be delivered.
A well known model is the Arden Syntax [25] originally developed as an observer
system to act as a hospital “watchdog” monitoring data values. It is a text based pro-
gramming language for encoding medical logic modules (MLMs), though is difficult
for non-computer literate medical experts to use. It has a simple grammar, rule-based
formalism and has been adapted for representation of guidelines by using interacting
MLMs. Similarly augmented decision tables (ADTs) [24] have also been used to
extend the rule-based functionality of Arden by augmenting rules with additional data
such as probability and utility. However neither the Arden Syntax nor ADTs provide
support for producing a guideline that evolves over time and with evidence accrual.
This makes individual modules weak in functionality and the more complicated mul-
tiple modules guideline model, increases complexity and decreases readability, mak-
ing it unsuitable for rapid refactoring and adaptation.
2.4 Limitations in Current State-of-the-art
The review of requirements given in this section, when compared against the abili-
ties of the current state-of-the-art systems used within breast cancer prognosis show a
distinct lack of correlation. Indeed, the software used today falls well short of provid-
ing even basic coordination, governance and adaptability, all essential tenants to ad-
vance prognosis through informatics.
The rest of this paper will focus on a proposed solution by promoting the notion of
self-governance to coordinate adaptation and usage of the decision process, based on
user requirement, and conformance regulation.
92

3 The Promotion of Distributed Self Governance
With systems in the field of eHealthcare and breast cancer prognosis in particular
requiring such fluid and adaptable requirements, yet with strict conformance to set
practices and guidelines, a notion of governance is required to reign in and coordinate
software requirements within a distributed organisation where individual users of the
system require tailoring of the processes of the software system.
In the static, closed systems described in section 2.3, these requirements are often
either hard-coded into the decision process, or variety is introduced through input by
the clinician in the form of a patient profile. In addition, the context of the user’s
request is discounted. Thus any redevelopment or evolution of the decision process is
applied to all users, no matter their requirement. To develop adaptive, self-governing
systems however, this notion of context and its effect upon the system is critical.
3.1 Providing Governance Through Context
Context is often captured by software to provide personalization services to users,
and to mould the experience of using the service to the particular requirement of the
user. Oftentimes this is facilitated through an authentication model as typified by
AAA [27], where a user provides credentials to identify themselves within the sys-
tem, and their personal experience is reproduced and tailored based on stored criteria.
Such authentication is widely used within the Internet community to provide forums
for discussion, to access to personal information, and to digitally sign documentation.
In effect, by providing authentication criteria, a context of the request is formed as
additional, meta-level descriptions can be attached to the profile of an authenticated
user. For stricter control, by applying the techniques of role-based authentication [5],
users can be placed into groups with specific responsibilities and requirements. Con-
text can therefore provide the first stage of governance within a distributed system,
where assessed conformance requirements, patient profiles, and access to evolved
decision models can be planned according to individual profiling.
In the context of clinical care, different organisations and institutions have differ-
ent conformance models, where any decision process needs ratification against, for
example, NICE guidelines. Other organisations do not require such ratification.
Through context, a request can be scrutinized accordingly, providing validation for
the decision process. As such, there exists a hierarchical model for conformance
based on context, as illustrated in Figure 1:
93
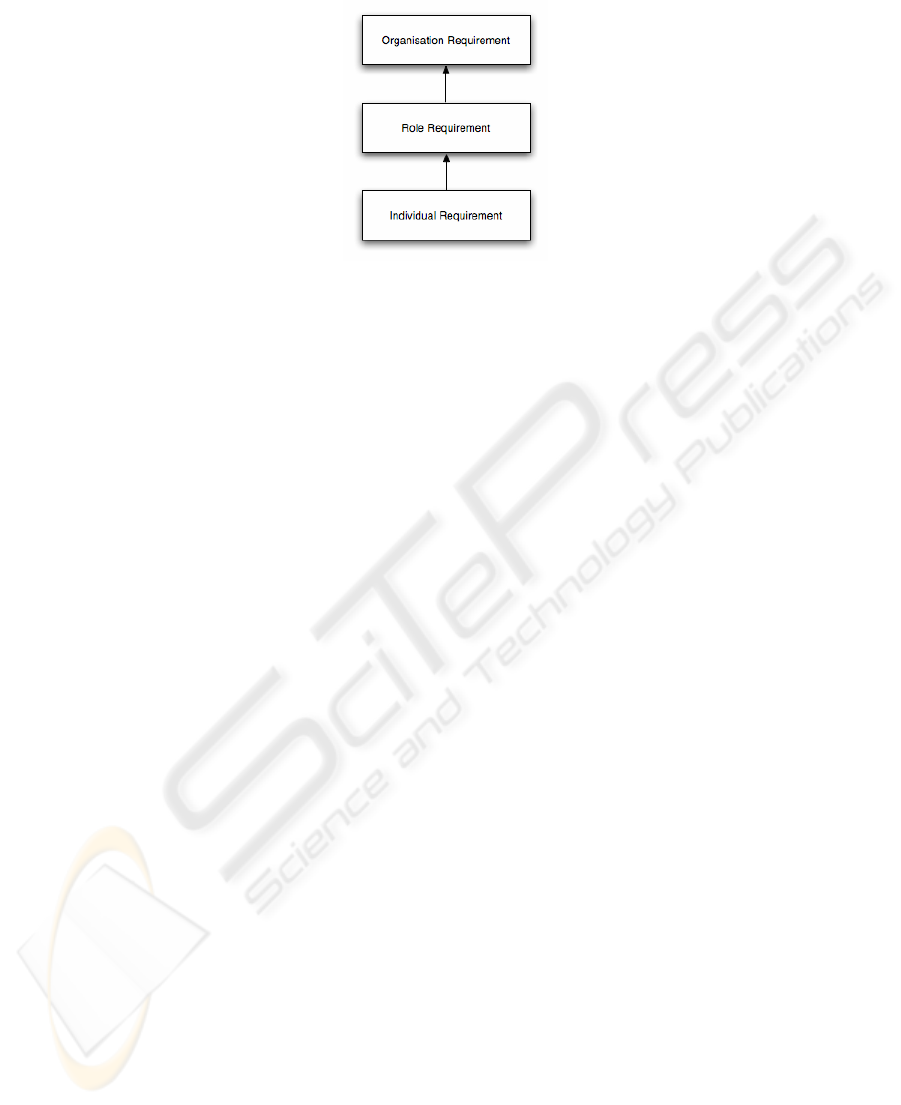
Fig. 1. Conformance hierarchy in a typical clinician scenario.
Accordingly, the individual concerns must conform to the requirements set out by
the role in which the individual exists within the organisation. This is then supplanted
by the requirements of the organisation as a whole. Thus, to govern adaptation of
requirement, each conformance model defined above the requirement level in the
hierarchy must ratify the change.
3.2 Ensuring Safety and Influence Through Governance
Thus the hierarchical model of governance is essential when defining the structures
required to represent and facilitate governance throughout the end system, and
thereby adapt the system based on requirement safely and predictably. Safety in com-
puter implemented guideline systems is a critical responsibility. Safety is very impor-
tant both in terms of the outputted decision, provability of the correctness of the rep-
resentation and completeness. These desirable characteristics are more likely in sys-
tems where there is “a recognised software design paradigm used, knowledge and
logic are separated, a simple tool kit is used, there is a minimal feature set expressive
enough to encode guidelines in a simple manner, a decision making process can be
followed and clinician knowledge can be used and the decision overridden” [7].
By constricting the goal of a decision process to be the successful conformance of
the decision process with the associated conformance models specified through the
hierarchy, an adaptation or alteration based on a changing requirement can be gov-
erned in a programmatic fashion. As an example, acceptance of a treatment plan is
itself a decision model, actuated by a clinician. The process of the decision model is
to recommend a treatment plan for a patient. This is the intention or requirement of
the clinician. However, for the process to be successful, it must ratify itself against
the conformance models specified within the hierarchy.
Such conformance can be thought of as having direct, external influence upon the
decision process of a model. After all, if a process does not successfully correspond
to the conformance models set out within the organisation, it cannot be completed.
This paradigm for governance is typified in the R
5
architectural model [11] which
states that a decision will often be made because of some internally or externally
imposed formality, and as such can be modelled in the form of rules, regulations and
94

recommendations. Thus, by applying the principals of R
5
to the requirements of con-
formance, a rigorous approach can be produced.
It has been discussed in the preceding sections of the importance of equipping
adaptive software with the notion of governance based on context. Coordinating and
actuating this model within software however, produces many challenges. Any solu-
tion must distribute the currently held conformance models amongst the organisation,
so that any adaptation requirement at any level of the system can be ratified. Adapta-
tions to requirements must then be actuated and distributed so their effect is included
at the required level within the organisation.
At a much lower level however, there needs to exist a methodology that supports
adaptable decision models, or SIGs. As discussed in 2.3, SIG implementations used
in the breast cancer prognosis are either static and hard-coded, or too complex to
enable adaptation during the execution of the system. In addition, for information
systems to support autonomic behaviour [26], that is, a systems ability to adapt itself
to perceived change, the system must be able to reason upon its own construction,
and have the necessary functionality to enable itself to adapt.
4 Implementation
4.1 Requirement Representation Using Neptune
In earlier work [16] the author’s introduced a programming language, Neptune, that
produces an object form of guidelines that can be inspected, modified and deliberated
upon at runtime. Neptune objects encapsulate the logic and assignments expressed
within a guideline in a transparent, introspective object notation, allowing fine-grain
adaptation of the decision process to take place. Accordingly, requirements of guide-
line conformance and user preferences can be encoded in such a form that they can be
both interpreted and adapted dynamically with or without direct human interaction.
As an example, Fig.2 shows a section of the NICE guidelines for operative breast
cancer care, encoded within Neptune:
define rule calcNPI
variables.sd = 0.2 * dataset.tumoursize + dataset.nodestatus + dataset.histological
if (variables.sd <= 5.399)
variables.npi = 2
else
variables.npi = 1
end if
end define
Fig.2. A rule as defined within the NICE guidelines for operative breast cancer care, encoded
within Neptune
A comprehensive guide to the language syntax is given in [15], and subsequent
discussion of its structural design is outside the scope of this paper. Of importance
95

however, is how this formulation of a rule in language is represented computationally
as an object, allowing object orientated programming models to be applied to the
decision process. Object serialisation techniques, allowing an object to be stored,
transferred and retrieved from information repositories, can thus be applied to Nep-
tune objects, allowing the safe and efficient distribution of decision models. In this
way, Neptune allows the modification and enhancement to the decision process dur-
ing any point of its lifetime whilst maintaining efficient transportation and storage.
4.2 Applying Self Governance Through CA-SPA Policy Modelling
Policies are a means of specifying and influencing governance behaviour within a
distributed system, without directly including the behaviour within the management
services themselves [13] unlike the approaches outlined in section 2.3. A policys’
intent commonly takes one of two forms: authorisational and obligational. Authorisa-
tion policies specify what activities a service is permitted or forbidden to do to a set
of target objects and are similar to security access-control policies. Obligation poli-
cies specify what activities a service must or must not do to a set of target objects and
essentially define the duty of a service. As such, the obligation policy provides a
suitable model for conformance enforcement.
Policy intentions are complex statements that cannot easily be encoded computa-
tionally. Much work has been undertaken [22]; [27] to represent policies using lan-
guage based methodologies, which has shown that whilst policies cannot be easily
represented in terms of attributes or directly translated into method definitions, the
traditional programming language constructs, they are often realised through a com-
bination of attribute and method implementation. Such methodologies however gen-
erally lack the mechanism to represent and enable evolved adaptation. Neptune, as
shown in [14] is well-suited to such representation, however.
By representing both the situation and required behaviour to enact upon the sys-
tem entering the situation in a policy form, a defined boundary of behaviour can be
produced. In other words, a model for conformance is achieved. Basing these repre-
sentations within Neptune, each stage of the conformance can be adaptable as re-
quired, using the introspective nature of the language.
CA-SPA is a methodology developed by the authors to produce such a policy
model, based on a situation, an action ontology, and a predicted situation that the
system should find itself within after execution of the action ontology [3]. This final
predicted situation is important to ensure that the intention of the policy has been
completed. To demonstrate the CA-SPA model efficiently, the earlier example of
ratifying a treatment plan against the conformance hierarch can be modeled as a CA-
SPA policy. The only situation in which a treatment plan can be accepted, is when the
treatment plan conforms to the organisation’s own guidelines, and for the purposes of
illustration, a set of government guidelines. These guideline models are themselves
encapsulated within Neptune objects
organisationGuidelines and governmentGuidelines
respectively. As such, the situation for the CA-SPA is thus:
If (organisationGuidelines.Conform && governmentGuidelines.Conform)
96

When this situation is entered, we can accept the treatement plan, as specified
within the ontology of the CA-SPA:
patientTreatmentPlan.Accept
Leaving our predicted situation, after the action ontology is executed, to represent
the fact a treatment plan has been accepted for the patient:
Patient.TreatmentPlan != Nothing
5 Case Study
As part of an EPSRC sponsored project, the techniques and methodology described in
section 4 have been implemented to produce a web based prognosis system using a
set of tools that enable the representation of guidelines used by Christie Hospital, and
the Linda McCartney Centre for Cancer Care of Royal Liverpool Hospital. This sec-
tion details the benefits from a developmental perspective of the design, and how it
addresses the problem domain as defined previously.
5.1 Venus: Medical Decision Support System
The medical system, known internally as Venus, produces a context of request by
requiring users to log into the system. It is at this stage that users are assigned roles
within the organisation based on predefined categorisation. All authentication data is
stored on a database that provides a centralized repository of requirement and role
data, meaning all levels of the system are granted access to this information.
At every stage of interaction within the system, the request is first ratified against a
stored set of CA-SPA documents, which are themselves a federated set of Neptune
objects (representing each stage of the CA-SPA). Thus, the widest set of situations
can be captured, and requirement adapted as and when required.
5.2 Adaptation Based on New Requirement
Whilst the system can facilitate adaptation in its use of Neptune and CA-SPAs to
represent the governance of the system, it is the ability of these methodologies to
represent autonomic behaviour that is of particular interest to adaptation processes.
By capturing evolving requirements during the lifetime of the application, all the
constructs exist so that seamless evolution of the system occurs based on the require-
ments of its users. This evolution is monitored and controlled by the self-governance
specified through the system, to provide validation and boundaries for the system.
Hence patient, clinician, organizational, and external requirements can all be repre-
sented and enacted to produce a stable system that takes all requirement into account.
In Venus, an early example of these techniques has been produced. By analyzing
the usage patterns of a system user, the interface can itself adapt to speed up the proc-
ess of using the system, by tailoring its process to match that of its user. Thus, options
97
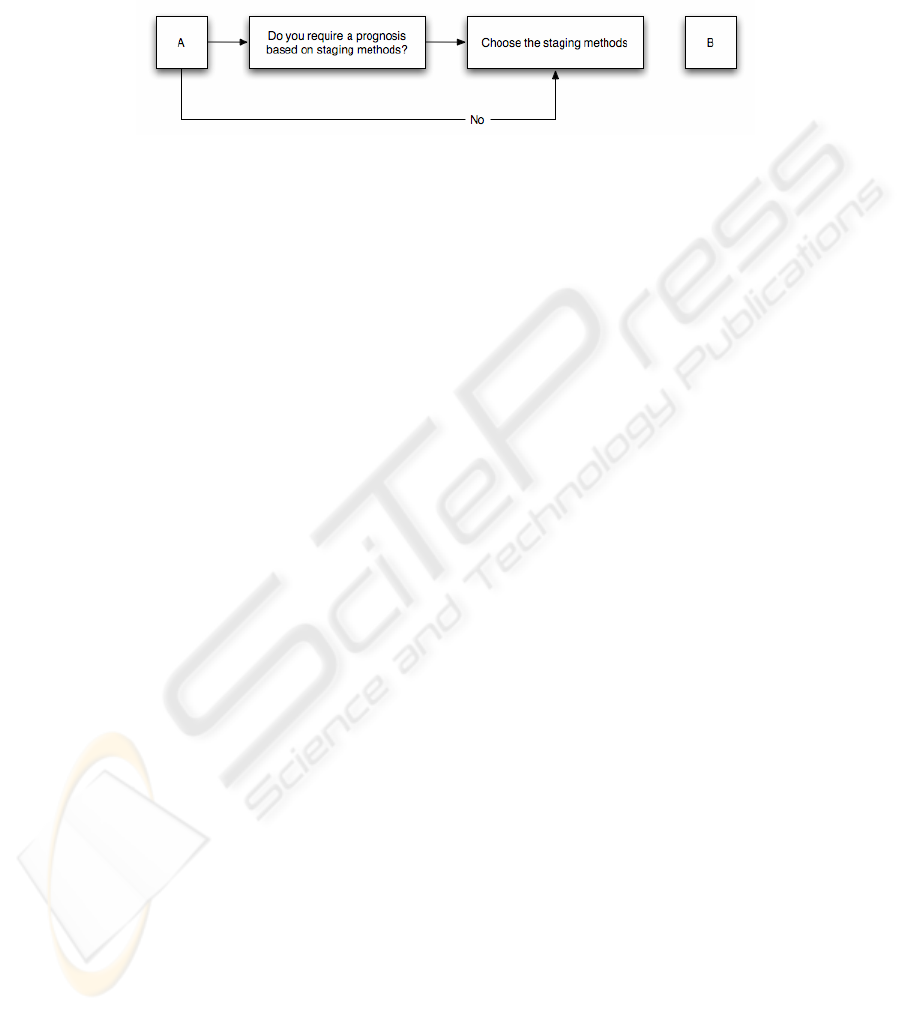
rarely used by the user are hidden, and stages can be skipped based on usage. This is
illustrated in figure 3, where to get from step A to step B within the process, a set of
stages are required.
Fig. 3. Part of the Venus process
Based on a CA-SPA whose situation is entered when the user decides “No” in the
above process for 5 subsequent times, these additional steps are removed from the
process creating a direct path from A to B. Provision exists within the interface to
restate the original process flow, if required at a later stage, as does the threshold in
which steps are removed from the process (in this case, 5 subsequent uses) as this can
adapt as required. In addition, patient concerns are expressed in Venus using the
HADS anxiety scale [10], where documentation for a patient is produced based on the
assessed anxiety (and therefore requirement) of the patient.
5.3 Application of Techniques to the Wider Field of e-Healthcare
Whilst the scope of this paper has focused on supporting breast cancer prognosis, the
techniques described herein can equally be applied to other areas of e-Healthcare as
shown by the production of a prototype decision support system for dental triage
services, for the Royal Liverpool Hospital using the Neptune and CA-SPA methodol-
ogy. The original system used by the Royal Liverpool Hospital combined a mixture
of Microsoft Word and Microsoft Excel documents to provide flow through the proc-
ess of triage for patients. In this way, information elicited from the patient formed the
basis of decisions on their perceived health. The more critical the condition (such as
persistent bleeding) the higher priority the patient was given to see a dentist.
The main requirement of the case study was to produce a system that could log pa-
tient details and their eventual classification by the system, with the end goal being
that the system could adapt its classification based on historical evidence to improve
the level of care given to patients. In addition, government targets facing the care of
dental patient, including waiting times needs to be considered.
By encoding the process flow within a Neptune object, an instance of the object
could be created for each patient as they passed through triage. Consequently, the
decision process, or rather, why the patient received the classification they did, is
encapsulated within the object instance itself. Storing this object instance, along with
the patient’s profile, comprehensive historical data was stored that could later form
the basis of evidence given to machine learning and data mining processes. Another
consequence of automating the storage of patient details and their path through the
decision model, patients modelled in the prototype could return to the hospital at a
later date, and clinicians would be presented with both the patient details and the
98

exact reasoning behind the decisions of the information system, essential in ascertain-
ing correct patient care.
6 Conclusions
This paper introduces the problem domain facing information systems in breast can-
cer prognosis, and offers a solution based on the notion of self-governance within a
system to provide flexibility in representing evolving user and system requirements,
whilst maintaining guideline conformance. It has been shown through the case study
that the issues resulting from the problem domain can be effectively solved using the
methodology introduced in this paper.
The issues facing breast cancer prognosis however, can be equally applied to a
wide range of fields, in both e-Healthcare and organisations as a whole. The need for
dynamic systems that adapt to perceived user and organisation requirement is felt in
many sectors that use IT to automate decision processes, as typified in the second
case study involving the automation of dental triage process. In the wider medical
viewpoint we can see applications for our approach in other areas of medicine, such
as the diagnosis and treatment of lymphoma which has a similar staging model to
breast cancer.
The authors gratefully acknowledge EPSRC for funding this research paper.
References
1. AdjuvantOnline. (2005). Http://www.Adjuvantonline.Com/.
2. Christie Hospital. (2005). Http://www.Christie.Nhs.Uk.
3. D. England, A. Taleb-Bendiab, P. Miseldine, M. Randles, & Murphy, K. (2005, February
2005). Integrating best practice and evidence based decision support for breast cancer care.
Paper presented at the Multi-disciplinary Workshop on Healthcare Information Services and
Future ICTs, UCL.
4. Feder, G., Eccles, et. al. (1999). Clinical guidelines: Using clinical guidelines. BMJ(318),
728-730.
5. Ferraiolo, D., Cugini, J., & Kuhn, D. (1995, December 1995). Role-based access control
(rbac): Features and motivation. Paper presented at the 11th Annual Computer Security Ap-
plication Conference, New Orleans, LA.
6. Finproject. (2005). Http://www.Finprog.Org/.
7. Fox, J., & Das, S. (2000). Safe and sound: Artificial intelligence in hazardous applications.
American Association for Artificial Intelligence.
8. Health, D. o. (1999). Strategic priorities in cancer research and development. In C. W. Group
(Ed.) (pp. 58): Department of Health.
9. Hiller, M. (1998). Software fault tolerance techniques from a real time systems point of
view: An overview: Chalmers University of Technology, Sweden.
10. Lampic, C., Essen, L. v., Peterson, V., Larsson, G., & Sjoden, P. (1996). Anxiety and de-
pression in hospitalized patients with cancer: Agreement in patient-staff dyads. Cancer Nurs-
ing, 19(6), 419-428.
99

11. Laws, A., Allen, M., & Taleb-Bendiab, A. (2002). Normative services for self-adaptive
software to support dependable enterprise systems. Paper presented at the 4th International
Conference On Enterprise Information Systems, Cludad Real, Spain.
12. Linda McCartney Cancer Research Centre. (2005). Http://www.Linda-mccartney-
centre.Org.Uk/.
13. Lupu, E. C., & Sloman, M. (1999). Conflicts in policy-based distributed systems manage-
ment. Software Engineering, 25(6), 852-869.
14. M. Randles, A. T.-B., P. Miseldine, A. Laws. (2005, April 2005). Adjustable deliberation
of self-managing systems. Paper presented at the 12th IEEE International Conference on the
Engineering of Computer-Based Systems (ECBS), Greenbelt, MD, USA.
15. Miseldine, P. (http://www.cms.livjm.ac.uk/2nrich/deliverables.asp). Neptune application
development guide.
16. Miseldine, P., & Taleb-Bendiab, A. (2005, June 2005). Rainbow: An approach to facilitate
restorative functionality within distributed autonomic systems. Paper presented at the PGNET
05, Liverpool.
17. National Institute for Clincial Excellence. (2005). Http://www.Nice.Nhs.Uk/.
18. Nauer, P., & Randell, B. (1969). Software engineering - report on a conference sponsored
by the nato scientific committee. Garmisch.
19. NCO. (2004). Revolutionizing health care through information technology. In N. C. Office
(Ed.): President's Information Technology Advisory Committee.
20. OpenClinician. (2005). Http://www.Openclinical.Org/prj_oncodoc.Html.
21. Overhage, J. M., Zhou, X. H., & McDonald, C. J. (1997). A randomized trial of corollary
orders to prevent errors of omission. JAMIA, 4(5), 354-375.
22. Ryutov, T., & Neuman, C. (2000, January 2000). Representation and evaluation of security
policies for distributed system services. Paper presented at the DARPA Informatioon Surviv-
ability Conference and Exposition, Hilton Head, South Carolina.
23. Sackett, D. L., Rosenberg, W. M. C., Gray, J. A. M., Haynes, R. B., & Richardson, W. S.
(1996). Evidence based medicine: What it is and what it isn't. BMJ, 312(7023), 71-72.
24. Shiffman, R. N. (1997). Representation of clinical practice guidelines in conventional
decision tables. JAMIA, 4(5), 382-393.
25. Starren, J., Hripcsak, G., Jordan, D., & Allen, B. (1994). Encoding a post-operative coro-
nary artery by-pass surgery care plan in the arden syntax. Comput. Biol. Med., 24(5), 411-
417.
26. Sterritt, R. (2002). Towards autonomic computing: Effective event management: IEEE
Computer Society.
27. Woo, T., & Lam, S. (1993, March 1998). Designing a distributed authorisation service.
Paper presented at the INFOCOM '89, San Francisco.
100
