
An Active Database Approach to Computerised
Clinical Guideline Management
Kudakwashe Dube and Bing Wu
Department of Computer Science, School of Computing, Dublin Institute of Technology,
Kevin Street, Dublin 8, Ireland.
Abstract. This paper presents a generic approach, and a case study practising
the approach, based on a unified framework harnessing the event-condition-
action (ECA) rule paradigm and the active database for the management of
computer-based clinical practice guidelines and protocols (CPGs). The CPG
management is cast into three perspectives: specification, execution and
manipulation, making up three management planes of our framework. The ECA
rule paradigm is the core CPG representational formalism while the active
database serves as the kernel within the CPG management environment
facilitating integration with electronic healthcare records and clinical workflow.
The benefits of the approach are: flexibility of CPG management; integration of
CPGs with electronic patient records and clinical workflows; and incorporation
of CPG management system into computerised healthcare systems.
1 Introduction
Clinical practice guidelines (CPGs) encapsulate medical knowledge about when
clinicians and patient should carry out specific activities in disease management.
CPGs are effectively “knowledge models of preferred processes of care” [1], which
can guide patient care activities and clinical workflow or care flow [2]. In practice, a
CPG is “a method that identifies actions that are to be performed and that specifies
conditions that govern when it is appropriate to perform them” [3]. Thus, a CPG
embodies the core compositional primitives of the event-condition-action (ECA) rule
paradigm. ECA rules are specified by an event, a condition and an action with the
semantic that the event must occur for the action to be executed subject to the
condition being satisfied [4]. An active database management system (ADBMS) is a
DBMS that incorporates the ECA rule mechanism and provides functionalities as
stipulated in the Active Database System Manifesto [5]. The ECA rule paradigm
could be a strong basis for formalising CPGs while an active database system could
be a promising management environment for computerised CPG. The authors’
hypothesise that, in combination, these two could facilitate a solution to the problem
of the integration of computer-based CPGs with the electronic patient record and
computerised clinical workflow. This paper presents a computerised CPG
management approach and a case study which uses a generic, unified management
framework and harnesses the ECA rule paradigm and the active database in the CPG
management task. The rest of this paper is organised as follows: Section 2 presents a
Dube K. and Wu B. (2006).
An Active Database Approach to Computerised Clinical Guideline Management.
In Proceedings of the 3rd International Workshop on Computer Supported Activity Coordination, pages 107-115
DOI: 10.5220/0002474001070115
Copyright
c
SciTePress

review of the ECA rule paradigm in computer-based CPG management support;
Section 3 presents the generic framework for CPG management; Section 4 presents
the method developed in this work for managing the CPGs using the ECA rule
paradigm and active databases within the SpEM framework; Section 5 presents a case
study in which the proof-of-concepts system is developed and used to manage the
microalbuminuria CPG for diabetes patients; and Section 7 summarises and concludes
this paper.
2 Relevant Work in Supporting Clinical Guideline Management
This section reviews relevant work in supporting computerised CPG management.
Research in computer-based support for the management of CPGs has been on-going
for over a decade. A number of approaches and systems have emerged during this
period. For a more general review, readers are referred to de Clercq et al [6]. Most
approaches focus on the formal representation and execution of computerised CPGs.
Among them, the Arden Syntax [7], an established HL7 standard [8], and HyperCare
[9] are most relevant to this work. While most approaches use control structure
primitives [6] to represent guidelines, the Arden Syntax and HyperCare use the ECA
rule paradigm. However, the Arden Syntax focuses on CPG specification only and
HyperCare focuses on execution only, using an active database system in its
implementation. Both the Arden Syntax and HyperCare do not create patient-specific
CPG instances. Instead, all rules operate with a global scope covering all patients.
Furthermore, these two approaches offer no support for the management of
information on both CPG specifications and their instances. Hence, they do not fully
exploit all the advantages of the database approach to realise CPG information
management. Departing from others, authors of this paper have developed a unified
CPG management framework which places equal emphasis on the CPG management
perspectives of specification, execution and manipulation and harnesses the active
database for supporting all aspects of this framework. In this framework, generic CPG
specifications are created and held in the database together with execution state and
effects for easy management. The CPG execution aspect supports patient-specific
CPG instances and harnesses the active mechanism of the DBMS. Furthermore,
database manipulation and query features are exploited for the computerised CPG
information management.
3 A Generic Framework for Clinical Guideline Management
This section presents a generic framework, SpEM [10] (Specification, Execution and
M
anipulation) developed by the authors for supporting the computerised CPG
management. As illustrated in Figure 1, the SpEM framework contains 3 planes:
specification plane; execution plane and; manipulation plane with the active database
as the integrating factor among the three planes.
108
Specification
Plane
Manipulation Plane
Customisation,
instantiation and
change propagation
Enforcement
Plane
Query, dynamic
interaction and
manipulation
Query, manipulation
and version maintenance
Application
Domain Database
System with
Active Mechanism
Specification
Plane
Manipulation PlaneManipulation Plane
Customisation,
instantiation and
change propagation
Enforcement
Plane
Query, dynamic
interaction and
manipulation
Query, manipulation
and version maintenance
Application
Domain Database
System with
Active Mechanism
Fig. 1. The SpEM framework.
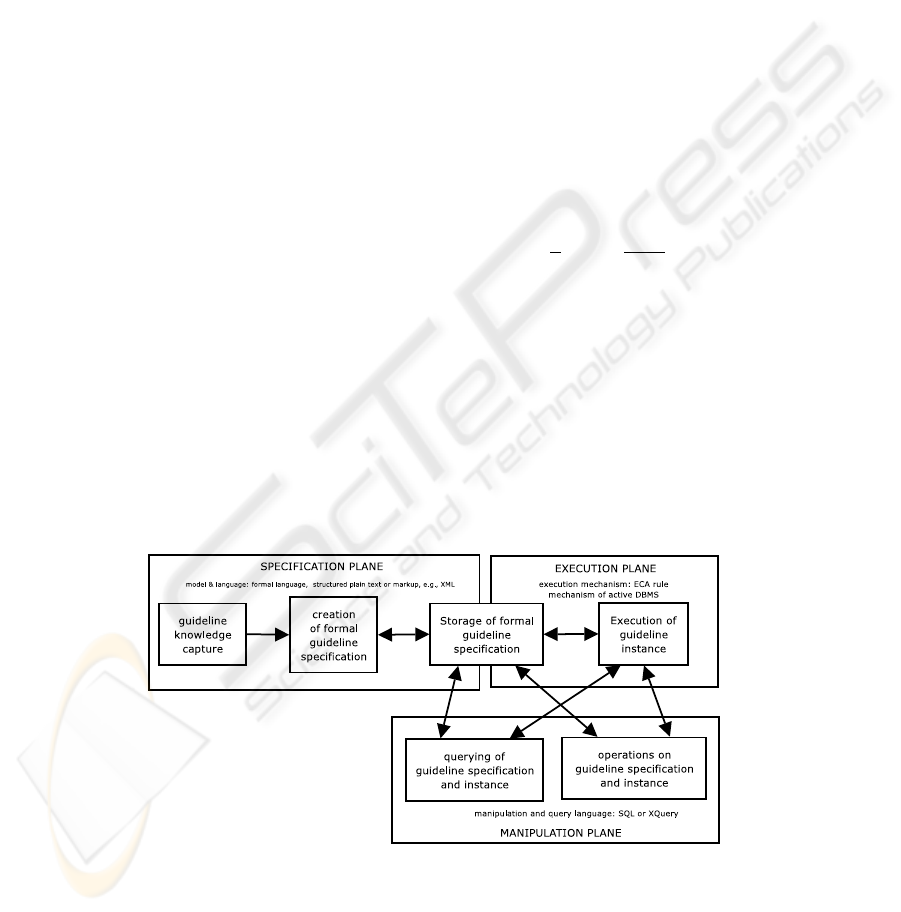
The CPG management process is fitted into the three planes of the framework. In the
specification plane, CPGs are translated into formal specifications and held
permanently in the database in a manageable form. In the execution plane, the stored
CPG specifications are used to create patient-specific CPG instances that are
executable by an engine based on the active database. In the manipulation plane, the
specifications and the executing CPG instances are manipulated using supported
operations and queries based on the SQL features of the underlying database system.
The active database is a base for an execution engine for CPGs. It provides facilities
for querying and manipulating information. It can also permanently hold the
electronic patient record in addition to CPG information and running processes.
Furthermore, it can guarantee future sharing of information through the generic nature
of databases and the standard language, the SQL. Table 1. summarises the support for
the SpEM framework in major existing CPG approaches and systems. However, these
approaches only provide guideline support mainly in terms of the specification and
execution of CPGs. Not much attention seems to have been paid to the support for the
manipulation and querying of the CPG information and to harnessing of database
features for CPG management. Manipulation of the static and dynamic aspects of
CPGs is important to allow flexibility and ease-of-use [19], which are some of the
major determining factors in the acceptability of guideline systems by clinicians [20].
Table 1. Support for the SpEM framework in existing CPG management systems.
SpEM Framework Support
Key: √ - full support, * - partially supported,
X – no support,
Manipulation
Guideline System
Specification Execution
Operation Query
Use of
Database
Features
DILEMMA/PRESTIGE
[11]
√ √ X X X
EON/Dharmma [12] √ √ X X X
PROforma [13]
√ √ X X X
GLIF [14] √ * X X X
Asgaard/ Asbru [15] √ √ * * X
GUIDE [2] √ √ X X X
PROGIDY [16] √ √ X X X
Arden Syntax [7]
√ X X X X
HyperCare [9]
X √ X X *
GASTON [17] √ √ * X X
GLARE [18] √ √ X X X
109
4 A Method for Computerised CPG Management
This section presents the method for managing computerised CPGs through the SpEM
framework. Fig. 2 illustrates how the method permeates the three planes of the
framework and allows CPGs to be formally specified, stored, executed with respect to
a given patient, and manipulated through querying and operations. Several aspects
need to be incorporated as components of the management process for supporting
CPG management. Domain knowledge, i.e., expertise and literature on recent
advances in medical knowledge, is the main source of CPGs. Its translation into CPGs
is done by clinicians and is outside the scope of SpEM.. Formal representation and
creation of CPG specifications and their storage are important aspects of the
computerisation of CPGs. Customisation and execution of computerised CPGs with
respect to specific individual patient are vital aspects of the management of
computerised CPGs. The manipulation of both the formal specifications and the
running process consists of the two aspects: querying; and performing manipulation
operations on the CPGs. The process illustrated in Fig. 2 is to ensure that most aspects
of the computerised CPGs can be managed. Fig. 2 also illustrates the main
functionality for supporting CPG management. The main requirement of the
specification plane is a declarative language, the clinical P
rotocol LANguage, PLAN,
together with its model [21]. PLAN was designed to use the ECA rule paradigm as
the core representation construct for specifying CPGs. Fig. 3. illustrates the general
syntax of PLAN in the Backus-Nuar Form (BNF). A PLAN specification consists of a
descriptive header; a set of schedules; and the protocol rule set. Just like a protocol, a
schedule is named and consists of an entry criteria and a list of rules each of which is
either a dynamic or static rule. For a more detailed discussion of PLAN, readers are
referred to Wu and Dube [21]. In the execution plane, the relevant PLAN
specification is customised and installed for each patient as an instance that runs
within the ECA rule mechanism of a database system. The execution of the guideline
instance follows the ECA mechanism. Within the manipulation plane, provision is
made to perform operations and to issue queries using a query and manipulation
language that is based on the SQL.
Fig. 2 The management support process in SpEM.
110
<static_rule>::= ECA rule with time events
<protocol>::=PROTOCOL<protocol_body>END PROTOCOL.
<protocol_body>::=<protocol_header>SCHEDULE_SET<schedule_ist>END
SCHEDULE_SET<protocol_rule_set>
<protocol_header>::=<name>;<description>,<creator_detail>;<category>;
<schedule_ist>::=<schedule> | <schedule>;<schedule_list>
<schedule>::=SCHEDULE<schedule-header>;<entry_criteria>;<rule_list>END SCHEDULE
<protocol_rule_set>::=RULE_SET<rule_list>END RULE_SET;
<rule_list>:=<rule> | <rule>;<rule_list>
<rule>::=<dynamic_rule> | <static_rule>
<dynamic_rule>::= ECA rule
Fig. 3. The high-level BNF syntax of PLAN.
5 Case Study: TOPS and the Management of the
Microalbuminuria CPG for Diabetes Patients
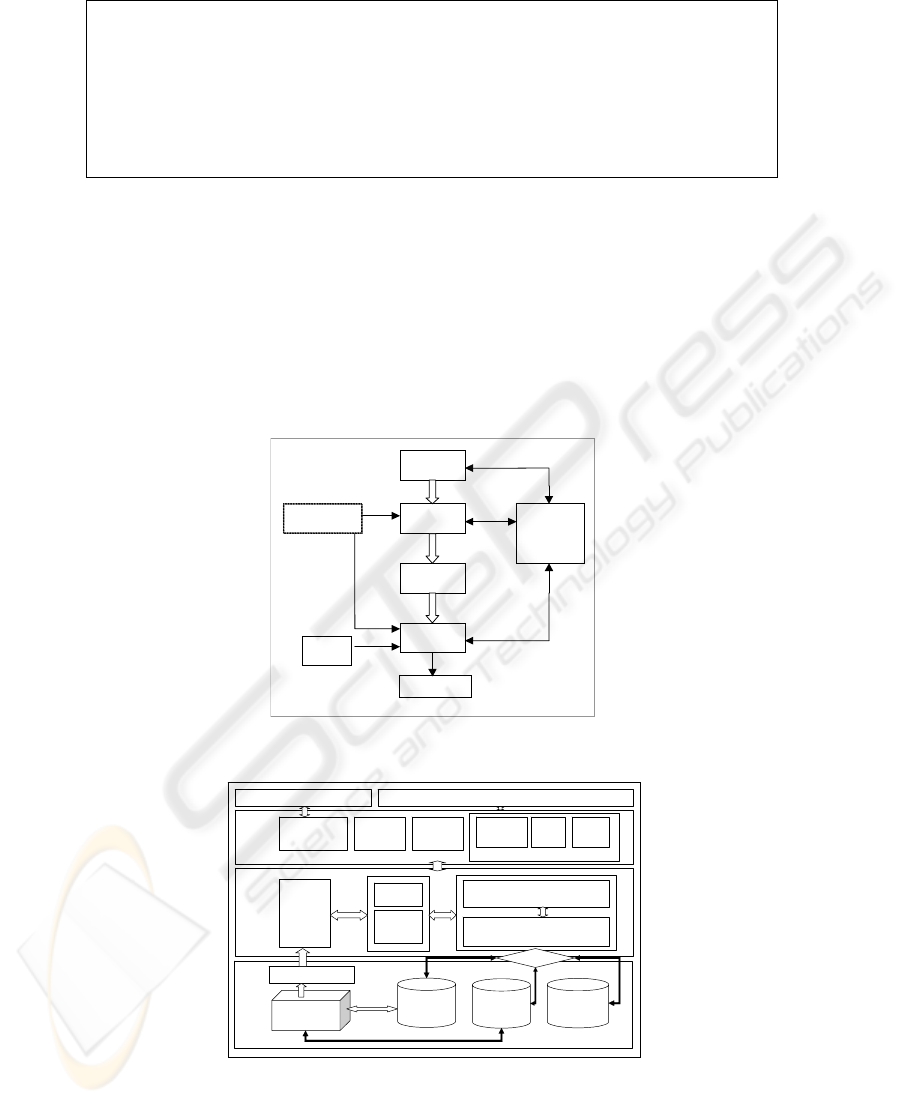
This section outlines the design of the proof-of-concepts system, TOPS, and a case
study in which TOPS is used to manage the CPG for microalbuminuria in diabetes
patients. Fig. 4 illustrates the generic CPG management method that is used in TOPS.
Specification
Phase
Customisation
Phase
Installation
Phase
Execution
Phase
Management
(querying &
modification)
P
atient Clinical
D
ata
Test
Results
Test orders, alerts,
alarms, etc
Category
p
rotocol specification
P
atient test
ordering plan
I
nstantiated patient
test plan
Fig. 4. The CPG Management Process for clinical protocols.
External
Communications
Module
Manipulation
Module
Specification
Module
Protocol
Management
Layer
Query
Module
Re-Play
Module
Instantiation
& Execution
Module
Management Components
External Systems Users
Database Access Manager
Rule Activity
Listener
Time Event
Generator
Dynamic SQL Generator
ECA Rule
Extension
Module
Execution Mechanism
and Database Access
Extension Layer
Rule Activity Notifier
Local
Patient
Record
Protocol
and Plan
Specifications
Plan
Execution
Logs
ECA
Mechanism
Protocol Execution
Engine (
DBMS)
DB Connectivity
External
Communications
Module
Manipulation
Module
Specification
Module
Protocol
Management
Layer
Query
Module
Re-Play
Module
Instantiation
& Execution
Module
Management Components
External Systems Users
Database Access Manager
Rule Activity
Listener
Time Event
Generator
Dynamic SQL Generator
ECA Rule
Extension
Module
Execution Mechanism
and Database Access
Extension Layer
Rule Activity Notifier
Local
Patient
Record
Protocol
and Plan
Specifications
Plan
Execution
Logs
ECA
Mechanism
Protocol Execution
Engine (
DBMS)
DB Connectivity
Fig. 5. Architecture of the proof-of-concepts system, TOPS.
111
In the specification phase, CPGs are formally represented and specified. Resulting
specification are stored in a database. The domain expert needs to be involved in this
process. In the customisation phase, the computerised CPG is customised to suit the
specific clinical problem suffered by the patient. This phase produces patient-specific
CPG specification instances as illustrated in Fig. 4. In the installation phase, all the
ECA rules in the CPG are added to the active database resulting in an active CPG
instance. In the execution phase, the execution process proceeds in accordance with
the ECA mechanism. The manipulation phase includes querying and manipulation
operations and permeates all the above phases. The architecture of TOPS has three
layers as illustrated in
Fig.
5. External to TOPS, are users and external systems. The top layer is the clinical
protocol management functionality for specifying, storing, executing, manipulating
and querying CPGs. The middle layer provides services that extend the ECA rule
execution mechanism of the underlying DBMS and handles database connectivity.
The bottom layer is the CPG execution engine as well as the system database, which
is currently based on the Oracle9i DBMS. The architecture provides support for the
three planes SpEM. Issues of concurrency and efficiency in rule execution are
handled by the Oracle9i DBMS with the exception of ECA rule extensions that are
implemented externally.
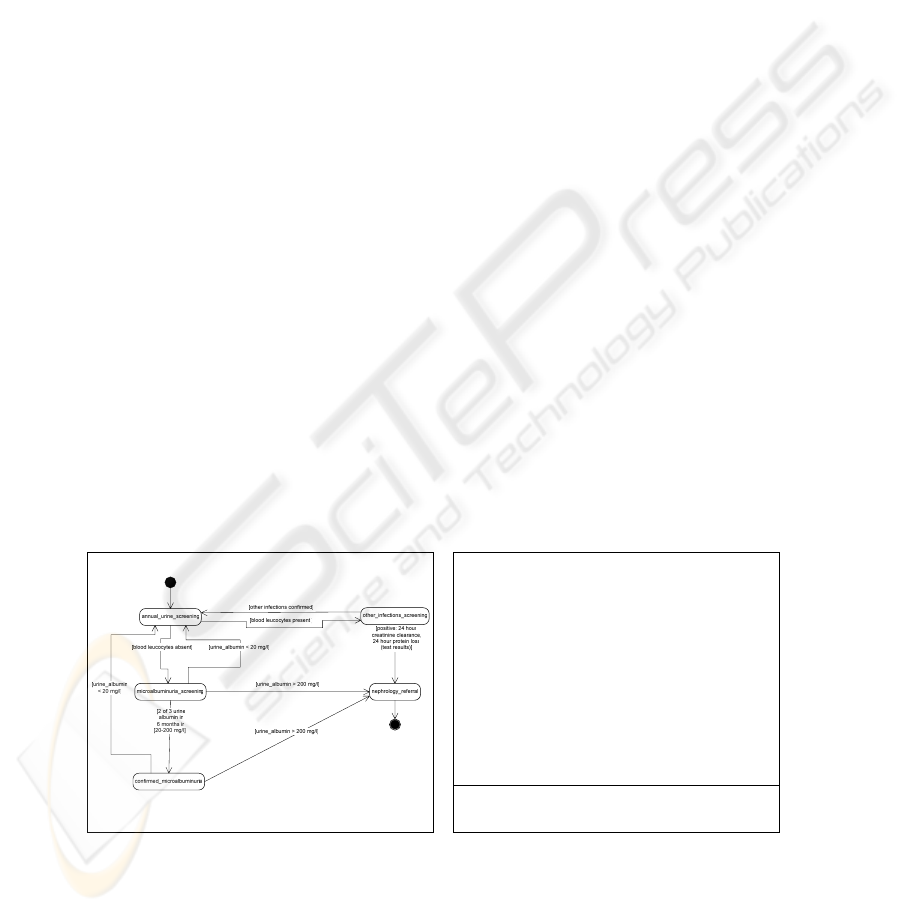
The SpEM framework in TOPS has been demonstrated through a case study
involving the CPG for the diagnosis and management of microalbuminuria (MA) in
diabetes mellitus as interpreted by a practising clinician at the local Diabetes Day
Clinic in Dublin. Fig. 6. illustrates the state chart for the microalbuminuria protocol
(MAP). For each state and its associated transitions, rules are designed to perform
what must be done when the patient enters, stays and exits from the state. Other rules
serve to trigger patient state transitions. Thus, the state chart guides creation of MAP
specification. Fig. 7. illustrates the outline structure and content of the resulting MAP
specification. The MAP specification used to create a patient plan when a user
requests the creation of a MAP instance for a specified patient. Patient plan execution
proceeds in an event-driven manner according to the set of ECA rules making up the
MAP instance. In the query illustrated in Fig. 8., a patient-specific MAP instance’s
snapshot at a given time or interval is retrieved. The MAP instance snapshot refers to
@PROTOCOL@ MAP;
DESCRIPTION: This is a protocol for the diagnosis and management of microalbuminuria in
diabetes patients;
CREATOR: DR JOHN NOLAN;
CATEGORY: DIABETIC_NEPHROPATHY;
#SCHEDULE_SET#
^SCHEDULE^ AUS, <AUS_rules> ^END SCHEDULE^
^SCHEDULE^ OIS, <OIS_rules> ^END SCHEDULE^
^SCHEDULE^ MAS, <MAS_rules> ^END SCHEDULE^
^SCHEDULE^ CMA, <CMA_rules> ^END SCHEDULE^
^SCHEDULE^ NPH, <NPH_rules> ^END SCHEDULE^
#END SCHEDULE_SET#
~RULE_SET~
STATIC_RULE AUS1,<body of rule AUS1>;
RULE OIS1,<body of rule OIS1>;
RULE MAS1,<body of rule MAS1>;
RULE CMA1,<body of rule CMA1>;
RULE CMA2,<body of rule CMA2>;
RULE CMA3,<body of rule CMA3>;
RULE CMA4,<body of rule CMA4>;
RULE NPH1, <body of rule NPH1>;
~END RULE_SET~
@END PROTOCOL@
Abbreviations:
AUS – Annual Urine Screening, OIS – Other-Infections Screening, MAS – MicroAlbuminuria
Screening, CMA – Confirmed MicroAlbuminuria, NPH – Nephrology referral
Fig. 6. State chart for the microalbuminuria
protocol.
Fig. 7. Structure of the Microalbuminuria
Protocol in PLAN.
112
the instance’s current state in terms of rule composition and the status of its rules at
that time or interval. The query illustrated in Fig. 9. provides information on what
tests were ordered with respect to the specified patient during the given time interval.
The term order in the query can be generalised to rule-action so that one can obtain
information on rule actions that have been performed during the specified time
interval. In this case study, the use of the highly intuitive UML state chart brings easy
communication with domain experts during CPG knowledge elicitation, capture and
specification. Subsequent extraction of the relevant ECA rules is also made easier
since the state chart naturally supports the ECA rule paradigm [22] and is also easily
understood by domain experts. The database offered a uniform and flexible way to
access, manipulate and query all information from specification, to executing process
state, to data in the patient record. The generation of SQL trigger code implementing
ECA rules of the MAP was automatically supported by TOPS and required minimal
intervention. This makes it easy for application domain experts to use TOPS with no
knowledge of the SQL trigger specification language. However, domain experts still
needed to be familiar with the specification language, PLAN, which is closer to their
domain language than the SQL. The execution of the rule actions was subject to the
availability of the appropriate software module that implements the action. Thus, rule
actions in the microalbuminuria CPG needed to be predefined and any new action
requires that the module to implement such an action be developed. However, rule
actions were designed to be generic and re-usable by other rules in other CPGs. Using
the database permits operations and queries on various aspects of the MAP through an
SQL-based manipulation language. It was shown that the MAP can be modeled and
specified by using the ECA rule paradigm guided by the state chart. This case study
demonstrated the applicability of the SpEM framework and the active database in
enabling the support for the management of the MAP for diabetes patients.
6 Summary and Conclusion
This paper has presented a unified CPG management framework, SpEM, for
computerized CPG management. The paper also presented a generic method with a
case study to harness the ECA rule paradigm and active databases to provide
computerized CPG support, by following the SpEM. Active databases combine the
ECA rule paradigm with data management to present a promising environment for
TOPS:\> query
QUERY:\> --->SELECT PLAN FROM SNAPSHOT WHERE TARGET:2005-7-19
01:55:02,2005-7-19 01:55:58; SOURCE:PATIENT_ID=25
processing query ...
…
PLAN [ PL$25$1$ ] SNAPSHOT @[2005-07-19 22:30:26.91]
[rule 1]--->[ 72, PL$25$1$AUS2, DYNAMIC, READY ]
[rule 2]--->[ 73, PL$25$1$AUS3, DYNAMIC, READY ]
[rule 3]--->[ 74, PL$25$1$OIS2, DYNAMIC, READY ]
[rule 4]--->[ 75, PL$25$1$OIS3, DYNAMIC, READY ]
[rule 5]--->[ 76, PL$25$1$OIS4, DYNAMIC, READY ]
…
[rule 19]--->[ 90, PL$25$1$CMA4a, DYNAMIC, READY ]
[rule 20]--->[ 91, PL$25$1$CMA4b, DYNAMIC, READY ]
[rule 21]--->[ 92, PL$25$1$NPH1, DYNAMIC, READY ]
[rule 22]--->[ 93, PL$25$1$main$AUS1, STATIC, EXECUTING ]
END SNAPSHOT FOR PLAN PL$25$1$.
QUERY:\> --->exit
TOPS:\>
TOPS:\> query
QUERY:\> --->SELECT ORDER FOR PATIENT WHERE TARGET:2005-7-16 17:48:30,2005-
7-16 17:51:25; SOURCE:PATIENT_ID=61
processing query ...
launching specialised query handler ...
processing ORDER query [ 2005-7-16 17:48:30,2005-7-16 17:51:25 ] for [ PATIENT ]
...
Tests ordered for [PATIENT_ID=61] during time interval [2005-7-16 17:48:30,2005-7-16
17:51:25]
Dip_stick_urine Profile, DSU, 2005-07-16 17:49:28.0
Urinary_Tract_Infection Profile, UTI, 2005-07-16 17:50:06.0
Urinary_Tract_Infection Profile, UTI, 2005-07-16 17:50:06.0
-------------------
End test listing.
QUERY:\> --->EXIT
TOPS:\>
Fig. 8. A query for a snapshot of the com-
position of a CPG instance in TOPS.
Fig. 9. A query to find out what clinical tes
t
orders where made during the specified time
interval.
113

supporting CGPs and their integration with the electronic medical record and clinical
workflow. This work contributes a generic approach with a framework to unify the
three CPG management dimensions and an active database method for computational
support. The benefits of the approach are: flexibility based on CPG information
management; ease of integration of CPGs with electronic patient records and clinical
workflows due to the active database approach; and ease of incorporation of CPG
management system into the healthcare systems due to ubiquity of database systems
within most institutions. Our future work will focus on: 1) finding ways to deploy and
evaluate the SpEM and TOPS in a real patient care setting without infringing on
confidentiality and proprietary license restrictions on APIs and schemas in existing
hospital systems; 2) improving our framework though enriched specification model
and language; 3) more efficient methods of exploiting and enhancing the active
mechanism by hybridising it with other paradigms; and 4) useful concepts and
methods for information manipulation, query and replay.
Acknowledgements
The Arnold F Graves Trustees and the Dublin Institute of Technology are gratefully
acknowledged for sponsoring this research work.
References
1. OpenClinical, The Medical Knowledge Crisis and its solution Through Knowledge
Management. 2001, OpenClinical.org.
2. Quaglini, S., Stefanelli, M., Cavallini, A., Micieli, G., Fassino, C., and Mossa, C.,
Guideline-based careflow systems. Artif Intell Med, 2000. 20(1): p. 5-22.
3. Pattison-Gordon, E., Cimino, J.J., Hripcsak, G., Tu, S.W., Gennari, J.H., Jain, N.L., and
Greenes, R.A., Requirements of a sharable guideline representation for computer
applications. 1996, Stanford University: Stanford, California, USA.
4. Widom, J. and Ceri, S., eds. Active Database Systems: Triggers and Rules for Advanced
Database Processing. 1996, Morgan Kaufmann: San Francisco, USA.
5. Dittrich, K.R., Gatziu, S., and Geppert, A. The Active Database Management System
Manifesto: A Rulebase of ADBMS Features. in 2
nd
Workshop on Rules in Databases
(RIDS). 1995. Athens, Greece: Springer.
6. de Clercq, P.A., Blom, J.A., Korsten, H.H., and Hasman, A., Approaches for creating
computer-interpretable guidelines that facilitate decision support. May. Artif Intell Med.,
2004. 31(1): p. 1-27.
7. Clayton, P.D., Pryor, T.A., Wgertz, O.B., and Hripcsak, G. Issues and Structures for
Sharing Medical Knowledge Among Decision-making Systems: The 1989 Arden
Homestead Retreat. in Annu Symp Comput Appl Med Care. 1989.
8. HL7, Arden Syntax for Medical Logic Modules., in Standards of the Health Level 7. 1999:
USA.
9. Caironi, P.V.C., Portoni, L., Combi, C., Pinciroli, F., and Ceri, S. HyperCare: a Prototype
of an Active Database for Compliance with Essential Hypertension Therapy Guidelines. in
AMIA Ann Fall Symposium. 1997. Philadelphia, PA: Hanley and Belfus.
114

10. Dube, K., A Generic Approach to Supporting the Management of Computerised Clinical
Guidelines and Protocols, PhD Thesis, in Computer Science. 2004, Dublin Institute of
Technology: Dublin. p. 324.
11. Gordon, C., Herbert, I., and Johnson, P. Knowledge Representation and Clinical Practice
Guidelines: the DILEMMA and PRESTIGE projects. in Medical Informatics Europe. 1996.
Copenhagen: IOS Press.
12. Musen, M.A., Tu, S.W., Das, A.K., and Shahar, Y., EON: A component-based approach to
automation of protocol-directed therapy. JAMIA, 1996. 3(6): p. 367-88.
13. Fox, J., Johns, N., Rahmanzadeh, A., and Thomson, R. PROforma: a method and language
for specifying clinical guidelines and protocols. in Medical Informatics Europe. 1996.
Amsterdam.
14. Ohno-Machado, L., Gennari, J.H., Murphy, S., Jain, N.H., Tu, S.W., Oliver, D.E., Pattison-
Gordon, E., Greenes, R.A., Shortliffe, E.H., and Barnett, G.O., The GuideLine Interchange
Format: A Model for Representing Guidelines. JAMIA, 1998. 5(4): p. 357-372.
15. Shahar, Y., Miksch, S., and Johnson, P., The Asgaard Project: A task-specific framework
for the application and critiquing of time-oriented clinical guidelines. Artificial Intelligence
in Medicine, 1998. 14: p. 29-51.
16. Johnson, P.D., Tu, S.W., Booth, N., Sugden, B., and Purves, I.N., A guideline model for
chronic disease management. 1999, Stanford Medical Informatics: Stanford.
17. de Clercq, P.A., Hasman, A., Blom, J.A., and Korsten, H.H.M., Design and implementation
of a framework to support the development of clinical guidelines. Int J Med Inf., 2001.
64(2-3): p. 285-318.
18. Terenziani, P., Molino, G., and Torchio, M., A modular approach for representing and
executing clinical guidelines. Artif Intell Med., 2001. 23(3): p. 249-76.
19. Quaglini, S., Stefanelli, M., Lanzola, G., Caporusso, V., and Panzarasa, S., Flexible
guideline-based patient careflow systems. Artif Intell Med, 2001. 22(1): p. 65-80.
20. Musen, M.A. Two decades of Models and Components: Why has Automation of Guideline-
Directed Care been so Difficult? in 1st European Workshop on Clinical Practice Guidelines
and Protocols (EWGLP 2000). 2000. Leipzig, Germany: IOS Press.
21. Wu, B. and Dube, K. PLAN: a Framework and Specification Language with an Event-
Condition-Action (ECA) Mechanism for Clinical Test Request Protocols. in 34th Hawaii
International Conference on System Sciences (HICSS-34): the Mini-Track in Information
Technology in Healthcare. 2001. Maui, Hawaii: IEEE Computer Society, Los Alamitos,
California.
22. Berndtsson, M. and Calestam, B., A Uniform Approach for Supporting Active Database
Features in UML and OMT. 2001, Computer Science Department, University of Skovde:
Skovde.
115
