
EMPOWERING PRIMARY HEALTH CARE SERVICES
THROUGH E-GOVERNANCE
A Case Study from Delhi Government
Rajan Vohra
Astt. Professor, Institute of Technology & Management, Gurgaon, India
Keywords: e-Governance, primary health care services, dispensaries, Delhi government.
Abstract: In the field of health care services the responsibility for their delivery is shared by many agencies in the
public sector. In addition there are central government ministries each with their own institutions. Each of
these agencies provides health care services in Delhi through a variety of outlets like dispensaries and
hospitals. These institutions function independently and there is neither proper coordination between the
government agencies managing them nor between the institutes themselves at the operational level. This
coordination is essential from the point of view of having a structured patient referral system and sharing of
resources between institutes in addition to providing feedback to shape government health policies. In this
research paper the study focuses on primary health service centres of Delhi Government. The research
objectives of this paper are:
• Study the working of Primary health centres including services provided.
• Study the level of IT usage in these dispensaries
• Analyze key problems faced by these dispensaries
• Propose an e Governance model to manage these dispensaries
• Determine obstacles & challenges in implementation of this model.
This research paper uses some technologies that are being used by National health services (NHS) of UK.
These technologies include use of call centers for service delivery and Decision support systems (DSS) that
are being used in patient interaction.
1 INTRODUCTION
Delhi is an old city and has slowly expanded over
the years to acquire its present status of a big
metropolis. As per the census of 2001 Delhi with an
area of 1483 sq km has a population of 137 lakhs
with a population density of 9294 persons per sq km,
which is the highest of India. In this population only
7 % are residing in rural areas making it a total
urban city. About 35 % of Delhi’s population lives
in slums. According to the projections of Registrar
General of India on 1
st
march 2005 the population of
Delhi was 15.6 million and is expected to reach 25
million by 2020.
The release of land for providing housing and
health infrastructure has not matched with the
growth of the city. As a result health infrastructure
of Delhi is inadequate in respect of actual needs.
In Delhi health care facilities are being provided by
both governmental and non governmental
organizations. Among the Government organizations
the Directorate of health services (DHS) is a major
service provider in the health sector. This directorate
participates in delivery of health care services, and
coordinates with other government and non
government organizations to provide health care to
Delhi’s citizens The DHS also coordinates and
monitors various health programs of state and
national importance.
The DHS provides health care facilities at primary
and secondary level through a chain of health outlets
like dispensaries and hospitals. The DHS is
providing primary health care services through a
chain of 180 allopathic dispensaries. The DHS
constantly monitors delivery of its programs by
collecting data regularly from its dispensaries. In
addition this directorate collects data on public
221
Vohra R. (2007).
EMPOWERING PRIMARY HEALTH CARE SERVICES THROUGH E-GOVERNANCE - A Case Study from Delhi Government.
In Proceedings of the Third International Conference on Web Information Systems and Technologies - Society, e-Business and e-Government /
e-Learning, pages 221-227
DOI: 10.5220/0001268502210227
Copyright
c
SciTePress

health and communicable diseases for analysis and
required action.
The health centres under DHS are its frontline
health outlets capable of providing health promotion,
health protection and treatment of various ailments
to the community. The vision of DHS is to promote
these health outlets as the backbone of health
services and overall health development with a view
to actively involve these outlets in bottom up
planning. The Planning branch of DHS is
responsible for planning the development of primary
health services including monitoring the functioning
of existing centres. The state of Delhi is divided into
8 districts with each district being headed by a Chief
District Medical Officer (CDMO). Each district has
its own chain of dispensaries.
In the UK, the NHS has used some key
technologies like call centers for patient interaction
and Decision support systems which are assisting in
this. The delivery model proposed also makes use of
nursing staff managed call centers and information
kiosks. The nurses are assisted by an online Decision
support system for patient counseling.
According to the NHS web
link:http://www.nhsdirect.com/aboutnhsdirect.html
enables a patient to search for the nearest doctor,
dentist, optician, pharmacies and hospitals including
a map search facility. The NHSDIRECT online is a
help line supported by a 24 hour nurse advice and
information help line. It can prescribe treatments for
common health problems by using a body key and
identifying symptoms by asking patients simple
queries. It has information on over 700 topics
covering tests, illnesses, treatment and operations. A
patient can also enquire about something by filling
an online form and the query is answered within five
days by a qualified professional. It has a searchable
database of doctors, hospitals, pharmacies and other
health care services.
According to (Kannabiran, 2004) citizen
relationship management (CZRM) is about
reorienting service operations of government around
citizens instead of administrative processes. The
core of a new e Government paradigm is to
transform customer relationships along with
processes and mediums that support them. E
Governance efforts need to be backed by end to end
process reengineering with citizen centric strategies.
The concept of Decision support systems(DSS)
along with its role and benefits in the practice of
General practitioners in UK has been discussed by
(Thornett, 2001). A rule based Decision support
system is being used in NHS Direct service,
launched in 1998, which is a 24 hour medical
telephone helpline, staffed by nurses. It provides
health care advice in out hours and saves the cost of
employing doctors in running its day to day services.
The sharing of information on Decision support
systems between General practitioners of NHS is
expected to improve the quality of health care in
primary health care services of the NHS in UK.
2 RESEARCH METHODOLOGY
A random sample size of 32 was selected out of 180
dispensaries by random sampling. A physical survey
was undertaken in each dispensary to count average
daily attendance and number of patients with access
to internet and telephone. A team of 4 surveyors
studied this count spending 5 days in each
dispensary with one day’s duration equal to 6 hours.
The entire survey was completed in 2 months by this
team in the year 2006. Also the functioning of
dispensaries was observed by study visits to all 32
dispensaries. The web site of Delhi government was
also studied for analysis and determining the on line
presence for dispensaries. In the same survey the
level of IT usage in each dispensary was determined.
The access of 56 doctors in these 32 dispensaries to
internet and mobile phones was also determined.
3 RESULTS AND DISCUSSION
3.1 Statistical Analysis
According to the annual report of (Directorate of
Health services, Government of Delhi, 2004-05), the
statistics for dispensaries for the last 7 years are
given in the table below:
Table 1: OPD attendance data in dispensaries.
YEARS(x) OPD
ATTENDANCE(y)
NO OF
DISPENSARIES(z)
1998-99 3682813 139
1999-2000 3823689 139
2000-01 6381712 155
2001-02 7032010 167
2002-03 7347775 171
2003-04 8550673 173
2004-05 9784722 179
Performing correlation between years(x) and
annual OPD attendance(y), we obtain the correlation
coefficient as r(x,y) = 0.976
WEBIST 2007 - International Conference on Web Information Systems and Technologies
222
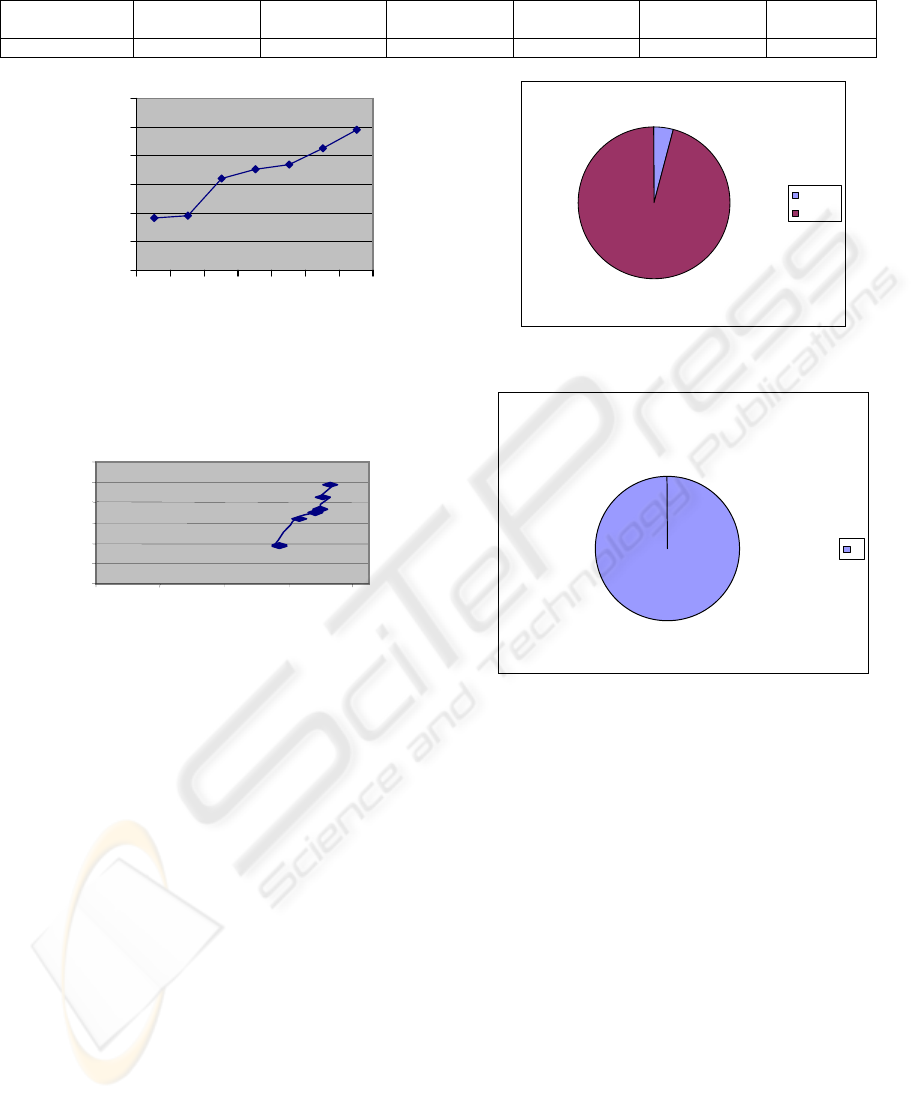
Table 2: Data showing IT usage in dispensaries.
Dispensaries Telecom
facility
No of
telephones
No of
computers
Internet facility Technical staff Website
32 nil 32 nil nil Nil Nil
0
2000000
4000000
6000000
8000000
10000000
12000000
1234567
Years
OPD attendance
Figure 1: Graph between years and OPD attendance.
Figure 2: Graph between OPD attendance and number of
dispensaries.
The Figure 1 between OPD attendance and
years along with the Figure 2 between OPD
attendance and number of dispensaries are shown
above.
Now, performing regression analysis between
OPD attendance(y) and number of dispensaries (z),
the following regression equation is obtained:
z = 113.61 + 0.7032 y (1)
Applying this equation, we obtain:
If y = 110, z = 191.
If z = 200, then y = 122.85(in units of 100,000).
4%
96%
internet
no net
Figure 3: Internet access in patients.
phone
100%
1
Figure 4: Telephone access in patients.
In the above figures it can be seen that out of a
total of 6800 patients surveyed in 32 dispensaries,
only 287 have access to internet either at home or in
a public cyber café while all 6800 surveyed have
access to a telephone either self, mobile, or a public
phone, which means that just over 4 % have access
to internet while 100 % have access to a telephone.
This is an important result for determining the most
effective medium for delivery of health care services
in dispensaries.
3.2 IT Usage in Dispensaries
We can infer from the above table 2 that none of the
32 dispensaries surveyed is computerized nor do
they have any technical staff. No dispensary
surveyed has internet facility.
Among the doctors surveyed in these 32
dispensaries it is found that out of a total of 56
doctors working in these 32 dispensaries, 34 doctors
0
2000000
4000000
6000000
8000000
10000000
12000000
0 50 100 150 200
N
o of dispensaries
OPD
EMPOWERING PRIMARY HEALTH CARE SERVICES THROUGH E-GOVERNANCE - A Case Study from Delhi
Government
223

are active users of internet and use it for professional
development even though no dispensary is having
any provision for internet facility. Thus about 60 %
of the doctors surveyed were familiar with internet
usage. Also all 56 doctors were having their own
mobile phone or 100 % of doctors surveyed had
access to their own mobile phones. This result can
be used while developing a model for delivery of
health care services in the next section of this paper.
However despite the lack of computerization the
web site of the health department of the Delhi
government at http://health.delhigovt.nic.in gives a
listing of dispensaries under DHS. This listing can
be obtained district wise also. It gives the address
and phone number of each dispensary. However the
map search facility in which one can open the profile
of each dispensary in a district does not function.
The resources in these health outlets like number of
doctors and diagnostic services provided are not
displayed for any dispensary. Even these details are
meaningless for more than 90 % of patients as they
lack access to internet and are unable to view this
information. In fact in our study over 32 dispensaries
only 4 % of patients were having internet access.
Therefore an alternative delivery mechanism needs
to be constructed.
3.3 Other Findings
These findings were obtained through personal study
visits to these 32 dispensaries in which their
functioning was studied. They can now be tabulated
as follows:
1. OPD timings: All dispensaries opened
between 8 am and 2 pm. Thus there was no
off hours support for patients.
2. There was a need for specialist doctors
visits to dispensaries on a regular basis as
these are managed by only General
practitioners.
3. Referral of patients is unidirectional and
no track of referred patients is kept. A
record of referred patients is kept in the
dispensary only for government employees
and not for general patients.
4. No contact between dispensary and
secondary hospital at point of referral.
5. A patient does not know which ailments
can be treated at the dispensary level. Even
for common ailments they are reaching
hospitals instead of first visiting the local
dispensary.
6. There is no medical records department in
these dispensaries and monthly reports are
compiled manually and carried by hand by
a Nursing orderly(NO) to the district
CDMO office. As a result previous year’s
statistics are not properly maintained at the
dispensary level.
7. The notification of infectious diseases is
done by the Dispensary MO by telephone
or through written document which is
again carried manually to the District
CDMO office.
8. The process of consultation with other
doctors by doctors from the dispensary is
done through their personal mobile phones
/ land phones and there is no official
facilitation for this process.
9. No separate space/ counter for OPD
registration exists in dispensaries and is
being done in the open space leaving
patients exposed to infectious threats like
TB from such patients who also visit these
dispensaries.
10. The dispensaries offer only basic lab tests
like urine, stool, and blood sugar, because
of lack of equipment like auto analyzer .A
patient who has to be tested for more tests
is referred to hospitals.
11. The present working strength of staff in a
dispensary indicates a shortage of
manpower like doctors, pharmacists and
the lab technician. As an example a
dispensary with one doctor faces a
problem if this doctor is on leave.
Similarly in a dispensary with 2 doctors if
one doctor is absent full patient load comes
on the single doctor. The same reasoning
applies to the working of pharmacists (2 in
a dispensary) and the single lab technician.
Thus there is no manpower back up to deal
with these situations.
12. The referral of patients from a dispensary
is occurring because of lack of more
diagnostic facilities in the pathology lab,
lack of X RAY machine, absence of
specialist doctors visits, lack of ultrasound
facilities, and ECG machine.
4 THE PROPOSED
E-GOVERNANCE MODEL
The present administrative hierarchy in dispensaries
is as follows:
WEBIST 2007 - International Conference on Web Information Systems and Technologies
224
DHS
DISTRICT CDMO
MO (DISPENSARY IN CHARGE)
Accordingly to support this structure the ICT
infrastructure for each district can now be designed.
This infrastructure will support the proposed e
Governance model.
In effect this categorization produces a hub and
spoke model in each district at the primary level.
This model can be used in:
• Load balancing: Redirection of patient flow
to balance patient loads within a district.
• Manpower planning: Plan deployment of
medical staff for Hub and for spokes.
• Equipment planning: Plan deployment of
medical equipment like x ray machines in
hub and spokes.
As an example we can show how load balancing can
be achieved.
We assume a OPD slot of 6 hours per day and 5
minutes per patient per doctor. Therefore a
dispensary with 1 doctor has a capacity of 12
patients per hour or 72 patients per day for a slot of
6 hours. Excess load for a dispensary is Present load
– Capacity. Then total excess load in the network
can be calculated as 724.
The Hub is selected to absorb all excess load
transferred from the spokes while by design the
spokes are constrained to their capacity. The Hub is
selected according to load(volume) . So the center
with the highest load i.e. dispensary e is the hub.
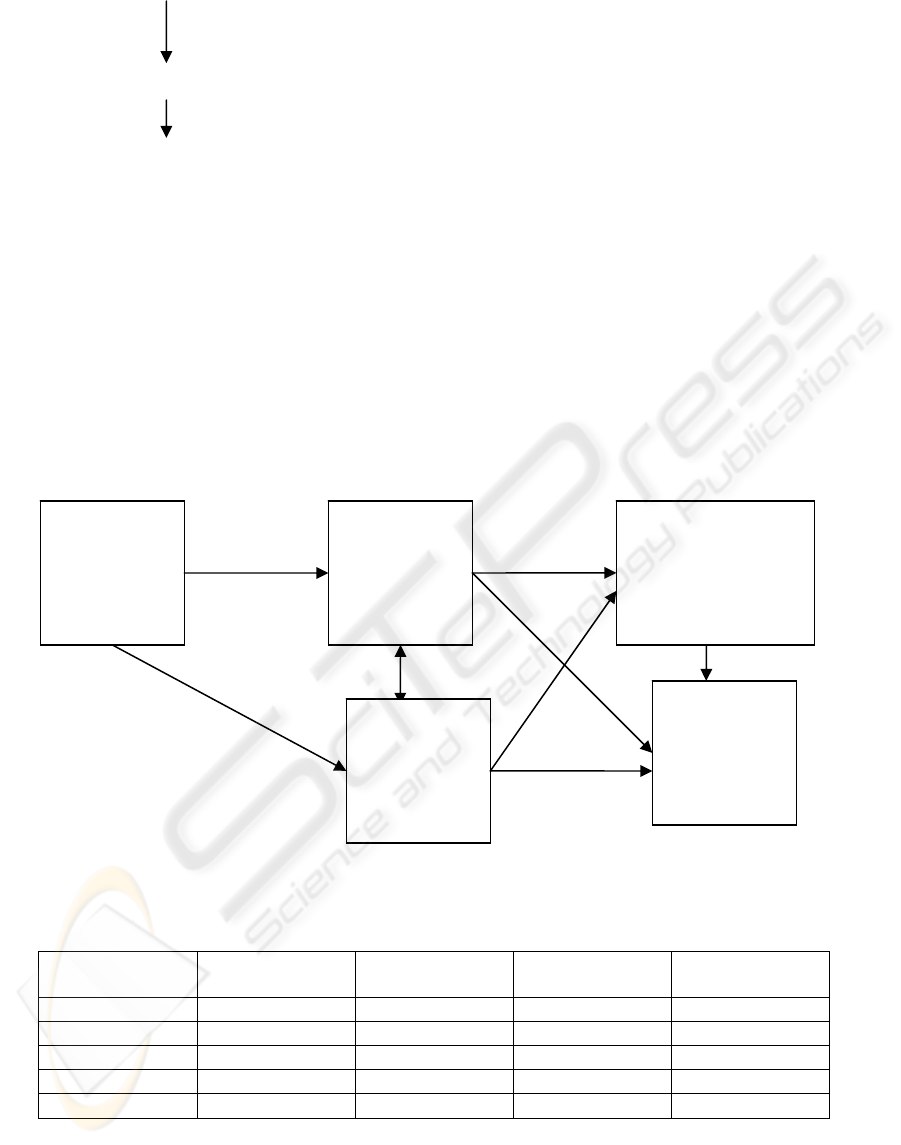
Figure 5: The proposed e Governance model.
Table 3: Hub and Spoke model input.
Name of
dispensary
No of Doctors Present load/day Capacity of
dispensary
Excess load
A 2 200 144 56
B 1 150 72 78
C 2 250 144 106
D 1 300 72 228
E 2 400 144 256
PATIENT
DISTRICT
CALL
CENTRE
INFORMA
TION
KIOSKS
DISTRICT
REFERRAL
DISPENSARY
OTHER
DISTT
DISPENS
ARIES
EMPOWERING PRIMARY HEALTH CARE SERVICES THROUGH E-GOVERNANCE - A Case Study from Delhi
Government
225
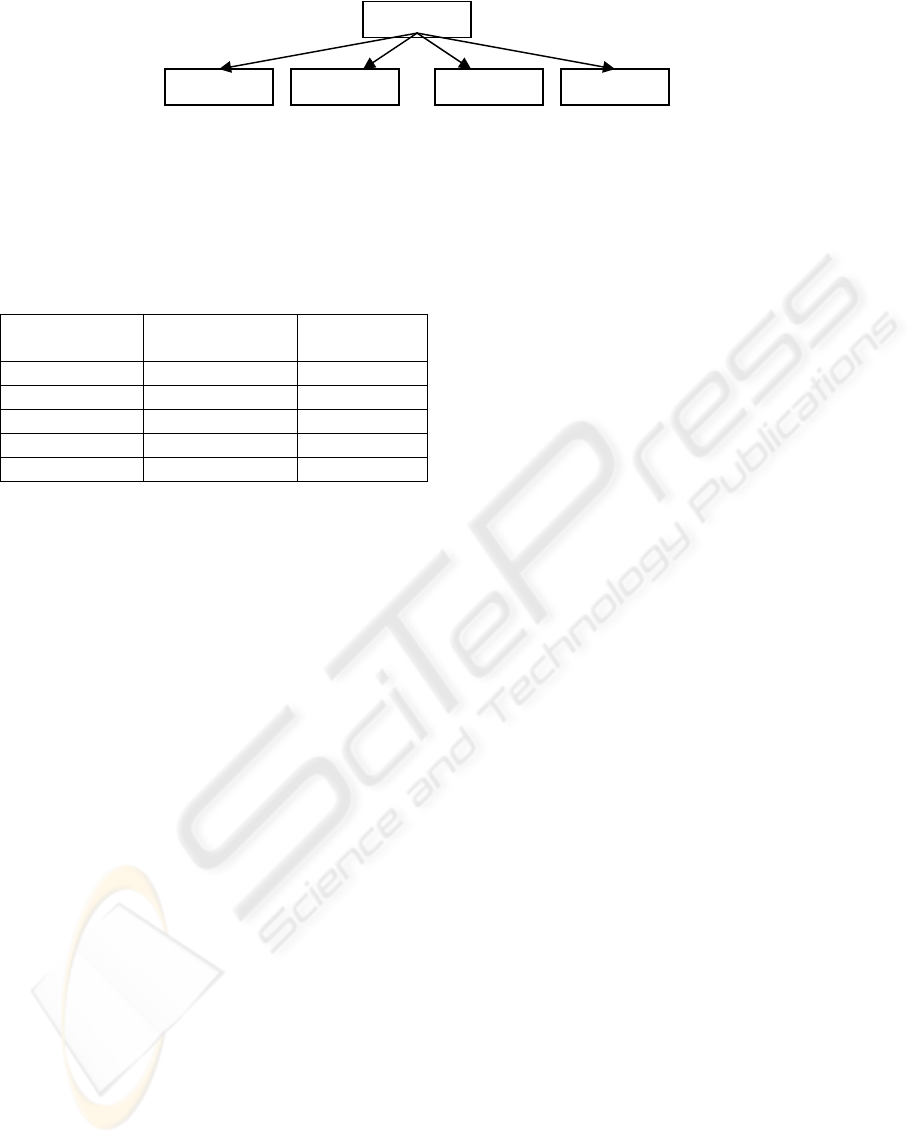
Spokes
Figure 6: Generation of Hub and Spokes.
This results in a hub and spoke model.
The new load distribution can now be calculated as
follows:
Table 4: New load distribution using hub and spoke
model.
Name of
dispensary
New loads on
dispensary
Number of
Doctors
A 144 2
B 72 1
C 144 2
D 72 1
E 724+144= 868 12
The number of Doctors needed in Hub (E)
is therefore 12. The health care managers can also
choose 2 hubs for a district, in which case the
dispensary with second highest load i.e. D (300)
becomes the second hub. In this case both hubs
share the total excess load transferred from the
spokes equally. The hubs can also be chosen
according to the distances between the dispensaries.
The Decision support system is thus model driven
and must have the capability of performing this load
balancing analysis along with manpower and
equipment planning using the same hub and spoke
model. The Hub and spoke model facilitates the
following:
• Decentralization of health care services by
forming hub and spoke models in the
districts.
• Regionalization of health care services:
This is done by directing patients to the
nearest region (district).
• Minimizing referral to secondary care
services in the district: This is done by
strengthening the hubs by providing more
manpower and equipment at the hubs.
Once a hub and spoke model is created ,
further requests for patient servicing can be satisfied
by : The present hub or its spokes(if they have free
capacity). However if the present network is full, the
requests for patient servicing must be redirected to
the nearest hub and spoke network. Again search is
performed in that network to verify if the request can
be satisfied by the hub or by its spokes.
This model proposes to set up a District
Call centre in each of the eight districts of Delhi.
This call centre will be linked to a network of
information kiosks. The delivery of health care
services in a district will now be routed through this
ICT infrastructure. In addition, one out of the
dispensaries in a district will be designated as
DISTRICT REFERRAL DISPENSARY. This
dispensary will be provided with equipment and
services that are currently lacking in a dispensary. In
particular this dispensary will be equipped with X
RAY machines, ECG machines, ultrasound facility,
and Auto analyzer for advanced pathological testing.
This dispensary will be equipped with Telemedicine
links to other dispensaries and to hospitals in the
district which will facilitate consultation between
General practitioners managing a dispensary and
specialist doctors working in hospitals in the district.
This will benefit such patients visiting a dispensary.
This removes the need to employ specialist doctors
for the referral dispensary as also for the other
district dispensaries.
The call centre in a District will be manned not
by ordinary call centre employees but with nurses.
This will be a 24hours help line. This will support
patients through the day. The nurses are supported
by an Online Decision support system which will
help them provide on line counseling to calling
patients for common ailments as well as for other
queries about the health system .It will help maintain
an online database of patients so that those patients
visiting dispensaries can be supported in off hours
through medication advice and counseling. This ICT
infrastructure will provide the following services:
• E Registration: online registration of OPD
patients visiting the dispensary.
• E pharmacy: The information kiosks
become mini pharmacies and dispense
medicines to repeat patients.
• The information kiosks and call centre
regionalize health care services in a district
by advising patients to visit the nearest
dispensary in the district.
• The District Referral dispensary becomes
the telemedicine hub for districts and links
to hospitals in the district.
E
(
hub
)
A B C D
WEBIST 2007 - International Conference on Web Information Systems and Technologies
226

• The Dispensary must be made the first
point of contact for all patients except
emergency patients. This will prevent
patients with common ailments from
directly visiting hospitals.
• All district dispensaries can have a common
website putting details of resources on line.
• Dispatch of all monthly reports by
dispensaries can be made online.
• Notification of infectious diseases is made
online.
• Online consultation groups for doctors
working in dispensaries. Computerization
of dispensaries should proceed in parallel
with this ICT infrastructure.
• Since 100 % doctors possess mobile
phones, they can use them to access the call
centre and this facility can be provided to
patients too.
• In order to monitor working of a dispensary
hospital managers must have access to an
Online DSS which can make predictions
about different resources required based on
the number of patients visiting the
dispensary. This will facilitate online
decision making and help health planners in
planning for new dispensaries.
5 CONCLUSIONS
• There is no computerization existing in
dispensaries
• Dispensaries lack resources of manpower and
equipment.
• Dispensaries can be empowered through e
Governance and a supporting ICT infrastructure.
• Telemedicine can be used to avoid employing
specialist doctors in dispensaries.
• Call centers and information kiosks broaden
access to patients as 100 % patients have access
to a telephone.
• A purely web based model is inadequate to
provide health care services to citizens. It has to
be a mix of Web, call centers, information
kiosks, radio and television.
• A separate department of IT needs to be set up in
the health department to make long term plans
and ensure coordination between different stake
holders. The department is presently dependent
on external IT vendors which reduces its
capacity to sustain the technology.
• The process of patient referral needs to be made
structured and bi directional between hospitals
and dispensaries.
• The District referral dispensary will reduce
patient load on hospitals while reducing referrals
from dispensaries. By using Telemedicine links
it gives access to specialist doctors to those
patients who need their services but are remotely
located from them.
• The ICT infrastructure further reduces load on
dispensaries by distributing services like OPD
registration and pharmacy.
REFERENCES
Kannabiran G, ‘Enabling e Governance through citizen
relationship management – concept, model and
applications’, Journal of services research, vol 4 no 2,
pages 223-240, oct 2004- march 2005.
Thornett Martyn Andrew, ‘Computer decision support
systems in general practice’, International journal of
information management, vol 21, issue 1, pages 39-47,
February 2001.
Annual report, Directorate of health services, Government
of Delhi, 2004-05,p3
EMPOWERING PRIMARY HEALTH CARE SERVICES THROUGH E-GOVERNANCE - A Case Study from Delhi
Government
227
