
INTERACTION OF TECHNOLOGICAL AND INSTITUTIONAL
CHANGE IN THE DEVELOPMENT OF AN ELECTRONIC
COMMERCE SYSTEM IN CHINA’S PHARMACEUTICAL
DISTRIBUTION CHAIN
A Transaction Cost Perspective
Kai Reimers
Faculty of Business and Economics, RWTH Aachen University, Johanniterstr. 22-24, 52064 Aachen, Germany
Mingzhi Li
School of Economics and Management, Tsinghua University, 100084 Beijing, P.R. China
Keywords: Electronic commerce, pharmaceutical industry, transaction costs, institutional change.
Abstract: In this paper, we describe the introduction of electronic commerce into the drug distribution industry in
China. This case is especially interesting because massive institutional changes coincide with the introduc-
tion of a new technology. For these reasons, it becomes possible to study the interaction of technological
and institutional change in real time and in their real-life context. We use two alternative transaction cost-
theoretic perspectives on the interaction between institutional and technological change as our theoretical
framework. The case study suggests that the rationale which motivates introduction of a new technology in
the context of institutional change may be different from the rationale which underlies the practices which
develop on the basis on the newly introduced systems and institutions.
1 INTRODUCTION
Studying the interaction of institutional and techno-
logical change in real time is generally a difficult
endeavour because of the slow speed at which insti-
tutions typically change. For this reason, scholars
have focused on two empirical strategies, namely
historical studies with respect to large-scale institu-
tional changes, usually on the national level, and
studies of institutional change on the level of indi-
vidual companies (where institutions are changed
more easily and thus more quickly). Prominent rep-
resentatives of these two approaches are Alfred
Chandler and Oliver Williamson respectively.
Large-scale institutional changes become visible
only after a substantial period of time has elapsed so
that only historical analysis is feasible; studies on
the level of individual organizations such as firms
can only reveal small-scale institutional changes.
While both approaches have yielded impressive re-
sults, studying the interactions between institutional
and technological changes on an intermediate level
in real time would be desirable for the following
reason. While institutions exist on multiple levels so
that institutional change can also be studied on mul-
tiple levels, new technological systems are generally
not developed on both the national scale and the
level of individual firms but on intermediate levels.
This is because development of new technological
systems typically requires the cooperation among
several organizations, not only because resources
and capabilities of individual organizations are too
limited but also because application of new systems,
at least in the initial stages, requires close coopera-
tion of users and suppliers who are thus actively
involved in the design and development process
(von Hippel, 1978).
However, institutional changes occurring on the
intermediate level are seldom observable in real time
because of the slow speed of institutional change on
this level. One exception to this rule can be found in
fast developing countries which actively experiment
with medium-scale institutional changes. China may
be the most interesting and relevant context in this
regard and within China, the healthcare sector is the
3
Reimers K. and Li M. (2008).
INTERACTION OF TECHNOLOGICAL AND INSTITUTIONAL CHANGE IN THE DEVELOPMENT OF AN ELECTRONIC COMMERCE SYSTEM IN
CHINA’S PHARMACEUTICAL DISTRIBUTION CHAIN - A Transaction Cost Perspective.
In Proceedings of the First International Conference on Health Informatics, pages 3-12
Copyright
c
SciTePress

one which currently receives the most attention by
policy makers due to its economic as well as social
and political importance.
Theoretically, the interaction between technical
and institutional change has been addressed from a
number of perspectives, including transaction cost
theory. However, as North and Wallis (1994) have
shown, existing institutional approaches -- including
those by Chandler and Williamson -- only consider
institutional change as a passive response to techni-
cal change. North and Wallis trace this traditional
limitation back to an assumption that transaction
costs cannot be observed or measured which has
prevented scholars from appreciating an important
mechanism through which technical change can also
contribute to proactive institutional change. Ac-
cording to North and Wallis, in this tradition it is
generally assumed that new technology requires
institutional adaptation in order to be implemented
which, however, will increase unit transaction costs
even though the transaction cost minimizing institu-
tional arrangement will be chosen. In contrast, if one
accepts that transaction costs can be empirically ob-
served, one will be naturally led to look for those
parts of the economy which directly express the
level of transaction costs existing in an economy at
any given moment in time. North and Wallis have
identified this sector as the ‘transaction sector’ and
used it to measure the existing level of transaction
costs in an economy (Wallis and North, 1986). By
this approach they can show how institutions can be
changed proactively as a result of a lowering of unit
transaction costs through technical change. Thus,
North and Wallis demonstrate two ways in which
technical change can lead to institutional change: (1)
in order to accommodate the requirements of a new
technology, new institutions may have to be created
which, however, increase unit transaction costs in an
economy; since transformation costs are lowered
simultaneously (through technical change), the over-
all effect can still be beneficial; (2) technical change
can lower unit transaction costs and thus enable the
creation of new institutional forms.
In this paper we want to explore this dual rela-
tionship using the case of a massive institutional
reform of the distribution of drugs in China which
coincided with the rise of e-commerce and led to a
new way of selling and distributing drugs in which
both elements of institutional and technological
change are intertwined. We want to investigate to
which extent emergence of this new structure fol-
lows the Williamson-Chandler pattern -- new tech-
nology needs new institutional forms which result in
higher unit-transaction costs -- and to which extent it
can be explained as a result of transaction-cost re-
ducing technological change according to North’s
framework.
2 THEORETICAL FRAMEWORK
Transaction cost economics takes the transaction as
its unit of analysis and therefore operates on an
analytical level suitable for studying technological
change affecting interaction among economic
agents. Williamson (1993) has used a three-layer
model to locate and motivate the analytic strategy of
transaction cost economics. The focal layer concerns
the governance of transactional relationships which
is influenced by factors residing on a macro and a
micro layer. On the macro layer, institutions such as
contract law, property rights and norms and customs
affect the comparative costs of governance. Changes
on this layer may therefore lead to adjustments of
governance structures as some forms of governance
become relatively more cost advantageous while
others become more costly. On the micro-level, be-
havioural traits of individuals influence governance
forms. Prominent among them in Williamson’s
analysis are opportunism and bounded rationality.
For example, governance forms need to prevent
economic agents from exploiting one another should
the possibility for such behaviour arise due to unan-
ticipated changes in the economic environment.
While Williamson has not specifically developed
his transaction cost-theoretic framework for the pur-
pose of analysing its impact, technological change
can be relatively easily incorporated into this
framework through the notion of asset specificity.
This notion refers to investments the value of which
depends on the identity of one’s business partners.
As a consequence of such investments, one can be-
come hostage to threats by that business partner to
break up a business relationship. Specially designed
governance forms need to anticipate and accommo-
date this situation. While creating these special gov-
ernance forms is costly -- increasing unit transaction
costs -- creating them can still be worthwhile since
these governance forms allow for degrees of asset
specificity which, in turn, may reduce transforma-
tion costs substantially. There are several types of
asset specificity such as specificity of location, hu-
man skills and machinery. For example, locating
one’s production facilities close to one’s customer’s
own production facilities may allow for superior
logistical organization (such as Just-in-time delivery
arrangements) which, however, creates a substantial
degree of asset specificity since the value of that
investment would be much reduced if the customer
would sever the business relationship. Technological
change can then be incorporated as investments in
new machinery. Since initially such innovative ma-
chinery still follows proprietary or unproven de-
signs, it may well be tailored to the specific needs of
one business partner and therefore increase the de-
HEALTHINF 2008 - International Conference on Health Informatics
4
gree of asset specificity in a business relationship.
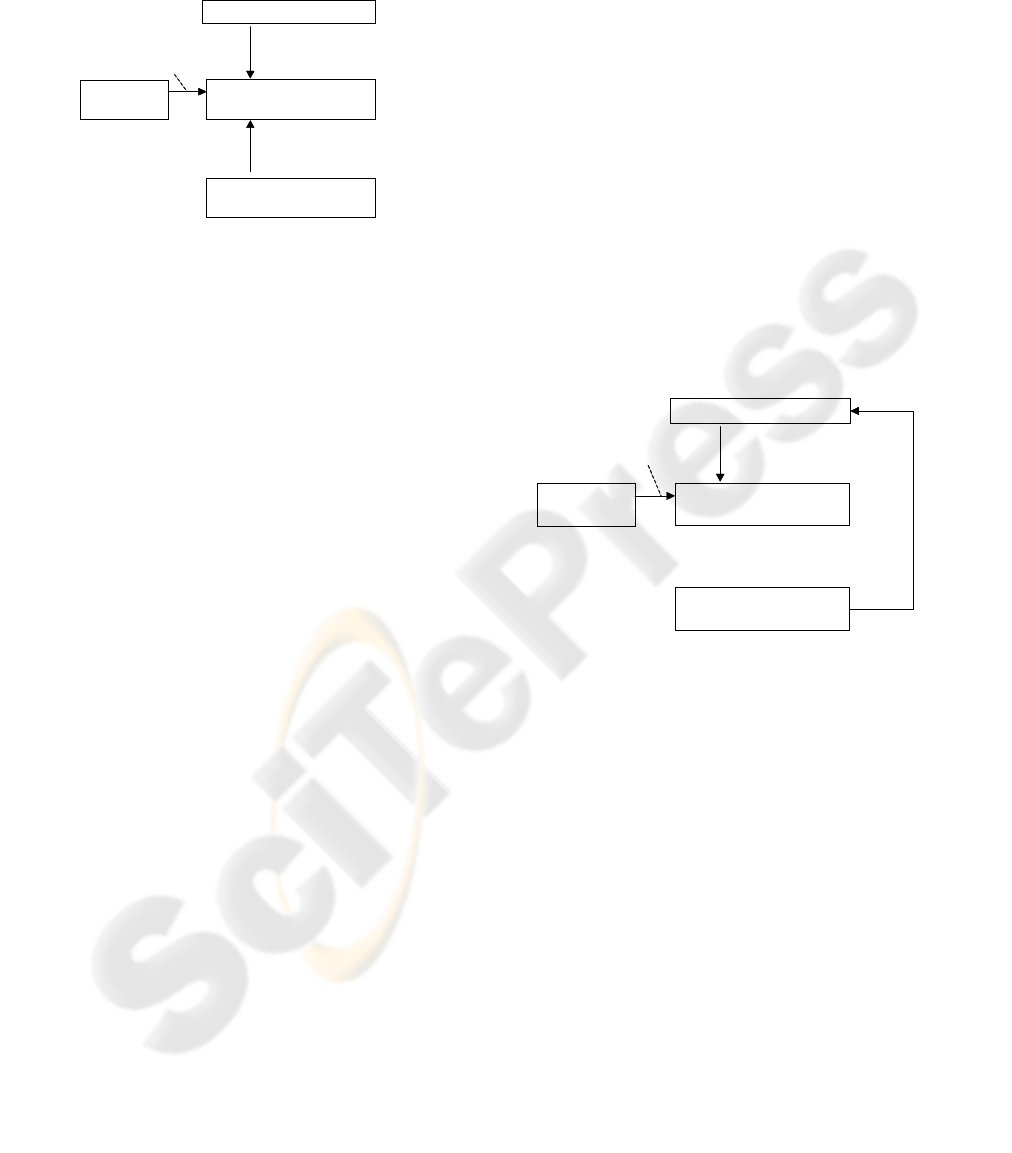
These concepts are summarized in Figure 1 which
extends and slightly modifies a figure presented in
Williamson (1993).
Institutional environment
Governance of
transaction relationship
Behavioural
assumptions
New
technology
Contract law, property
rights, customs etc. affect
comparative costs of
governance
Asset specificity
requires dedicated forms of
governance, thus increasing
unit transaction costs
Opportunism and bounded
rationality make governance
necessary
Institutional environment
Governance of
transaction relationship
Behavioural
assumptions
New
technology
Contract law, property
rights, customs etc. affect
comparative costs of
governance
Asset specificity
requires dedicated forms of
governance, thus increasing
unit transaction costs
Opportunism and bounded
rationality make governance
necessary
Figure 1: Technological change in a Williamsonian
framework (modified from Williamson (1993) excluding
feedback and indirect effects and adding the effect of new
technology).
The Northian framework combines elements of
neoclassical economic theory and transaction cost
economics. North is not directly concerned with
explaining or describing forms of governance but
rather analyses development of macro entities such
as whole economies/societies or sectors within one
economy. In order to compare his approach to that
of Williamson and to make it relevant for our analy-
sis, it therefore needs to be ‘mapped’ onto the trans-
actional level. In North’s (1990) framework forms of
governance are treated as behaviour of organizations
on economic markets which is influenced by formal
and informal institutions through affecting levels of
transaction costs (organizations are the players, in-
stitutions are the rules of the game). Some organiza-
tions engage in the production of new knowledge
which, if incorporated into products, becomes tech-
nological change on economic markets. In addition,
some organizations also engage in activity on politi-
cal markets in order to affect institutions (and thus
the rules of the game played on economic markets).
Whether such political activity results in transaction
cost reducing or increasing changes of the institu-
tional framework largely depends on ideology
(which thus becomes a major force in explaining rise
and decline of whole societies). In analogy to the
entrepreneur who drives technical progress on eco-
nomic markets, North (1981) also introduces the
political entrepreneur who drives change on political
markets (which activity is in addition to the political
activity of organizations). (North has incorporated
some more elements in his framework such as mar-
kets for knowledge creation which we suppress here
in order to keep complexity on a level allowing for
comparing the two frameworks; for a more detailed
description and analysis, cf. Reimers (1995), pp. 11-
18).
When mapped onto Williamson’s three layer
model, the role of institutions is mostly identical to
that assigned by Williamson to them. They act as
“shift parameters” (Williamson, 1993) affecting the
costs of doing business on the economic markets, i.e.
transaction costs. However, changes on this level are
incorporated into the analysis and are thus given a
more active role while in Williamson’s framework
institutional changes are treated as exogenous
events. Thus, actions of organizations or entrepre-
neurs to affect institutions and thus indirectly be-
haviour on economic markets (including design of
governance forms) is included in the framework.
While such behaviour is affected by many factors,
North assigns a prominent role to ideology which
can be viewed as located on the micro-level in Wil-
liamson’s three layer model (cf. Figure 2 for a sum-
mary of those elements of North’s framework which
are relevant from the perspective of Williamson’s
three layer model).
Institutional environment
Governance of
transaction relationship
Behavioural
assumptions
New
technology
Political entrepreneurs
and organizations create
new rules which affect
governance forms
Transaction cost lowering
technology enables new
governance forms
Ideology shapes governance
forms indirectly through
influencing political action
Institutional environment
Governance of
transaction relationship
Behavioural
assumptions
New
technology
Political entrepreneurs
and organizations create
new rules which affect
governance forms
Transaction cost lowering
technology enables new
governance forms
Ideology shapes governance
forms indirectly through
influencing political action
Figure 2: Technological change in a Northian framework
(as mapped onto Williamson’s three layer model).
The main difference between the two frame-
works -- apart from the different roles new technol-
ogy plays in them -- consists in the effect ascribed to
behavioural assumptions. In Williamson’s frame-
work, behavioural assumptions necessitate creation
of dedicated governance structures which thus take a
prominent place in the framework and generally
increase unit transaction costs. In North’s frame-
work, behavioural assumptions affect behaviour on
political markets (which take centre stage in the
framework) which then affects transaction costs on
economic markets. Technological change enters
through different routes too, albeit in both cases in-
directly. In Williamson’s framework, technology
appears as a special form of asset specificity (thus,
by necessity, increasing unit transaction costs); in
North’s framework, technological change enters as
‘technical progress’ created on ‘knowledge markets’
(given the right ideology has emerged stimulating
INTERACTION OF TECHNOLOGICAL AND INSTITUTIONAL CHANGE IN THE DEVELOPMENT OF AN
ELECTRONIC COMMERCE SYSTEM IN CHINA’S PHARMACEUTICAL DISTRIBUTION CHAIN - A Transaction
Cost Perspective
5

the demand for ‘productive’ knowledge; in Figure 2,
this relationship between new technology and
knowledge markets in not expressly modelled).
The question arises how these two explanations
can be empirically tested. While it would be temp-
ting to approach the problem in a direct manner by
estimating the effect of new technology on transac-
tion costs (whether it lowers or increases unit trans-
action costs), such an approach would not be accept-
able from a Williamsonian perspective since by as-
sumption -- as pointed out and criticized by North --
transaction costs cannot be measured directly ac-
cording to that perspective. However, it should be
possible to observe for which purpose new technol-
ogy is being used, taking use as an indication for its
effect (on transaction and/or transformation costs).
According to a Northian interpretation, new technol-
ogy which coincides with the emergence of new
governance structures should be used for purposes of
preparing, negotiating, or monitoring contracts
while, according to a Williamsonian perspective,
new technology which coincides with the creation of
new governance structures should be used for trans-
formative purposes (making production and/or dis-
tribution/logistics more efficient).
In addition, certain characteristic differences
should be observed. While institutional changes (i.e.
changes in the institutional environment as defined
by the three layer model) are not mandatory for new
technology to have its predicted effects, they can co-
exist with technological change. However, from a
Williamsonian perspective, technological change
and institutional change, should they both be ob-
served simultaneously, would have independent ef-
fects on governance structures except for the case of
institutionally mandated technological change.
While institutional change may increase or decrease
transaction cost levels technological change will
always increase unit transaction costs. Thus, tech-
nological change will only occur if the resulting in-
crease in unit transaction costs is accompanied by an
even larger reduction in transformation costs or if
changes in the institutional environment lead to the
adoption of governance structures which are re-
quired to accommodate the technological change. In
contrast, from a Northian perspective, one would
expect political entrepreneurs or economic organi-
zations to lobby for institutional change which
would exploit the transaction cost lowering proper-
ties of new technology if such technology should
become available. Thus, institutional change would
have a different character in both cases. From a
Williamsonian perspective, it would have the char-
acter of enforcing new governance structures (or be
completely independent of technological change)
while, from a Northian perspective, it would have
the character of being enabled by technological change.
Finally, behavioural assumptions would play dif-
ferent roles in the two theoretical frameworks and
thus in any explanation of empirical phenomena.
Specifically, from a Williamsonian perspective, they
would underlie the design of governance structures;
from a Northian perspective, they would shape po-
litical behaviour by political entrepreneurs and/or
economic organizations.
The discussion can be summarized by the fol-
lowing two propositions:
Proposition 1 (Williamsonian interpretation):
Technological change which coincides with institu-
tional change and affects the governance of trans-
actional relationships leads to systems which in-
crease efficiency of logistical and/or production
processes. In addition, institutional change takes on
the character of enforcing the new governance
structure which, in turn, will reflect behavioural
traits of agents.
Proposition 2 (Northian interpretation): Tech-
nological change which coincides with institutional
change and affects the governance of transaction
relationships leads to systems which are used for
lowering relevant transaction costs. In addition, in-
stitutional change takes on the character of being
enabled by the technological change while behav-
ioural traits of agents are reflected in the institutional
change.
3 DESCRIPTION OF THE CASE
3.1 Description of Data Sources and
Method
We used a single case study design for our research.
Use of the case study research method is justified
because our questions concern the ‘how’ and ‘why’
of an organizational phenomenon which cannot be
studied outside its real-life context and which in-
volves interaction of a large number of variables
(Yin, 2003). Use of a single case design is justified
because of the uniqueness of the case -- massive
institutional change on an industry level coinciding
with technological change -- and the difficulties of
obtaining empirical data in that context (ibid.).
Specifically, the healthcare industry in China is ex-
posed to an intense public debate about its practices
because of a widespread dissatisfaction with health-
care services and the difficult situation of central
HEALTHINF 2008 - International Conference on Health Informatics
6

government in this discussion. For these reasons, it
is very difficult and time-consuming to gain access
to key informants in the industry. We have therefore
focused our research on the case of drug distribution
in Beijing.
In total, 12 interviews were conducted with 15
informants between September 2004 and May 2007.
Informants represent manufacturers, wholesalers, e-
commerce intermediaries, a so-called bidding centre
(a government agency), the Ministry of Health, and
the key person driving the introduction of e-com-
merce into drug distribution in China. That person
was interviewed four times over the research period,
allowing us to follow the evolution of the techno-
logical and institutional change over three years. In
addition, documented material -- mostly in the form
of Chinese websites -- was used for supplementing
our data.
All information presented in the case description
below has been triangulated by at least two inter-
view sources except in cases where informants re-
presented the subjective view of their organizations;
such instances are explicitly in1dicated in the fol-
lowing description when they occur.
3.2 The Problem which Triggered
Institutional Action
The reform of economic structures in China started
in the late 1970s has not only led to the emergence
of business organizations and economic markets but
also deteriorated existing economic organizational
structures. One characteristic of these previously
dominating structures was the tight integration of
work organizations and social services such as
housing, education and healthcare. These integrated
units -- called dan wei -- were not only internally
integrated but, to a large extent, externally insulated.
Workers would seldom leave the compounds on
which all facilities required for everyday life existed.
The main connection with the economic environ-
ment consisted of flows of intermediate goods
among these organizations (Walder, 2000). Thus, the
functional separation that came with the emergence
of dedicated business organizations -- as opposed to
these integrated work organizations -- implied that
social services would have to either be provided as a
commercial service as well or by government. To
some extent, both of these directions were pursued,
especially with regard to healthcare. Specifically,
while, through a reform of the health insurance sys-
tem in 1998, all workers in cities are covered by a
governmental insurance system, rural families re-
ceive practically no any health insurance coverage
(cf. Dou, 2003, and IMS Health, 2004). Most medi-
cal expenses need to be paid out of pocket by rural
families (ibid.). At the same time, governmental
health insurance for urban workers covers only basic
services so that a large number of privately-based
insurance schemes has sprung to live covering addi-
tional health risks (ibid.).
While this situation was not satisfactory for most
people and organizations involved in healthcare, it
continued to function to the extent that healthcare
costs could be kept low. The healthcare system
started to be defunct, however, once the drug prices
started to increase significantly. While one cause of
the rise in drug prices was the entering of multi-
national pharmaceutical firms into the Chinese mar-
ket and the accompanying rise of branded drugs --
alongside the much cheaper so-called ethnic drugs,
i.e. drugs based on traditional Chinese medicine --
the root cause for this development was the chronic
under-financing of hospitals. In order to survive in
the new economic environment, hospitals took to
earning most of their income (on average 80%)
through the selling of drugs which naturally created
incentives to sell expensive drugs with high margins.
Central government initiated several institutional
measures to mitigate the situation. For example, it
kept prodding provincial and local governments to
improve healthcare provisioning and to develop in-
surance schemes for the rural population. It also in-
stituted that all business organizations operating in
the distribution of drugs had to be certified by the
year 2004. The reason for this measure was an in-
tention to cut down on the huge number of distribu-
tors, wholesalers and other intermediaries which,
around the year 2002, was estimated to be between
16 and 17 thousand (Dou, 2003). This large number
of intermediaries in the distribution of drugs was
supposed to create inefficiencies through fragmenta-
tion (lack of economies of scale) and multiple mark-
ups (each intermediary would add a mark-up to the
price). Moreover, central government required hos-
pitals to separate their internal pharmacy accounts
from their other accounting processes in order to
increase transparency regarding the extent to which
hospitals financed themselves through the sale of
drugs; a second institutional reform concerned the
introduction of a centralized bidding process through
which hospitals were expected to purchase drugs.
There has also been some efforts to promote the de-
velopment of an independent retail pharmacy sector
because it was assumed that through this process the
monopoly power hospitals traditionally held over the
sale of drugs could be broken or at least diminished.
All these measures are very recent, beginning in
the year 2000, and government is continuing to ex-
periment with new approaches. However, govern-
ment is severely restricted in enforcing its policies
INTERACTION OF TECHNOLOGICAL AND INSTITUTIONAL CHANGE IN THE DEVELOPMENT OF AN
ELECTRONIC COMMERCE SYSTEM IN CHINA’S PHARMACEUTICAL DISTRIBUTION CHAIN - A Transaction
Cost Perspective
7

for two reasons. First, it depends upon the services
of hospitals, a fact which came to light during the
SARS epidemic in 2003. Therefore, government
cannot afford to let a large number of hospitals go
out of business. Second, government is not a unified
force but internally highly fragmented along vertical
and horizontal lines. Specifically, regulatory and
administrative powers regarding the healthcare sec-
tor were, in 2002, distributed across nine govern-
mental agencies and ministries (Dou, 2003) some of
which were later merged. Vertically, government
power is spread across central and provincial gov-
ernments, for example with respect to inspecting and
certifying drug manufacturing.
In the following, we will focus on the introduc-
tion of the centralized purchasing process since this
was the main force shaping the development of
electronic commerce systems in drug distribution
but also consider the effects of the other measures
since they are all interdependent.
3.3 An Early Experiment
In order to curb corruption related to the problems
outlined above, the provincial government in Henan
province centralized all drug procurement related to
hospital demand in 1993. Resistance by hospitals to
this measure, however, lead to the discontinuation of
the practice two years later. The person in charge of
implementing this measure, Mr. Li, then visited the
US in order to study drug distribution there and be-
came convinced that centralization of drug procure-
ment was the “direction for the future of China” but
that this was only possible by using e-commerce.
After two years of preparation, an e-commerce sys-
tem for procuring drugs commenced operations,
initially with good results -- according to Mr. Li --
but which was closed down after just half a year of
operations upon being declared illegal by central
government under then premier minister Mr. Zhu
Rongji because business operations had to be sepa-
rated from their regulation. The system was then
sold to a private company -- Haihong -- which
would re-launch it in Henan and introduce it to sev-
eral other provinces, among them Guangdong,
Hainan, and Beijing.
3.4 How the System is used in Beijing
In Beijing, a centralized, e-commerce-based pro-
curement system for drugs began operations in 2004.
However, institutional reforms preparing for that
system go back to the year 2000 when the ‘Beijing
Bidding Centre’ was set up as a joint effort by nine
government agencies involved in the regulation of
drug distribution to hospitals. These agencies in-
clude, for example, the Beijing Health Bureau
(which has a role similar to a national Ministry of
Health albeit on a provincial level), the Beijing Price
Bureau and the Beijing Traditional Chinese Medi-
cine Bureau. Based on experiences with similar
systems in other provinces, most of them supported
by Haihong’s software and services, a process for
drug procurement was established; while the core
elements of this process are similar across the whole
country some elements show distinct characteristics
distinguishing the process from those implemented
in other provinces. In general, drug distribution is
still a highly localized business; distributors who are
fierce competitors in one province may therefore be
business partners in 1another province. The
following account focuses on the practices
associated with the e-commerce system in Beijing.
Preparing list
of agents
Public Tender
Manufacturers
apply for
participation
Manufacturers
are evaluated
and invited
Bids are
submitted
electronically
Data are
cleansed and
formatted
Bids are
evaluated
Winning bids
are published
Contracts
between
hospitals and
manufacturers
are closed
Preparing list
of agents
Public Tender
Manufacturers
apply for
participation
Manufacturers
are evaluated
and invited
Bids are
submitted
electronically
Data are
cleansed and
formatted
Bids are
evaluated
Winning bids
are published
Contracts
between
hospitals and
manufacturers
are closed
Figure 3: The bidding process (bold boxes indicate steps
supported by the e-commerce system).
The bidding centre usually initiates a bidding
process once per year. The process steps are de-
picted in Figure 3. The core step consists of evalu-
ating competing bids by manufacturers on individual
pharmaceutical agents (chemical substances) ac-
cording to multiple criteria, including price and ser-
vice quality of distributors (which must be assigned
by manufacturers in advance and which often take
over the paperwork associated with participation in
the bidding process). The list of agents comprises
about 15 thousand items on which manufacturers
can bid. Evaluation is done by a group of experts for
each of the province’s -- Beijing is a province as
well as a city -- six hospital groups which have been
set up according to certain differences in their de-
mand for drugs. Once bids have been selected, hos-
pitals are required to place purchase orders for drugs
only among the winning bids. The main purpose of
this process is to ensure that hospitals use high qual-
ity drugs while controlling drug prices.
HEALTHINF 2008 - International Conference on Health Informatics
8

The bidding process is facilitated by a number of
intermediaries which have been certified for that
purpose. While seven intermediaries have received
such certificates, only three are active. Each hospital
group selects one of them to help them with operat-
ing the bidding process. The largest among them --
serving four hospital groups -- is Haihong. The re-
quirements according to the certification process
also include ownership and operation of an e-com-
merce system. Regarding the bidding process itself,
that system collects all documents which need to
accompany a bid and which have to be submitted
electronically. The intermediaries then pass these
data -- after some data cleansing and format adjust-
ments -- on to the bidding centre. Once winning bids
have been selected, the results are published on the
e-commerce systems.
The more important role which these e-com-
merce systems play, however, concerns the ordering
process. Hospitals are required -- according to
stipulations by the Beijing Health Bureau -- to sub-
mit orders through these systems. For that purpose,
they log onto the system over a web interface and
enter their orders directly into the system. Distribu-
tors then download order data from the system --
also by logging onto the system through a web inter-
face -- and hospitals are automatically informed that
distributors have downloaded order data. However,
distributors cannot confirm or change purchase or-
ders.
The express purpose of this use of e-commerce
systems is to facilitate the monitoring of compliance
with the rules of the bidding process. Specifically,
the bidding centre is charged with the task of moni-
toring hospital purchasing activity in order to ensure
that hospitals only buy ‘from the list’, i.e. do not
circumvent the drugs which have been selected in
the evaluation process.
The percentage of drugs sold/procured through
these systems has increased continuously since their
inception in 2004 and was estimated to be close to
100% in 2006. Use of the system is accredited with
having caused a significant drop in the number of
distributors in Beijing which fell from around 200 in
2004 to about 120 at the beginning of 2007.
The e-commerce system replaces a practice in
which distributors took drug orders from hospitals
by phone (orders by distributors to manufacturers
continue to be placed over the telephone or by fax).
The services of intermediaries complement the e-
commerce system’s functionality, mostly by offering
a ‘screening service’; if a distributor does not re-
spond to an order, the intermediary will help the
hospital to procure the drugs through other channels.
The intermediaries also improve the efficiency of the
ordering process by harmonizing data. For example,
hospitals often use internal codes to identify drugs.
These codes are matched to standard drug identifiers
defined by the China Food and Drug Administration
(FDA) so that distributors can use the FDA codes for
their internal processes rather than having to cope
with multiple proprietary codes used by hospitals.
While some of the data used for the ordering and
for the bidding processes are identical, the systems
are separated (including separate databases) because
they are regulated by different government agencies
(as a side-effect of this separation, the ordering sys-
tem could also be used by other organizations who
do not have to participate in the bidding process
such as independent pharmacies; because of capacity
problems, however, use of the system is currently
limited to hospitals). Operational efficiencies of us-
ing the e-commerce system for supporting the bid-
ding process are minor as compared to the ordering
process. The main benefits concern ease of selecting
and evaluating drugs which facilitates the work of
the expert group who selects bids. Again, this re-
quires harmonization of data supplied by manufac-
turers (or distributors acting on behalf of manufac-
turers) which is done by the intermediaries.
The vision of Mr. Li, who continues to advise
Haihong regarding further development of its e-
commerce system, is to provide a comprehensive
platform for managing the whole drug supply chain
from manufacturers to hospitals. However, currently
only the order process is supported by the system
and even this support is rather limited (as evidenced
by a lack an order confirmation or change function).
For example, it was intended to use the system for
enabling zero-inventories in hospital pharmacies.
However, hospitals were not interested in such a
capability because they do not have to pay manu-
facturers for unsold inventories. While Haihong’s
system was the first to be developed, the systems of
all three intermediaries are rather similar in terms of
functionality and capacity and do not constitute a
main competitive differentiator for them.
Thus, while the operational scope of the three e-
commerce systems is rather narrow, they are indeed
used for improving operational efficiency of the or-
dering process. For example, while, in 2004 the as-
sociation of drug wholesalers and pharmacies re-
ceived broad support by its constituency when sub-
mitting a petition to government objecting introduc-
tion of the e-commerce-based distribution system,
that support is waning as large distributors (whole-
salers) are discovering operational benefits of the
system and because the system has led to a consoli-
dation of the industry favouring the larger players.
Hospitals have to contract with the intermediary
as well as with manufacturers. Each hospital group
INTERACTION OF TECHNOLOGICAL AND INSTITUTIONAL CHANGE IN THE DEVELOPMENT OF AN
ELECTRONIC COMMERCE SYSTEM IN CHINA’S PHARMACEUTICAL DISTRIBUTION CHAIN - A Transaction
Cost Perspective
9

selects one intermediary which, however, charges
fees to manufacturers as stipulated by the Beijing
Health Bureau. The licenses of intermediaries need
to be renewed each year but the relationship between
a hospital group and an intermediary tends to be
stable and long-term. Upon conclusion of the bid-
ding process, hospitals have to contract with manu-
facturers that have succeeded in the bidding process.
Occasionally, hospitals also negotiate with manu-
facturers again before placing orders on the e-com-
merce system in order to receive discounts. In the
evaluation process, it is also possible that the bid-
ding centre negotiates with manufacturers who have
participated in the bidding process. This occurs
when for a specific agent (chemical substance) only
one bid has been submitted. In addition, manufactur-
ers use sales agents and other wholesalers to market
and also sell their drugs to hospitals. However, these
agents, who may receive the drugs at a discounted
price, still have to use the licensed distributors for
delivering the drugs to hospitals.
The specific governance structure used for oper-
ating e-commerce systems through intermediaries is
justified by two rationales. First, the main benefit of
the system is seen in the ease of monitoring compli-
ance with the bidding rules. This is considered cru-
cial since hospitals have very strong incentives to
circumvent these rules in order to increase their in-
come through the sale of branded and therefore
high-margin drugs. Second, Mr. Li argues that e-
commerce in China is only viable if facilitated by
third parties. He points to an effort in Shanghai
where wholesalers have tried to build e-commerce
systems to directly connect with hospitals. These
efforts have failed because of the fragmented market
structure (hospitals typically deal with around 30
different distributors), fierce competition among
distributors (forestalling cooperation among them)
and low trust among all parties.
The e-commerce systems, however, are not used
for the purpose of monitoring compliance with the
bidding rules. Specifically, the bidding centre does
not make any use of its ability to log onto the sys-
tems in order to check hospitals’ compliance with
the bidding rules (as reflected in their ordering be-
haviour). While the bidding centre claims that 50-
60% of all purchasing transactions are reported to it
by intermediaries, it turns out that this feedback is
based on aggregated data which are provided by
intermediaries to the bidding centre on paper and
this only upon request which occurs infrequently and
usually only once per year. The intermediaries sug-
gest that the bidding centre lacks the technical skills
required for making sense of the data provided by
the systems directly. The bidding centre itself indi-
cates that its ability to sanction hospitals (through
exposing non-compliance) is rather limited because
it is difficult to tell violations of rules from “market
behaviour”, a view shared by Mr. Li. It was also
frequently mentioned that hospitals often have suffi-
cient “market power” to resist any sanctioning ef-
forts. Mr. Li cited yet another reason for the failure
of the bidding centre to directly use the e-commerce
systems to monitor purchasing behaviour of hospi-
tals. The data in the systems cannot be easily ana-
lysed because of a lack of data standards (apart from
the use of proprietary product codes by hospitals
mentioned above, other data such as names of manu-
facturers are not standardized either). Moreover,
some hospitals ask intermediaries to provide them
with so-called ‘soft systems’ for their data input
which are tweaked so as to make it even more diffi-
cult to monitor their purchasing behaviour.
4 CASE ANALYSIS
Referring to the two propositions developed in the
theory section, it becomes clear that the e-commerce
systems described above have been developed with a
Northian intention. The main idea of Mr. Li -- who
can be viewed as the political entrepreneur described
by North -- was that centralization of the procure-
ment process -- i.e. a specific instance of institu-
tional change -- was only possible if accompanied
by an e-commerce system. He assumed that elec-
tronic commerce would facilitate the monitoring of
hospital drug purchasing behaviour which was a
central element in the introduction of the bidding
process. These costs are an instance of transaction
costs since they concern the monitoring of a con-
tract, albeit one imposed on the participants in the
market. Thus, the e-commerce system’s ability to
reduce transaction costs would be exploited for the
purpose of institutional reform. Also, the organiza-
tions active on the economic market -- mostly dis-
tributors and hospitals -- tried to prevent the institu-
tional reform through lobbying activity.
The bidding process centralized all negotiations
between hospitals and manufacturers while the e-
commerce system centralized ordering and delivery
(for a small group of hospitals in Beijing, govern-
ment has actually taken over all procurement activi-
ties, thus reversing the earlier decree by central gov-
ernment to separate regulation and business activ-
ity). Also, the very idea of solving the problems
characterizing drug distribution through taking over
HEALTHINF 2008 - International Conference on Health Informatics
10

central control of the process seems to be in line
with the overall ideology of economic policy in
China. Thus, all elements suggested by a Northian
interpretation of the interaction between institutional
and technological change -- technology-enabled in-
stitutional change, activity on political markets to
bring about or prevent the institutional change, a
‘national’ characteristic trait of the intended institu-
tional reform -- seem to be in place.
However, the e-commerce system is not used for
the intended purpose (facilitating institutional
change through reducing the costs of monitoring
compliance with the new rules); yet, the main actors
in the industry continue to offer the rationale of fa-
cilitating monitoring of hospital drug purchasing
behaviour as an explanation for continued use of the
e-commerce systems. While there are several rea-
sons for the factual avoidance of using the system
for monitoring hospital transactions, including bar-
gaining power of hospitals and lack of alternative
funding schemes, the fact that the e-commerce sys-
tems are not used for their intended purpose allows
us to reject the Northian interpretation of this case.
The new institutional process -- the bidding process
-- was not enabled by a reduction of transaction
costs -- in this case monitoring costs -- through use
of the e-commerce system; continued existence of
the new institutional arrangement can only be ex-
plained by government’s use of sanctions and ad-
ministrative force. In addition, significant violation
of the rules stipulated by the bidding process was
tolerated by government agencies which may have
reduced resistance to the new institutional order.
Regarding a Williamsonian interpretation, it
seems reasonable to argue that the e-commerce sys-
tems did not reduce transaction costs but probably
contributed to increased efficiency of the ordering
process. For example, distributors do not have to
handle multiple systems for identifying drugs
through proprietary product codes while hospitals
can place orders to distributors in one process rather
than sending individual orders to each distributor
separately. (Note that costs associated with placing
orders are not transaction costs since they neither
concern the costs of negotiating contracts -- this has
been done through the bidding process resulting in
bilateral contracts between hospitals and manufac-
turers -- nor do they constitute costs of monitoring
contracts; if the supply chain would be controlled by
one organization, it would still be necessary to create
(internal) orders for replenishing inventories in hos-
pital pharmacies.)
On the other hand, transaction costs associated
with the new governance structure may well have
been increased because the bidding process intro-
duced new costs into the distribution system; e.g.,
the expert groups have to evaluate bids on 15 thou-
sand agents (chemical substances) by multiple sup-
pliers. While the e-commerce systems provide some
support for this process, the main work is manual. In
addition, multiple other channels for negotiating
between hospitals and manufacturers continue to be
used. Finally, bilateral contracting between hospitals
and manufacturers is still necessary, although these
contracts are based on the prices quoted in the bid-
ding process. In any case, hospitals would prefer to
bilaterally negotiate with manufacturers even so they
do not have to pay for the work of the bidding centre
(which is completely funded by the Beijing govern-
ment). Also, mandatory use of the new inter-
mediaries did impose some new costs on the distri-
bution system. Presently, these are carried by the
manufacturers (who must -- by law -- be charged for
the intermediaries’ services -- although they serve
the hospital groups). It was anticipated that hospitals
would effectively oppose any efforts to make them
pay for the services of intermediaries, e.g. by asking
manufacturers to take over these fees ).
The governance structure used for facilitating
set-up and operation of e-commerce systems also
seems to display typical ‘Chinese characteristics’ as
these systems are developed and operated by third
parties rather than within a bilateral governance
structure typical for Western EDI-based models of e-
commerce. Thus, all elements suggested by a Wil-
liamsonian interpretation can be identified in the
way these systems are actually used. The govern-
ance structure underlying operation of the e-com-
merce systems is likely to have increased overall
transaction costs in the distribution of drugs between
distributors and hospitals. However, operational ef-
ficiencies in the ordering process could (partly)
compensate for these increased transaction costs. As
the operational efficiencies become clearer, resis-
tance towards using the e-commerce systems wanes
(this fading resistance seems also to be related to
recognition among the main players that the systems
are not used for monitoring their market behaviour).
However, because of a lack of hard data, a Wil-
liamsonian interpretation cannot be proven. More-
over, this lack of hard data could well be implied in
the approach itself, a problem which motivated the
critique of North and Wallis in the first place. Yet,
we find that the Northian interpretation explains the
motives behind the political initiative to create a
centralized, e-commerce-based drug procurement
process while actual use of the system contradicts
such an interpretation.
INTERACTION OF TECHNOLOGICAL AND INSTITUTIONAL CHANGE IN THE DEVELOPMENT OF AN
ELECTRONIC COMMERCE SYSTEM IN CHINA’S PHARMACEUTICAL DISTRIBUTION CHAIN - A Transaction
Cost Perspective
11

5 CONCLUSIONS
In exploring two alternative transaction cost-based
explanations of the interaction of institutional and
technological change in the case of China’s drug
distribution system, we have found evidence that a
Northian interpretation -- which suggests that trans-
action cost reducing technological change enables
institutional change -- does not apply to the actual
practice of distributing drugs based on new institu-
tional rules and an e-commerce system but does ac-
curately describe intentions and political behaviour
which has resulted in these new arrangements. Ac-
tual use of the e-commerce system and its govern-
ance structure seems to be more in line with a Wil-
liamsonian interpretation which suggests that insti-
tutions and governance structures need to be adapted
to enable implementation of new technology in or-
ganizational systems, resulting in increased opera-
tional efficiency, albeit at the expense of increased
transaction costs.
We therefore conclude that development and use
of new technology as well as intentions associated
with an institutional change and the practices based
on these changes may well follow different ration-
ales. More generally, while a certain perceived inter-
action between technological and institutional
change may motivate these changes, the practices
which result from these changes could follow a dif-
ferent logic of interaction. This result is reminiscent
of early formulations of neo-institutional theory
(Meyer and Rowan, 1977). These formulations sug-
gested that organizations maintain a ‘gap’ between
their internal operational processes and their exter-
nal, symbolic justification of these processes. While
these early propositions have been strongly criti-
cized by institutional theorists themselves (Powell,
1991), our results suggest that such a gap could be
the result of an implementation process in which the
rationales that motivated technological and institu-
tional change continue to exist as a ‘distant echo’ in
actual practices. However, actual practices have
adapted to a different rationale.
While our results are not sufficient to accept or
reject one transaction cost-theoretic interpretation
over the other, they suggest that further exploration
of these two explanations in settings which study the
interaction of technological and institutional change
on an intermediate level between that of individual
organizations and whole economies is a worthwhile
effort. Moreover, our study shows that the two ex-
planations could account for different phases in the
evolution of that interaction, a result which was not
expected at the outset of this study.
ACKNOWLEDGEMENTS
The first author would like to acknowledge support
by the Deutsche Forschungsgemeinschaft (grant
number 1328/2-2); the second author would like to
acknowledge support by the China Natural National
Science Foundation (grant numbers 70621061 and
70672007) and the China MOE Project of the Key
Research Institute of Humanity and Social Sciences
at Universities (number #06JJD630014).
REFERENCES
Dou, W. (2003). The Chinese Pharmaceutical and Bio-
technology Market Guide 2003. SCRIP Report No. BS1210,
28 March 2003, Richmond/Surrey: PJB Publications.
IMS Health (2004). IMS Market Prognosis Australasia
2004-2008 – China. IMS Health, London, March 2004.
Meyer, J. W., & Rowan, B. (1977). Institutionalized
Organizations: Formal Structure as Myth and
Ceremony. American Journal of Sociology, 83, 440-463.
North, D. C. (1981). Structure and Change in Economic
History. N.Y., London: W. W. Norton.
North, D. C. (1990). Institutions, Institutional Change,
and Economic Performance. Cambridge: Cambridge
University Press.
North, D. C., & Wallis, J. J. (1994). Integrating
Institutional Change and Technical Change in
Economic History -- A Transaction Cost Approach.
Journal of Institutional and Theoretical Economics,
150, 609-624.
Powell, W. W. (1991). Expanding the Scope of
Institutional Analysis. In: W.W. Powell & P.J.
DiMaggio (eds.), The New Institutionalism in
Organizational Analysis (pp. 183-203). Chicago et al.:
University of Chicago Press.
Reimers, K. (1995). Normungsprozesse – Eine Trans-
aktionskostentheoretische Analyse. Wiesbaden: Gabler
Verlag (Neue betriebswirtschaftliche Forschung Bd. 146).
Von Hippel, E. (1978). A Customer-active Paradigm for
Industrial Product Idea Generation. Research Policy, 7,
240-266.
Walder, A. G. (2000). China's Transitional Economy. In: J.T. Li
et al. (eds.), Management and Organizations in the Chinese
Context (pp. 63-83). Houndsmills et al.: Macmillan,.
Wallis, J. J., & Douglass C. N. (1986). Measuring the
Transaction Sector in the American Economy 1870 -
1970. In: S.L. Engerman & R.E. Gallman (eds.), Long
Term Factors in American Economic Growth,
Chicago: University of Chicago Press.
Williamson, O. E. (1993). Transaction Cost Economics
and Organization Theory. Industrial and Corporate
Change, 2, 107-156.
HEALTHINF 2008 - International Conference on Health Informatics
12
