
PROCESS MINING IN HEALTHCARE
A Case Study
R. S. Mans, M. H. Schonenberg, M. Song, W. M. P. van der Aalst
Eindhoven University of Technology, P.O. Box 513, NL-5600 MB, Eindhoven, The Netherlands
P. J. M. Bakker
Academic Medical Center, University of Amsterdam, Department of Innovation and Process Management
Amsterdam, The Netherlands
Keywords:
Process mining, healthcare processes.
Abstract:
To gain competitive advantage, hospitals try to streamline their processes. In order to do so, it is essential
to have an accurate view of the “careflows” under consideration. In this paper, we apply process mining
techniques to obtain meaningful knowledge about these flows, e.g., to discover typical paths followed by
particular groups of patients. This is a non-trivial task given the dynamic nature of healthcare processes. The
paper demonstrates the applicability of process mining using a real case of a gynecological oncology process
in a Dutch hospital. Using a variety of process mining techniques, we analyzed the healthcare process from
three different perspectives: (1) the control flow perspective, (2) the organizational perspective and (3) the
performance perspective. In order to do so we extracted relevant event logs from the hospitals information
system and analyzed these logs using the ProM framework. The results show that process mining can be used
to provide new insights that facilitate the improvement of existing careflows.
1 INTRODUCTION
In a competitive health-care market, hospitals have to
focus on ways to streamline their processes in order
to deliver high quality care while at the same time re-
ducing costs (Anyanwu et al., 2003). Furthermore,
also on the governmental side and on the side of the
health insurance companies, more and more pressure
is put on hospitals to work in the most efficient way
as possible, whereas in the future, an increase in the
demand for care is expected.
A complicating factor is that healthcare is charac-
terized by highly complex and extremely flexible pa-
tient care processes, also referred to as “careflows”.
Moreover, many disciplines are involved for which
it is found that they are working in isolation and
hardly have any idea about what happens within other
disciplines. Another issue is that within healthcare
many autonomous, independently developed applica-
tions are found (Lenz et al., 2002). A consequence
of this all is that it is not known what happens in a
healthcare process for a group of patients with the
same diagnosis.
The concept of process mining provides an in-
teresting opportunity for providing a solution to this
problem. Process mining (van der Aalst et al., 2003)
aims at extracting process knowledge from so-called
“event logs” which may originate from all kinds of
systems, like enterprise information systems or hos-
pital information systems. Typically, these event logs
contain information about the start/completion of pro-
cess steps together with related context data (e.g. ac-
tors and resources). Furthermore, process mining is a
very broad area both in terms of (1) applications (from
banks to embedded systems) and (2) techniques.
This paper focusses on the applicability of process
mining in the healthcare domain. Process mining has
already been successfully applied in the service in-
dustry (van der Aalst et al., 2007a). In this paper, we
demonstrate the applicability of process mining to the
healthcare domain. We will show how process mining
can be used for obtaining insights related to careflows,
e.g., the identification of care paths and (strong) col-
laboration between departments. To this end, in Sec-
tion 3, we will use several mining techniques which
will also show the diversity of process mining tech-
niques available, like control flow discovery but also
the discovery of organizational aspects.
118
S. Mans R., H. Schonenberg M., Song M., M. P. van der Aalst W. and J. M. Bakker P. (2008).
PROCESS MINING IN HEALTHCARE - A Case Study.
In Proceedings of the First International Conference on Health Informatics, pages 118-125
Copyright
c
SciTePress

In this paper, we present a case study where we
use raw data of the AMC hospital in Amsterdam, a
large academic hospital in the Netherlands. This raw
data contains data about a group of 627 gynecolog-
ical oncology patients treated in 2005 and 2006 and
for which all diagnostic and treatment activities have
been recorded for financial purposes. Note that we did
not use any a-priori knowledge about the care process
of this group of patients and that we also did not have
any process model at hand.
Today’s Business Intelligence (BI) tools used in
the healthcare domain, like Cognos, Business Ob-
jects, or SAP BI, typically look at aggregate data seen
from an external perspective (frequencies, averages,
utilization, service levels, etc.). These BI tools fo-
cus on performance indicators such as the number of
knee operations, the length of waiting lists, and the
success rate of surgery. Process mining looks “inside
the process” at different abstraction levels. So, in the
context of a hospital, unlike BI tools, we are more
concerned with the care paths followed by individual
patients and whether certain procedures are followed
or not.
This paper is structured as follows: Section 2 pro-
vides an overview of process mining. In Section 3 we
will show the applicability of process mining in the
healthcare domain using data obtained for a group of
627 gynecological oncology patients. Section 4 con-
cludes the paper.
2 PROCESS MINING
Process mining is applicable to a wide range of sys-
tems. These systems may be pure information sys-
tems (e.g., ERP systems) or systems where the hard-
ware plays a more prominent role (e.g., embedded
systems). The only requirement is that the system
produces event logs, thus recording (parts of) the ac-
tual behavior.
An interesting class of information systems that
produce event logs are the so-called Process-Aware
Information Systems (PAISs) (Dumas et al., 2005).
Examples are classical workflow management sys-
tems (e.g. Staffware), ERP systems (e.g. SAP), case
handling systems (e.g. FLOWer), PDM systems (e.g.
Windchill), CRM systems (e.g. Microsoft Dynamics
CRM), middleware (e.g., IBM’s WebSphere), hospi-
tal information systems (e.g., Chipsoft), etc. These
systems provide very detailed information about the
activities that have been executed.
However, not only PAISs are recording events.
Also, in a typical hospital there is a wide variety of
systems that record events. For example, in an inten-
sive care unit, a system can record which examina-
tions or treatments a patient undergoes and also it can
record occurring complications for a patient. For a ra-
diology department the whole process of admittance
of a patient till the archival of the photograph can be
recorded. However, frequently these systems are lim-
ited to one department only. However, systems used
for billing purposes have to ensure that all services
delivered to the patient will be paid. In order for these
systems to work properly, information from different
systems needs to be collected so that it is clear which
activities have been performed in the care process of
a patient. In this way, these systems within the hos-
pital can contain information about processes within
one department but also across departments. This in-
formation can be used for improving processes within
departmentsitself or improving the services offered to
patients.
The goal of process mining is to extract informa-
tion (e.g., process models) from these logs, i.e., pro-
cess mining describes a family of a-posteriori anal-
ysis techniques exploiting the information recorded
in the event logs. Typically, these approaches as-
sume that it is possible to sequentially record events
such that each event refers to an activity (i.e., a well-
defined step in the process) and is related to a particu-
lar case (i.e., a process instance). Furthermore, some
mining techniques use additional information such as
the performer or originator of the event (i.e., the per-
son/resource executing or initiating the activity), the
timestamp of the event, or data elements recorded
with the event (e.g., the size of an order).
Process mining addresses the problem that most
“process/system owners” have limited information
about what is actually happening. In practice, there
is often a significant gap between what is prescribed
or supposed to happen, and what actually happens.
Only a concise assessment of reality, which process
mining strives to deliver, can help in verifying process
models, and ultimately be used in system or process
redesign efforts.
models
analyzes
records
events, e.g.,
messages,
transactions,
etc.
specifies
configures
implements
analyzes
supports/
controls
people
machines
organizations
components
business processes
Figure 1: Three types of process mining: (1) Discovery, (2)
Conformance, and (3) Extension.

The idea of process mining is to discover, mon-
itor and improve real processes (i.e., not assumed
processes) by extracting knowledge from event logs.
We consider three basic types of process mining (Fig-
ure 1): (1) discovery, (2) conformance, and (3) exten-
sion.
Discovery: Traditionally, process mining has
been focusing on discovery, i.e., deriving informa-
tion about the original process model, the organiza-
tional context, and execution properties from enact-
ment logs. An example of a technique addressing the
control flow perspective is the α-algorithm (van der
Aalst et al., 2004), which constructs a Petri net model
describing the behavior observed in the event log. It is
important to mention that there is no a-priori model,
i.e., based on an event log some model is constructed.
However, process mining is not limited to process
models (i.e., control flow) and recent process mining
techniques are more and more focusing on other per-
spectives, e.g., the organizational perspective, perfor-
mance perspective or the data perspective. For exam-
ple, there are approaches to extract social networks
from event logs and analyze them using social net-
work analysis (van der Aalst et al., 2005). This allows
organizations to monitor how people, groups, or soft-
ware/system components are working together. Also,
there are approaches to visualize performance related
information, e.g. there are approaches which graph-
ically shows the bottlenecks and all kinds of perfor-
mance indicators, e.g., average/variance of the total
flow time or the time spent between two activities.
Conformance: There is an a-priori model. This
model is used to check if reality conforms to the
model. For example, there may be a process model
indicating that purchase orders of more than one mil-
lion Euro require two checks. Another example is the
checking of the so-called “four-eyes” principle. Con-
formance checking may be used to detect deviations,
to locate and explain these deviations, and to measure
the severity of these deviations.
Extension: There is an a-priori model. This
model is extended with a new aspect or perspective,
i.e., the goal is not to check conformance but to en-
rich the model with the data in the event log. An ex-
ample is the extension of a process model with perfor-
mance data, i.e., some a-priori process model is used
on which bottlenecks are projected.
At this point in time there are mature tools such as
the ProM framework(van der Aalst et al., 2007b), fea-
turing an extensive set of analysis techniques which
can be applied to real-life logs while supporting the
whole spectrum depicted in Figure 1.
3 HEALTHCARE PROCESS
In this section, we want to show the applicability of
process mining in healthcare. However, as health-
care processes are characterized by the fact that sev-
eral organizational units can be involved in the treat-
ment process of patients and that these organizational
units often have their own specific IT applications, it
becomes clear that getting data, which is related to
healthcare processes, is not an easy task. In spite of
this, systems used in hospitals need to provide an inte-
grated view on all these IT applications as it needs to
be guaranteed that the hospital gets paid for every ser-
vice delivered to a patient. Consequently, these kind
of systems contain process-related information about
healthcare processes and are therefore an interesting
candidate for providing the data needed for process
mining.
To this end, as case study for showing the ap-
plicability of process mining in health care, we use
raw data collected by the billing system of the AMC
hospital. This raw data contains information about a
group of 627 gynecological oncology patients treated
in 2005 and 2006 and for which all diagnostic and
treatment activities have been recorded. The process
for gynecological oncology patients is supported by
several different departments, e.g. gynecology, radi-
ology and several labs.
For this data set, we have extracted event logs
from the AMC’s databases where each event refers to
a service delivered to a patient. As the data is coming
from a billing system, we have to face the interesting
problem that for each service delivered for a patient
it is only known on which day the service has been
delivered. In other words, we do not have any infor-
mation about the actual timestamps of the start and
completion of the service delivered. Consequently,
the ordering of events which happen on the same day
do not necessarily conform with the order in which
events of that day were executed.
Nevertheless, as the log contains real data about
the services delivered to gynecological oncology pa-
tients it is still an interesting and representative data
set for showing the applicability of process mining
in healthcare as still many techniques can be applied.
Note that the log contains 376 different event names
which indicates that we are dealing with a non-trivial
careflow process.
In the remainder of this section we will focus on
obtaining, in an explorative way, insights into the
gynecological oncology healthcare process. So, we
will only focus on the discovery part of process min-
ing, instead of the conformance and extension part.
Furthermore, obtaining these insights should not be

limited to one perspective only. Therefore, in sec-
tions 3.2.1, 3.2.2 and 3.2.3, we focus on the discov-
ery of care paths followed by patients, the discovery
of organizational aspects and the discovery of per-
formance related information, respectively. This also
demonstrates the diversity of process mining tech-
niques available. However, as will be discussed in
Section 3.1, we first need to perform some prepro-
cessing before being able to present information on
the right level of detail.
3.1 Preprocessing of Logs
The log of the AMC hospital contains a huge amount
of distinct activities, of which many are rather low
level activities, i.e., events at a low abstraction level.
For example, for our purpose, the logged lab activi-
ties are at a too low abstraction level, e.g. determina-
tion of chloride, lactic acid and erythrocyte sedimen-
tation rate (ESR). We would like to consider all these
low level lab tests as a single lab test. Mining a log
that contains many distinct activities would result in
a too detailed spaghetti-like model, that is difficult to
understand. Hence, we first apply some preprocess-
ing on the logs to obtain interpretable results during
mining. During preprocessing we want to “simplify”
the log by removing the excess of low level activi-
ties. In addition, our goal is to consider only events
at the department level. In this way, we can, for ex-
ample, focus on care paths and interactions between
departments. We applied two different approaches to
do this.
Our first approach is to detect a representative for
the lower level activities. In our logs, this approach
can be applied to the before mentioned lab activities.
In the logs we can find an activity that can serve as
representative for the lab activities, namely the activ-
ity that is always executed when samples are offered
to the lab. All other (low level) lab activities in the log
are simply discarded.
The log also contains groups of low level activ-
ities for which there is no representative. For in-
stance at the radiology department many activities
can occur (e.g., echo abdomen, thorax and CT brain),
but the logs do not contain a single event that oc-
curs for every visit to this department, like a reg-
istration event for example. We apply aggregation
for low level activities in groups without a repre-
sentative by (1) defining a representative, (2) map-
ping all activities from the group to this representa-
tive and (3) removing repetitions of events from the
log. For example, for the radiology department we
define “radiology” as representative. A log that orig-
inally contains “
...,ultrasound scan abdomen,
chest X-ray, CT scan brain,...
”, would con-
tain “
...,radiology,...
”, after mapping low level
radiology activities to this representative and remov-
ing any duplicates.
3.2 Mining
In this section, we present some results obtained
through a detailed analysis of the ACM’s event log
for the gynecological oncology process. We concen-
trate on the discovery part to show actual situations
(e.g. control flows, organizational interactions) in the
healthcare process. More specifically, we elaborate
on mining results based on three major perspectives
(i.e. control flow, organizational, performance per-
spectives) in process mining.
3.2.1 Control Flow Perspective
One of the most promising mining techniques is con-
trol flow mining which automatically derives process
models from process logs. The generated process
model reflects the actual process as observed through
real process executions. If we generate process mod-
els from healthcare process logs, they give insight into
care paths for patients. Until now, there are several
process mining algorithms such as the α-mining al-
gorithm, heuristic mining algorithm, region mining
algorithm, etc (van der Aalst et al., 2004; Weijters
and van der Aalst, 2003; van Dongen et al., 2007).
In this paper, we use the heuristic mining algorithm,
since it can deal with noise and exceptions, and en-
ables users to focus on the main process flow instead
of on every detail of the behaviorappearing in the pro-
cess log (Weijters and van der Aalst, 2003). Figure
2 shows the process model for all cases obtained us-
ing the Heuristics Miner. Despite its ability to focus
on the most frequent paths, the process, depicted in
Figure 2, is still spaghetti-like and too complex to un-
derstand easily.
Since processes in the healthcare domain do not
havea single kind of flow but a lot of variants based on
patients and diseases, it is not surprising that the de-
rived process model is spaghetti-like and convoluted.
One of the methods for handling this problem is
breaking down a log into two or more sub-logs until
these become simple enough to be analyzed clearly.
We apply clustering techniques to divide a process
log into several groups (i.e. clusters), where the cases
in the same cluster have similar properties. Cluster-
ing is a very useful technique for logs which contain
many cases following different procedures, as is the
usual case in healthcare systems. Depending on the
interest (e.g., exceptional or frequent procedures), a
cluster can be selected. There are several clustering
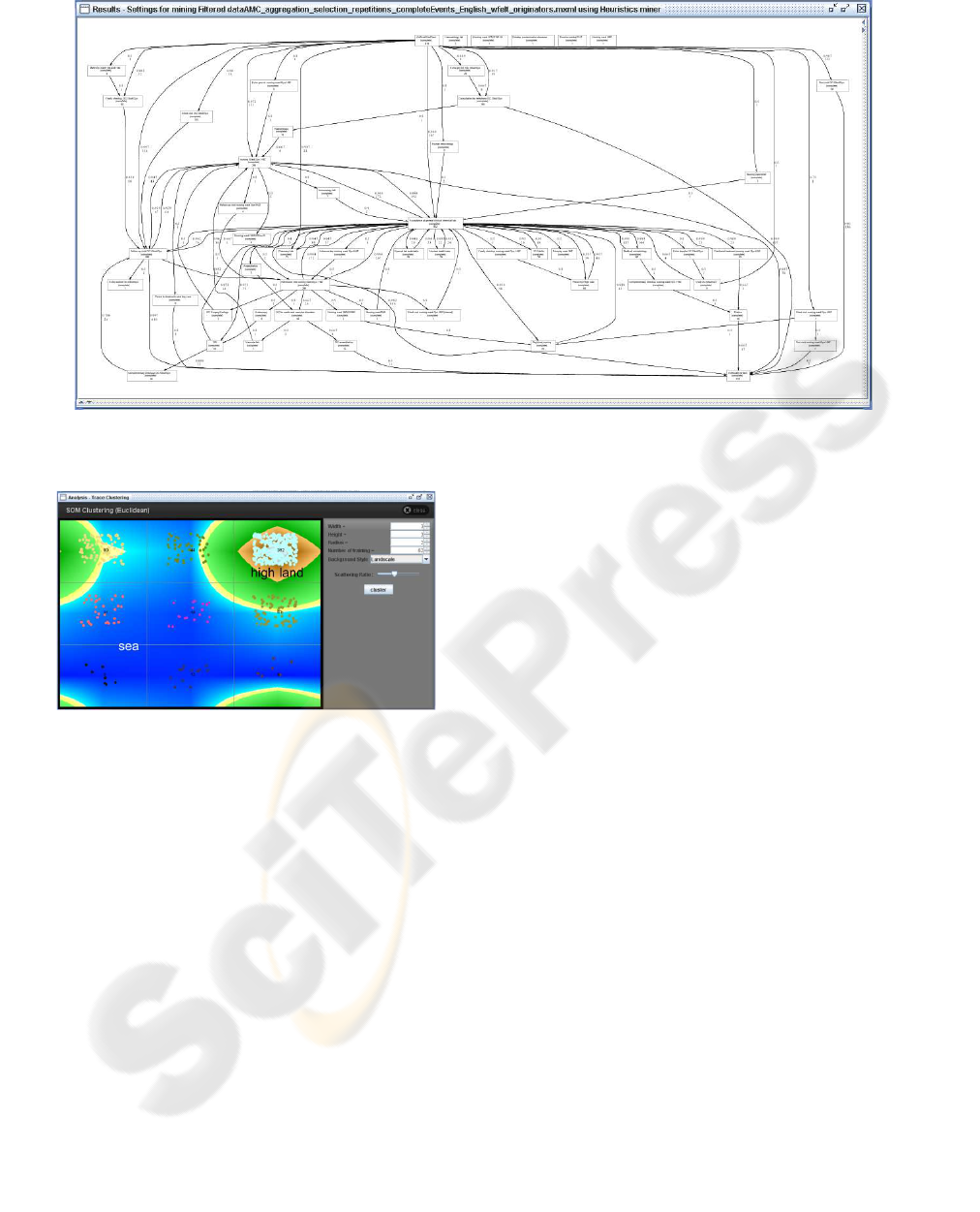
Figure 2: Derived process model for all cases.
Figure 3: Log clustering result.
techniques available. Among these, we use the SOM
(Self Organizing Map) algorithm to cluster the log be-
cause of its performance (i.e., speed). Figure 3 shows
the clustering result obtained by applying the Trace
Clustering plug-in. Nine clusters are obtained from
the log. In the figure, the instances in the same cell
belong to the same cluster. The figure also shows
a contour map based on the number of instances in
each cell. It is very useful to take a quick glance at
the clusters – are there clusters with many similarities
(high land), or are there many clusters with excep-
tional cases (sea).
By using this approach, we obtained several clus-
ters of reasonable size. In this paper we show only
the result for the biggest cluster, containing 352 cases
all with similar properties. Figure 4 shows the heuris-
tic net derived from the biggest cluster. The result is
much simpler than the model in Figure 2. Further-
more, the fitness of this model is “good”. The model
represents the procedure for most cases in the cluster,
i.e., these cases “fit” in the generated process model.
A closer inspection of this main cluster by domain
experts confirmed that this is indeed main stream fol-
lowed by most gynecological oncology patients.
When discussing the result with the people in-
volved in the process, it was noted that patients, re-
ferred to the AMC by another hospital, only visit the
outpatient clinic once or twice. These patients are al-
ready diagnosed, and afterwards they are referred to
another department, like radiotherapy, for treatment
and which is then responsible for the treatment pro-
cess. Also, very ill patients are immediately referred
to another department for treatment after their first
visit.
3.2.2 Organizational Perspective
There are several process mining techniques that ad-
dress organizational perspective, e.g., organizational
mining, social network mining, mining staff assign-
ment rules, etc. (van der Aalst et al., 2005). In this pa-
per, we elaborate on social network mining to provide
insights into the collaboration between departmentsin
the hospital. The Social Network Miner allows for the
discovery of social networks from process logs. Since
there are several social network analysis techniques
and research results available, the generated social
network allows for analysis of social relations be-
tween originators involving process executions. Fig-
ure 5 shows the derived social network. To derive the
network, we used the Handover of Work metric (van
der Aalst et al., 2005) that measures the frequency of
transfers of work among departments.
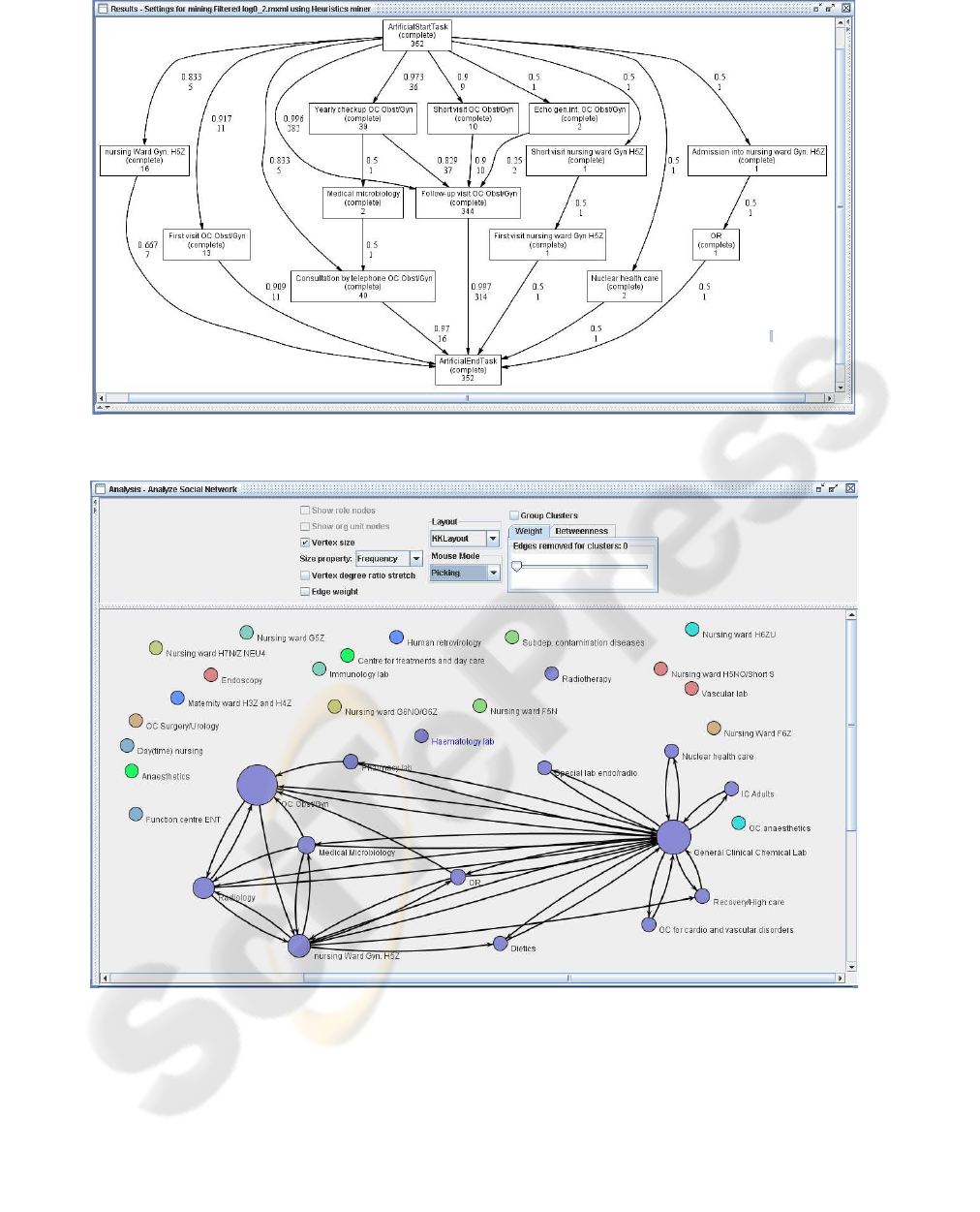
Figure 4: Process model from the biggest cluster.
Figure 5: Social network (handover of work metrics).
The network shows the relationships between
originators above a certain threshold. Originators, for
which all relationships are below the specific thresh-
old, appear as isolated circles. The originators that
were highly involved in the process appear as larger
dots in the figure. These results are useful to de-
tect whether there are frequent interactions between
originators (departments, in our case). In hospitals
there are many departments that interact and hand
over work to each other. The mining result shows that
the general clinical chemical lab is highly involved in
the process and interacts with many departments. The
outpatient clinic (OC) for gynecology and obstetrics
is also often involved, but is not directly connected to

all other departments. For instance there is no rela-
tionship (within this threshold) between this OC and
the vascular lab. This means that there is no, or not
much, interaction between these two departments.
When this result was presented to the people in-
volved in the process, they confirmed the strong col-
laboration with the departments shown in Figure 5.
However, they were surprised about the rather strong
collaboration with the dietics department. Neverthe-
less, this can be explained by the fact that, when a pa-
tient has to go to several chemotherapy sessions, then
a visit to the dietician is also often needed.
Moreover, they also noted that the many interac-
tions between the lab and other departments is mis-
leading as all the examinations are requested by gy-
necological oncology and not by the lab. This can be
explained by the many lab tests and resulting interac-
tions between the lab and other departments.
3.2.3 Performance Perspective
Process mining providesseveral performanceanalysis
techniques. Among these, the dotted chart is a method
suitable for case handlingprocesses which are flexible
and knowledge intensive business processes and focus
not on the routing of work or the activities but on the
case (e.g. careflows). In this paper, we use the dotted
chart to show overall events and performance infor-
mation of the log. Figure 6 shows the dotted chart. In
the chart, events are displayed as dots, and the time is
measured along the horizontal axis of the chart. The
vertical axis represents case IDs and events are col-
ored according to their task IDs. It supports several
time options such as actual, relative, logical, etc. In
the diagram, we use relative time which shows the
duration from the beginning of an instance to a cer-
tain event. Thus it indicates the case duration of each
instance. It also provides performance metrics such
as the time of the first and of the last events, case du-
rations, the number of events in an instance, etc. For
example, in the figure (top right, average spread in
seconds), the average case duration is about 49 days.
Users can obtain useful insights from the chart,
e.g., it is easy to find interesting patterns by looking at
the dotted chart. In Figure 6, the density of events on
the left side of the diagram is higher than the density
of those on the right side. This shows that initially pa-
tients have more diagnosis and treatment events than
in the later parts of the process. When we focus on
the long duration instances (i.e. the instances hav-
ing events in the right side of the diagram), it can be
observed that they mainly consist of regular consulta-
tion (red dot), consultation by phone (red dot), and lab
test (violet dot) activities. It reflects the situation that
patients have regular consultation by visiting or being
phoned by the hospital and sometimes havea test after
or before the consultation. It is also easy to discover
patterns in the occurrences of activities. For example,
seven instances have the pattern that consists of a lab
test and an admittance to the nursing ward activities.
When the results were presented to the people in-
volved in the process, they confirmed the patterns that
we found. Furthermore, for the last pattern they indi-
cated that the pattern deals about patients who get a
chemotherapy regularly. The day before, they come
for a lab test and when the result is good, they get the
next chemotherapy.
4 CONCLUSIONS
In this paper, we have focussed on the applicability
of process mining in the healthcare domain. For our
case study, we have used data coming from a non-
trivial care process of the AMC hospital. We focussed
on obtaining insights into the careflow by looking at
the control-flow, organizational and performance per-
spective. For these three perspectives, we presented
some initial results. We have shown that it is pos-
sible to mine complex hospital processes giving in-
sights into the process. In addition, with existing tech-
niques we were able to derive understandable models
for large groups of patients. This was also confirmed
by people of the AMC hospital.
Furthermore, we compared our results with a
flowchart for the diagnostic trajectory of the gynae-
cological oncology healthcare process, and where a
top-down approach had been used for creating the
flowchart and obtaining the logistical data (Elhuizen
et al., 2007). With regard to the flowchart, compa-
rable results have been obtained. However, a lot of
effort was needed for creating the flowchart and ob-
taining the logistical data, where with process mining
there is the opportunity to obtain these kind of data in
a semi-automatic way.
Unfortunately, traditional process mining ap-
proaches have problems dealing with unstructured
processes as, for example, can be found in a hospital
environment. Future work will focus on both devel-
oping new mining techniques and on using existing
techniques in an innovative way to obtain understand-
able, high-level information instead of “spaghetti-
like” models showing all details. Obviously, we plan
to evaluate these results in healthcare organizations
such as the AMC.
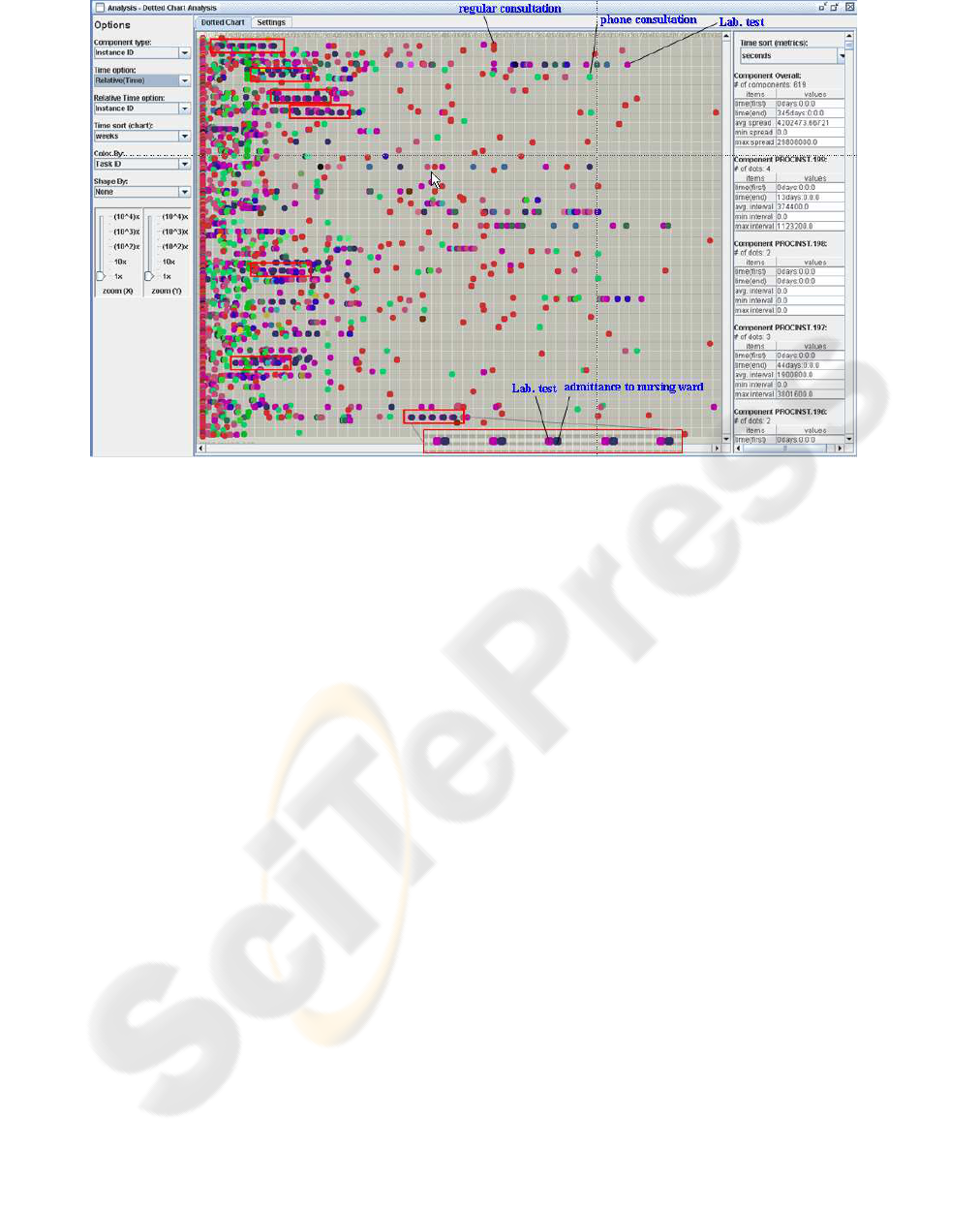
Figure 6: Dotted Chart.
ACKNOWLEDGEMENTS
This research is supported by EIT, NWO-EW, the
Technology Foundation STW, and the SUPER project
(FP6). Moreover, we would like to thank the many
people involved in the development of ProM.
REFERENCES
Anyanwu, K., Sheth, A., Cardoso, J., Miller, J., and Kochut,
K. (2003). Healthcare Enterprise Process Develop-
ment and Integration. Journal of Research and Prac-
tice in Information Technology, 35(2):83–98.
Dumas, M., van der Aalst, W., and ter Hofstede, A. (2005).
Process-Aware Information Systems: Bridging People
and Software through Process Technology. Wiley &
Sons.
Elhuizen, S., Burger, M., Jonkers, R., Limburg, M.,
Klazinga, N., and Bakker, P. (2007). Using Busi-
ness Process Redesign to Reduce Wait Times at a
University Hospital in the Netherlands. The Joint
Commission Journal on Quality and Patient Safety,
33(6):332–341.
Lenz, R., Elstner, T., Siegele, H., and Kuhn, K. (2002). A
Practical Approach to Process Support in Health In-
formation Systems. Journal of the American Medical
Informatics Association, 9(6):571–585.
van der Aalst, W., Reijers, H., and Song, M. (2005). Discov-
ering Social Networks from Event Logs. Computer
Supported Cooperative Work, 14(6):549–593.
van der Aalst, W., Reijers, H., Weijters, A., van Dongen,
B., de Medeiros, A. A., Song, M., and Verbeek, H.
(2007a). Business process mining : an industrial ap-
plication. Information Systems, 32(5).
van der Aalst, W., van Dongen, B., G¨unther, C., Mans, R.,
de Medeiros, A. A., Rozinat, A., Rubin, V., Song,
M., Verbeek, H., and Weijters, A. (2007b). ProM
4.0: Comprehensive Support for Real Process Anal-
ysis. In Kleijn, J. and Yakovlev, A., editors, Ap-
plication and Theory of Petri Nets and Other Mod-
els of Concurrency (ICATPN 2007), volume 4546 of
Lecture Notes in Computer Science, pages 484–494.
Springer-Verlag, Berlin.
van der Aalst, W., van Dongen, B., Herbst, J., Maruster,
L., Schimm, G., and Weijters, A. (2003). Workflow
Mining: A survey of Issues and Approaches. Data
and Knowledge Engineering, 47(2).
van der Aalst, W., Weijters, A., and Maruster, L. (2004).
Workflow Mining: Discovering Process Models from
Event Logs. IEEE Transactions on Knowledge and
Data Engineering, 16(9):1128–1142.
van Dongen, B., Busi, N., Pinnaand, G., and van der Aalst,
W. (2007). An Iterative Algorithm for Applying the
Theory of Regions in Process Mining. BETA Work-
ing Paper Series, WP 195, Eindhoven University of
Technology, Eindhoven.
Weijters, A. and van der Aalst, W. (2003). Rediscovering
Workflow Models from Event-Based Data using Lit-
tle Thumb. Integrated Computer-Aided Engineering,
10(2):151–162.
