
A SMART MEDICINE MANAGER DELIVERING HEALTH CARE
TO THE NETWORKED HOME AND BEYOND
An Overview of the iCabiNET System
Martín López-Nores, José J. Pazos-Arias, Jorge García-Duque and Yolanda Blanco-Fernández
Department of Telematics Engineering, University of Vigo, Spain
Keywords:
Remote health care, smart medicine packaging, residential networks, semantic reasoning.
Abstract:
Misuse of prescription and over-the-counter drugs is a growing problem that impinges heavily on the well-
being of people and the economics of public health systems. Most commonly, misuses arise from forgetfulness
or lack of information about drugs and their interactions, hence there is much place for solutions to automati-
cally monitor medicine intake, issue reminders and deliver medical advice. This paper presents a system that
accomplishes these tasks by harnessing recent advances in smart medicine packaging, residential networks
and semantic reasoning. Such a combination yields a medicine manager featuring great precision in drug
monitoring, plus unprecedented capabilities to reach the users and provide them with valuable information.
1 INTRODUCTION
Recent statistics reveal that the misuse of prescrip-
tion and over-the-counter drugs is becoming a major
problem as life expectancy increases and the range
of medications grows, to the point of being as dan-
gerous and costly as many illnesses (Sullivan et al.,
1990; Downey et al., 2000). To ground this signifi-
cance in numbers, consider the following USA facts,
retrieved from (American Heart Association, 2007;
Akram, 2000; Office of Applied Studies, 2005):
• 50% of filled prescriptions are taken incorrectly.
In the worst extreme, 65% of the elderly fail to
comply with their medication regimens, with 26%
of those errors being potentially serious.
• 23% of nursing home admissions are due to abuse
or non-compliance, costing $31.3 billion per year
and affecting 380,000 people. The same happens
with 10% of hospital admissions, costing $15.2
billion and affecting 3.5 million people.
• $75 billion are annually spent on preventable hos-
pitalizations due to medication misuse, plus other
$30 billion on additional medications prescribed
after non-compliance.
• 125,000 deaths occur annually due to drug inter-
actions.
As noted in (Hughes et al., 2001; MedPrompt,
2007), misuses typically arise from forgetfulness or
lack of information about the different drugs avail-
able. This has raised enormous interest in developing
solutions to automatically monitor medicine intake,
issue reminders and deliver medical advice (Bricon-
Souf and Newman, 2007). Some precedents for this
idea can be found in (Wan, 1999; Ho et al., 2005),
with embedded systems that employed RFID
1
de-
vices to recognize medicaments and weighing scales
to guess the doses available. However, those systems
are impractical due to the following drawbacks:
• The weighing scales require the users to pick one
medicament at a time and put it back before pick-
ing another. This is a cumbersome discipline to
follow in many cases, entailing a clear risk of
monitoring imprecision.
• The means available to reach the users are very
limited, merely consisting of embedded screens,
lights or alarms. Thus, it is not possible to pre-
vent forgetfulness if the user happens to be out of
home, or simply in a room where he/she cannot
see the lights or hear the alarms.
• Finally, the previous systems rely on the assump-
tion that people use a medicine cabinet as the
1
RFID: Radio Frequency IDentification.
167
L
´
opez-Nores M., J. Pazos-Arias J., Garc
´
ıa-Duque J. and Blanco-Fern
´
andez Y. (2008).
A SMART MEDICINE MANAGER DELIVERING HEALTH CARE TO THE NETWORKED HOME AND BEYOND - An Overview of the iCabiNET System.
In Proceedings of the First International Conference on Health Informatics, pages 167-172
Copyright
c
SciTePress
only place for medication keeping. Nevertheless,
polling data reveals that this may not be true in
as many as 90% of the cases, as people tend to
store their medicines in various places around the
house (Fishkin and Consolvo, 2003).
With these problems in mind, we introduce in this
paper a system, called the iCabiNET, that tackles the
aforementioned issues by integrating recent advances
in various areas of research. The basic ideas behind
this system are explained in the overviewof Section 2.
After that, Section 3 describes two usage scenarios
to illustrate the benefits and the potential uses of our
approach. Section 4 provides technical details of an
implementation capable of realizing those scenarios.
Finally, Section 5 includes a summary of conclusions
and motivates future work.
2 SYSTEM OVERVIEW
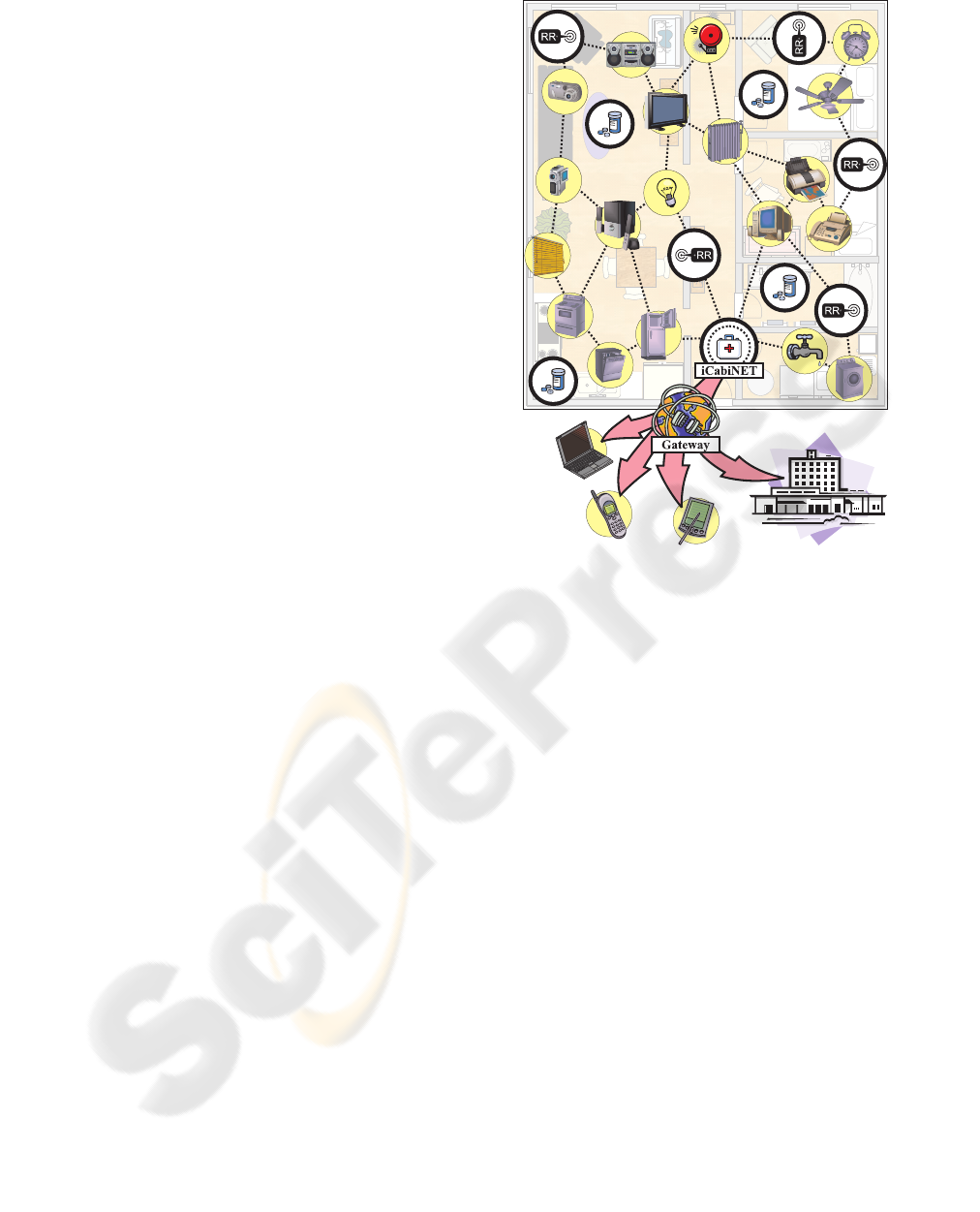
As shown in Fig. 1, we have conceived the iCabiNET
as a new element of a residential network, ready to
communicate directly with other appliances installed
in a house, and with the outside world through a res-
idential gateway. Within this setting, the operation of
the system consists of two major steps, to be detailed
in the following subsections:
• Gathering information about available drugs and
doses.
• Processing that information to identify and react
to actual or potential misuses.
2.1 Gathering Information
In what concerns the gathering of information about
available medicines and doses, the iCabiNET can
coexist with any of the previous monitoring so-
lutions (Wan, 1999; Floerkemeier and Siegemund,
2003; Ho et al., 2005), given that they propagate
data over the residential network. Furthermore, we
have introduced support for the smart packagingtech-
nologies currently promoted by stakeholders of the
pharmaceutical industry. As explained in (Goodrich,
2006; Harrop, 2006), the idea is to integrate RFID
devices and different types of sensors with the pack-
aging of the medicines, to allow tracking not only
medicine names, but also the doses available with no
additional equipment. A common example is that
of smart blister packs, which record the removal of
a tablet simply by breaking an electric flow into the
RFID’s integrated circuit; other possibilities exist for
liquid medicines, ointments and so on.
Figure 1: The iCabiNET system in a residential network.
Smart packaging enables the iCabinet to monitor
the intake of drugs from anywhere, with the highest
precision, with no need to keep all drugs in a unique
place, and with no risk of mistaking one drug for
another. The system simply gathers information by
polling RFID readers deployed around the house (the
RR devices in Fig. 1) or connected to the residential
network from other places (e.g. from the office).
2.2 Reacting to Misuses
Primarily, the iCabiNET is intended to enforce some
medication guidelines, such as “
the user should take
one of these tablets every 4 to 6 hours
”. Accordingly,
in the operational scheme of the system (see Fig. 2),
there is a ‘Watchdog’ module devoted to continually
supervising the information gathered about available
medicines and doses, to check that the former remain
in good condition and the latter decrease correctly
with time. This module detects odd circumstances
driven by rules that may involve user conditions (like
age, gender or previous diseases), and notifies those
circumstances by triggering different types of events.
The events are the input for a second module, the
‘Actuator’, to decide what actions will be performed
to issue warnings or deliver health care information to
the user. This module firstly considers generic state-
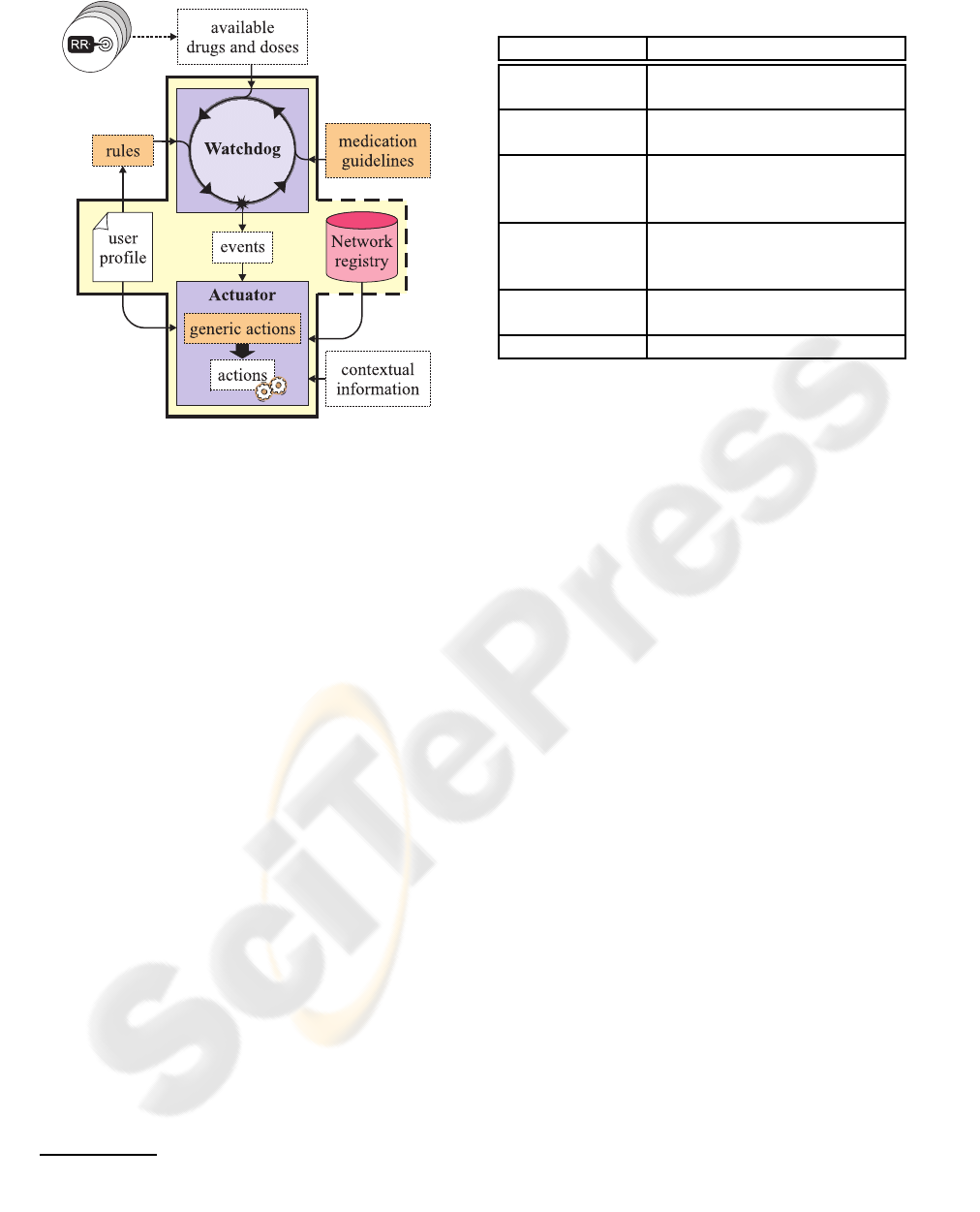
Figure 2: The operational scheme of the iCabiNET.
ments with no liaison to specific appliances, such as
those of Table 1. Then, it instantiates those statements
on demand, using the appliances it finds most conve-
nient. In doing so, the ‘Actuator’ takes into account
data from the user’s profile, contextual information
provided by external devices (e.g. about whether the
user is sleeping, watching TV or out of home) and
descriptions stored in a network registry of the ap-
pliances connected to the residential network and the
operations they can do.
2
Thus, for example, a “
warn
the user
” action can be automatically made to trig-
ger an alarm clock, to interrupt a TV program and
display some message on screen, or to make a tele-
phone call. The enormous range of possibilities en-
abled by the residential network to reach the user is
precisely the point that makes the iCabiNET most ad-
vantageous with regard to previous systems.
Orchestrating appliances as explained above re-
quires the iCabiNET to take a great number of de-
cisions that cannot be determined beforehand. No-
ticeably, this intelligence is not catered for by the cur-
rent residential network standards (Baxter, 2005), be-
cause they merely provide for executing pre-compiled
programs (usually referred to as bundles). Thus, it
would be necessary to write different versions of the
same behavior for all the possible configurations of
devices in and out of home, even considering the dif-
ferent ways to invoke the same operations for appli-
ances assembled by different manufacturers. Such an
approach would obviously exhibit limited flexibility
2
The registry can reside in the iCabiNET or in any other
device permanently connected to the residential network,
most typically the residential gateway.
Table 1: Some events types and actions they might trigger.
Event Action
Oblivion “
Wait up to 90 minutes before
reminding the user
”
Expiration “
Deliver increasingly serious
warnings day after day
”
Depletion “
Arrange an appointment with
the doctor to get a new pre-
scription
”
Interaction “
Recommend an innocuous
combination of drugs with the
same effects
”
Discontinuation “
Restart the medication at a
lower dose
”
Abuse “
Warn the local authorities
”
and severe scalability problems. The iCabiNET’s so-
lution to these questions builds upon two main ideas:
• The first idea is to deliver virtual bundles contain-
ing no implementation, but rather process flows
that arrange medication guidelines, user condi-
tions, rules, events and generic actions in semi-
formal constructs.
• The second idea is to enhance the network registry
with mechanisms from the Semantic Web (Anto-
niou and van Harmelen, 2004), using ontologies
as unique conceptualizations of what the different
appliances can do and how: operations, input and
output parameters, quality attributes, etc.
As shown in Fig. 3, when a virtual bundle appears
in the system, the iCabiNET creates one implementa-
tion bundle to supervise the occurrence of events in
the corresponding process flow. Then, when it is time
to perform some actions, the implementation bun-
dle uses matching techniques like those of (Paolucci
et al., 2002; Fujii and Suda, 2005) to find the most
suitable appliances at the moment (A, B, D and E in
Fig. 3) and start invoking their operations in the spec-
ified order. This approach promotes openness and in-
teroperability, making it possible to deliver the same
virtual bundles to everybody, regardless of the par-
ticular appliances owned by each user. Furthermore,
nothing has to be re-programmed when any element
changes, and it is even possible to incorporate newly-
invented devices and functionalities with a simple up-
date of the ontologies.
Following the commented scheme, several virtual
bundles are preloaded in the iCabiNET to deal with
common tasks, such as checking interactions between
available drugs by accessing remote data bases, or
downloading process flows to drive the monitoring of
new drugs acquired by the user. Other virtual bundles
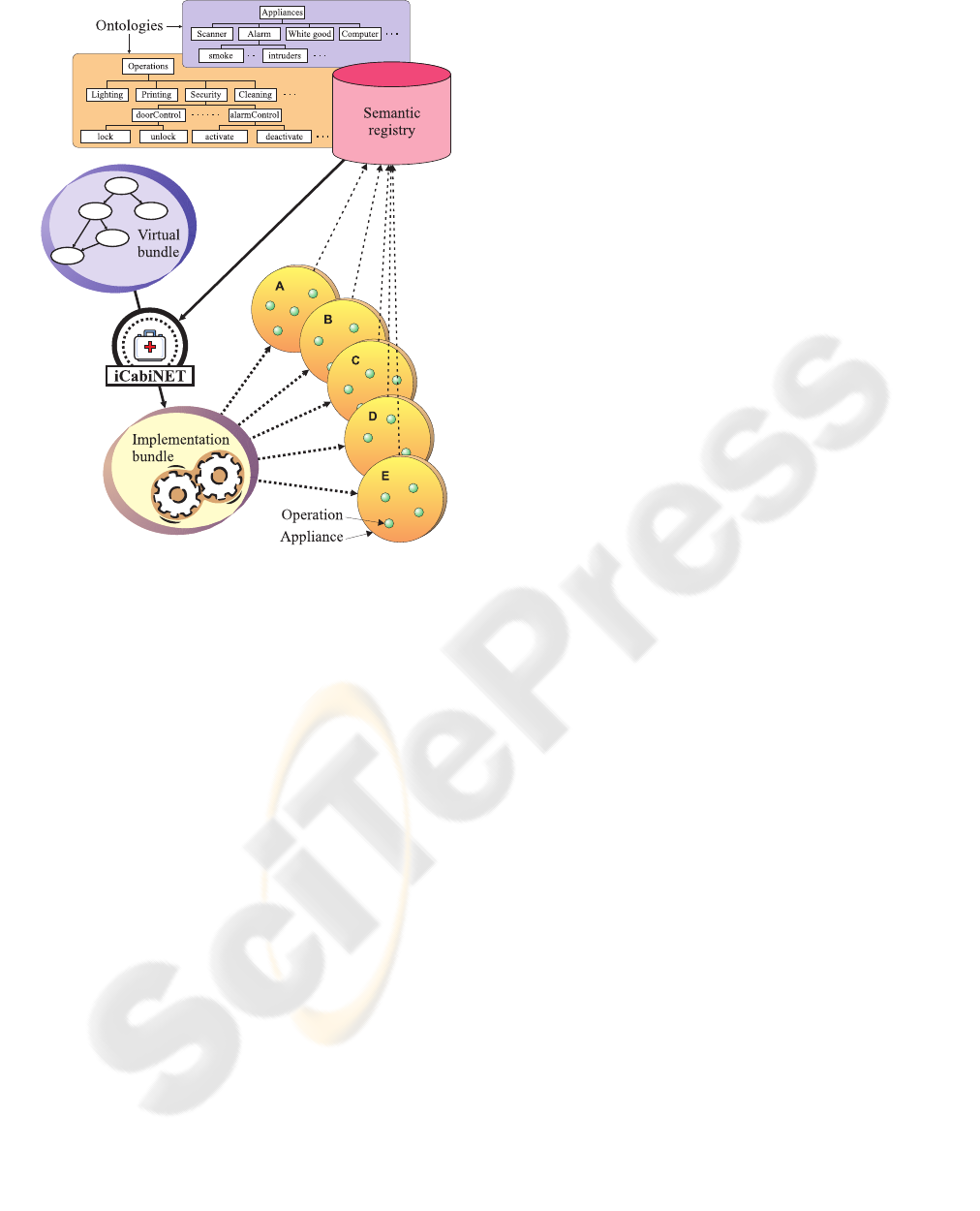
Figure 3: Activating appliances from virtual bundles.
can be entered by the user or by authorized external
entities, like health institutions (they know what the
user needs) or pharmaceutical companies (they know
the best way to take their products).
3 USAGE SCENARIOS
Having explained the essentials of the iCabiNET, we
now describe two usage scenarios to illustrate the
range of functionalities it can deliver. The technolo-
gies employed to make these scenarios possible are
described in Section 4.
3.1 Scenario #1
Ann is having breakfast before going to work, and
switches on the radio to hear the first news of the
day. When she is about to turn off the apparatus, the
iCabiNET reminds her of the medicines she should
carry, playing a pre-recorded message. Later, follow-
ing the prescription issued by the doctor (loaded into
the iCabiNET directly from the health center), Ann
receives an SMS message in her mobile phone every
three hours to remember taking her drugs. At the end
of the day, when Ann is back in her house, the iCab-
iNET attempts to check that the available doses have
decreased as expected, but it turns out that Ann has
left them behind. In this case, the iCabiNET rings the
in-home telephone to ask Ann whether she has taken
the medicines correctly; she replies affirmatively by
pressing the asterisk key. During the night, the alarm
clock in Ann’s bedroom will be responsible for wak-
ing her up when it is time for new doses.
3.2 Scenario #2
While having a walk outside, Bob decides to buy an
over-the-counter drug to treat his allergy to pollen.
Afterwards, when he enters his house, the iCabiNET
records the tablets he has bought, and automatically
downloads medication guidelines for adults from the
manufacturer. A few days later, Bob is watching TV
in the living room. When it is time to take a pill, the
iCabiNET pops up a reminder on the screen, indicat-
ing the drug’s commercial name, a photograph of its
packaging and the recommended dose. For the best
comfort, the system starts flashing the lights of the
room where Bob had left the tablets the last time he
took one. As Bob takes a new dose, the iCabiNET
finds that the pills are running out; so, when he sits
back in the sofa, he is faced with an interactive TV
application that he can use to buy new supplies from
an online drugstore. Bob uses the remote control to
enter shipping and payment details, and takes the op-
portunity to buy some throat lozenges he likes.
4 PROTOTYPE
IMPLEMENTATION
In order to assess the feasibility of the approach de-
scribed in Section 2, we have developed and tested
a prototype of the iCabiNET taking the scenarios of
Section 3 as a reference of the functionalities it should
provide. It is worth noting that the system needs not
be a standalone device, hence we built it as a software
package to run on any device that is permanently con-
nected to a residential network. Within this perspec-
tive, we strove to employ standard technologies and
open-source software packages.
As the basis for our implementation, we chose the
frameworkproposed by OSGi (OSGi Alliance, 2005),
which is nowadays the most popular standard for res-
idential networks. This platform is advantageous for
various reasons: (i) it supports different widespread
protocols for secure and non-secure communication
among appliances in home and outside, (ii) it defines
a cooperative model where appliances can dynami-
cally discover and invoke the operations provided by
others, and (iii) it enables remote management of the

appliances and the operations they provide. From
among other possibilities, we implemented the iCab-
iNET as an OSGi bundle using the open software
packages from the OSCAR
3
project, because they are
particularly well documented.
Just like the other residential network standards,
OSGi provides no support for orchestrating appli-
ances according to virtual bundles as described in
Section 2.2. To this aim, inspired by the work
of (Slomiski, 2006), we opted to borrow solutions
from the most mature related field of research: Web
Services. Therefore, we express the process flows us-
ing the BPEL language (Juric, 2006), which provides
constructs to describe arbitrarily complex processes,
focusing on the invocation of operations and the flow
of control between them. There are many tools sup-
porting this language, offering plenty of facilities to
create, edit and execute process flows. We have devel-
oped the core of the iCabiNET over the ActiveBPEL
4
engine, introducing the following enhancements:
• The BPEL flows can include declarative rules
written in Jess
5
to drive the generation of events
related to the intake of medicines. Accordingly,
the ‘Watchdog’ module of Fig. 2 incorporates a
Jess execution environment, which is the only
protected part of our implementation —it is only
free for academic purposes.
• The actions in the BPEL flows include concepts
of the SOUPA and GUMO ontologies presented
in (Chen et al., 2004; Heckmann et al., 2005),
which are also used in a semantic registry main-
tained by the iCabiNET itself. With those bases,
plus the context-aware features of (Gu et al.,
2004; Zhang et al., 2005), the ‘Actuator’ mod-
ule of Fig. 2 uses the Protégé OWL API
6
to apply
the same semantic matching mechanisms we de-
signed for (Díaz-Redondo et al., ress) —the rea-
soning abilities are not linked to any specific do-
main of application.
As regards the interactive applications presented
to the user to realize actions in the virtual bundles
(e.g. the online drugstore of Scenario #2), the au-
thors of (Ramos-Cabrer et al., 2006) proposed a way
to merge OSGi with the MHP standard of applications
for Digital TV (Digital Video Broadcasting, 2003).
We have extended those mechanisms to support ap-
plications for PCs and mobile devices as well, and to
handle descriptions of those applications also in terms
of the SOUPA and GUMO ontologies.
3
http://oscar.objectweb.org
4
http://www.activebpel.org
5
http://herzberg.ca.sandia.gov/jess
6
http://protege.stanford.edu
All the code aforementioned pieces of the iCab-
iNET are written in Java, and so we used this lan-
guage for the code to glue those elements together.
That code was executed by a J2ME virtual machine
running on a residential gateway. Out of the iCabi-
NET itself, in what concerns the gathering of infor-
mation about the availability and intake of medicines,
we completed the settings for our trials with purpose-
built smart blister packs, because smart packaging
technology is not yet available in retail drugs (only
in clinical trials). Besides, we developed our own
RFID readers for those blister packs, since we did not
find suitable alternatives in the market ready to work
within an OSGi network.
5 CONCLUSIONS
Technology may be an important aid to fight the wor-
risome health problems and the increasing economic
costs due to the misuse of prescription and over-the-
counter drugs. With this vision in mind, we have de-
signed and implemented the iCabiNET system, which
is the first outcome of a multidisciplinary research ef-
fort to put technology to the service of better medica-
ment monitoring and management.
The iCabiNET can be regarded as a powerful ex-
tension of previously-existing solutions to monitor
medicine intake (e.g. the embedded systems of (Wan,
1999; Floerkemeier and Siegemund, 2003; Ho et al.,
2005)), introducing the ability to issue warnings and
deliver medical advice using any appliance connected
to a residential network. Eventually, when the smart
packaging technologies finally take up the market,
the iCabiNET approach will actually replace that of
previous systems, providing the greatest flexibility
and precision in monitoring, limitless possibilities to
reach the user using whichever technological means,
and unprecedented capabilities to interact with health
institutions, drug manufacturers and retailers.
Also, the iCabiNET can be seen as introducing
support to monitor the intake of drugs in previously-
existing platforms to provide health care information
through Internet-enabled personal computers (Roine
et al., 2001), Digital TV (Simonov et al., 2007) or
mobile devices (Komninos and Stamou, 2006). In
this regard, we can emphasize the integrated and
technology-neutral solution achieved with the seman-
tic reasoning features, which render an open environ-
ment with feasible and scalable exploitation models.

ACKNOWLEDGEMENTS
This work has been supported by the Spanish Min-
istry of Education and Science (Project TSI2007-
61599).
REFERENCES
Akram, G. (2000). Over-the-counter medicines: An emerg-
ing and neglected drug abuse. Journal of Substance
Use, 5(2):136–142.
American Heart Association (2007).
http://www.americanheart.org.
Antoniou, G. and van Harmelen, F. (2004). A Semantic Web
primer. The MIT Press.
Baxter, L. (2005). Residential networks. Thomson Delmar
Learning.
Bricon-Souf, N. and Newman, C. (2007). Context aware-
ness in health care: A review. International Journal
of Medical Informatics, 76(1):2–12.
Chen, H., Perich, F., Finin, T., and Joshi, A. (2004).
SOUPA: Standard Ontology for Ubiquitous and Per-
vasive Applications. In MOBIQUITOUS’04, 1st An-
nual International Conference on Mobile and Ubiqui-
tous Systems: Networking and Services, Cambridge,
USA.
Díaz-Redondo, R. P., Fernández-Vilas, A., Ramos-Cabrer,
M., Pazos-Arias, J. J., García-Duque, J., and Gil-
Solla, A. (In press). Enhancing residential gateways:
A semantic OSGi platform. IEEE Intelligent Systems.
Digital Video Broadcasting (2003). The Multimedia Home
Platform specification. ETSI standard TS 102 812.
http://www.mhp.org.
Downey, G., Hind, C., and Kettle, J. (2000). The abuse and
misuse of prescribed and over-the-counter medicines.
Hospital Pharmacist, 7(9):242–250.
Fishkin, K. and Consolvo, S. (2003). Results of medication
questionnaire #1. Technical Report IRS-TR-03-002,
Intel Research.
Floerkemeier, C. and Siegemund, F. (2003). Improving
the effectiveness of medical treatment with pervasive
computing technologies. In Ubicomp’03 Workshops,
Seattle, USA.
Fujii, K. and Suda, T. (2005). Semantics-based dynamic
service composition. IEEE Journal on Selected Areas
in Communications, 23(12):2361–2372.
Goodrich, N. (2006). Smart packaging. http://www.pac.ca/
/Chapters/ONSmartPkgDownloads.html.
Gu, T., Pung, H., and Zhang, D. (2004). Toward an OSGi-
based infrastructure for context-aware applications.
IEEE Pervasive Computing, 3(4):66–74.
Harrop, P. (2006). Opportunities in pharmaceutical RFID
and smart packaging. IDTechEx.
Heckmann, D., Schwartz, T., Brandherm, B., Schmitz,
M., and von Wilamowitz-Moellendorff, M. (2005).
GUMO: The General User Model Ontology. In
UM’05, 10th International Conference on User Mod-
eling, Edinburgh, UK.
Ho, L., Moh, M., Walker, Z., Hamada, T., and Su, C.-F.
(2005). A prototype on RFID and sensor networks
for elder healthcare. In SIGCOMM’05 Workshops,
Philadelphia, USA.
Hughes, C. M., McElnay, J. C., and Fleming, G. F. (2001).
Benefits and risks of self medication. Drug Safety,
24(14):1027–1037.
Juric, M. (2006). Business Process Execution Language for
Web Services. Packt Publishing.
Komninos, A. and Stamou, S. (2006). HealthPal: An in-
telligent personal medical assistant for supporting the
self-monitoring of healthcare in the ageing society. In
UbiHealth’06, 4th International Workshop on Ubiq-
uitous Computing for Pervasive Healthcare Applica-
tions, Orange County, USA.
MedPrompt (2007). http://www.medprompt.com.
Office of Applied Studies (2005). Na-
tional survey on drug use & health.
http://www.drugabusestatistics.samhsa.gov.
OSGi Alliance (2005). Open Service Gateway initiative.
http://www.osgi.org.
Paolucci, M., Kawamura, T., Payne, T., and Sycara, K.
(2002). Semantic matching of Web Services capa-
bilities. In ISWC’02, 1st International Semantic Web
Conference, Sardinia, Italy.
Ramos-Cabrer, M., Díaz-Redondo, R., Fernández-Vilas, A.,
Pazos-Arias, J., and García-Duque, J. (2006). Control-
ling the smart home from TV. IEEE Transactions on
Consumer Electronics, 52(2):421–429.
Roine, R., Ohinmaa, A., and Hailey, D. (2001). Assessing
telemedicine: A systematic review of the literature.
Canadian Medical Association Journal, 165(6):765–
771.
Simonov, M., Brizzi, P., Gavelli, M., and Sciarappa, A.
(2007). TV for health: One-to-one personalized con-
tent delivery in living room. In EuroITV’07 Work-
shops, Amsterdam, The Netherlands.
Slomiski, A. (2006). On using BPEL extensibility to imple-
ment OGSI and WSRF grid workflows. Concurrency
and Computation: Practice and Experience, 18(10).
Sullivan, S., Kreling, D., and Hazlet, T. (1990). Noncompli-
ance with medication regimens and subsequent hospi-
talizations: A literature analysis and cost of hospital-
ization estimate. Journal of Research in Pharmaceu-
tical Economics, 2:19–33.
Wan, D. (1999). Magic Medicine Cabinet: A situated por-
tal for consumer healthcare. In HUC’99, 1st Interna-
tional Symposium on Handheld and Ubiquitous Com-
puting, Karlsruhe, Germany.
Zhang, D., Gu, T., and Wang, X. (2005). Enabling
context-aware smart home with Semantic Web tech-
nologies. International Journal of Human-friendly
Welfare Robotic Systems, 6(4):12–20.
