
A WIRELESS ACQUISITION SYSTEM FOR MONITORING THE
INFLUENCE OF LOADS ON VERTEBRAL COLUMN
BEHAVIOUR
João Eduardo Castro Ribeiro
ξ
and João Paulo Pereira do Carmo
χ
ξχ
Instituto Politécnico de Bragança, Bragança, Portugal
ξ
Departamento de Tecnologia Mecânica
χ
Departamento de Electrotecnia
Keywords: Biotelemetry, biomechanical and Wireless electromyography (EMG).
Abstract: This paper presents a wireless acquisition module (WAM). This allows the monitoring of heavy loads
influence on vertebral column’s behaviour. Each module makes the electromyography (EMG), to measure
the electric potentials on the iliocostalis and longissimus thoracis muscles, and use a dual-axis accelerometer
to get the movements of the body, in order to obtain the complete behaviour of the vertebral column. The
solution chosen to transmit the body’s measured signals for further processing, is a wireless link working in
the 433 MHz ISM band. The acquired information is transmitted with a maximum rate of 40 kbps, a
resolution of 9.8 μV, and accommodates two analog channels. An analog channel with differential input
connected to the electrodes, is used to measure the EMG signal, while the remained channel is used in the
patient’s movements measurements. The dimensions of the proposed acquisition system are
about 7×5×2 cm, and will help to understand the influence of heavy loads as a risk factors in the vertebral
column, such as the scoliosis and lordosis.
1 INTRODUCTION
The human posture has been an object of studies in
biomechanics, once some deviations of structural
and functional positions induce an unbalanced body.
These deviations usually, affects the vertebral
column and are caused by physical efforts, bad
postures in work, deficiency in sustentation muscles,
infections and congenital causes. The main
pathologies of vertebral column caused by the
referred deviations, are the scoliosis and lordosis.
Sometimes these pathologies appears in children
when they carry the heavy backpacks on the backs,
in this case, it’s very important monitoring the
influence of loads (backpack weight) in vertebral
column behaviour.
The vertebral column has very important functional
requirements, which the most significant are: it
carries and supports the thoracic cage, maintaining
the balance between it and abdominal cavity; it gives
attachment to many muscles of the pectoral and
pelvic girdles; it provides anchorage for many
powerful muscles, which move the vertebral
column, these same muscles maintaining the balance
and erectness of the human trunk; it acts as shock
absorber, by virtue of its curvatures and the
intervertebral discs, receiving and distributing the
impacts associated with the dynamic functioning of
the body; it is able, by virtue of its flexibility, to
produce and accumulated moments of force as well
as to concentrate and transmit forces receiving from
other parts of the body (Palastanga et al, 2002).
When someone carries a heavy object like a
backpack on the back, the center of gravity of body
changes and it will be necessary some adaptations to
maintain the balance, these adaptations are possible
because the action of powerful muscles like
iliocostalis or longissimus thoracis, and the relative
movement among the intervertebral discs. In the
children who carries heavy backpacks repeatedly
and for long time they could suffer injuries in the
vertebral column that can develop pathologies like
scoliosis. Figure 1 show vertebral column with a
scoliosis.
The study of influence of backpack weighs on the
vertebral column of children is an important issue,
that has been worked by many researchers for years
(Nissinen at al, 1994; Widhe, 2001; Skaggs et al,
2006).
In this work it is used a different approach, applying
indirect information, using the electrical potential
233
Eduardo Castro Ribeiro J. and Paulo Pereira do Carmo J. (2008).
A WIRELESS ACQUISITION SYSTEM FOR MONITORING THE INFLUENCE OF LOADS ON VERTEBRAL COLUMN BEHAVIOUR.
In Proceedings of the First International Conference on Biomedical Electronics and Devices, pages 233-237
DOI: 10.5220/0001049302330237
Copyright
c
SciTePress

generated by the muscles, when they contract and
when they are rest. The technique which could
measure this electrical potential is the
electromyography (EMG). Based on the results of
EMG, combined with the movements of the body,
measured by the accelerometers, it is possible to
know by numerical simulation, the displacement
occurred on the insertions points between the
muscles and the vertebral column
(Conceição, F. et al, 2007; Pato, M. et al, 2007).
Using these values of displacements in a finite
element code, like ANSYS®, we can compute the
value of stress field in the vertebral column,
especially it is possible to observe where are the
points more affected and the respective stress value.
Figure 1: Radiograph showing a vertebral column with a
scoliosis.
2 KINEMATICS
The skeletal system of the trunk comprises the
pelvis, vertebral column and rib cage. The vertebral
column is divided into four regions: cervical;
thoracic; lumbar and sacrum.
The vertebral column is a flexible rod with seven
mobile segments in the cervical region, twelve
segments in the thoracic region and five segments in
the lumbar region. The fourth region of the vertebral
column, the sacral-coccyx region, includes nine
fused vertebrae that together with the right and left
ilia form the pelvis.
Two adjacent vertebrae and their interposed
intervertebral disk form a motion segment of the
vertebral column. Each segment has six degrees of
freedom (DOF). In the vertebral column, there are
two types of joints: the intervertebral joints between
the vertebrae and adjacent disks and the facet joints
between the facets (articular processes) of the
neighbouring vertebrae. Movement at the
intervertebral and facet joints of the same motion
segment is coupled.
Figure 2: The regions of the vertebral column (Bridwell,
2007).
The intervertebral disks are flexible spacers between
adjacent vertebrae. The disk consists of a central
nucleus pulposus, which is a ball of hydrophilic
jelly, and the outer annulus fibrosus, a series of
laminae formed by collagen fibers. The disc height
(thickness) increases from the cervical lumbar
region from about 3 mm to 9 mm.
Any change in vertebral column posture involves the
joined movement of several motion segments.
People cannot move the individual motion segments
independently.
Kinematics of the vertebral column deals either with
the specific motion segments or with the entire
region of the vertebral column or
both (Zatsiorsky, 1998).
Each of the motion segments has six DOF: because
the intervertebral disks can deform, the vertebrae, in
addition to being able to rotate, and translate. The
vertebral column as whole can produce only three
movements: flexion-extension, lateral flexion and
axial rotation. The vertebral column movement
results from concurrent rotation and translation of
the vertebrae. The amount of motion available at
various motion segments depends mainly on the size
of the disks, while the orientation of the facet joint
surfaces, which changes from region to region,
defines the direction of the allowable movement.
The relative movement of the motion segments of
the vertebral column is allowed by an elastic
connection provide by the intervertebral disks.
Vertebral flexion and extension causes compression
in one part of the disk and traction in another part.
When a relative motion between two consecutive
vertebrae is analyzed, the lower vertebra is usually
considered a fixed body and the upper vertebra is
treated as moving body. The coordinate axes are
taken along the inferior and posterior margins of the
stationary, lower vertebra.
BIODEVICES 2008 - International Conference on Biomedical Electronics and Devices
234
Because the disks can deform, the same resultant
force and torque being applied to various vertebrae
produces different movements depending on the disk
stiffness and its dimensions, height and diameter.
The rotation and translation of the vertebrae results
in a torsion and bending of intervertebral disks. In
case of torsion, the disk is subjected to equal and
opposite twisting couples at the two adjacent
vertebrae. The axial rotation, α
a
, is the angle by
which the top vertebra turns with respect to the
bottom vertebra. For a disk of a height H, radius r,
and cross-sectional area A, on which a torque M
a
is
acting, the angle of twist is:
a
a
p
M
H
GI
α
=
(1)
where G is the shear modulus and I
p
is the polar
moment of inertia. The bending occurs when the line
of force does not coincide with the symmetry axis of
de column, and appears a bending stress
(Adams and Dolan, 1991). The equation relating
angular displacement of the disk, α
b
, with the
applied bending moment, M
b
, is
b
b
d
M
H
EI
α
=
(2)
where E is the modulus of elasticity and I
d
is a
diametral moment of inertia, I
d
= 0.5I
p
.
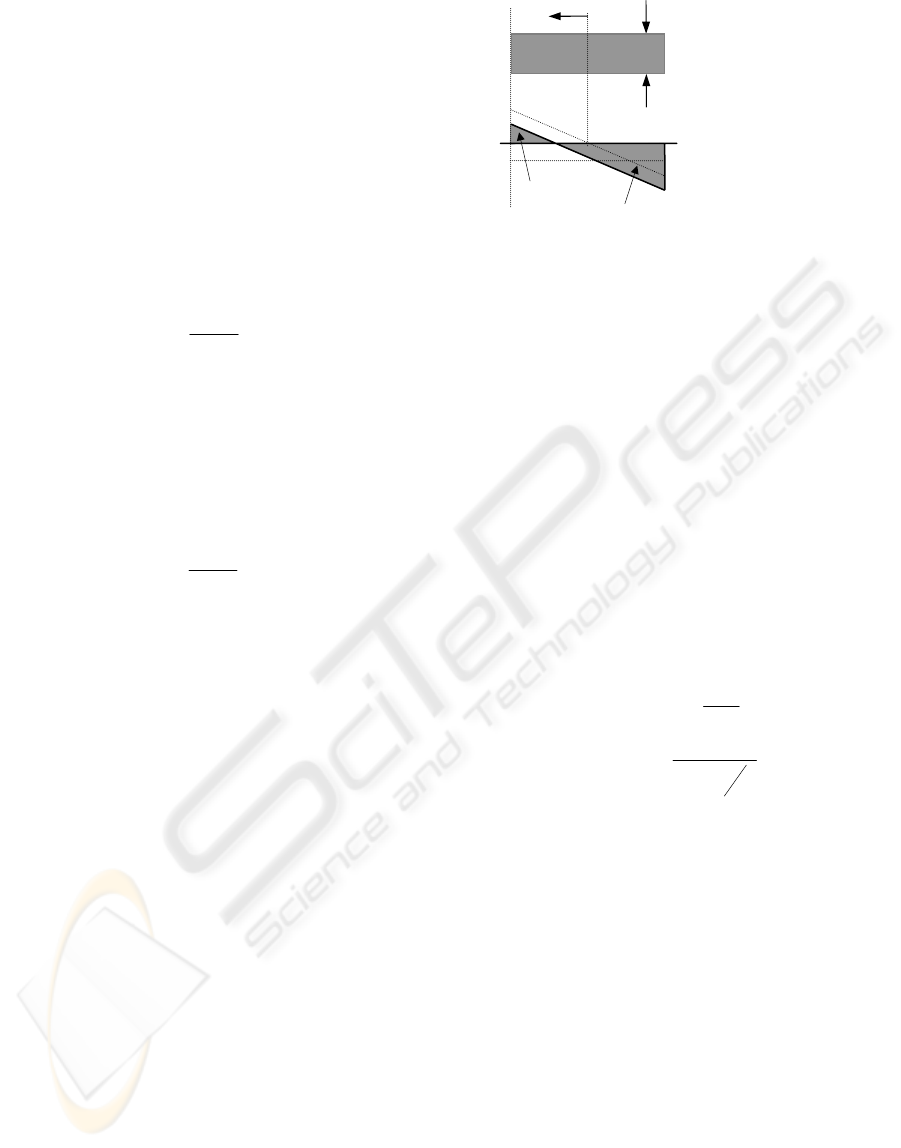
Considering that the column is loaded with two
forces, F and –F, acting in opposite directions along
the same line of action.
The line of action does not pass through the center
of gravity (G). The center of gravity is the location
of the resultant force acting in compression and
proportional to the elements of area. The column is
under joint action of compression and bending and is
stressed correspondingly (Adams and Dolan, 1988).
The compressive stress is F/A, where A is the area
of the horizontal section. The bending stress is
M.y/I, where M is the bending moment; y is the
distance from the neutral line of the column (this is
the line that experiences neither compression nor
tension during bending); and I is the area moment of
inertia. The bending moment equals the product F×e,
where e is the eccentricity (distance from the line of
force to the center of the column). This distance is
crucial in provoking bending stress.
The relative movement of a vertebra with regard to
the vertebra immediately below it can be viewed as a
combination of rotation and translation. An infinite
number of combinations of rotation and translation
can describe the same movement. To simplify the
kinematics analysis is assuming that a vertebra
rotates around a pole whish (1) is located on the
inferior end plate of the moving vertebra and (2)
moves parallel to the inferior margin of the reference
vertebra, axis X of the coordinate system.
In framework of this model, the vertebral motion is
viewed as a translation along the axis X and the
rotation around the pole, the center of rotation
(Cossette, J. et al, 1971). Because a rotation about
the instantaneous center of rotation (ICR) is equal to
the rotation about any parallel axis, the angle
subtended at the ICR by the arc of motion of C is
equal to the angle of rotation (θ) undergone by the
whole vertebra. Because the triangle CC’R is an
isosceles triangle, HR = CC’/2tan(θ/2), where HR
and CC’ are the height and base of the triangle. If
the location of the ICR is experimentally
determined, location of C can be found as
'
2
CR IRC
CC
XX=−
(3)
()
'
2tan
2
CR IRC
CC
YY
θ
=−
(4)
The position of the ICR is determined by the
location of the center of the rotation, the translation
of the vertebra in parallel with the axis X and the
rotation of the vertebra. In some patients, as
compared with healthy people, the ICR is displaced.
The displacement can be explained in terms of the
three mentioned factors. For example, elevation of
the ICR can occur only when the translation is
decreased, the rotation is increased, or both. The
three mentioned mechanisms can be explained by a
combination of biomechanical changes, such as
increased muscle pull.
F
Disc
Stress diagra
m
Zero stress
A
B
C
A
B
C
e
G
G
Extension
Compression
y
-F
Figure 3: A model of intervertebral disk bending: the
stress distribution is in vertical cross section of a column
loaded by off-center forces, F and –F.
A WIRELESS ACQUISITION SYSTEM FOR MONITORING THE INFLUENCE OF LOADS ON VERTEBRAL
COLUMN BEHAVIOUR
235

Figure 4: An illustration of a vertebra that has rotate and
translated from an initial position to a final position about
an ICR located at R. The center of rotation C translates to
C’. H is the midpoint of interval CC’. θ is the angle of
rotation.
3 WIRELESS ACQUISITION
MODULE
The application described in this paper, needs
wireless acquisition modules (WAMs), to
simultaneously acquire the information from the
muscles and the movements of the patient. In the
first case, the use of standard electrodes makes
possible to measure the electrical potential, above
the patient’s tissue. In the second case, a dual-axis
accelerometer will measure the motion and the
positioning of the patient.
Normally, the barrier layer forms the typical 50 kΩ
impedance for 1 cm
2
of skin. There is also a skin
potential between the inside and outside of the
barrier layer of typically 30 mV. When the skin
stretches, the skin potential decreases to about
25 mV and this 5 mV change is what we observe as
motion artifact (Webster et al, 1984). These are the
signals that are being acquired by the electrodes, and
further amplified by the instrumentation and further
converted to the digital domain.
The Figure 5 shows the architecture of a WAM,
which is composed by an amplifier, followed by an
analog-to-digital converter (ADC) to convert the
amplified EMG signals to the digital domain, and a
dual-axis accelerometer.
The amplifier is a chain composed by the MAX4460
instrumentation amplifier, and by the MAX4249
single-ended low-noise amplifier. The MAX4460
was chosed due to its characteristics, e.g., the
low-power consumption, the ultra low-power input
current and the increased common-mode rejection
performance. This chip amplify the differential
signals obtained from the two potentials collected
with the EMG electrodes, placed in the patient’s
skin. The high input impedance of this amplifier
matches with the small-signal differential voltages
collected in the electrodes. The microcontroller
automatically selects the most appropriated gain of
this amplifier, which can be: one, ten and one
hundred. The MAX4249 makes the differential to
single ended conversion of the acquired EMG
signal, while makes a further amplification. This
amplifier was choosed due its low-noise
characteristics, to not contaminate the EMG signal.
2-axis
accelerometer
16F628
uController
ADC
A
RF
transceiver
GND
Electrodes
To the
antenna
Figure 5: The block diagram of the wireless acquisition
module.
The analysis of the EMG signal is made in the
amplitude domain, thus, before proceeding to the
ADC conversion, it is required a peak detection of
the amplified EMG signal, followed by an
integration (Robertson et al, 2004). This is
mandatory process eliminates the fluctuations that
characterise the EMG signal. As shown in Figure 6,
the discharge of the capacitor, is made with a bipolar
junction transistor (BJT). The pulse transformer is
made in the WAM’s PCB, in order to not
compromise the compactness of the WAM. The
circuit size WAM achieved, using surface mount
(SMDs) devices, for all the components, including
the micropower, rail-to-rail output, dual op-amp
MAX4471, used in the circuit of the integrator.
The measurements of the motion and the positioning
of the patient’s body is made with the use of the
ADIS16003, dual-axis accelerometer of MEMS
type. This chip connects to the microcontroller, by
way of an integrated Serial Port Interface (SPI). This
accelerometer was choosed, due its build-in
temperature sensor. This sensor is very useful to
make the compensation of the temperature gradients,
specially when the devices are placed in contact with
the human body.
θ
/2
θ
H
C
C’
(X
CR
, Y
CR
)
R
(X
ICR
, Y
ICR
)
X
Y
θ
BIODEVICES 2008 - International Conference on Biomedical Electronics and Devices
236
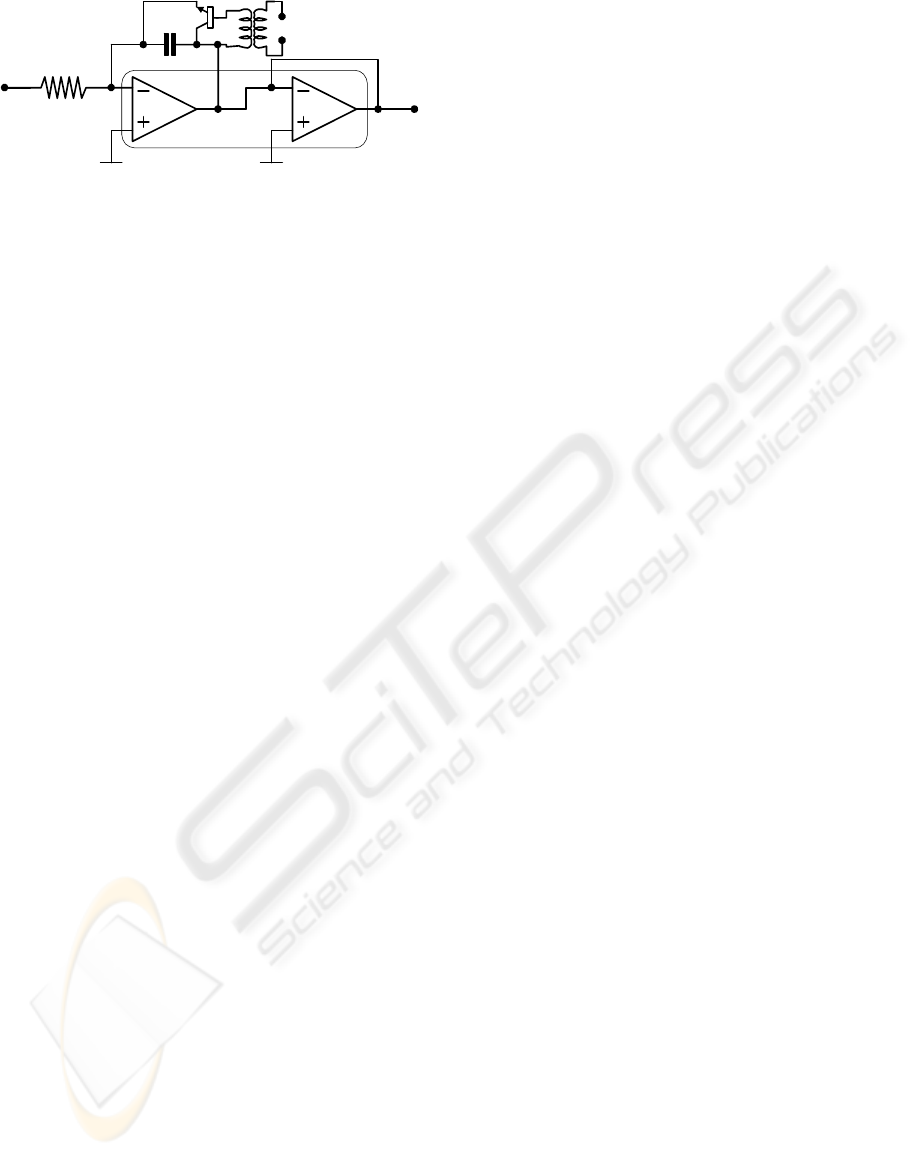
Figure 6: Integration circuit.
The microcontroller PIC16F628 from the Microchip
manufacturer, controls all the electronics, as well as
the communication between WAMs, and from the
WAM and the external base-station, where all the
processing of the acquired data is made by a health
professional, or a medical doctor. It was selected the
BiM433 radio-frequency (RF) transceiver, from the
Radiometrix manufacturer to wirelessly send the
data. A set of routines and services were developed
to make the RF communication the most reliable as
possible. The most important of these routines are
the Manchester line coding, used to solve de DC
balancing problem in the communication, when long
sequences of zeros or ones must be transmitted. It
was included a mechanism of error control in all
data frames (information, control and acknowledge
frames), e.g., the CRC field. This field makes the
detection of transmission errors in the received
bitstream (Schmidt, 2000). To make the
multi-element communication possible and reliable,
the WAMs use the Carrier Sense Multiple Access
with Collision Avoidance protocol (CSMA-CA) to
start the transmissions (Chandra et al, 2000). This
simplifies the management procedures of the
communication among modules, and between the
base-station. This makes easy to place (or remove)
new WAMs in the clothes of patients, in a
plug-and-play fashion.
4 CONCLUSIONS
It was described in this paper, a wireless acquisition
module, which will be used on the diagnosis of
vertebral column risk factors, such as the scoliosis
and lordosis. These factors normally associated to
appears in children when they carry the heavy
backpacks on the backs. Thus, it’s of extremely
importance to characterise the influence of heavy
loads (backpack weight) in the vertebral column
behaviour. This solution fits the medical doctors
requirements for an easy placement and removal of
the WAMs. This is true for the target application,
because it is needed only with a low number of
WAMs (no more than five), making possible to
mount a wireless network with these plug-and-play
modules. The main advantage of this solution, is the
maintenance of the mobility and lifestyle of patients
during the diagnosis.
A set of two alkaline 1.5-V class AA bateries
supplies the wireless acquisition module. When the
RF subsystem is on, these modules have a power
consumption of 46 mW. With the RF subsystem off,
these modules have a consumption of only 10 mW.
REFERENCES
Adams, M., Dolan, P., 1991, A technique for quantifying
bending moment acting on lumbar spine in-vivo,
Journal of Biomechanics, Vol. 24, pp. 117-126.
Adams, M., Dolan, P., Hutton, W., 1988, The lumbar
spine in backward bending, Spine, Vol. 13,
pp. 1019-1026.
Choi, P., et al, 2003, An experimental coin-sized radio for
extremely low-power WPAN (IEEE 802.15.4)
application at 2.4 GHz, IEEE Journal of Solid State
Circuits, Vol. 38, No. 12, pp. 2258-2268.
Conceição, F. et al, 2007, Modelação do actuador
músculo-tendão: os elementos elásticos em série como
slemento central de potenciação de força, Proceedings
of CMNE/CILAMCE, In Portuguese.
Cossette, J. et al, 1971, The instantaneous center of
rotation of the third lumbar intervertebral joint, Journal
of Biomechanics, Vol. 4, pp. 149-153.
Bridwell, K., 2007, http://www.spineuniverse.com/
displayarticle.php/article1286.html.
Kaggs D., et al, 2006, Back pain and backpacks in school
children, Journal of Pediatric Orthopedy, Vol. 26,
Nr. 3, pp. 358-363.
Nissinen M, et al, 194, Anthropometric measurements and
the incidence of low back pain in a cohort of pubertal
children, Spine, Vol. 19, Nr. 12, pp. 1367-1370.
Pato, M., Martins, J., Pires, E., 2007, Um modelo de
elementos finitos para músculos esqueléticos,
proceedings of CMNE/CILAMCE, In Portuguese.
Robertson, D., et al, 2004, Research methods in
biomechanics, Human Kinetics.
Schmidt, T., 2000, Microchip Technology Inc., CRC
generation and checking, Application note AN730.
Webster, J. et al, 1984, Reducing motion artifacts and
interference in biopotential recording, IEEE
Transactions on Biomedical Engineering, Vol. 31,
No. 12, pp. 823-826..
Widhe T., 2001, Spine: posture, mobility and
pain - A longitudinal study from childhood to
adolescence, European Journal of Spine,
Vol. 10, Nr. 2, pp. 118-123.
Palastanga, N., et al, 2002, Anatomy and human
movement, Fourth Edition, Edited by Butterworth
Heinemann, pp. 445-537.
Zatsiorsky, V., 1998, Kinematics of human motion, Edited
by Human Kinetics, pp. 311-326.
discharge
MAX4471
R
C
A WIRELESS ACQUISITION SYSTEM FOR MONITORING THE INFLUENCE OF LOADS ON VERTEBRAL
COLUMN BEHAVIOUR
237
