
NEWBORN HEARING SCREENER BASED ON AUTOMATIC
AUDITORY BRAINSTEM RESPONSE DETECTION
Julio Aldonate, Carlos Mercuri, José Biurrun, Juan Manuel Reta, Claudia Bonell
Gerardo G. Gentiletti, Sergio Escobar and Rubén Acevedo
Laboratorio de Ingeniería de Rehabilitación e Investigaciones Neurológicas y Sensoriales, Facultad de Ingeniería
Universidad Nacional de Entre Ríos, Ruta 11 - Km10, Oro Verde, Entre Ríos, Argentina
Keywords: Auditory brainstem response, hearing loss, automatic detection, newborn hearing screening.
Abstract: Hearing loss is one of the pathologies with the highest prevalence in newborns. If it is not detected in time,
it can affect the nervous system and cause problems in speech, language and cognitive development. The
recommended methods for early detection are based on otoacoustic emissions (OAE) and/or auditory
brainstem response (ABR). In this work, the design and implementation of an automated system based on
ABR to detect hearing loss in newborns is presented. Preliminary evaluation in adults was satisfactory.
1 INTRODUCTION
According to the Health World Organization, 5 per
1,000 neonates are born with significant hearing
loss. This pathology has a negative incidence on the
nervous system, causing a delay in the development
of speech and language, and consequently affecting
cognitive and behavioral skills (Priesler, 1999;
Jacobson, 1985).
Early detection of hearing impairment is
therefore essential, in order to allow a more
successful intervention and rehabilitation.
Recommended practice begins with universal
newborn hearing screening (UNHS) using objective
physiological methods, preferably either before
being discharged from the hospital or no later than
at 2 or 3 months of age (Gracey, 2003).
All over the world, strategies used in UNHS are
based on otoacoustic emissions (OAE) and auditory
brainstem response (ABR). Particularly, methods
based on ABR are well-considered due to their high
specificity and sensitivity rates and their high
correlation between impairment and alteration in the
ABR pattern (American Academy of Pediatric,
1999; European Consensus Statement on Neonatal
Hearing Screening, 1998).
However, traditional analysis is complex and
time consuming, limiting its use to selective
screening of a small percentage of newborns. With
the development of Automatic ABR (AABR)
analysis, results are obtained faster, facilitating its
application on a larger population (Suppiej &
Rizzardi, 2007).
In this context, the Facultad de Ingeniería de la
Universidad Nacional de Entre Ríos (Argentina), in
cooperation with the Hospital Materno Infantil San
Roque (HMISR), Paraná, Argentina, and the Centro
de Especialidades Médicas Ambulatorias (CEMA),
Rosario, Argentina, have begun a technological
development project, aiming at designing and
building a universal hearing screening system based
on AABR. This work presents the design and
preliminary results obtained with an implemented
prototype, named AudioScreen.
2 SYSTEM REQUIREMENTS
A universal hearing screener based on AABR should
be able to evoke, record, store and process
electroencephalographic (EEG) signals coming out
from the brain (McAllister & McCullagh, 2000).
Therefore, suitable hardware and/or software for
these purposes must be able to perform the
following tasks:
Stimulate the auditory system according with
specific parameters (Mercuri et al., 2006).
Record the EEG signals from the scalp,
synchronizing the acquisition with the
stimulation (Acevedo et al., 2006).
174
Aldonate J., Mercuri C., Biurrun J., Manuel Reta J., Bonell C., G. Gentiletti G., Escobar S. and Acevedo R. (2008).
NEWBORN HEARING SCREENER BASED ON AUTOMATIC AUDITORY BRAINSTEM RESPONSE DETECTION.
In Proceedings of the First International Conference on Biomedical Electronics and Devices, pages 174-177
DOI: 10.5220/0001052401740177
Copyright
c
SciTePress
Perform a digital processing on the EEG
signals, in order to detect whether the ABR is
present or not (Acevedo et al. 2006).
The system has to be flexible enough to allow a
range of stimulation and recording options. Tables 1
and 2 summarize specific requirements for this
system.
Table 1: Stimulation parameters.
Parameter Description
Stimulus type Condensation click
Stimulus width 100 µs
Stimulus intensity
20 to 70 dB peSPL in 10 dB
steps
Stimulation frequency 11 and 31 clicks/s
Audio output Mono
Masking None
Table 2: Recording parameters.
Parameter Description
Gains 500 a 100.000 in 10 steps
Bandwidth 100 Hz – 2500 Hz
Input impedance
> 10
6
Ω
CMRR > 80 dB
Isolation > 3.000 V
RMS
Sampling frequency 200 Hz to 20 kHz
Sampling period Up to 15 ms
Resolution > 10 bits
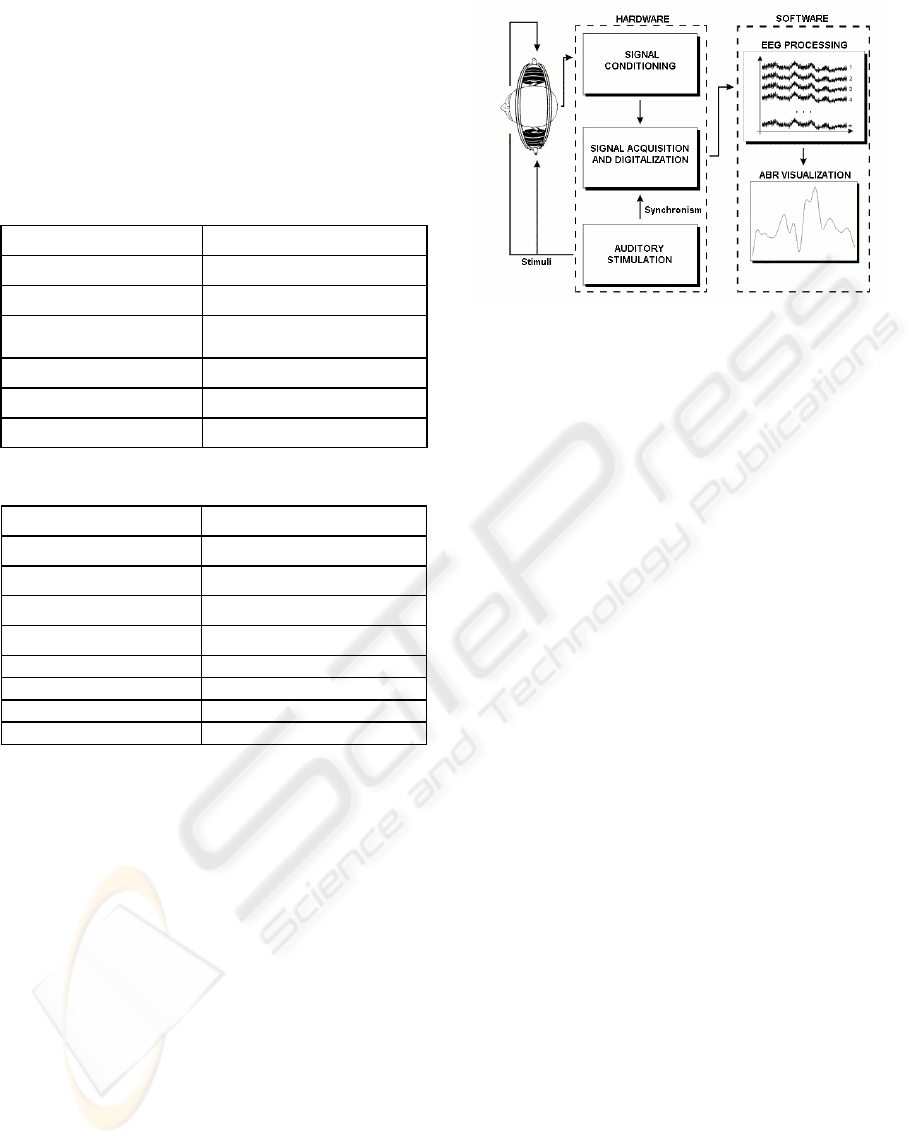
3 SYSTEM DESIGN
The design of the hearing screener is based on four
modules: auditory stimulation (AS), signal
conditioning (SC), signal acquisition and
digitalization (SAD) and signal processing and
visualization (SPV). Figure 1 shows a block diagram
of these modules.
As this is the first research prototype, it is
planned to be used both in research and clinical
environments. The former requires this system to be
flexible at the digital processing stage, in order to
allow testing and evaluation of different algorithms
for automatic ABR detection. For this reason, the
SPV module is implemented in software, and a
personal computer is required in order to use the
screener. Future versions of AudioScreen will
implement this module in specific hardware, making
the system independent from the computer.
Figure 1: Block diagram of the AudioScreen hearing
screener modules.
A brief description of the system operation would be
as follows: initially, the computer sends a number of
configuration parameters for the AS and the SAD
modules. When a start signal is received, the
stimulator generates acoustic stimuli, which are
applied to the patient through headphones. At the
same time, a synchronism signal is generated and
sent to the SAD module to establish the beginning of
the EEG recording which is amplified and filtered in
the SC module. Finally, the EEG is digitalized and
transmitted to the computer via USB 1.0, where the
SPV module stores it for further processing and
visualization.
4 SYSTEM IMPLEMENTATION
4.1 Auditory Stimulation Module (AS)
The auditory stimulator produces digital clicks
(electrical stimuli) whose amplitude is set by a gain-
controlled amplifier (PGA2310 Texas Instruments
Inc). Then, the clicks are transduced to auditory
stimuli by headphones (Telephonics
®
TDH39). Two
stimulation parameters can be set: intensity, ranging
from 20 to 70 dB peSPL in 10 dB steps, and
frequency in two possible values, 11 or 33 clicks/s.
The selected values are indicated by LEDs on the
front panel. In this way, different configurations may
be used for auditory stimulation.
The electronic circuit is implemented with an 8-
bit RISC microcontroller. The microcontroller
configures the gain-controlled amplifier through a
serial port interface and it is linked up with the SAD
module using two ports: one is used to generate the
synchronism signal and the other is used to receive a
start signal to begin the stimulation.
NEWBORN HEARING SCREENER BASED ON AUTOMATIC AUDITORY BRAINSTEM RESPONSE DETECTION
175

4.2 Signal Conditioning Module (SC)
Appropriate integrated circuits (IC) for medical
instrumentation are used. This module consists of
four parts:
Instrumentation amplifier: INA128 (Burr-
Brown Corp.). This IC has high input
impedance (10
10
Ω) and common-mode
rejection (120dB at G ≥ 100), very low offset
voltage (50µV) and drift (0.5µV/°C).
Programmable gain amplifier: OP07 (Analog
Devices Inc.). Gain can be set in the range of
500 and 100000 in 10 steps.
Isolating amplifier: ISO121 (Burr-Brown
Corp.). This IC has unitary gain and it is based
on a 2 pF differential capacitive barrier, which
results in a 3500 V
RMS
isolation.
Filter: a band pass filter is implemented using
a cascade design of Sallen-Key cells with
cutoff frequencies in 2500 Hz for low pass
and 100 Hz for high pass. In order to reduce
the electromagnetic induction produced by the
power line, a Sallen-Key notch filter centered
in 50 Hz is implemented. This notch filter can
be enabled or disabled using onboard jumpers.
4.3 Signal Acquisition and
Digitalization Module (SAD)
This module is based on another 8-bit RISC
microcontroller which controls the AD module as
well as the communication with the computer. The
AD module includes a 12-bits, bipolar input range,
analogical to digital converter and a low-noise,
temperature-stabilized, precision reference. The
sampling frequency can be set to a maximum of 20
kHz and the acquisition window is set to 15 ms.
4.4 Power Supply
The power supply has two stages: one of them is not
isolated and the other is isolated according to the
IEC 60610 standard. Isolation is achieved using
PWR1303A (C&D Technologies Inc.). Table 3
summarizes its specifications.
Table 3: Power supply specifications.
Parameter Description
Isolated stage ± 5 V, 150 mA, 4 kV DC
Non-isolated stage ± 5 V, ± 12 V, 1 A
Hardware-implemented modules are shown in
Figure 2.
Figure 2: Inside view of the screener; (a) SAD module
board, (b) SC module board, (c) power supply board, and
(d) AS module board.
4.5 Signal Processing and Visualization
Module (SPV)
SPV module block diagram is shown in Figure 3.
This module was programmed using Borland
®
C++
Builder
®
, and the database was generated with
Microsoft
®
Access
®
2003. The user interface was
designed taking into account pieces of advice from
several professionals of the health centers mentioned
above.
EEG ACQUISITION EEG PROCESSING
DATABASE
ABR
VISUALITATION
REPORT
GENERATION
Figure 3: Block diagram of the SPV module.
The database stores all the information about the
screening, which basically consists of newborn’s and
mother’s personal information, along with the
signals recorded with the EEG acquisition block and
the parameters used in the study, e.g. stimulation
frequency and intensity.
The EEG processing block performs two main
tasks: signal averaging to enhance signal-to-noise
ratio, and automatic ABR detection using the FSP
algorithm (Gentiletti et al., 2003). The results of the
study are visualized in the computer monitor (Figure
BIODEVICES 2008 - International Conference on Biomedical Electronics and Devices
176

4), and can be printed along with a full report of the
study.
Figure 4: ABR visualization window.
5 EXPERIMENTS AND RESULTS
Figure 5 shows the complete system, which
complies with the IEC 60610 standard for medical
equipment.
Figure 5: AudioScreen system with the software running
on the computer; (a) screener; (b) software interface; (c)
electrode cable; (d) power supply.
The user interface was assessed by HMISR and
CEMA personnel, and the resulting evaluation was
satisfactory. Finally, a full set of tests were carried
out with healthy patients, which verified the correct
performance of the system.
6 CONCLUSIONS
A first prototype of the AudioScreen system was
designed, built and it’s has been tested. It was done
using adequate off the shelf electronic components,
which met the standard for medical equipment and
were fully operational. The following step is to
perform system validation at the HMISR as well as
the CEMA. In addition, an algorithm of ABR signal
detection based on support vector machines is being
developed, which will be validated and contrasted
against the Fsp method.
ACKNOWLEDGEMENTS
This work was supported by the Secretary of
Science, Technology and Productive Innovation
(SeCTIP) and by the Council of Investigations of the
National University of Entre Ríos (CIUNER).
REFERENCES
Priesler G., 1999. The Development of Communication
and Language in Deaf and Severely Hard of Hearing
Children: Implications For The Future. Int J Pediatr
Otorhinolaryngol; 49(Suppl 1):S39-43.
T. Jacobson. 1985. The Auditory Brainstem Response,
Boston, Editorial Collage-Hill Press.
Gracey K. 2003.Current Concepts in Universal Newborn
Hearing Screening and Early Hearing Detection And
Intervention Programs. Advances in Neonatal Care,
Vol. 3, No. 6 (December): pp 308-317
American Academy of Pediatric, 1999. Newborn and
Infant Hearing Loss: Detection and Intervention.
Pediatrics; 103: 527-30.
European Consensus Statement on Neonatal Hearing
Screening. Milan. May 1998.
Suppiej A, Rizzardi E, Zanardo V, Franzoi M, Ermani M,
Orzan E, 2007. Reliability of Hearing Screening in
High-Risk Neonates: Comparative study of automated
OEA, and conventional ABR. Clin Neurophysiol. 2007
Apr; 118(4):869-76. Epub Feb 20.
McAllister H. and McCullagh P, 2000. Objective methods
of hearing assessment. Computing and Control
Enginnerging Journal. April, 53-64
Mercuri C., Escobar S., Cadirola F., Astiasaran P.,
Gerardo G., Aldonate J., Bonell C., Acevedo R., 2006.
Estimulador auditivo para audiometría tonal y
potenciales evocados auditivos, Revista Argentina de
Bioingeniería, vol 12, nro 2, pp. 13-19.
Acevedo R., Bonell C., Gentiletti G., Aldonate J., Mercuri
C., Escobar S., Biurrun J., 2006. Potenciales
Evocados Auditivos De Tronco Cerebral: Aspectos
tecnológicos del Registro, Revista Argentina de
Bioingeniería, vol. 12 No. 1, pp. 10-17.
Gentiletti G., Yañez O., Cornejo J, 2003. Evaluation of
Automatic Identification Algorithms for Auditory
Brainstem Response used in Universal Hearing Loss
Screening. Proceedings of 25 th Annual International
Conference of the IEEE EMBS.
a
b
c
d
NEWBORN HEARING SCREENER BASED ON AUTOMATIC AUDITORY BRAINSTEM RESPONSE DETECTION
177
