
PRINCIPAL COMPONENT ANALYSIS OF THE P-WAVE
Quantification of Not-Dipolar Components of Atrial Depolarization
Federica Censi, Giovanni Calcagnini, Pietro Bartolini
Department of Technologies and Health, Istituto Superiore di Sanità, Roma, Italy
Chiara Ricci
Department of Statistics, Probability and Applied Statistics, Univ. of Rome "La Sapienza", Rome, Italy
Renato Pietro Ricci, Massimo Santini
Department of Cardiology, San Filippo Neri Hospital, Roma, Italy
Keywords: Principal component analysis, atrial fibrillation, P-wave, not dipolar components.
Abstract: Aim of this study is to perform the principal component analysis (PCA) of the P-wave in patients prone to
atrial fibrillation (AF). Eighteen patients affected by paroxysmal AF and implanted with dual chamber
pacemakers were studied. Two 5-minute ECG recordings were performed: during spontaneous (SR) and
paced rhythm (PR). ECG signals were acquired using a 32-lead mapping system (2048 Hz, 24 bit, 0-400 Hz
bandwidth). For each patient, PCA of the averaged P-waves extracted in any of the 32 leads has been
performed. We extracted PCA parameters related to the dipolar (using the first 3 PCs) and not dipolar (from
the 4
th
to the 32
nd
PCs) components of the P-wave. The number of PCs according to the latent root criterion
ranges between 2 and 3 during SR and between 2 and 4 during PR. PCA parameters related to the 3 largest
PCs, and describing the dipolar component of the P-wave, did not significantly differ during SR and PR.
The not dipolar components during SR were significantly lower than during PR (PCAres%: 0.03±0.06 vs
0.12±0.21, p=0.001; PCAres [mV
4
]: 0.10±0.14 vs 0.49±0.73, p=0.001). Factor analysis showed that on
average all leads contributes to the first principal component
.
1 INTRODUCTION
Atrial fibrillation (AF) is the most commonly
encountered arrhythmia in clinical practice. It is
defined by the absence of coordinated atrial systole,
since it results from multiple reentrant electrical
wavelets that move randomly around the atria.
Althought it is not a lethal disease, AF may increase
mortality up to 2-fold, primarily due to embolic
stroke.
Indeed, the lack of coordinated atrial contraction
leads to unusual fluid flow states through the atrium
that could favour the formation of thrombus at risk
to embolize, expecially after return to normal sinus
rhythm.
The incidence of atrial fibrillation increases
significantly with advancing age. When a patient
spontaneously alternates between AF and a normal
rhythm, the condition is known as paroxysmal AF.
When a patient continues with AF as the dominant
cardiac rhythm without reversion to the normal
rhythm, the condition is known as chronic AF. Two
main electrophysiological conditions are indicated
for AF initiation and perpetuation (Clavier et al.,
2002): slower conduction velocity in some atrial
areas and heterogeneity of cell refractory periods.
This heterogeneity of structural and
electrophysiologcal properties leads to a longer and
more fragmented P-wave (Davies et al., 1963;
Kawano et al., 1988; Dilaveris et al., 1998).
Thus, many studies focused on the analysis of
the P-wave to extract parameters to recognize a
patient with paroxymal AF as well as to predict the
development of AF (Dilaveris et al., 1998; Jordaens
et al., 1998; Dilaveris et al., 2001; Darbar et al.,
2002; Dilaveris et al., 2002).
Given the technical difficulties to analyze the P-
wave, and the different acquisition and processing
551
Censi F., Calcagnini G., Bartolini P., Ricci C., Pietro Ricci R. and Santini M. (2008).
PRINCIPAL COMPONENT ANALYSIS OF THE P-WAVE - Quantification of Not-Dipolar Components of Atrial Depolarization.
In Proceedings of the First International Conference on Bio-inspired Systems and Signal Processing, pages 551-557
DOI: 10.5220/0001060005510557
Copyright
c
SciTePress

Figure 1: Scheme of the electrodes positioning and of the P-wave pre-processing procedure.
systems used, these studies often lead diverse
and not-comparable results in terms of cutoff values.
Indeed, the analysis of the T-wave, corresponding to
the ventricular repolarization, has been extensively
used to quantify repolarization inhomogeneity that
may create an arrhythmogenic ventricular substrate.
Promising results have been obtained by measuring
the QT interval (QT dispersion) and by performing
the principal component analysis of the T-wave (De
Ambroggi et al., 1997; Acar et al, 1999; Malik et al.,
2000; Kesek et al., 2004).
The former analysis have been already applied to
the P-wave: P-wave dispersion (which is the
difference between the maximum and the minimum
P-wave duration recorded from the 12 standard
leads), has been shown to distinguish patients with
paroxymal AF (Dilaveris et al., 1998; Jordaens et al.,
1998; Dilaveris et al., 2001; Darbar et al., 2002;
Dilaveris et al., 2002).
PCA of the T-wave has been extensively used to
quantify both the complexity and the not dipolar
components of the T-wave (De Ambroggi et al.,
1997; Acar et al, 1999; Malik et al., 2000; Kesek et
al., 2004): particularly, if the ECG would be
completely explained by a single electrical dipole,
the three largest principal components (PCs), and
their corresponding orthogonal eigenvectors, would
span the real three dimensional space (dipolar
components), while the remaining PCs (not dipolar
components) would be zero (Kesek et al., 2004).
For the T-wave it has been demonstrated that the
not dipolar components, quantified by the PCA, are
not zero, and reflect local repolarization
inhomogeneity (Kesek et al., 2004). PCA has never
been applied to the P-wave.
Following the approach already used for the
analysis of the T-wave, the aim of this study is to
perform the PCA of the P-wave in patients prone to
AF in order to: 1) evaluate how many principal
components are necessary for an AF patient and in
which way they are correlated with the ECG leads;
2) evaluate if and to which extent pacing affects the
dipolar and the not dipolar components of the atrial
depolarization (as quantified by PCA).
2 METHODS AND MATERIALS
2.1 Study Population
Nineteen patients with paroxysmal atrial fibrillation
and permanent dual chamber pacemakers (AT500-
Medtronic Inc., Minneapolis, MN, USA) were
recruited from S. Filippo Neri Hospital, Rome, Italy.
The AT500 device combines atrial sensing and
detection algorithms for monitoring and diagnostics,
and atrial therapy delivery functions.
The system can store up to 35 episodes of atrial
tachycardia/ flutter with electrograms and up to 128
episodes text summaries, without electrograms.
This pacemaker allows for accurate classification
of atrial fibrillation episodes, with detailed
information about episode instant of occurrence and
duration, and further features three distinct
programmable pacing algorithms that suppress atrial
tachyarrhythmia trigger mechanisms.
When an episode occurs, the device is also
programmed for arrhythmia termination. Three atrial
pace-termination algorithms can recognise treatable
atrial tachycardias and deliver antitachycardia pace-
therapies to restore sinus rhythm.
The study population consisted of 9 female and 10
men, aged 72±10.
P-wave
averaging
P-wave
template
P-wave
extraction
BIOSIGNALS 2008 - International Conference on Bio-inspired Systems and Signal Processing
552

2.2 Experimental Protocols
Two five-minute recordings were performed for
each subject. In the first recording the pacemaker
was programmed in VVI mode, i.e. in single-
chamber ventricular pacing mode set to a rate of
40/min, so that to have spontaneous rhythm.
In the second recording, pacemaker settings were
changed back to the common operating DDD mode,
i.e. with both atrial and ventricular pacing functions
activated.
Recordings were made using a multi-lead
mapping system for high-resolution biopotential
measurement (ActiveTwo, Biosemi, The
Netherlands).
The system is made of a battery powered isolated
AD box that digitises the signals and transfers them
to a PCI receiver on computer through a fibre-optic
connection. The signals were digitised at a sampling
rate of 2048 Hz and a resolution of 24 bits with a
frequency response in the full DC-400Hz range.
No further filtering was applied to the data.
Thirty-two leads were positioned on the thorax
(figure 1), to allow accurate recordings of atrial
signals.
ECG recordings were acquired as single-ended
signals, with respect to a common reference
position. Before starting the acquisition, signals
were visualised on a computer screen to check for
good electrode contact.
2.3 P-wave Pre-processing
Every lead signal was pre-processed and analysed to
extract the average P-wave characteristic.
The first step is to isolate the P-waves from the
acquired signals: after detecting the R-wave (using
an algorithm similar to that proposed by Pan and
Tompkins) (Pan and Tompkins, 1985), P-waves are
extracted in a 200ms-long window (410 samples)
starting 300ms before the R-wave (figure 1).
Secondly, a beat-by-beat linear piecewise
interpolation was used to remove baseline wander,
on each P-wave. Fiducial points for linear
interpolation were taken from TP and PQ tracks of
each beat.
Third, a P-wave template is constructed (figure
1) by averaging each extracted P-wave having a
cross-correlation coefficient with the current
template higher than 0.9.
In order to take into account the variations in PR
interval and/or the inaccuracy in R-wave detection
before averaging P-waves were aligned according to
the lag at which the cross-correlation function
between the current averaged P-wave and each
single P-wave shows its maximum (coherent
averaging procedure).
The coherent averaging procedure went on until
200 beats were included. If the residual noise level
(measured in the isoelectric TP track) remained at
more than 1μV even after averaging of 200 beats,
averaging procedure continued until the noise level
reached a value lower than 1μV.
If it was impossible, the lead was excluded from the
study.
2.4 Principal Component
Analysis – Measures of Atrial
Depolarizatrion
Characteristics
For each patient, PCA of the 32 averaged P-waves
extracted from the 32 leads has been performed.
Since PCA transforms the measured P-wave to
virtual parameters that are mutually independent
(orthogonal), the 3 largest PCs would contain all the
information in the P-wave stemming from the
vectorial concept of a single electrical dipole.
Following an approach already applied to the T-
wave (Kesek et al., 2004; Acar et al, 1999), the other
principal components (in this case from the 4
th
to the
32
nd
) represent the not dipolar components of the
atrial depolarization.
We thus extracted the following parameters:
where s
i
denotes the i-th eingenvalue associated with
the i-th principal component. We also extracted the
number of principal components suggested by the
latent root criterion (PCA number).
In addition, in order to estimate to which extent
each lead contributes to the first principal
component, factor loadings have been calculated.
Analogous to Pearson's coefficient, the squared
PRINCIPAL COMPONENT ANALYSIS OF THE P-WAVE - Quantification of Not-Dipolar Components of Atrial
Depolarization
553

Table 1: Results of the PCA parameters during spontaneous rhythm (SR) and during paced rhythm (PR) for all 18 patients.
Figure 2: Example of the 32 P-wave templates and of the results of the PCA for one patient.
[mV
4
] [%]
[%] [%]
[%]
BIOSIGNALS 2008 - International Conference on Bio-inspired Systems and Signal Processing
554
factor loading is the percent of variance in that
variable explained by that PC (i.e the degree of
correlation between the original data and the first
principal component expressed in percentage).
In addition, in order to estimate to which extent
each lead contributes to the first principal
component, factor loadings have been calculated.
Analogous to Pearson's coefficient, the squared
factor loading is the percent of variance in that
variable explained by that PC (i.e the degree of
correlation between the original data and the first
principal component expressed in percentage).
3 RESULTS
Figure 2 shows the 32 P-wave templates and the
results of the PCA for one patient.
Table 1 summarizes the results obtained by the
PCA parameters. The number of principal
components according to the latent root criterion
ranges between 2 and 3 (2,56±0,51) during
spontaneous rhythm and between 2 and 4 during
pacing (2,67±0,69, p=0,6).
PCA parameters related to the three largest PC
(PCA
1
[%], PCA
2
[%] and PCA
3
[%]), that describe
the dipolar component of the P-wave, did not
significantly differ during spontaneous and paced
rhythm (table 1, Wilcoxon test for paired data). The
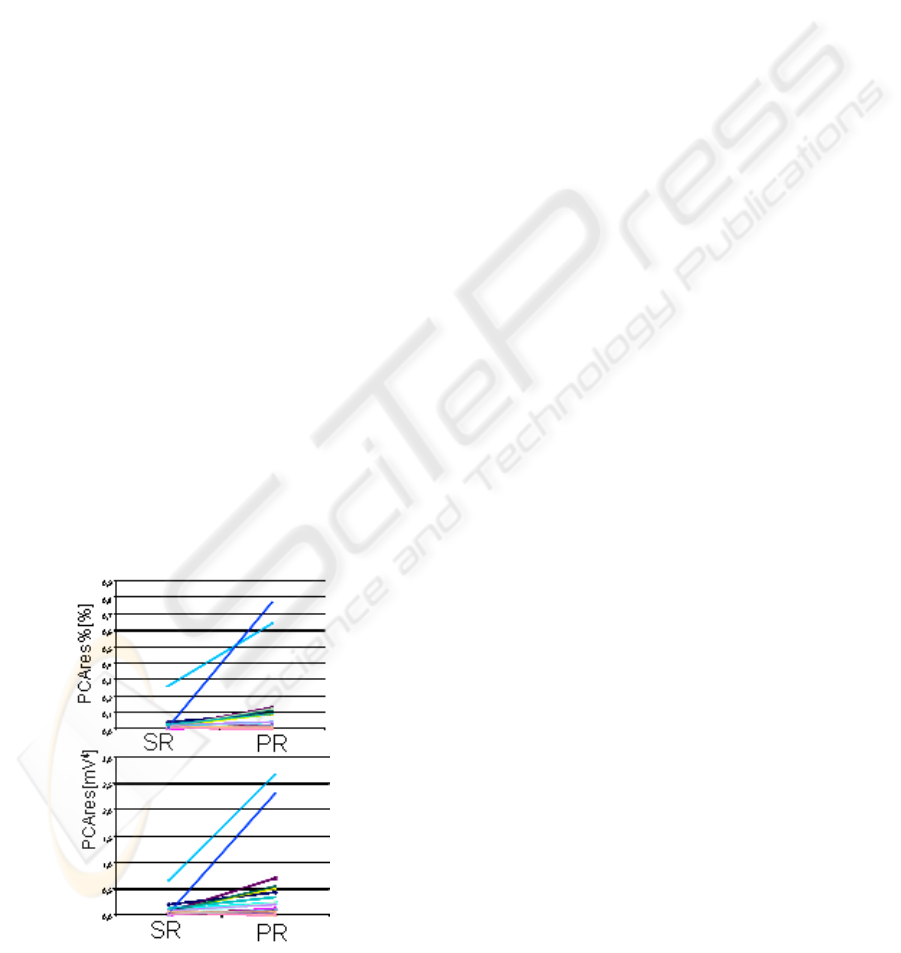
not dipolar component (figure 3) as defined by both
PCAres and PCAres% during spontaneous rhythm
were significantly lower than during pacing
(PCAres%: 0,03±0,06 vs 0,12±0,21, p=0,001;
PCAres[mV
4
]: 0,10±0,14 vs 0,49±0,73, p=0,001).
Figure 3: Notdipolar components as defined by both
PCAres and PCAres% during spontaneous rhythm and
during pacing.
Factor analysis showed that on average all leads
contributes to the first principal components. Figure
4 shows the factor loadings averaged (in absolute
values) all over the population during spontaneous
rhythm and during pacing. Each lead but one in
spontaneous rhythm (lead A17) correlates with the
first principal component.
4 DISCUSSION
Analysis of the P-wave had been extensively
developed to extract parameters related to atrial
depolarization heterogeneities useful to recognize
patients with paroxymal AF or to predict the
development and the perpetuation of AF (Dilaveris
et al., 1998; Jordaens et al., 1998; Dilaveris et al.,
2001; darbar et al., 2002; Dilaveris et al., 2002).
However, the technical difficulties to acquire and
process the P-wave, had so far limited its clinical
use. Indeed, promising results have been obtained by
performing the PCA of the T-wave, in terms of
quantification of ventricular repolarization
inhomogeneity that may create an arrhythmogenic
ventricular substrate (De Ambroggi et al., 1997;
Acar et al, 1999; Malik et al., 2000; Kesek et al.,
2004).
We hereby used an 32-lead ECG acquisition
system particularly suitable for P-wave analysis,
having 24 bit resolution and being DC-coupled. We
performed the PCA of the P-wave in patients prone
to AF. PCA has been applied to the average P-wave
extracted in any of the 32 leads.
For each patient we extracted the same PCA
parameters employed for the T-wave (Kesek et al.,
2004; Acar et al, 1999). As for the T-wave, the PCA
parameters related to the first three PCs are
associated to the dipolar component of the P-wave,
while the remaining PCs (form the 4
th
to the 32
nd
)
are associated with the not dipolar component of the
P-wave.
To our knowledge this is the first time the PCA
is performed on the P-wave, thus physiological
interpretation and critical discussion can be related
only to previous experimental evidences of
ventricular conduction disturbance (PCA of the T-
wave ) (Kesek et al., 2004; Acar et al, 1999).
The first important result is that pacing provokes
a significant increase of the not dipolar components
of the P-wave. Thus atrial pacing changes the atrial
activation, disturbing the normal atrial
depolarization process and generating additional
paths not explainable by a single P-vector. Such a
PRINCIPAL COMPONENT ANALYSIS OF THE P-WAVE - Quantification of Not-Dipolar Components of Atrial
Depolarization
555

Figure 4: Factor loadings obtained during spontaneous rhythm and during pacing.
result is in agreement with previous studies showing
an increase in P-wave duration and low-frequency
energy during pacing respect to sinus rhythm in
patients with AF (Keane et al., 1995). Non-dipolar
components is plausible to be associated with local
atrial depolarization inhomogeneity: pacing seems to
provoke parts of the myocardium depolarized in a
normal sequence and parts depolarized from an
abnormal direction.
The second important results is that, on average,
all the 32 leads contributes to the first PC, having a
significant correlation coefficient with almost all
variables.
Since any leads systematically show a not
significant correlation with first PC, each lead seems
to contribute to a similar extent to the dipolar
component. However, we found an inter-patient
variability for the factor loadings – some patients
had not significant factor loadings in some leads.
This result suggests that maps of the correlation with
the first PC (or of the average correlation with the
first 3 PCs) could help in identifying those leads (i.e.
body surface zones) which mainly contribute to the
dipolar component of the atrial depolarization.
In conclusion, the study of the dipolar and not
dipolar components of the P-wave could provide
important information not present in a classical
ECG. If the assumption that the not dipolar signal is
associated with local depolarization inhomogeneity
of the atrium is correct, the PCA is a useful
mathematic tool to deeply investigate the atrial
conduction disturbances as well as the effects of
pharmacological or electrical therapies. This first
study tempting the PCA on the P-wave shows that
pacing alters the atrial depolarization patterns,
provoking an increase of the not dipolar component
of the P-wave.
REFERENCES
Acar B, Yi G, Hnatkova K, Malik M. Spatial, temporal
and wavefront direction characteristics of 12-lead T-
wave morphology. Med Biol Eng Comput. 1999
Sep;37(5):574-84.
Clavier L, Boucher JM, Lepage R, Blanc JJ, Cornily JC.
Automatic P-wave analysis of patients prone to atrial
fibrillation. Med Biol Eng Comput. 2002
Jan;40(1):63-71.
Darbar D, Jahangir A, Hammill SC, Gersh BJ. P-wave
signal-averaged electrocardiography to identify the
risk for atrial fibrillation. Pace 2002; 25:1447-1453.
0, 00
0, 20
0, 40
0, 60
0, 80
1, 00
1, 20
1234567891011121314151617181920212223242526272829303132
0.00
0.20
0.40
0.60
0.80
1. 0 0
1. 2 0
1234567891011121314151617181920212223242526272829303132
ECG lead
Factor loading
Factor loading
Spontaneous rhythm
Paced rhythm
120
[%]
50
0
120
[%]
50
0
BIOSIGNALS 2008 - International Conference on Bio-inspired Systems and Signal Processing
556

Davies LG, Ross IP. Abnormal P-waves and paroxysmal
tachycardia Br Heart J. 1963 sep;25:570-4.
De Ambroggi L, Aimè E, Ceriotti C, Rovida M, Negroni
S. Mapping of ventricular repolarization potentials in
patients with arrhythmogenic right ventricular
dysplasia: principal component analysis of the ST-T
waves. Circulation. 1997 Dec 16;96(12):4314-8.
Dilaveris P, Gialafos J. Future concept in P-wave
morphological analyses. Card Electrophysiol Rev
2002; 6:221-224.
Dilaveris PE, Gialafos JE, Sideris S. Simple
electrocardiographic markers for the prediction of
paroxysmal idiopathic atrial fibrillation. Am Heart J
1998;135:73-8.
Dilaveris PE, Gialafos JE. P-wave dispersion : a novel
predictor of paroxysmal atrial fibrillation. A.N.E.
2001; 6:159-165.
Jordaens L, Tavernier R, Gorgov N, ‘T Kindt H, Dimmer
C, Clement D. Signal-averaged P-wave: predictor of
atrial fibrillation. J cardiovasc Electrophysiol 1998;
9:S30-S34.
Kawano S, Hiraoka M, Sawanobori T.
Electrocardiographic features of P waves from patients
with transient atrial fibrillation. Jpn Heart J. 1988
Jan;29(1):57-67.
Keane D, Stafford P, Baker S, Lewis S, Jackson G,
Vincent R. Signal-averaged electrocardiography of the
sinus and paced P wave in sinus node disease. Pacing
Clin Electrophysiol. 1995 Jul;18(7):1346-53.
Kesek M, Jernberg T, Lindahl B, Xue J, Englund A.
Principal component analysis of the T wave in patients
with chest pain and conduction disturbances. Pacing
Clin Electrophysiol. 2004 Oct;27(10):1378-87.
Malik M, Acar B, Gang Y, Yap YG, Hnatkova K, Camm
AJ. QT dispersion does not represent
electrocardiographic interlead heterogeneity of
ventricular repolarization. J Cardiovasc
Electrophysiol. 2000 Aug;11(8):835-43.
Pan J, Tompkins WJ. A real-time QRS detection
algorithm. IEEE Trans Biomed Eng. 1985
Mar;32(3):230-6.
PRINCIPAL COMPONENT ANALYSIS OF THE P-WAVE - Quantification of Not-Dipolar Components of Atrial
Depolarization
557
