
INFLUENCES OF DIGITAL BAND-PASS FILTERING ON THE
BCG WAVEFORM
Mikko Koivuluoma
1
, Laurentiu Barna
1
, Teemu Koivistoinen
2
1) Institute of Signal Processing, Tampere University of Technology, Korkeakoulunkatu 1, Tampere, Finland
Tiit Kööbi
2
, Alpo Värri
1
2) Department of Clinical Physiology, Tampere University Hospital, Tampere, Finland
Keywords: Ballistocardiogram, ProHeMon, EMFi.
Abstract: The band pass filter is used to attenuating breathing originated signal from the heart originated BCG signal.
The bandwidth of the both signals slightly overlap, hereby the complete attenuation of the breathing is not
possible without also altering the heart originated BCG waveforms and the parameters which are obtained
from the BCG. In our study we investigated the optimal lower cut-off frequency, and 1.3 Hz was found as
the reasonable compromise between the attenuation of the breathing and the altering of the heart originated
BCG.
1 INTRODUCTION
The developments in sensors, recording devices, and
signal processing techniques, experienced over the
past two decades, significantly increase the analysis
possibilities of the ballistocardiogram (BCG). The
potential of BCG to provide valuable information
about the condition of the heart was clearly
demonstrated even from early stages, when it was
used to predict the evolution of ischemic myocardial
diseases. Other clinical studies in which BCG
proved useful include prognosis, monitoring,
physical conditioning, stress tests, evaluation of
therapy, and cardiovascular surgery (Marinelli
1991). The use of BCG has also been reported in
epidemiological and cardiovascular screening
studies (Star and Wood, 1961; Kiessling, 1970;
Lynn and Wolf, 1974). Because during the signal
measurement stage, no electrodes need to be
attached to the body of the subject, BCG presents
great potential for modern healthcare, especially in
the case of home care monitoring.
The majority of modern BCG analysis methods
rely on two separate stages, the signal measurement
and the offline signal analysis with the help of a
digital computer. When this is the case, one can
closely look into the measured signal and decide
about the filtering methods appropriate for each
particular measurement. Such offline or visual
analysis of BCG signals is time consuming and the
costs associated with it are considerable. A better
solution was offered by the advances of computers
and electronic technology that provide a good basis
for automatic cardiac performance monitoring and
heart disease diagnosis, by assisting clinical practice
and thus saving diagnosis time.
Because the raw BCG signal is usually corrupted
with breathing and movement artifacts, a pre-
processing of the raw data is necessary before the
interpretation stage can take place. For a real-time
automatic BCG analysis system, one should know in
advance how this preprocessing will affect the BCG
waveform. In the mid sixties the subjects were
asked to hold their breath for some part of the
recording, in order to eliminate the respiration effect
on the BCG signal. Although this technique
increases the quality of the raw BCG signal, it
cannot be performed over long periods of time and it
is rather uncomfortable for the subject. For these
reasons digital filtering was proposed as an
alternative, but was not pursued until recently due to
the limitations of computing power at that time.
This study was made to investigate how
bandpass filtering the raw BCG signal at different
cut-off frequencies affects the BCG waveform, with
respect to the BCG waveform parameters usually
taken into consideration as meaningful diagnostic
information.
84
Koivuluoma M., Barna L., Koivistoinen T., Kööbi T. and Värri A. (2008).
INFLUENCES OF DIGITAL BAND-PASS FILTERING ON THE BCG WAVEFORM.
In Proceedings of the First International Conference on Bio-inspired Systems and Signal Processing, pages 84-89
DOI: 10.5220/0001061100840089
Copyright
c
SciTePress
Q
Q
Q
R
R
R
S
S
S
H
H
H
I
I
I
JJ
J
K
K
K
L
L
M
M
N
N
O
O
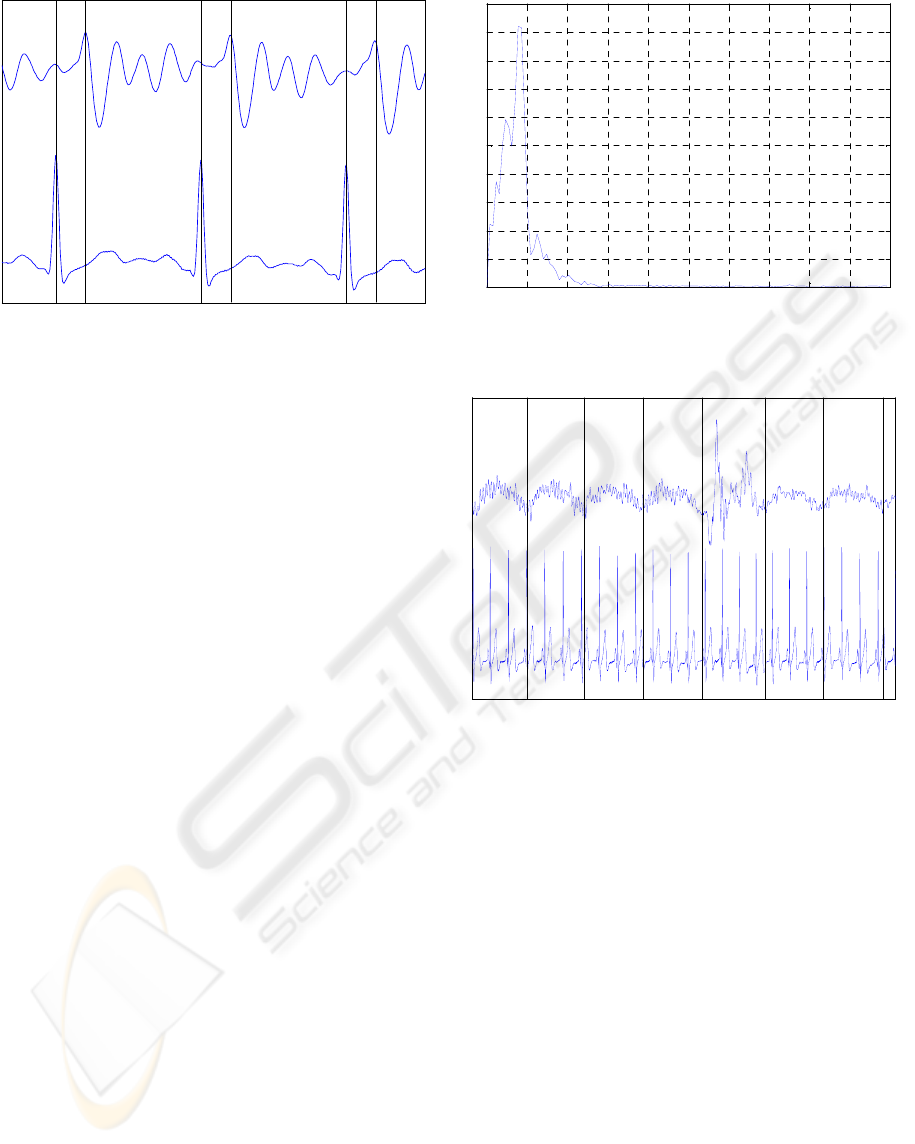
BCG Signal
ECG Signal
Figure 1: One dimensional BCG (top) and ECG (bottom)
signals from a normal healthy subject during breath
suppression.
2 THE BALLISTOCARDIOGRAM
BCG is a measure of the heart’s mechanical activity
associated with the flow of blood out of the heart’s
chambers. It was studied very actively from the
1940s until the mid-1970s when research activity in
this area ended almost completely due to the
technical limitations of sensors, signal conditioning
electronics, recording devices and the high
diagnostic value of the already available
electrocardiogram (ECG). With the advance of
technology, BCG signals can now be easily
recorded, unobtrusively, both on supine and sitting
positions using noninvasive modern techniques.
The idealized BCG waveform consists of seven
components, labeled the H through N wave (Starr
and Noordergraaf, 1967) with the IJK-complex
being the predominantly identifiable segment (see
Fig. 1). In time, typically the BCG will trail the ECG
by about 0.1-0.3s (Braunstein and Thomas, 1953).
A simple spectral analysis of the BCG signal
shows that the spectra power of the BCG waveform
is mostly within 20Hz (see Fig. 2) but in literature is
was reported that the BCG waveform lies between
0.1 Hz and 40 Hz.
BCG waves change with respiration and from
one patient to another making BCG analysis a rather
difficult task. Moreover, usually the raw BCG signal
is also corrupted with movement artifacts, which
makes the recognition of characteristic BCG
waveforms almost impossible (see Fig. 3). In order
to eliminate the respiration effect, seen as a drift
from the baseline of the signal, various bandpass
digital filters have been used and reported in
literature with the most common frequency range
0 10 20 30 40 50 60 70 80 90 100
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
Frequency (Hz)
Figure 2: Power spectrum of the BCG wave shown in Fig.
1. As it can be seen, the spectra power are mostly within
20Hz.
BCG signal
ECG signal
movement artifact
breath cycle
Figure 3: One dimensional BCG (top) and ECG (bottom)
signals from a normal healthy subject. Notice the
breathing effect on the BCG signal as a drift from the
baseline and the movement artifact that causes
abnormalities in the signal and makes the detection of the
BCG peaks difficult.
being between 1 Hz and 20 Hz. Filtering above 1 Hz
should eliminate the respiration effect but as
different people have different respiration
frequencies the filter could be selected at a lower or
higher cut-off frequency, depending on the
parameters studied. Because the BCG signal has
components below 1 Hz as well and any kind of
digital filtering will affect those components, it is
important to know how the BCG waveform will be
affected by filtering at different cut-off frequencies
in order to know the tradeoff between the selected
cut-off frequency and the changes suffered by the
BCG waveform due to filtering.
Traditionally the physicians interpret different
parameters of the measured BCG waveforms and
calculate relevant indicators to determine whether or
not the heart shows signs of cardiac diseases.
INFLUENCES OF DIGITAL BAND-PASS FILTERING ON THE BCG WAVEFORM
85

The various reported off-line analysis methods
use different relations between the BCG peaks to
classify the waveforms. The average cardiac stroke
volume can be estimated as follows (Starr et al
1940):
3/2
7(3 2)ACSV I J AC=+
(1)
where I and J are the BCG waves (in mm), A the
subject’s aortic internal diameter (in cm
2
) and C the
duration of the cycle (in seconds). From the ACSV,
the cardiac output can be further calculated (Brown,
Hoffman and De Lalla 1950, Starr et al 1940 ).
The amplitudes of the H-I, I-J, and J-K segments
and their expiratory and inspiratory ratios HI
E
/HI
I
,
IJ
E
/IJ
I
, JK
E
/JK
I
were used to express respiratory
variation in BCG waves and the HI
M
/IJ
M
and
JK
M
/IJ
M
ratios of the averaged mean amplitudes
were used as amplitude ratios (Onodera 1964,
Scarborough 1953, March 1955). The time
amplitudes (TA) obtained by dividing the amplitude
of a segment by its interval measured in expiratory
and inspiratory phases investigated on H-I, I-J, and
J-K intervals have also been reported. Other
intervals measured in the literature are: the P-H
interval measured from the beginning of the P wave
of the electrocardiogram to the tip of the H of the
Ballistocardiogram the Q-H, Q-I, Q-J and Q-K
measured from the beginning of the Q wave of the
electrocardiogram to the H, I, J, and K tips of the
Ballistocardiogram (Onodera 1964).
3 PATIENTS AND METHODS
In this study we used a subset of 15 subjects from
the signal database recorded during the ProHeMon
project (Koivistoinen et al. 2004). All the
measurements were conducted by an experienced
research nurse at the Department of Clinical
Physiology of the University Hospital from
Tampere, Finland. The study protocol was approved
by the Ethical Committee of Tampere University of
Tampere and a written consent was obtained from
each subject measured. Part of the measurement
protocol included the parallel measurement of ECG,
impedance cardiogram (ICG) and two BCG
channels. The subjects were divided into three
groups (5 subjects in each group):
1. 20-30-year old healthy students
2. healthy 50-70-year old men
3. 50-70 year old men with myocardial infarct
in their medical history
Figure 4: Recording setup. In this case, no ICG leads were
connected.
All measurements were done with CircMon™, a
commercially available circulation monitor (
Jr
Medical Ltd). The ECG and ICG leads were
connected to their own dedicated channels of
CircMon and two BCG signals were connected to
auxiliary input channels. A measurement chair with
electromechanical film (EMFi™) (Kirjavainen
1987) foils and a dedicated BCG amplifier specially
designed and built for this study were used to record
and amplify the BCG signals from the back and the
seat of the chair (Junnila et al 2004, Barna et al
2005, Junnila et al 2005). The quality of the signals
was visually inspected and assessed by specialist
medical doctors. In this setup CircMon functioned as
an A/D converter and a sampling frequency of 200
Hz was used for each recording. The recordings
lasted for about 13 minute per subject. At the
beginning of the recording, the subject was placed in
supine position and no BCG signal was recorded.
This study does not include the study of the ICG
signals obtained. The gain of the BCG amplifier was
increased after the first group was recorded, so the
absolute signal values between groups are not
comparable.
The BCG signal, was filtered offline with a
Parks-McClellan optimal equiripple band-pass Finite
Impulse Response (FIR) filter designed in Matlab®
7.2 (The MathWorks Inc.). The advantage of using
an FIR filter is that the phase of the input signal is
not distorted and the delay introduced by the filter
can be easily calculated, the information about the
time location of the BCG waveform being
preserved. The lower cut-off frequency of the pass-
band was varied between 0.7 Hz and 4.6 Hz with a
step of 0.1 Hz and the upper cut-off frequency was
fixed at 20.5 Hz. A ripple of 0.1 dB was set for the
pass-band and attenuation of 60 dB for both stop-
BIOSIGNALS 2008 - International Conference on Bio-inspired Systems and Signal Processing
86
0 10 20 30 40 50 60 70 80 90 10
0
−120
−100
−80
−60
−40
−20
0
Magnitude (dB)
Frequency (Hz)
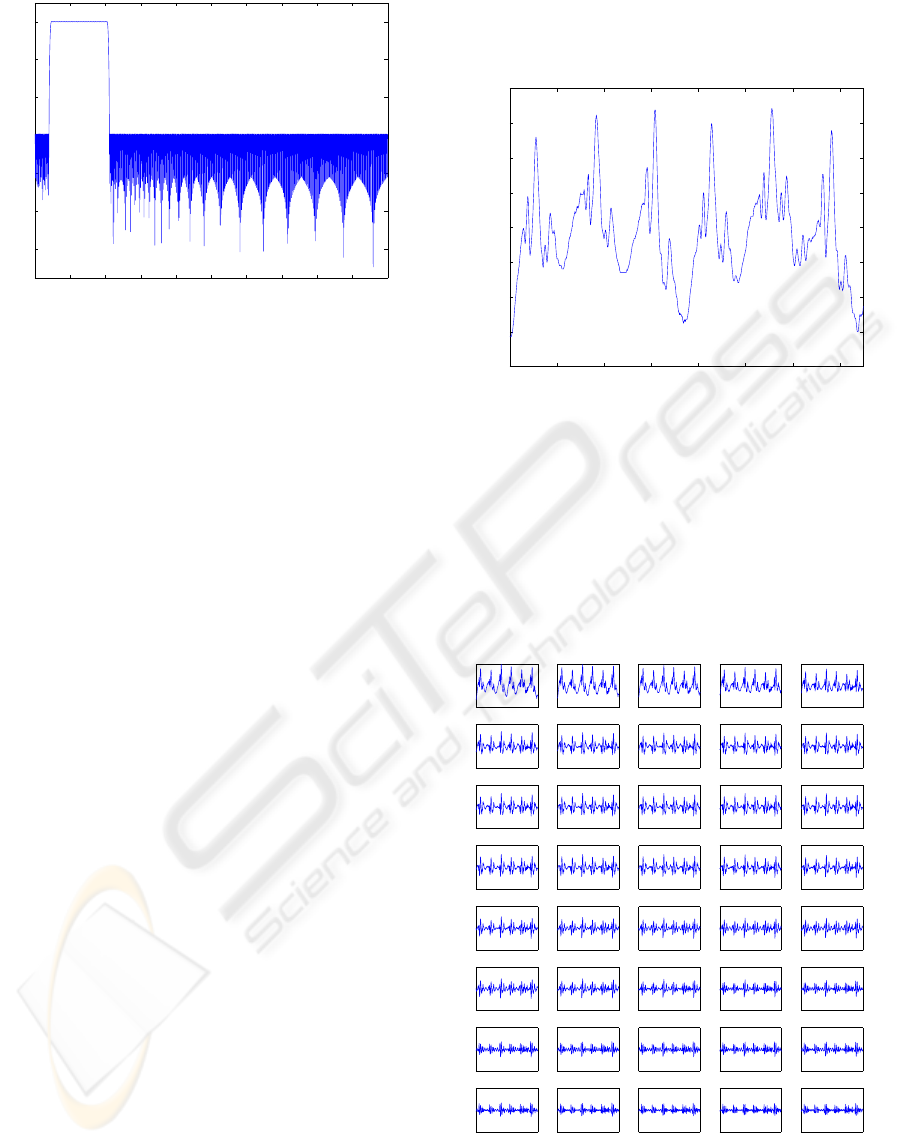
Figure 5: One FIR filter used in study. This filter have
passband from 4.6 to 20.5 Hz.
bands. The transition band width was set to 0.6 Hz
(see Fig. 5 for example). The order of the filters used
was rather high (N = 848), which resulted in a high
computation time at filtering.
After filtering, the locations of the BCG
waveforms were determined using the R spikes of
the parallel ECG tracing. The BCG signal was
divided into sections of 151 samples. A mean BCG
waveform (BCGM
NB
) was calculated as the mean of
50 % of the most similar BCG waveforms found
from the artifact free epochs of the recording. Cross
correlation was used as the measurement of the
similarity, and no visual inspection was involved.
For each mean BCG waveforms the following
parameters were calculated:
- the amplitudes of the mean H-I and I-J waves
- HI
M
/IJ
M
ratios of the mean H-I and I-J waves
4 RESULTS
In this section, a sample recording is first analyzed,
followed to an overall assessment for all the
recordings involved in this study.
In the Figure 6, the original signal (A01) with six
heartbeats is shown. The respiratory signal can be
clearly seen as a low frequency drift from the
baseline of the signal. In this example, the
measurement of characteristic BCG waveforms is
not difficult, because the heart originated component
has relatively high amplitudes compared to the
respiratory signal. Figure 7 shows the same section
of the BCG signal, band-pass filtered at different
cutt-off frequencies. When the lower cut-off
frequency is between 1.3 Hz (row one, column two)
and 2.5 Hz (row four, column four), the shape of the
signal is almost constant. Therefore, an optimal
lower cut-off frequency of about 1.3 Hz is
recommended. By studying the changes in
amplitudes of the different waveforms and HI
M
/IJ
M
ratio, we can find a more accurate cut-off frequency.
0 1 2 3 4 5 6 7
−0.2
−0.15
−0.1
−0.05
0
0.05
0.1
0.15
0.2
Amplitude
Time (s)
Figure 6: Raw BCG signal (subject A01).
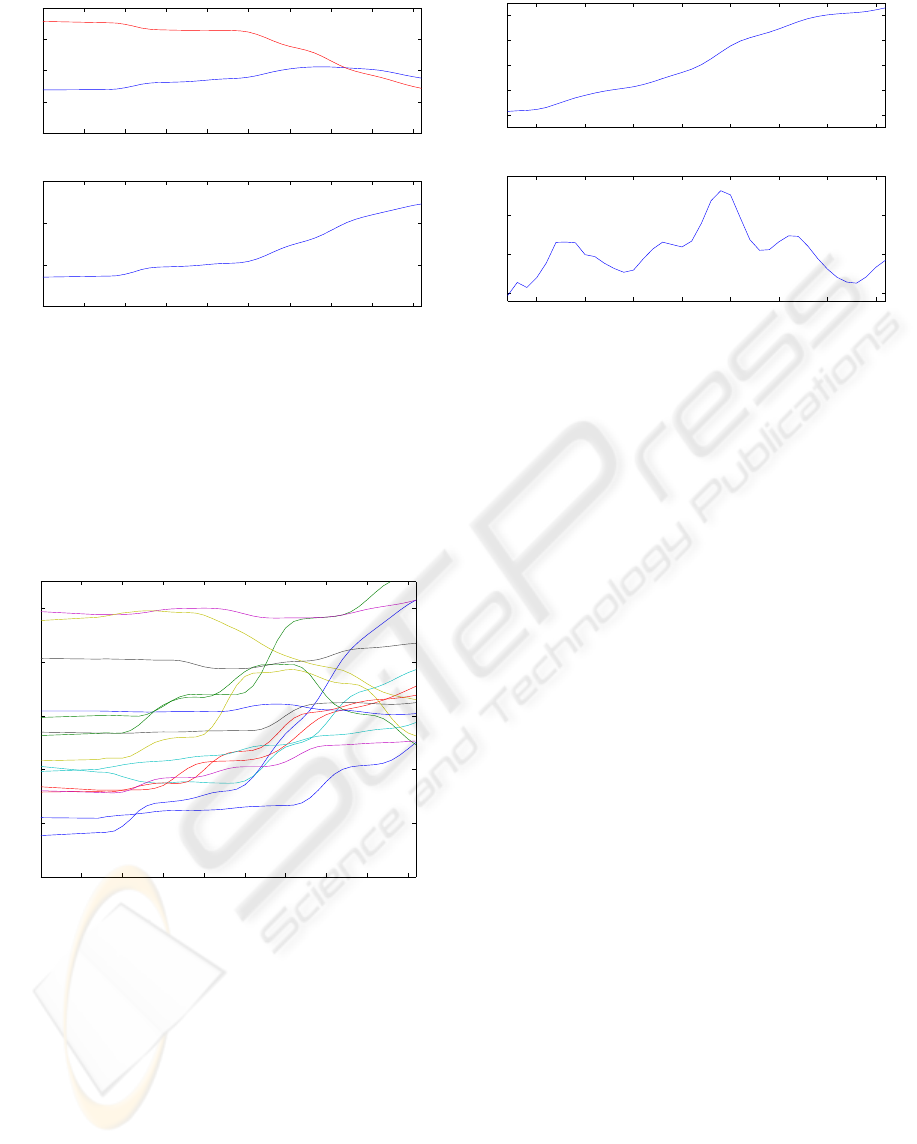
The changes of different parameters resulted from
filtering, and expressed as function of the lower cut-
off frequency are shown in figure 8. As seen from
the previous graphics, the parameters remain
relatively constant between 1.3 Hz and 2.5 Hz, with
significant changes occurring between 1 Hz and 1.2
Hz, and after 2.6 Hz. A lower cut-off frequency can
be therefore selected between 1.3 Hz and 2.5 Hz
without greatly compromising the BCG parameters.
Figure 7: The section of the BCG-signal filtered with 40
different band pass filter. In the upper left corner is the
output of the filter with pass band from 0.7 Hz to 20.5 Hz,
and in the lower right corner is the output of the filter with
pass band from 4.6 Hz to 20.5 Hz.
INFLUENCES OF DIGITAL BAND-PASS FILTERING ON THE BCG WAVEFORM
87
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5
0
0.05
0.1
0.15
0.2
Amplitude
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5
0
0.5
1
1.5
Ratio
Frequenzy (Hz)
Figure 8: The different parameters as the function of the
lower cut-off frequency. Up: mean I-J amplitude (red) and
mean H-I amplitude (blue). Down: HI
M
/IJ
M
ratio.
Figure 9, shows the HI
M
/IJ
M
ratios of the all
recordings used in this study. In the most cases,
HI
M
/IJ
M
ratios present a flat section between 1.3 Hz
to 2.2 Hz, the mean HI
M
/IJ
M
ratio and approximate
derivative of the mean HI
M
/IJ
M
, shown in Figure 10
supporting this observation.
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5
0.2
0.4
0.6
0.8
1
1.2
Frequency (Hz)
Ratio
Figure 9: HI
M
/IJ
M
ratios of the recordings used in this
study. Although up to 1Hz the ratios remain rather flat and
between 1Hz and 1.3Hz they get significantly changed,
when filtering at 1Hz the effect of respiration is still
visible in the signal, but at 1.3Hz this effect gets
eliminated (this being better for a visual inspection of
Starr classes).
Based on the observations made upon the entire
set of BCG recordings employed, the optimal lower
cut-off frequency recommended is of 1.3 Hz. For
this value, most of the signal remains unaltered, and
the major effects of the respiration are removed.
1 1.5 2 2.5 3 3.5 4 4.5
0.7
0.75
0.8
0.85
0.9
Ratio
1 1.5 2 2.5 3 3.5 4 4.5
0
5
10
15
x 10
−3
Frequency (Hz)
Figure 10: Up: the mean HI
M
/IJ
M
ratio. Down:
Approximate derivative of the mean HI
M
/IJ
M
ratio.
5 DISCUSSION
Setting the cut-off frequency of the BCG band-pass
filter is a trade-off between attenuating breathing
and altering the heart-originated components of the
raw BCG signal. Individual cut-off frequencies
might be optimal, but that would make the
comparison between patients more difficult. By
using a cut-off frequency 1.3 Hz, a reasonable
compromise was found.
Our results also show that changes of BCG
components as a result of filtering can be estimated
and accounted for in reporting BCG derived
measures and ratios. By analyzing BCG data from
recordings involving breath suppressed epoch, we
expect to refine our results in a future study.
In this study no attempts have been made to link
the amplitudes and ratio calculated from the BCG
signal to any of the cardiovascular variables such as
stroke volume
The equation presented in section “The
Ballistocardiogram” for the average cardiac stroke
volume was not feasible because no calibration has
been performed for the BCG system used and the
subjects were recorded in sitting position, unlike
Starr et al, in which the recordings were performed
in supine position. As future improvements, we plan
to combine the information available in the ECG and
ICG recordings with the one obtained from BCG..
REFERENCES
Barna, L.C., Koivuluoma, M., Värri, A., “Heart-rate
detection using EMFi sensors on a normal looking
BIOSIGNALS 2008 - International Conference on Bio-inspired Systems and Signal Processing
88

chair”, Proceedings of the 3rd European Medical &
Biomedical Engineering Conference, IFMBE
European Conference on Biomedical Engineering,
EMBEC 2005, Prague, Czech Republic, 20-25
November, pp. 5 p, 2005
Braunstein, J., Thomas, C., “The ballistocardiogram, a
dynamic record of the heart,” Springfield, IL:
Springfield, 1953
Brown, H.R., Hoffman, M.J., De Lalla, V.,
"Ballistocardiographic findings in patients with
symptoms of angina pectoris," Circulation, vol. 1, pp.
132-140, January 1950
Jr Medical Ltd, “U.S. Patent No. 6,228,033 B1: Apparatus
and methods for a noninvasive measurement of
physiological parametres,” May 8 2001.
Junnila, S., Koivistoinen, T., Kööbi, T., Niittylahti, J.,
Värri, A., "A Simple Method for Measuring and
Recording Ballistocardiogram," in Proc. 17th Int.
EURASIP Conference BIOSIGNAL 2004, Brno,
Czech Republic, June, pp. 232–234, 2004
Junnila, S., Barna, L., Koivistoinen, T., Koivuluoma, M.,
Alametsä, J., Kööbi, T., Turjanmaa, V., Niittylahti, J.,
Värri, A., “Development of a wireless proactive
ballistocardiograph chair,” In: Linden, G. (ed.).
Proceedings of the Proactive Computing Workshop
PROW 2004, Helsinki, Finland, 25-26 November, pp.
pp. 25 - 28, 2004
Junnila, S., Akhbardeh, A., Koivistoinen, T., Värri, A.,
“An EMFi-film Sensor based Ballistocardiographic
Chair: Performance and Cycle Extraction Method,”
Proc. IEEE Workshop on Signal Processing Systems,
Athens, Greece, 2-4 Nov 2005
Kiessling, C.E., “A preliminary appraisal of the prognostic
value of ballistocardiography,” Bibl. Cardiol., vol. 26,
pp. 292-295, 1969
Kirjavainen, K., “U.S. patent #4654546:
Electromechanical film and procedure for
manufacturing same,” 1987.
Koivistoinen, T., Barna, L., Alametsä, J., Junnila, S.,
Koivuluoma, M., Kööbi, T., Turjanmaa, V., Värri, A.
“Ballistocardiograms from young adults in sitting
position using EMFi sensors,” Proceedings of the 31st
Annual Meeting of Computers in Cardiology 2004,
Chicago, Illinois, USA, 19-22 September, pp. 5 p, 2004
Koivistoinen, T., Junnila, S., Värri, A., Kööbi, T., "A new
method for measuring the ballistocardiogram using
EMFi sensors in a normal chair," Proc. 26th Annual
International Conference of the IEEE Engineering in
Medicine and Biology Society, San Francisco,
California, USA, 1-5 September, pp. 4 p, 2004
Lynn, T.N., Wolf, S., “The prognostic significance of the
ballistocardiogram in ischemic heart disease,” Am.
Heart J., vol. 88, pp. 277-280, 1974
March, H.W., “Three-Plane Ballistocardiography: The
Effect of Age on the Longitudinal, Lateral, and
Dorsoventral Ballistocardiograms,” irculation, vol. 12,
pp. 869, 1955
Marinelli, R.A., Penney, D.G., Marinelli, W.A.,
Baciewicz, F.A., Jr., “Rotary motion in the heart and
blood vessels: A Review,” J. Appl. Cardiol., vol. 6,
pp. 421-431, 1991
Onodera, K., “A study on ballistocardiogram recorded
during valsalva maneuver in healthy persons and
patients with abnormal blood pressure,” Jpn Circ J.,
vol. 28, pp. 493-504, July 1964
Scarborough, W.R., Davis, F.W., Baker, B.M., Mason,
R.E., Singewald, M.L., Lore, S.A., Fox, L.M., “A
ballistocardiographic study of 369 apparently normal
persons; an analysis of normal and borderline
ballistocardiograms,” Am Heart J., vol. 45, pp. 161-
89, February 1953
Starr, I., Schroeder, H.A., “Ballistocardiogram. II. Normal
standards, abnormalities commonly found in diseases
of the heart and circulation, and their significance”, J
Clin Invest., vol. 19, pp. 437–450, May 1940
Starr, I., and Wood, E.C., “Twenty years studies with the
Ballistocardiograph, the Relation between the
amplitude of the first record of ‘health’ adults and
eventual mortality and morbidity form heart disease,”
Circulation, vol. 23, pp. 714–732, 1961
Starr, I., Noordergraaf, A., “Ballistocardiography in
cardiovascular research,” Philadelphia (PA): JB
Lippincott, pp. 166-189, 1967
INFLUENCES OF DIGITAL BAND-PASS FILTERING ON THE BCG WAVEFORM
89
