
A FRAMEWORK FOR DYNAMIC KNOWLEDGE ACQUISITION
Ana Aguilera and Alberto Subero
Facultad de Ciencias y Tecnología, Universidad de Carabobo, Valencia, Venezuela
Keywords: Collaborative Work, Multi-agents, Medical diagnosis.
Abstract: This article proposes a conceptual model based on agents in medical workgroups for the resolution of
clinical cases. Our objective is to provide a suitable conceptual framework for the dynamic acquisition of
expert knowledge from different sources. This framework is sufficiently flexible to allow its transformation
to the symbolic level that finally characterizes the implementation approach; it is a design model prior to
implementation. We considered an interface design to be used for the integration and combination of
different sources of expertise. The subject which interests us is the knowledge produced in the workgroup
processes.
1 INTRODUCTION
There are many applications related to the
workgroup such as decision-making, monitoring,
transmission, planning, idea generation, problem
resolution, resulting discussion, negotiation, conflict
resolution, analysis and system design and
collaborative group activities such as the preparation
and distribution of documents, to mention just a few.
This work style is illustrated by real-life
applications, where their nature is clearly
collaborative. Several of these applications imply
various specialized fields, such as medical diagnosis.
The field of medicine has become so vast that it is
divided into several specialities and many medical
cases are considered by group analysis. Among the
various workgroup activities, complex-problem
resolution is highlighted as being an increasingly
important subject today.
Different information technologies which
consider these group modalities have been
developed in software engineering. Thus, we found
a broader field entitled group support systems or
electronic meeting systems which include other wide
areas like Group Decision Support Systems (GDSS),
Distributed Group Support Systems (DDSS),
Computer Support Collaborative Work (CSCW),
Groupware, where the common denominator of such
technologies covers, but is not limited to, distributed
facilities, computer hardware and software, audio
and video technology, procedures, methodologies,
facilitation, and applicable group data (Turban,
1995).
On the other hand, the evolution of the
application domain in traditional Artificial
Intelligence (AI) to cover other complex and
heterogeneous fields such as aid to decision-making,
form recognition and comprehension, process
control, etc., shows the limits of traditional AI
approaches. All this has contributed to the birth of a
new discipline: Distributed Artificial Intelligence
(DAI), which is interested in the intelligent
behaviours (and their modelling) that are the
outcome of cooperative activity between several
agents. Nevertheless, the passage from individual
behaviour to collective behaviour is not only
considered as an extension but as an enrichment of
AI, as new properties and new behaviours emerge
from it. The purpose of DAI is to provide a remedy
for the shortcomings of the traditional AI approach
by proposing expertise distribution for an agent
group capable of working and acting in a common
environment, and solving possible conflicts. New
concepts in AI have appeared, such as cooperation,
action coordination, negotiation and emergence.
Three fundamental research areas of DAI are multi-
agent systems (MAS) (Weiss, 2000), distributed
problem solving (DPS) and Parallel Artificial
Intelligence (PAI).
2 THE PROBLEM
Everyday medical work (implying inter-consultation
between specialists, case conferences, and hospital
morning rounds) includes exchange and cognitive
58
Aguilera A. and Subero A. (2008).
A FRAMEWORK FOR DYNAMIC KNOWLEDGE ACQUISITION.
In Proceedings of the International Conference on e-Business, pages 58-63
DOI: 10.5220/0001913800580063
Copyright
c
SciTePress

processes within groups. It is possible to observe
different physicians (specialists and non-specialists)
working together, at the same time or at the different
time, on the same patient (clinical examination often
requires the cooperation of several specialists). The
contribution of these exchanges to solve complex
problems is becoming more and more essential.
These acts of collaboration are important for clinical
decision-making concerning diagnosis and treatment
both for students still in training and recently
qualified physicians, without forgetting the
continuous experience which helps to develop expert
knowledge. There are several examples: cases of
multi-system illnesses where physiopathology and
the nature of origin of the illness make it necessary
to examine the results of several diagnostic
procedures; patients with chronic disorders such as
diabetes mellitus, obstructive pulmonary illnesses,
cardiological illnesses; or patients receiving
palliative care at home.
On the whole, the most frequent scenarios where
it is possible to observe this collaborative pattern
are:
Inter-consultations. This is a process where a
physician needs specialized consultation with
several other physicians. There are two possibilities
for this process: 1) between specialists with the same
speciality (consultation between radiologists who
study an image to decide on a diagnosis) and 2)
between specialists with different specialties (an
obstetrician who refers his/her patient to a
cardiologist for a coronary problem).
Case Conferences and morning rounds. There are
cases where it is possible to find several physicians
(specialist physicians interconnected with general
practitioners) exchanging information on several
medical cases in order to make patient evaluations,
to work on the publication of cases, etc. These are
considered as staff meetings.
A clinical case illustrating this type of work is
shown in figure 1 (A more detailed explication is
found in (Quintero, 2003). In this case, we can
observe the interaction between a generalist, a
radiologist and a pathologist.
3 PROPOSITION
3.1 Architecture
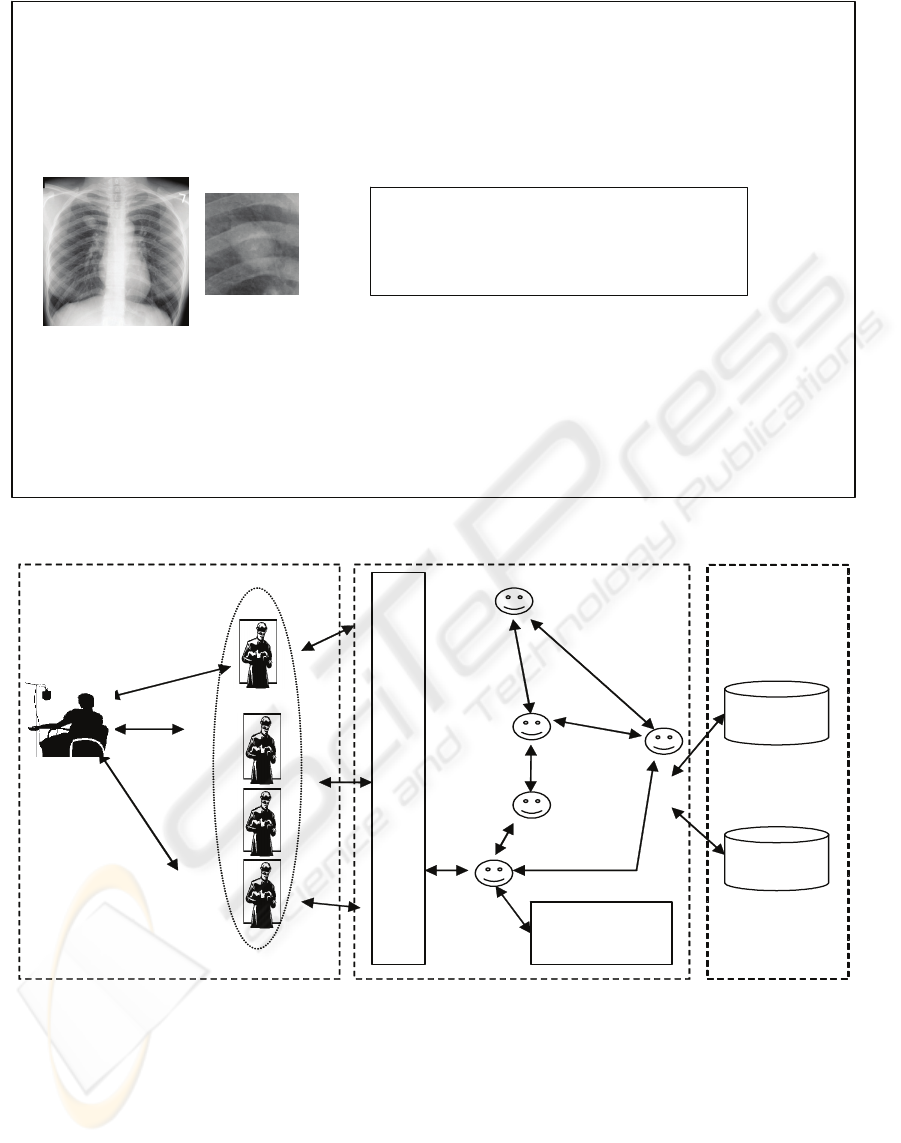
The problem follows a structure on three levels
(Figure 2): the collaborator level or users (human
agents), computer systems agents (software agents)
and the data level (databases and knowledge bases).
This architecture determines the structure on which
the framework will be defined and permits us to
clarify the semantic definition of the problem under
study.
3.2 Methodology
Different methodologies for the development of
knowledge-based systems (where knowledge
acquisition and modelling play a leading role) have
emerged during the past 15 years. We can mention
in particular methodologies such as KADS
(Schreiber, 1993), VITAL (Domingue, 1993),
REFLECT (Reinders, 1991), (van Harmelen, 1992),
ACKnowledge (van Heijst, 1992), CommonKADS
(Schreiber, 2000) and KATEMES-MultiExp
(Ladibi, 1995). KADS and VITAL focus on the
development cycle of a knowledge-based system,
REFLECT proposes theories and architectures for
reflexive systems, ACKnowledge introduces
directive models for knowledge modelling.
CommonKADS offers methodology for knowledge-
intensive system development and for knowledge
management and KATEMES-MultiExp is a
prototype tool for multi-expert knowledge
acquisition.
The approach used is based on an extension of the
KATEMES-MultiExp methodology. This method
integrates a set of models for modelling multi-
expertise and its objective is to help the knowledge
engineer in the collecting and modelling phase of
human behaviours in cooperative problem solving.
These models are: agent, organization, cooperation,
task and communication models (Aguilera, 2003b).
We added a coordination model (Aguilera, 2003a)
because originally KATEMES was designed for
knowledge acquisition before system development
and we considered the dynamic knowledge
acquisition approach. One of the important features
considered is the ability to extract expertise in a non-
intrusive way. This minimizes biased behaviour by
monitoring expert decision makers directly (through
the information system) during their daily tasks,
without changing anything about their choices or
strategies. The approach is based on the concept of
the agent, with the idea of modelling a group of
experts via a community of agents in interaction.
This gives us the additional advantage of multi-agent
systems which provide a way to relax the constraints
of centralized, planned, sequential control and to
make systems that are decentralized, emergent and
concurrent available. We are convinced that, the
modularity of a multi-agent architecture facilitates
knowledge acquisition and the parallel design of
each expertise. In fact, the multi-agent systems are
A FRAMEWORK FOR DYNAMIC KNOWLEDGE ACQUISITION
59
Circumscribed 2-3 cm Nodule located in the
right upper lobe of the lung with the
p
resence of
interior calcifications of non-specified type.
Scanner recommended. Heart and rest of study
without obvious modifications.
CAT Lung scanner: It indicates a 2 x 3 cm mass with non-epimacular aspect located in the right upper lobe of
the lung with non-specified calcifications.
There is no affectation of Mediastinum lymphatic ganglia. There are no other masses in the thorax.
Pulmonary biopsy: macro and microscopic analysis of post-operative piece.
Diagnosis: ENDOBRONCHIAL HAMARTHOMA.
The patient leaves the hospital and considering the benign origin of the pathology, the doctor recommends an
annual check up with his general practitioner.
Patient data
Age: 40 years old.
Sex: masculine
Context: He is a non-smoker and he does not present any obvious particular antecedents in his past medical
history.
Symptoms: He went to his general practitioner with a non-productive cough of three months.
Physical Test: normal
Treatment: palliative treatment
Complementary Tests: laboratory and paraclinical tests (Postero-anterior chest x-ray)
Figure 1: A clinical case.
Medical
Past History
I
N
T
E
R
F
A
C
E
Medical
Staff
Physician
(in charge
of the case)
Collaborator Level
Knowledge
base
Distributor
Agent
Planning
Agent
Manager
Agent
Interface
Agent
Data
Agent
Computer Systems Level
Data Level
App. Speciality-
oriented
Figure 2: Problem Structure.
suitable for highly dynamic domains. They belong to
the complex open systems category and make
incremental application development possible.
Our choice is justified because agent modelling
adapts well to the distributed nature of the problem,
as well as, to the preliminary phases of the
knowledge acquisition and to the development of
collaborative activities between several experts.
3.3 The Framework
It is clear that the installation of a knowledge
acquisition environment coming from multiple
experts requires a multi-field approach which, at the
same time, integrates social, cognitive and data-
processing dimensions. It is for this reason that the
objective of this model is to integrate social aspects
ICE-B 2008 - International Conference on e-Business
60

coming from the human activities, cognitive aspects
held in the databases and knowledge bases of the
system, and the aspects related to computer systems.
This proposal considers important aspects of multi-
agent systems and software engineering.
We consider the importance of the conceptual
model phase in the development of any technology,
since it provides a good definition and a clear
analysis of the problem treated. The model helps the
knowledge engineer to consider the presence of all
significant elements and their correct interrelations
and it is also an instrument which enables him to
exchange opinions with colleagues and experts, etc.
The advantage of this framework is that it offers us a
high level tool of abstraction. This tool enables us to
discuss viewpoints with others and is therefore a
facilitator for conceptual analysis. Additionally, this
framework is a set of models that gives a wide
vision including all actors, their interrelations, their
organization, their communication mechanisms, and
more.
The framework definition is given,
simultaneously in the structuring and
conceptualizing of each model in the extended
KATEMES-multiexpert methodology. At the
conceptual level we can define the following
models:
• Agent model
This model enables us to identify and define all
human and artificial individuals interacting and
taking part in cooperative problem solving. These
agents are (figure 2):
- The medical meeting agent: This is considered
as a high level hierarchical agent. It is a set of agents
and it is defined to identify the group of physicians.
The communication protocol between agents follows
human communication procedure based on personal
conversations; that is, somebody intervenes and the
others remain silent and listen, and when one person
has finished, another intervenes and so on. The
leadership position can be assumed by the doctor
sitting opposite the patient (Physician in charge of
the case).
- Medical speciality agents. They define a
classification based on the different medical
specialities, i.e., human agents such as radiologists,
neurologists, pathologists and others. The
knowledge of agents is heterogeneous. The agents
divide the tasks amongst themselves and share data
about the patient. Each one of these specialists can
observe only one part of the “outside” (i.e., the
patient).
- The patient: A human agent who as an active
being takes part in his/her treatment. He/she requests
medical appointments, takes part in his/her cure,
asks for information. He/she makes it possible to
establish the clinical context.
- The planning agent: An artificial agent which
manages everything related to time in the system:
assigns the tasks with a time context, checks the
time of their activation, execution and ending. It
returns the requests of task assignments if it has not
received an opportune response. It centralizes
information about task executions and their different
states of development.
- The distributor agent: An artificial agent which
locates the agents that will execute the tasks,
according to their specialities and availability for
executing them. For this, it takes into account the
urgency of tasks required. It centralizes information
about group members.
- The manager agent: An artificial agent which
controls the requests for tasks. It sends and receives
results.
- Interface agent: Artificial agent who controls
the security accesses to systems and data. It
adequately adapts the appropriate interface
according to each user with his/her different levels.
It centralizes general access information.
- The data agent: An artificial agent which
manages data in the databases and knowledge bases.
It manages metadata, user view definitions and
authorizations to data access. It also controls
anything related to data integrity and recovery
mechanisms.
Subsequently and for reasons of brevity we will
define only the radiologist agent. This is a human
agent, an expert and a specialist belonging to the
radiology department. He may be or not be
subordinate according to his status. He is part of a
community including radiologists or other
colleagues of different specialities (general
practitioners, pathologists, etc). All of these people
rank equally and take part in the development of a
diagnostic solution. This agent also has a
hierarchical relationship with the department head.
With respect to inter-agent relationships, the
radiologist could influence the reasoning line of an
agent with another speciality, who requires his
service for a diagnostic examination, or he could
directly influence another radiologist who discusses
a particular case with him. In the radiology
department, software systems for image processing
are frequently used. The execution of these systems
can be initiated or stopped at any time by
radiologists. Concerning cooperative relationships,
the agent can assist another radiologist in the
establishment of a diagnostic hypothesis or in other
tasks. In the medical group context, his task does not
interfere with other tasks but sometimes its
A FRAMEWORK FOR DYNAMIC KNOWLEDGE ACQUISITION
61

accomplishment is important for the continuation of
other tasks. Other inter-agent relationships can be
established, but in order to simplicity, only those
related to the example given (figure 1) will be
mentioned.
• Expertise model
Knowledge based systems are founded on a
separation between the knowledge necessary for
problem solving (domain knowledge) and the
reasoning mechanisms needed to exploit this
knowledge (inferential process knowledge for
problem solving). In the research field, this subject
remains open and there is a great diversity of
analyses and different viewpoints about it. This topic
is related to reasoning mechanisms used by doctors
in diagnostic problem solving. Many variables are
considered: patient, doctor experience, general
medical knowledge. The discussion of this theme is
extended and goes beyond the domain of this article.
We suggest readers refer to specialised literature
(Torasso 2001, Long, 2001), in particular, we refer
to (Park, 2003).
• Organisation model
In the architecture proposed (Figure 2), we find
artificial and human agents. From this, we identify
the medical group as a hierarchical structure with
two levels; headed by the physician treating the
patient, and then the rest of the doctors are
considered to be collaborators. This structure can
change by establishing as group leader another
doctor in any other speciality.
It is also possible to observe other hierarchical
structures, for example in a medical group within the
same department (radiology department, pathology
department, etc.), with the department head at the
highest level.
Within a group of artificial agents, some have
only coordination functions. A hierarchical structure
is present and centralized in the manager agent. It is
possible to observe delegation of tasks. For example,
the manager agent requests that the planning agent
specify the localization of a task and then the latter
asks to the distributor agent which finally assigns the
task.
• Cooperation model
The model presupposes the cooperative
motivation of its participants. In the case of a
medical group, the doctors can be assisted within the
same speciality, when they request consultation at
any step of the diagnostic process (doubts,
confirmations, etc.). In different specialities, no one
interferes directly with the others but their effective
participation, in the total establishment of diagnosis,
is decisive.
• Task model
To arrive at a diagnosis, doctors carry out several
tasks. In particular we mention: hypothesis
generation, selection and test of hypotheses and
diagnostic conclusion. In the case of hypothesis
generation, which is the example presented here, it is
not clear if the same process is followed equally in
every medical speciality. Undoubtedly, there are
different contexts and expertise models can vary
within the same speciality. However, it is not our
objective to present a discussion of the diagnostic
process.
• Communication model
There are several communication mechanisms
between agents given by the type of their
interrelations. For example, in the communication
between human agents, there are communications
based on spoken conversations, written
conversations (chats) or by data (medical file).
Between human and artificial agents, the
communication is established by an interface agent.
Among artificial agents, there are mechanisms based
on message passing, and finally, between artificial
agents and data, through a data agent.
Communication modelling is described by inter-
agent relationships via R-intervention relationships
which do not contradict the organisational structures
described. Some of them are shown in the definition
of the radiologist agent.
• Coordination model
Coordination is supported by artificial agents: the
manager, the planning and the distributor agent.
They centralize everything related to the
coordination tasks required. Coordination will also
depend on the dynamics of the cases exposed, their
characteristics, their emergency requirements, their
resources and the interrelations established between
the active agents..
Therefore services offered by this model depend
on: the session context, the resources provided by
participants and the social behaviour of participants
(actions carried out by human agents) (Ossowski,
1999). The combination of these three elements
creates the dynamics of coordination and the basic
actions for this collaboration; the context fixes the
limits of these dynamics.
3.4 System Design and Implementation
At implementation level, we design a multi-agent
architecture based on the framework proposed. The
different medical specialities are modelled well with
a modular structure. The current project is
progressing. So far, we have designed and
implemented a groupware application that facilitates
the management of clinical cases (Cárdenas, 2001)
and a groupware application for radiological
ICE-B 2008 - International Conference on e-Business
62

teleconsultations. The conceptual data model of our
application uses an entity relationship model. At the
moment, we are developing a workflow application
for the coordination of medical diagnostic work.
4 CONCLUSIONS
In this article we defined an agent-based conceptual
framework that integrates the social aspects of
human activities, the cognitive aspects structured in
databases and knowledge bases of the system, as
well as, the computer system aspects which are
present in the software applications and information
technologies, in the medical diagnostic context. This
approach is model-based; thus six models are
defined: the agent model, the organization model,
the cooperation model, the task model, the
communication model and the coordination model.
It is possible to instantiate these models for
particular situations, for example, clinic and hospital
frameworks. We have considered the extension of
the metamodel proposed in (Ladibi, 1995), the
annexing of the coordination model and we provided
general templates for medical groupwork. The
selection of the model-based method and the design
of the model were directed towards the dynamic
knowledge acquisition produced in collaborative
medical interactions, which is the next the step in
this research.
ACKNOWLEDGEMENTS
We are grateful to FONACIT, Venezuela, under
Project No G-2005000278, which has sponsored this
work.
REFERENCES
Aguilera A.(a), “An agent model for medical diagnostic
support with multi-experts", Sciences of Electronic,
Technology of Information and Telecommunications,
SETIT 2003, Sousse, Tunisia, Mars 2003, paper
R234A002.
A. Aguilera (b), « Télé-consultation en radiologie
médicale », Département ITI, ENSTB. Colloque Les
Nouvelles Technologies dans la cité, Rennes- France,
Déc. 2003 WWW : http://tic-cite.univ-
rennes1.fr/resume.php?lien=42.txt&mail=ana.aguilera
@enst-bretagne.fr.
F. Cárdenas, J. Pacheco, “Desarrollo del software para un
sistema colaborativo de diagnosis médica”. Thesis in
electrical engineering, Universidad de Carabobo,
2001.
J. Domingue, E. Motta Et S. Watt, “The Emerging VITAL
Workbench”, Lecture Notes in Computer Science,
volume 723, pp. 320-339. Springer-Verlag, Toulouse
and Caylus, France, 7th European Workshop, EKAW,
1993.
S. Ladibi, “Ingénierie de la Connaissance dans le cadre de
Projets Multi-Experts : Méthode, Techniques et
Outil”. Thèse Doctorale, Université de Nice – Sophia
Antipolis, 1995.
W. J. Long, “Medical informatics: reasoning methods”,
Artificial Intelligence in Medicine, Volume 23, Issue
1, August 2001, Pp. 71-87.
S. Ossowski, “Coordination in Artificial Agent Societies.
Social Structure and Its Implications for Autonomous
Problem-Solving Agents”, Number 1202 in LNAI.
Springer Verlag, 1999.
W. Park, “Causalité et Raisonnements dans le
diagnostique médical”, proceedings Setit, Sousse-
Tunisia, 2003.
J. Quintero, “Décision collaborative dans le domaine
médical analyse d’un cas de diagnostic”, proceedings
Setit, Sousse- Tunisia, 2003.
M. Reinders, H. Akkermans, et al., “A conceptual
modelling framework for knowledge-level reflection”,
AI-Communications, 4(2/3) :74-87, 1991.
G. Schreiberakkermans, H., Anjewierden, A., et al.,
“Knowledge Engineering and Management. The
CommonKADS Methodology”. The MIT Press, 2000.
P. Torasso, “Multiple representations and multi-modal
reasoning in medical diagnostic systems”, Artificial
Intelligence in Medicine, Volume 23, Issue 1, August
2001, Pp 49-69.
E. Turban, “Decision support and Expert Systems.
Management Support Systems”, Prentice Hall, 4°
Edition, 1995.
R. Van Harmelen, “Knowledge-level reflection :
Specifications and architectures”, Technical Report
R.2 RFL/UvA/III.2, ESPRIT Basic Research Action
P3178 REFLECT, REFLECT Consortium, 1992.
G. Van Heijst, P Terpstra, et al., “Using generalized
directive models in knowledge acquisition”, In Proc.
of the 6th European Knowledge Acquisition
Workshop, pp. 112-132, Heidelberg and
Kaiserslautern, Germany, Lecture Notes in Artificial
Intelligence, 1992.
G. Weiss, “Multiagent Systems: A Modern Approach to
Distributed Artificial Intelligent”, The MIT Press,
2000.
A FRAMEWORK FOR DYNAMIC KNOWLEDGE ACQUISITION
63
