
A COMPUTERIZED TESTING SYSTEM FOR SCREENING
DEMENTIA IN COMMUNITY-BASED SETTINGS
Masashi Inoue
Information Media center, Tottori University, Yonago, Japan
Yuka Okayama, Toru Horie, Tomomi Miki, Daiki Jinbo, Miyako Taniguchi, Katsuya Urakami
Department of Biological Regulation, School of Health Science, Faculty of Medicine, Tottori University,Yonago, Japan
Keywords: Computer, Screening, Dementia, Alzheimer’s disease.
Abstract: We have developed a computerized testing system for screening dementia in community-based settings. The
system was assembled with a touch-panel display and computer devices unified into one case. This made
the hardware a very compact, light and easy to carry unit. Two test programs were implemented in the
system, one for primary screening and the other for close examination. The primary screening program,
which was intended to screen persons who are suspected of having dementia in community-based settings,
consisted of 4 test tasks. The close examination program was designed to diagnose the dementia and was
composed of 10 test tasks. Throughout the whole process, users were guided not only by text prompts but
also by voice instructions. In the test process, the system presents questions by text, figures and/or voice.
Then the system shows the choice icons on the computer display and requires the subject to touch the
correct icon. By this method, even aged persons could easily operate the system. Results of the primary
screening program yielded maximum sensitivity and specificity values of 96% and 86% for the total score,
respectively. By applying this system to community-based settings, we have detected 55 persons as mild
cognitive impairment (MCI) and 74 persons as suspicious of suffering from dementia out of 998 elderly
residents.
1 INTRODUCTION
One of the most important issues in public health in
Japan is the rapidly aging society. The number of
aged persons over 65 years of age is now about
twenty-six million which amounted to over 20% of
all Japanese people in 2006. The Japanese rate of
prevalence for dementia was reported to be 10% of
all people over 65 years of age. This means that the
number of persons with dementia is estimated to
have reached more than two million in Japan. It is
important to detect the early stages of dementia
because intervention programs are more effective
when useful cognitive function can still be preserved
(Buschke et al., 1999), (Barker, et al., 2005).
Moreover, at the present time some medication can
improve symptoms and functioning and may slow
the progression of the basic disease process
(Knopman DS, 2006). However, because most
dementia patients visit the hospital after their
symptoms have become worse, medication is too
late in many cases (Bennet et al., 2006), (Ganguli et
al., 2004).
Community-based screening is the usual way to
detect persons with dementia in the early stage and
is carried out in many places. In the case that the
mass-screening is administered by human testers,
several examiners are required and their treatment
seems to be biased according to their experience or
knowledge. Moreover, there seems to be a risk that
the criteria could vary from tester to tester. The
necessary requirements which a test method must
fulfil in mass-screening are speed, objectiveness and
unbiased results even if the examiner changes.
Using a computerized cognitive test system
yields some useful features; for example, it can
provide quick, objective and precise results based on
the same standards as more involved tests (Letz et
al., 1996). For the screening of community-dwelling
elderly people with dementia, we have developed a
computerized testing system in which two test
401
Inoue M., Okayama Y., Horie T., Miki T., Jinbo D., Taniguchi M. and Urakami K. (2009).
A COMPUTERIZED TESTING SYSTEM FOR SCREENING DEMENTIA IN COMMUNITY-BASED SETTINGS.
In Proceedings of the International Conference on Health Informatics, pages 401-404
DOI: 10.5220/0001123804010404
Copyright
c
SciTePress
programs are executed, one for primary screening
and the other for close examination. In this paper,
we present a description of the system and
application of the system in community-based
settings.
2 DESCRIPTION OF THE
COMPUTERIZED SYSTEM
The system was assembled with a touch-panel
display and computer devices unified into one case.
This made the hardware a very compact (450W x
300L x 38D mm), light (2Kg) and easy to carry unit
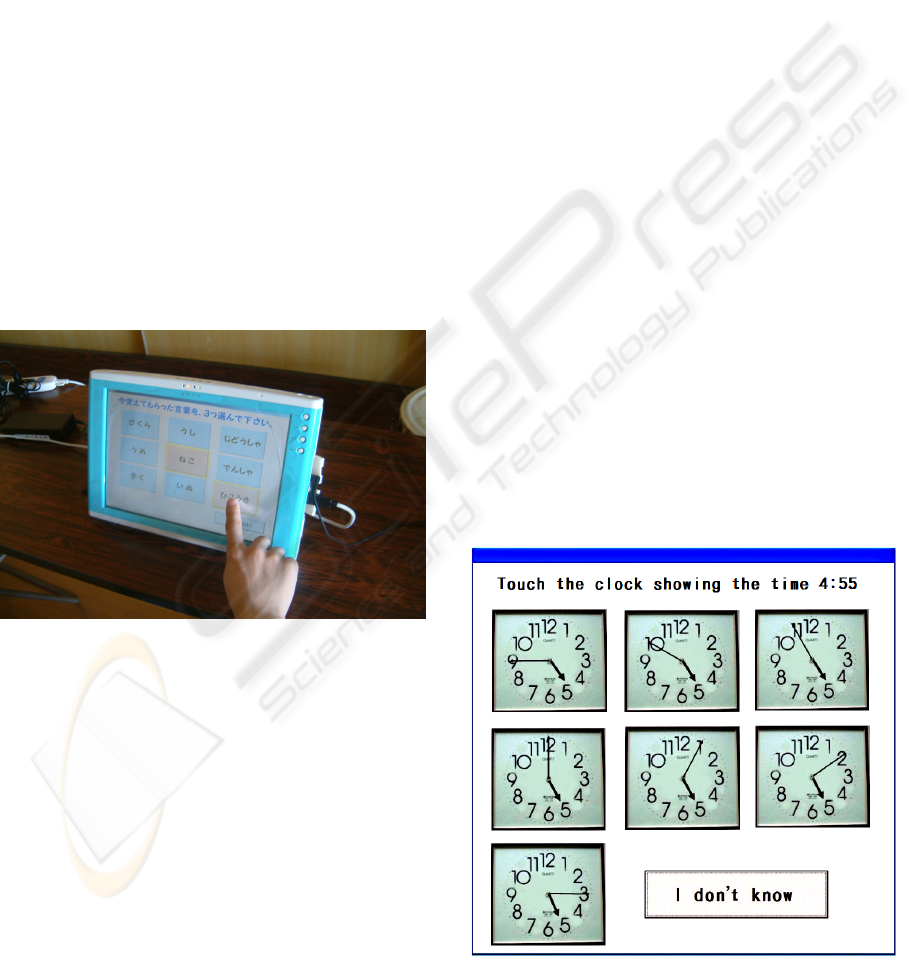
(Fig.1). The program was developed with Microsoft
Visual Basic 6.0 and run under the Windows 2000
operating system. The system was designed for use
by the elderly. We adopted a touch panel display as
an input device so that aged people could operate it
easily by touching the icon shown on the display
without using a keyboard or mouse. Throughout the
whole process, users were guided not only by text
prompts but also by voice instructions.
Figure1: Exterior view of the system.
3 DESCRIPTION OF THE TEST
PROGRAM
In the test process, the system presents questions by
text, figures and/or voice. Then the system shows
the choice icons on the computer display and
requires the subject to touch the correct icon. The
system determines if the selection is “true” or
“false” according to the icon touched.
The primary screening program was made with
reference to the Hasegawa dementia rating scale
(Katho et al., 1991)
and consisted of 4 test tasks, the
procedures usually being completed altogether
within 5 minutes. This program was intended to
screen persons who are suspected of having
dementia in community-based settings. The total
number of points on this test is 15.
Each test tasks is as follows:
(1) Three word memory test
(2) Temporal orientation test
(3) Three-dimensional visual-spatial perception test
(4) Delayed recall test
The close examination program was designed to
diagnose dementia and was made in reference to the
Alzheimer's Disease Assessment Scale (ADAS-
Cog), (Doraiswamy et al., 1997). Although, the
original ADAS-Cog was composed of 40 test items,
it was difficult to computerize all the items because
they were created based on dialogical observation.
Therefore, we selected items which were highly
significant and easy modifiable to computerization,
and assembled these into 10 computerized test tasks.
The close examination program is usually
administered within 30 minutes. In this procedure, a
perfect score is 0 which increases according to the
number and value of false answers. The score
reaches 107 when all answers are incorrect. The test
tasks for the close examination are as follows:
(1) Word recall
(2) Comprehension of spoken language
(3) Orientation
(4) Figure recognition
(5) Object recognition(6) Following a command
(7) Finger name recognition
(8) Money calculation
Figure 2: A sample computer display which assesses clock
timer recognition.
HEALTHINF 2009 - International Conference on Health Informatics
402

(9) Accuracy of the order of a process
(10) Clock time recognition (non-digital)
Figure 2 shows a sample computer display which
assesses “Clock time recognition”.
4 SUBJECTS AND METHODS
Outpatients in the Memory Disorder and Dementia
clinics at Tottori University Hospital participated.
They received neuropsychological tests as well as
neuroimaging examinations among other medical
checks. Diagnosis of dementia was made according
to criteria from Diagnostic and Statistical Manual of
Mental Disorders (3rd ed., revised) (DSM-III-R),
(American Psychiatric Association, 1987). Finally,
seventy-two patients were diagnosed with dementia.
We recruited community-dwelling elderly residents
aged over 65 as control subjects. The control group
was comprised of one hundred and two subjects with
no neurological or psychiatric pathology. All
subjects gave informed consent. By use of these
subjects, we determined the cut-off point for the
primary screening program which helped
differentiate the dementia group from the healthy
control group.
5 RESULTS
5.1 Results of the Primary Screening
Program
Results of the primary screening program showed
that the dementia group performed worse than the
control group on each of the 4 tasks. The unpaired
Student's t-test revealed that there was a significant
difference between the two groups for each
individual test and for the total score (Table1). The
sensitivity and specificity parameters and cut-off
points for the "Delayed recall test" and the
"Temporal orientation test", and the total score,
which revealed a high t-value, comparing the
dementia group with the control group, is calculated
by use of Receiver Operating Characteristic
Analysis. Finally, the analysis yielded maximum
sensitivity and specificity values of 96% and 86%
for the total score, respectively, with a cut-off point
of 13.
5.2 Result of the Screening Procedure
Nine hundred ninety-eight elderly residents aged
over 65 underwent the screening. The screening
process was done using the system as follows: first,
we screened any person whose primary test score
was 13 or less as hi-risk; then, we introduced those
hi-risk participants into the close examination test.
We regarded a person whose score on the close
examination to be 14 or more as suspicious of
suffering from dementia and recommended them to
have a medical examination. Also, we regarded any
person whose score on the close examination to be
from 7 to 13 as mild cognitive impairment (MCI).
Two hundred ninety-five people were screened as
hi-risk based on the primary test. Subsequently, they
were introduced into close examination and 151 of
them took the examination. Finally, we detected 55
persons as MCI and 74 persons as suspicious of
suffering from dementia, respectively. The suspected
74 persons were recommended to receive a medical
examination. Out of the 74 persons, 48 had received
a medical examination by the time this paper was
Table 1: The demographic characteristics of samples and results of individual test tasks out of dementia group and control
groups.
Dementia Control t-value
Sample size 72 102
Age (years) 80.0±5.1 77.1±5.8
Sex M/F 12/60 37/65
Three word memory test 2.57±0.55 2.99±0.01 5.6
*
Temporal orientation test 2.56±1.76 3.87±0.11 9.5
*
Three-dimensional visual-spatial perception test
0.82±0.15 0.92±0.07 2.1
*
Delayed recall test 3.64±4.09 5.92±0.15 11.1
*
Total score 9.87±8.53 14.1±0.53 14.0
*
* p<0.05
A COMPUTERIZED TESTING SYSTEM FOR SCREENING DEMENTIA IN COMMUNITY-BASED SETTINGS
403

written. Final diagnosis by medical specialists was
as follows: 41 were diagnosed with Alzheimer’s, 2
with vascular dementia and 5 with other diseases.
6 DISCUSSIONS
Community-based screening is a useful way to
detect persons with dementia in their early stages.
Several different tests were developed for the
purpose of screening dementia. The Mini-Mental
State Examination (MMSE) and the Hasegawa
dementia scale, which are basically based on face-
to-face interviews, are widely used to differentiate
between normal aged people and cases of dementia
in Japan. However, these tests were originally
designed to diagnose dementia, and are not suitable
for community-based settings because they take too
long and are too cumbersome to administer(David
and Jeffrey, 1999). A useful screening battery for
dementia needs to be brief, simple and accurate. In
this study, the primary screening program revealed
that overall sensitivity and specificity for screening
dementia was 96% and 86%, respectively, which
were equivalent to other studies (Mendiondo et al.,
2003), (Shulman, 2000), (Solomon et al., 1998).
When we develop a computer system whose main
target users are elderly persons, the system should be
easy to operate even by a person with slight mentally
debilitating disorders or without any type of
experience with a computer. Adopting a touch panel
display as an input device with the help of text
prompts and audio instructions could present an easy
user-computer interface and almost all of the
subjects could understand how to interact with the
system and completed the tasks by themselves. In
the actual screening procedure, we detected 55
persons with MCI and 74 persons as suspected of
suffering with dementia out of 998 elderly residents.
We believe that this computerized screening system
is useful for community-based settings and
contributes toward the early detection of persons
with dementia.
REFERENCES
Buschke H, Kuslansky G, Katz M, et al. Screening for
dementia with the Memory Impairment Screen.
Neurology 1999; 52: 231-238.
Barker WW, Luis C, Harwood D, et al. The effect of a
memory screening program on the early diagnosis of
Alzheimer disease. Alzheimer Dis Assoc Disord.
2005; 19: 1-7.
Knopman DS. Current treatment of mild cognitive
impairment and Alzheimer's disease. Curr Neurol
Neurosci Rep 2006; 6: 365-371.
Bennett DA, Schneider JA, Arvanitakis Z, et al.
Neuropathology of older persons without cognitive
impairment from two community-based studies.
Neurology 2006; 66: 1837-1844.
Ganguli M, Rodriguez E, Mulsant B, et al. Detection and
management of cognitive impairment in primary care:
The Steel valley Senior survey. J Am Geriatr Soc
2004; 52: 1668-1675.
Letz R, Green RC, Woodard JL. Development of a
computer-based battery designed to screen adults for
neuropsychological impairment. Neurotoxicol Teratol
1996; 18(4): 365-370.
Katho S, Shimogaki H, Onodera A, et al. Development of
the revised version of Hasegawa’s Dementia Scale,
Ronen Seishin Igaku Zasshi 1991; 2: 1339-1347. (in
Japanese)
Doraiswamy PM, Bieber F, Kaiser L, Krishnan KR, et al.
The Alzheimer's Disease Assessment Scale: patterns
and predictors of baseline cognitive performance in
multicenter Alzheimer's disease trials. Neurology.
1997;48(6):1511-1517.
American Psychiatric Association. Diagnostic and
statistical manual of mental disorders. 3rd ed, revised.
Washington, DC: American Psychiatric Association;
1987.
David RD, Jeffrey LC. Evaluating dementia screening
tests. Neurology 1999; 52: 224-227.
Mendiondo MS, Ashford JW, Kryscio RJ, Schmitt FA.
Designing a Brief Alzheimer Screen (BAS). J
Alzheimers Dis 2003; 5: 391-398.
Shulman KI. Clock-drawing: is it the ideal cognitive
screening test? Int J Geriatr Psychiatry 2000; 15: 548-
561.
Solomon PR, Hirschoff A, Kelly B, et al. A 7 minute
neurocognitive screening battery highly sensitive to
Alzheimer's disease. Arch Neurol 1998; 55: 349-355.
HEALTHINF 2009 - International Conference on Health Informatics
404
