
DESIGN AND ANALYSIS OF AN AMBIENT INTELLIGENT
SYSTEM SUPPORTING DEPRESSION THERAPY
Fiemke Both, Mark Hoogendoorn, Michel Klein and Jan Treur
Department of Artificial Intelligence, Vrije Universiteit, De Boelelaan 1081a, 1081HV Amsterdam, The Netherlands
Keywords: Depression therapy, Mobile phone, Internet therapy, Activity scheduling.
Abstract: This paper addresses the design of an ambient intelligent system to support humans that follow “activity
scheduling” therapy to recover from a uni-polar depression. The system consists of a personalized website
and a mobile-phone based reporting a reminder system. To analyze the system, a previously developed
dynamic model is used to simulate a client. It is illustrated by interactive simulation that the system is more
effective than the plain internet-based therapy that is offered at the moment. In continuation of the work
described in this paper a clinical trial is planned in the first half of 2009.
1 INTRODUCTION
A clinical depression is one of the most prominent
disturbances in mood. It is a common psychiatric
disorder, affecting about 7–18% of the people at
least once in their lives. In the USA, the prevalence
is approximately 14 million adults per year.
Symptoms of a depression are a deep feeling of
sadness, and a noticeable loss of interest or pleasure
in favorite activities. There is not one specific cause
of a depression, most experts believe that both
biological and psychological factors play a role.
A variety of therapies is available to intervene
within a depression, such as cognitive therapy and
activity scheduling (Lewinsohn, Youngren and
Grosscop, 1979). The basis for activity scheduling is
that a depression can be treated by increasing the
positive reinforcement through increasing the
quantity and quality of activities. Recently, it is
shown that activity scheduling interventions offered
via the Internet are very effective (Spek et al, 2007).
The problem with such Internet inventions is
however that the patient is not continuously
supported in the therapy. Having this more
continuous support might lead to a more effective
intervention. Therefore, this paper aims at given the
patient support via the mobile phone. The advantage
of using a mobile phone is that patients typically
carry this device around with them most of the time.
The support model is specified in a formal fashion to
allow for logical simulation. In order to evaluate the
effectiveness of the continuous support, a
computational model (cf. Both, Hoogendoorn, Klein
& Treur, 2008) of mood and depression is used to
investigate the influence of the support upon these
factors.
This paper is organized as follows. Section 2,
first summarizes the dynamic model for depression
adopted from (Both et.al., 2008). Section 3 briefly
describes the idea of activity scheduling. In the next
section, the ambient intelligent system model to
support activity scheduling is described. In Section
5, a simulation of two different scenarios based on
the dynamic client model is explained. This shows
that, according to the models, the system is more
effective than plain internet-based support. Finally,
Section 6 concludes the paper and describes the
clinical trial that to evaluate the system in practice
that is planned for the second half of 2008.
2 DYNAMIC MODEL OF
DEPRESSION
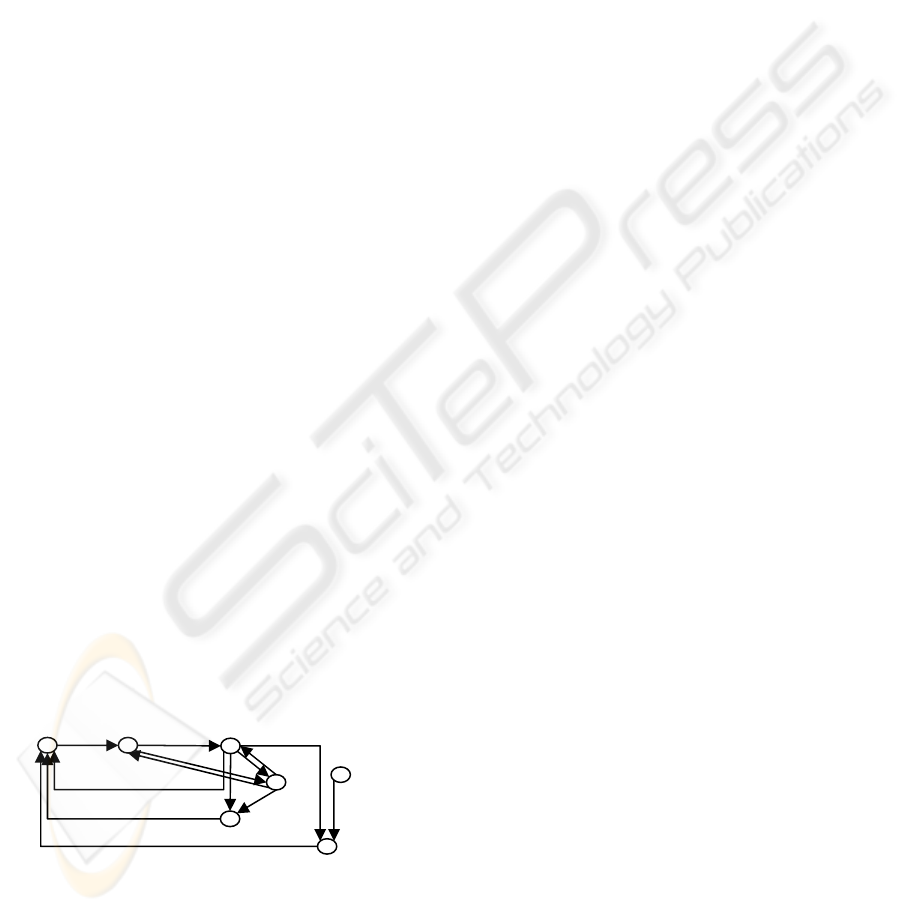
Figure 1 gives a conceptual overview of the model
developed in (Both et.al., 2008), which is based on
the major theories about a uni-polar depression. In
the model, it is assumed that every situation has an
emotional value, which represents the extent to
which a situation is experienced as something
positive.
The objective emotional value of situation
(OEVS) represents how an average person would
perceive the situation. A situation can be an event or
series of events one has no control over, or that are
chosen or influenced by the person. The subjective
emotional value of situation (SEVS) can differ from
142
Both F., Hoogendoorn M., Klein M. and Treur J. (2009).
DESIGN AND ANALYSIS OF AN AMBIENT INTELLIGENT SYSTEM SUPPORTING DEPRESSION THERAPY.
In Proceedings of the International Conference on Health Informatics, pages 142-148
DOI: 10.5220/0001432501420148
Copyright
c
SciTePress
OEVS when the thoughts of the person are more
positive or more negative than average. Negative
thoughts will cause the SEVS to be lower than
OEVS, which is often the case with a depression.
How one perceives the situation (SEVS) influences
the mood one is in and the thoughts one has. When
the person is in a positive situation, mood level and
thoughts will increase. For example, attending a
birthday party, which is usually a positive
experience, causes a better mood and more positive
thoughts. In contrast, an argument with a close
friend has a low emotional value and causes a bad
mood and negative thoughts. By changing or
choosing a situation, one can influence their own
mood level (e.g. choosing to go to the birthday party
when one feels down increases the mood level). The
complex notion of mood is represented by the
simplified concept mood level, ranging from low
corresponding to a bad mood to high corresponding
to a good mood. The mood level influences and is
influenced by thoughts. Positive thinking has a
positive effect on the mood and vice versa. The
mood level someone strives for, whether conscious
or unconscious, is represented by prospected mood
level. This notion is split into a long term prospected
mood level, an evolutionary drive to be in a good
mood, and a short term prospected mood level,
representing a temporary prospect when mood level
is far from the prospected mood level. The node
sensitivity represents the ability to change or choose
situations in order to bring mood level closer to
prospected mood level. A high sensitivity means that
someone’s behavior is very much affected by
thoughts and mood, while a low sensitivity means
that someone is very unresponsive. The level of
sensitivity itself is influenced by mood level and
thoughts. A low mood level and negative thoughts
can decrease the sensitivity and a high mood level
and positive thoughts can increase the sensitivity.
Mood level, prospected mood level and sensitivity
together influence OEVS by choosing or changing a
situation.
Figure 1: Model of mood dynamics.
The new value of a node is determined by
preceding nodes and the previous value of that node.
Decay factors determine how fast the previous value
of the node decays. For the entire model there are
two decay factors: diatheses for downward
regulation and coping for upward regulation. The
term diatheses represents the vulnerability one has
for developing a depression. The term coping
represents the skills one has to deal with negative
moods and situations. A person with very low
diatheses will probably never get a depression,
because mood, thoughts and sensitivity will go down
very slowly with a negative event. That person is
therefore always capable of choosing situations that
have a positive influence on his/her mood level and
emotions. High diatheses and low coping skills will
cause a person to get a depression very easily when
a negative event occurs, because mood, thoughts and
sensitivity will decrease fast. It will be very difficult
to climb out of a depression: the upward regulation
of mood, thoughts and sensitivity will go very slow.
3 ACTIVITY SCHEDULING
Activity scheduling (AS, also called behavioral
activation) is an intervention for clinical depression
based on a theory by Lewinsohn, Youngren &
Grosscop (1979) who say that a low rate of behavior
(often caused by inadequate social skills) is the
essence of a depression and the cause of all other
symptoms. Part of his theory is the hypothesis that
there is a causal relationship between lack of
positive reinforcement from the environment and the
depression. A depression can be treated by
increasing the positive reinforcement through
increasing the quantity and quality of (social)
activities. Many studies have shown that this type of
intervention works just as well as or even better than
other popular treatments, such as cognitive
(behavior) therapy (CT or CBT) and antidepressant
medication (Dimidjian et al, 2006; Jacobson et al,
1996; Iqbal & Bassett, 2008). Recently, it is shown
that interventions offered via the internet are very
effective (Christensen et al, 2004; Proudfoot, 2004,
Andersson et al, 2005, Spek et al, 2007).
There are two stages in AS: the first stage is
observing that pleasant activities and a good mood
come together by writing down all pleasant activities
and mood level. Usually, the more pleasant activities
have been performed, the better the mood has been.
The second stage is changing the activity schedule
so that the patient participates in more pleasant
activities with the goal of increasing the mood level.
By doing more pleasant activities in stage 2, the
mood increases on a short term, and by learning that
pleasant activities influence mood level positively,
patients are more capable of dealing with future
situations. In our model of mood and depression,
these effects can be seen as a positive influence on
sensitivity
mood level
subj. emotional value
of situation
thoughts
obj. emotional value
of situation
LT prospected
mood level
ST prospected
mood level
DESIGN AND ANALYSIS OF AN AMBIENT INTELLIGENT SYSTEM SUPPORTING DEPRESSION THERAPY
143
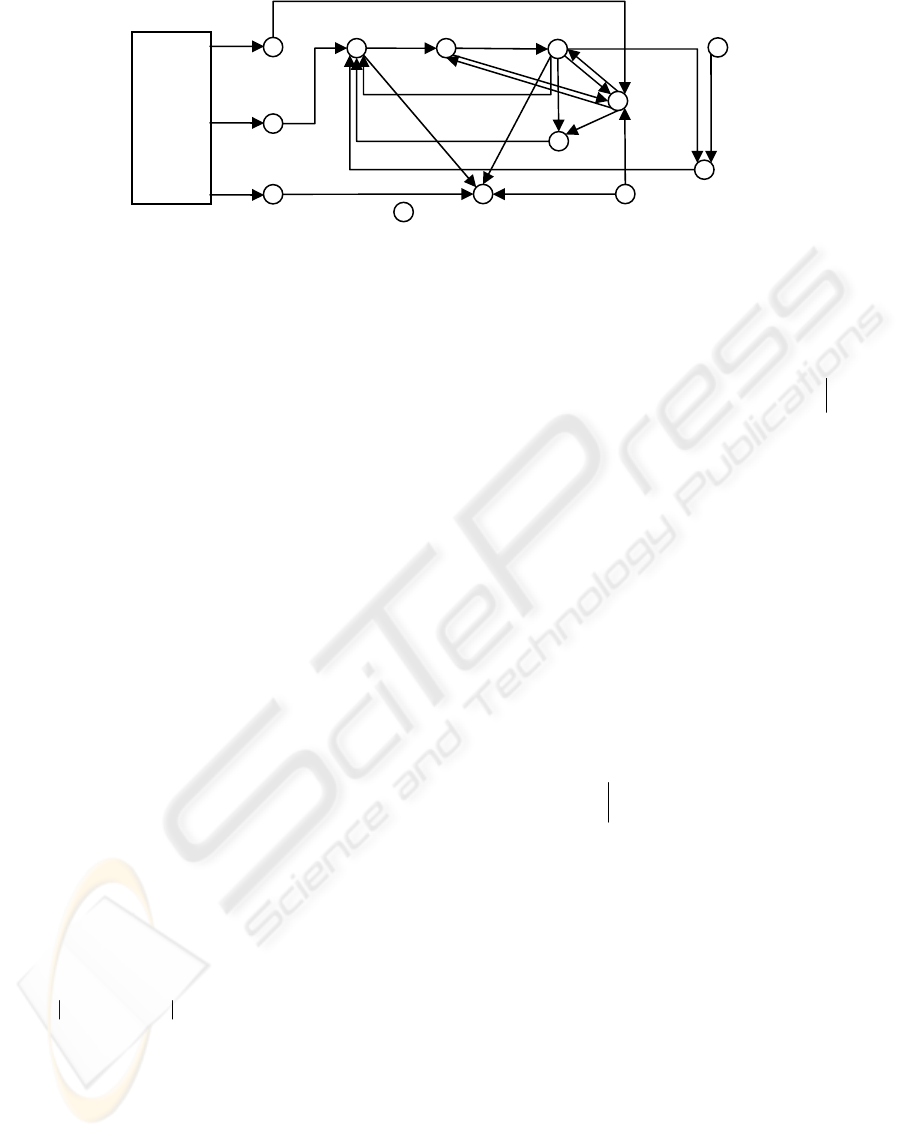
Figure 2: Effect of activity scheduling therapy in the depression model.
OEVS (increasing the number of positive activities),
thoughts and coping (learning that pleasant activities
lead to a better mood on short term and long term).
By first showing the patient that positive situations
increase mood level, negative thoughts about self,
others and world will decrease. This will result in a
higher sensitivity: the patient is more capable of
choosing a situation that increases the mood level.
When the patient is more able to choose positive
situations both by an increased sensitivity and by
stimulation from the AS intervention, the patient
will perceive the situation better and the mood level
will go up.
There may also be an initial positive influence on
the short-term prospected mood level when a person
with depression seeks counseling. This may explain
the placebo effect of antidepressant medication and
the ‘fact’ that people on a waiting list improve.
The influence of the activity scheduling occurs
on three places within the model. First of all, the
planning of activities can be used to determine the
new OEVS. Secondly, the fact that the patient is
undergoing the activity therapy will influence the
thoughts in a positive way (intervention). Finally,
activity scheduling makes the patient aware of the
relationship between OEVS and the mood level
resulting in better coping skills (reflection). Below,
in Figure 2, the graphical representation is shown.
The sensitivity for therapy influences the impact of
AS on thoughts and coping.
In the model coping is calculated as follows.
The idea behind the formula is that the patient is
learning the relationship between mood and the
OEVS. This means that the patient will learn faster
in case the two are closer. Furthermore, the more
sensitive the patient is for therapy, the faster this
learning process will go. For the calculation of
thoughts the following formula is used, which takes
the positive influence of the therapy into account:
In case the condition holds, the former is true,
otherwise the latter. The formula specifies that in
case the activity scheduling therapy is undergone
(i.e.
intervention(t) = 1) the thoughts are positively
influenced by multiplying the difference between
“optimal” thoughts (i.e. 1) and actual thoughts (i.e.
the current thoughts plus the difference caused by
the other states) with the sensitivity for the therapy.
The emotional value of a situation is determined
by the current and prospected mood levels, the
sensitivity for choosing optimal situations and the
activities done according to the AS therapy. When a
pleasant activity is done, the formula for OEVS is as
follows.
where w1 is the influence of the ability to choose a
good situation, and w2 is the influence of the
activities planned following the AS therapy.
4 DESIGN OF THE AMBIENT
ASSISTIVE SYSTEM
The activity scheduling therapy is provided in
different ways, for example with support of a
therapist (Lewinsohn et al, 1986), via self-help
books (also called bibliotherapy, e.g. Clarke 1990)
and as internet-based course.
4.1 Overall System Design
The system presented in this paper functions as a
activity
scheduling
intervention
sensitivit
y
mood level
subj. emotional
value of situation
thoughts
obj. emotional
value of situation
LT prospected
mood level
ST prospected
mood level
co
p
in
g
sensitivity
for therapy
vulnerabilit
y
reflection
activities
mood_prosp_lt)t(mood
))t(oevs(
)t(oevs
)t(activitiesw)t)t(ysensitivit)t(oevs(w)tt(oevs
mood
mood
mood
mood
mood
⋅−=
<
>=
⋅−
⋅
=
⋅+Δ⋅⋅−⋅=Δ+
βδ
δ
δ
δ
δ
ϕ
ϕ
0
0
1
21
t))t(coping())t(mood)t(oevs(
)t(therapy_for_ysensitivit)t(reflection()t(coping
)tt(coping
Δ⋅−⋅−−
⋅⋅+
=Δ+
11
)(__)(int
)()(
)(
)(
)))(()((1())(()(
)))(()((1())(()(
)(
__
ttherapyforysensitivitterventionI
wtmoodwtsevs
tth
tth
tItthdiathesestthtthdiathesestth
tItthcopingtthtthcopingtth
ttthoughts
thoughtsmoodthoughtssevs
⋅=
⋅+⋅=
<
>=
Δ⋅⋅−⋅+−+−⋅+
Δ⋅⋅−⋅+−+−⋅+
=Δ+
φ
φ
φ
φφ
φφ
HEALTHINF 2009 - International Conference on Health Informatics
144

combination of an internet-based course and the use
of smartphones: a patient plans his course via the
internet, where a server maintains personal data of
the patient and keeps track of his progress and
status; based on this status, the patient receives
personalized support via a smartphone.
Figure 3: Combined smartphone and internet support.
The basic ingredients of the internet course are
keeping a regular diary of activities and the
perceived mood, and planning and performing
pleasant activities, possibly supported by small
rewards. The assistive system helps with both tasks.
At the start of the course, the patient first has to
define his personal ordering of pleasant activities
and a list of rewards (such as “buying my favorite
magazine). For the first task of the course (keeping
the diary), the patient has to register every day the
number of pleasant activities he has undertaken and
a grade for his perceived mood. In the internet-only
version of the course, he has to do this every day
behind a computer. With the assistive system, he
will be able to report this via a simple interface on a
smartphone. For this, the phone shows the pre-
defined list of pleasant activities and allows the user
to check the activities that he has undertaken or add
a new pleasant activity. In addition, the user is asked
to rate his own mood on a scale from 1 to 10. All
provided information is then stored in the personal
profile at the web server. Because of the mobility of
the phone, the user can choose to report his activities
and mood on a more frequent basis than the per day
basis in the internet-only version, e.g. per morning,
afternoon and evening. As a consequence, the
system will result in a more fine-grained registration
of the mood, and therefore probably help people to
recognize the relation between pleasant activities
and mood earlier.
In the second phase of the course, the patient has
to plan activities. This is normally done via the
website. In this phase, the system can support by
sending reminders to the phone before the planned
start of an activity. It is up to the user to define for
which type of activity reminders are desired. For
example, activities that require a long preparation do
not benefit from short-term reminders. The
reminders could stimulate people to better keep to
their planning and thus doing more pleasant
activities. After a planned activity, the system will
ask the user whether he indeed undertook the
activity, how pleasant it was, and how he feels. The
system will give immediate positive feedback if the
mood is higher than before, e.g. ‘good to see that
you feel better now after playing tennis than you felt
this morning’. This again helps the patient to see the
relation between activities and mood. In addition,
the system will suggest to effectuate some of the
rewards if some progress has been made (e.g. a
number of pleasant activities have been performed).
After a few days of doing activities, the system
can analyze the activities and mood levels and give
personalized advice about how to proceed. For
example: ‘activity x was not as pleasant as you
thought, maybe you shouldn’t schedule it for next
week’, or ‘you have done many expensive activities,
is that why your mood is not improving?’.
The internet is the main interface that is used for
the longer term feedback. Via his personal website,
the user can consult tables and graphs that show the
relation between the number of activities undertaken
and the reported mood. Also, the long term
development of the mood level can be shown. The
user can also request this information via the
smartphone.
4.2 System Rules
Phase 1
1. if pre-set time interval has passed, prompt user
via smartphone to check the activities that have
been performed
∀I, I2:integer
frequency_set_for_first_stage(I) ∧
current_time(I2) ∧ (I2 mod I = 0) →
output(check_activities_please)
2. if pre-set time interval has passed, prompt user
via smartphone to report mood level
∀I, I2:integer
frequency_set_for_first_stage(I) ∧
current_time(I2) ∧ (I2 mod I = 0) →
output(score_mood_level_please)
Phase 2
3. if it is less than X minutes before a planned
activity and the type of activity is set to receive a
reminder, send a reminder to the smartphone
∀I, I2:integer, A:ACTIVITY
activity_scheduled_begin_time(A, I) ∧
reminder_active(A) ∧ current_time(I2) ∧
I2 = I – X →
output(do_not_forget_to_perform_activity, A)
4. if X minutes have been passed after a planned
activity, ask the user whether the activity has
been performed
∀I, I2:integer, A:ACTIVITY
activity_scheduled_end_time(A, I) ∧
DESIGN AND ANALYSIS OF AN AMBIENT INTELLIGENT SYSTEM SUPPORTING DEPRESSION THERAPY
145

current_time(I2) ∧ I2 = I + X →
output(did_you_perform_actitvity, A)
5. if the activity has been performed, prompt the
user to rate the pleasantness of the activity and
his mood
∀A:ACTIVITY
input(performed_activty, A, yes) →
output(score_mood_level_please)
6. if the reported mood level is higher than the
previously reported mood level, and the activity
was pleasant, give positive feedback message
∀I, I2:integer
input(mood_level, I) ∧ previous_input(mood_level, I2) ∧
I > I2 ∧ I > BOUNDRY_POSITIVE_MOOD
→ output(well_done_progress_can_be_seen)
7. if the first pleasant activity during the course has
been performed, suggest a reward from the
predefined list via the smartphone
∀I, I2:integer, A, A2:ACTIVITY, R:REWARD
input(performedactivity, A, yes) ∧
previous_input(performed_activity, A2, no) ∧
suitable_reward(A, R)
→ output(well_done_reward_yourself, R)
4.3 Example System Simulation
The intervention as described in the previous section
has been implemented in a simulation environment,
i.e. LEADSTO (Bosse et al,, 2007). Using this
environment, we mimicked the functioning of the
cell phone system in different scenarios. The results
of using the cell phone system in the first stage of
the activity scheduling therapy are shown in Figure
4. In the figure, the x-axis represents time (in hours)
whereas the y-axis indicates the atoms that occur
over time. In the figure a dark box indicates that the
atom is true at a particular time point, whereas a
grey box indicates it is false. It can be seen that a
frequency is initially set by the patient to receive
messages every five hours:
input(frequency_of_first_stage, 5)
As a result, the patient receives two messages asking
him to check the activities and the mood level:
output(score_mood_level_please)
output(check_activities_please)
Thereafter the patient responds with the answer that
the mood level is 2, and one activity which has been
performed, namely walking in the park:
input(mood_level, 2)
input(performed_activity, walk_in_the_park, yes)
Of course, the process continues every five hours,
but these have been left out for the sake of clarity.
The output of the support system for the second
run is shown in Figure 5. It can be seen that the
patient inputs the schedule for the day, including a
period of running from 15:00 till 16:00, going out
for dinner between 19:00 and 20:00 and going to a
birthday of a friend between 23:00 and 24:00:
input (activity_scheduled_begin_time (go_running, 15))
input (activity_scheduled_end_time(go_running, 16))
input (activity_scheduled_begin_time
(go_out_for_dinner,19))
input(activity_scheduled_end_time(go_out_for_dinner,20))
input (activity_scheduled_begin_time
(go_to_friends_birthday, 23))
input (activity_scheduled_end_time
(go_to_friends_birthday, 24))
Furthermore, reminders are set active for all
activities except for the running activity. After the
running activity schedule indicates the activity has
ended, the cell phone system asks the patient
whether the activity has been performed:
output(did_you_perform_activity, go_running)
The patient answers that this activity has not been
performed. Just before the going out for dinner
activity has been scheduled the cell phone sends a
warning, since warnings are enabled for this activity:
output(do_no_forget_to_perform_activity,
go_out_for_dinner)
After the activity is finished the cell phone asks
whether the activity has been performed, which is
indeed the case in the trace. As a result, the cell
phone sends an encouraging message (since
previously a scheduled activity was not performed):
output(well_done_reward_yourself_with,
buy_nice_present_for_yourself)
Moreover, a question is posed what the mood level
of the patient is, which is in this case ranked as 5:
input(mood_level, 5)
For the final activity scheduled for the day, a
reminder is sent again. After the activity has been
scheduled, a question is posed by the cell phone
again whether the activity has been performed. This
is indeed the case, resulting in the used scoring the
mood level which is now a 7. Since the mood has
increased compared to the previous mood level, the
cell phone sends a message:
output(well_done_progress_can_be_seen)
input(frequency_of _first_stage, 5)
output(check_activities_please)
output(score_mood_level_please)
input(mood_level, 2)
input(performed_activity, walk_in_the_park, yes)
time
0 0.5 1 1.5 2
Figure 4: Results using the cell phone system in phase one.
HEALTHINF 2009 - International Conference on Health Informatics
146
input(activity_scheduled_begin_time(go_running, 15))
input(activity_scheduled_end_time(go_running, 16))
input(activity_scheduled_begin_time(go_out_for_dinner, 19))
input(activity_scheduled_end_time(go_out_for_dinner, 20))
input(activity_scheduled_begin_time(go_to_friends_birthday, 23))
input(activity_scheduled_end_time(go_to_friends_birthday, 24))
input(reminder_active(go_out_for_dinner))
input(reminder_active(go_to_friends_birthday))
suitable_reward(go_out_for_dinner, buy_nice_present_for_yourself)
reminder_active(go_out_for_dinner)
reminder_active(go_to_friends_birthday)
output(did_you_perform_activity, go_running)
input(performed_activity, go_running, no)
output(do_not_forget_to_perform_activity, go_out_for_dinner)
output(did_you_perform_activity, go_out_for_dinner)
input(performed_activity, go_out_for_dinner, yes)
output(well_done_reward_yourself_with, buy_nice_present_for_yourself)
output(score_mood_level_please)
input(mood_level, 5)
output(do_not_forget_to_perform_activity, go_to_friends_birthday)
output(did_you_perform_activity, go_to_friends_birthday)
input(performed_activity, go_to_friends_birthday, yes)
input(mood_level, 7)
output(well_done_progress_can_be_seen)
time
0 5 10 15 20 25 3
0
Figure 5: Results using the cell phone system in phase 2.
0
0.2
0.4
0.6
0.8
1
0 20 40 60 80 100 120 140 160 180 200 220 240 260
tim e
value
oevs
sevs
mood
thoughts
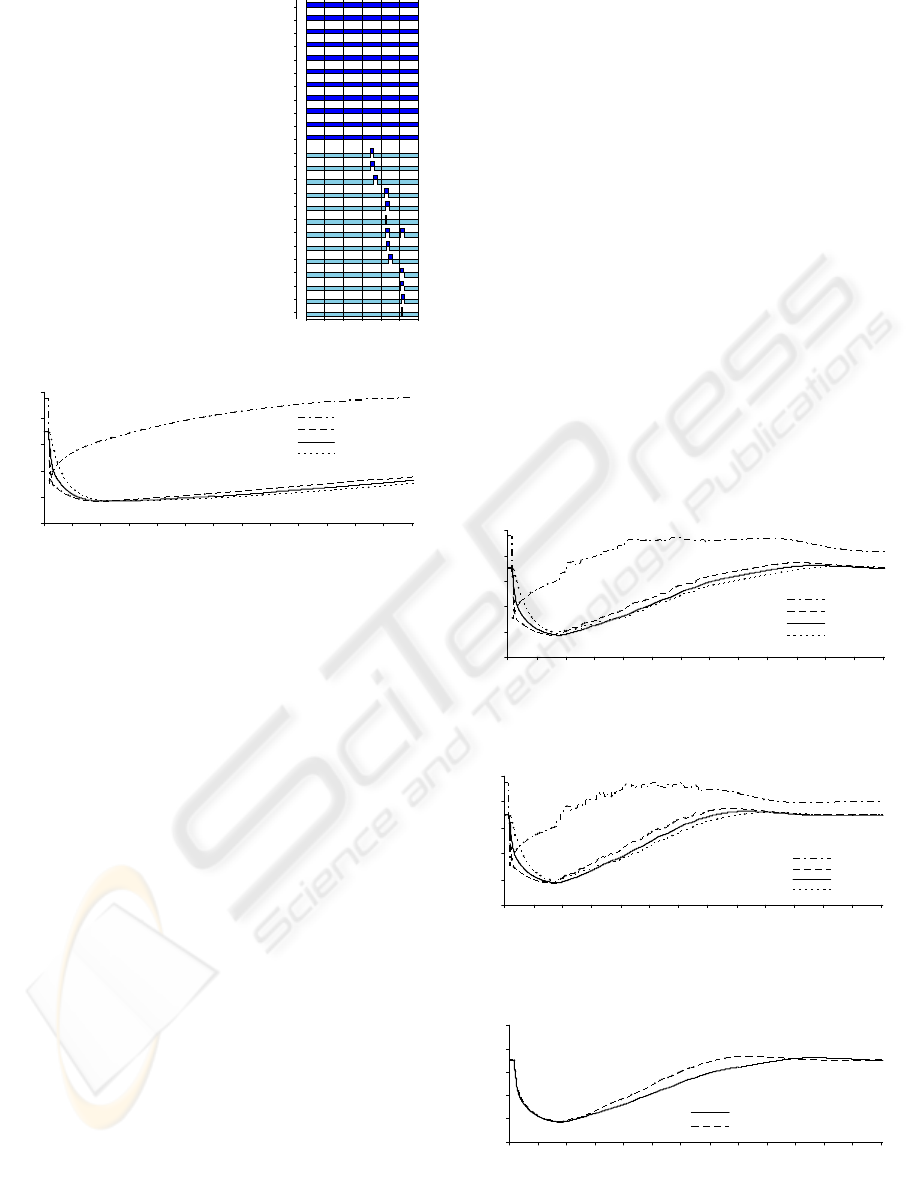
Figure 6: Unhealthy person, 1 negative event, no therapy.
5 SIMULATION-BASED
ANALYSIS OF THE SYSTEM
To analyze the system, a number of system
simulations have been performed in interaction with
a simulated client. In this interactive simulation
processes, the simulation for the system is based on
the model description in Section 4, the simulation of
the client is based on the mood dynamics model
described in Section 3. A selection of the results is
shown in Figures 6 to 9. These results show how the
supporting system has a substantial impact on the
course of the depression.
All figures show the simulated mood level
(continuous line) of a patient that has relative high
vulnerability and low coping skills. In addition, the
average objective emotional value of all events
(oevs) is shown, the perceived emotional value of
the situation (sevs), and the simulated thoughts level.
At time point 3 an event with a negative
emotional value occurs. As can be seen in all
figures, this event causes a depression in the patient:
the mood-level decreases. In Figure 6, which
represents a patient that does not receive therapy,
one can see that the average objective emotional
values of the situations increases, but that this is not
directly followed by the mood-level of the patient.
Figure 7 represents a patient (with otherwise the
same conditions as in the patient represented by
Figure 6) who receives web-based activity
scheduling therapy. The figure clearly shows that the
therapy helps to recover from the depression. The
capricious line for the objective emotional value is
caused by the pleasant activities that are undertaken
by the patient, stimulated by the therapy. In addition,
although not directly visible in the graph, the
interventions in the therapy have a positive effect on
the thoughts, and the reflection about the relation
between activities and the perceived emotional value
of the situation causes an increase in of the coping
skills.
Finally, Figure 8 shows a representation of the
same patient that follows the same therapy, but now
supported by the ambient assistive system. The
difference with the previous scenario is that the
system, following the rules described in Section 4,
helps the patient to keep to his own schedule (thus
increasing the number of pleasant activities) and is
giving positive feedback (thus further increasing the
0
0.2
0.4
0.6
0.8
1
0 20 40 60 80 100 120 140 160 180 200 220 240 26
0
tim e
value
oevs
sevs
moo d
thoughts
Figure 7: Unhealthy person, 1 negative event, web-based
activity scheduling therapy.
0
0.2
0.4
0.6
0.8
1
0 20 40 60 80 100 120 140 160 180 200 220 240 26
0
time
value
oevs
sevs
moo d
thoughts
Figure 8: Unhealthy person, 1 negative event, web-based
activity scheduling therapy with smartphone.
0
0.2
0.4
0.6
0.8
1
0 20 40 60 80 100 120 140 160 180 200 220 240 260
time
value
mood AS therapy
mood AS therapy smartphone
Figure 9: Comparison of mood level between activity
scheduling with and without smartphone.
DESIGN AND ANALYSIS OF AN AMBIENT INTELLIGENT SYSTEM SUPPORTING DEPRESSION THERAPY
147

reflection and consequently the coping skills).
Figure 9 depicts the mood-level of both types of
therapy in one diagram. The additional effect of the
supportive system is that the patient recovers more
quickly from the depression, and that his coping
skills at the end of the simulation are higher.
6 DISCUSSION
In this paper the design of an ambient intelligent
system to support people that receive activity
scheduling therapy is introduced. The system adds
personalized support for patients by analyzing their
behavior and giving them reminders, advices and
feedback during the therapy. Although the system
acts according to static rules, the rules are triggered
by actions (or the lack of actions) of patients, and as
such it provides personalized actions. The main rules
of the system are described and formalized in a
simulation environment, thus allowing for
automated simulation of the system.
Secondly, based on an earlier model of the
dynamics of mood and depression, an extension is
presented that explains the effect of (activity
scheduling) intervention. This extended model is
used to simulate a patient that receives therapy.
Together with the simulation of the system, it is
shown that the ambient assistive system indeed helps
a patient to recover more quickly from a depression,
by improving his adherence to the therapy and
increasing the level of feedback. Of course, these
conclusions are dependant on the assumptions that
underlie the model; however, as have been shown in
earlier work (Both et.al., 2008), the assumptions are
in line with the major psychological literature about
depression (therapy). Therefore, it seems reasonable
to use the model to evaluate the added value of a
specific type of support.
In the first half of 2009, a clinical trial is planned
in which this system will be tested in practice. This
requires a more detailed development of the
interface used in the smartphone to allow for simple
reporting of the mood level and performed activities.
In the future, we will work on a new version of the
system that uses the model of depression and
therapy described in this paper to reason about the
state of the patient. Using this, it would be possible
to give even more personalized advices, based on the
predicted effect of the behavior of a patient. This
would require a more thorough validation of the
model for mood and depression, as the actions of the
system will then depend on its correctness. In the
current version, there are no ethical deliberations, as
all proposed actions towards patients are already
validated and tested as part of the existing therapy.
ACKNOWLEDGEMENTS
We would like to thank prof. dr. Pim Cuijpers for his
contribution to the development of this intervention.
REFERENCES
Andersson, G., J. Bergstrom, F. Hollandare, P. Carlbring,
V. Kaldo & L. Ekselius (2005). Internet-based self-
help for depression: randomised controlled trial.
British Journal of Psychiatry, 187, 456-461.
Bosse, T., Jonker, C.M., Meij, L. van der, and Treur, J.
(2007). A Language and Environment for Analysis of
Dynamics by Simulation. International Journal of AI
Tools, vol. 16, 2007, pp. 435-464.
Both, F., Hoogendoorn, M., Klein, M.A., and Treur, J.,
Formalizing Dynamics of Mood and Depression
(2008). In: Ghallab, M. (ed.), Proceedings of the 18th
European Conference on Artificial Intelligence,
ECAI'08. IOS Press 2008, pp. 266-270
Christensen, Helen.;Griffiths, Kathleen M.; Jorm, Anthony
F. Delivering interventions for depression by using the
internet: randomised controlled trial. BMJ. 2004 Jan
31;328(7434):265.
Clarke GN, Lewinsohn PM, Hops H. (1990). Instructor’s
Manual for the Adolescent Coping with Depression
Course. Eugene, OR: Castalia Press.
Dimidjian, S. et al., Randomized trial of behavioral
activation, cognitive therapy, and antidepressant
medication in the acute treatment of adults with major
depression, J. Consult. Clin. Psychol. 74 (2006), pp.
658–670.
Iqbal, S., M. Bassett (2008) Evaluation of perceived
usefulness of activity scheduling in an inpatient
depression group. Journal of Psychiatric and Mental
Health Nursing 15 (5) , 393–398.
Jacobson, N.S., Dobson, K.S., Truax, P.A., Addis, M.E.,
Koerner, K., Gollan, J.K., Gortner, E., & Prince, S.E.
(1996). A component analysis of cognitive-behavioral
treatment for depression. Journal of Consulting and
Clinical Psychology, 62, 295-304.
Lewinsohn, P.M., Youngren, M.A., & Grosscup, S.J.
(1979). Reinforcement and depression. In R. A. Dupue
(Ed.), The psychobiology of depressive disorders:
Implications for the effects of stress (pp. 291-316).
New York: Academic Press.
Lewinsohn, P. M., Munoz, R.F., Youngren, M.A., et al
(1986) Control Your Depression. New York: Prentice-Hall.
Moore, R., Lopes, J., 1999. Paper templates. In
TEMPLATE’06, 1st International Conference on
Template Production. INSTICC Press.
Proudfoot, J. (2004). Computer-based treatment for
anxiety and depression: is it feasible? Is it effective?
Neuroscience and Biobehavioral Rev 28, 353-363.
Spek, V.R.M., Nyklicek, I., Smits, N., Cuijpers, P., Riper,
H., Keyzer, J.J., & Pop, V.J.M. (2007). Internet-based
cognitive behavioural therapy for subthreshold
depression in people over 50 years old: A randomized
controlled clinical trial. Psychological Medicine,
37(12), 1797-1806.
HEALTHINF 2009 - International Conference on Health Informatics
148
