
HIGH ANGULAR FIBER TRACKING ON THE GRID
Jasper van Leeuwen and Anca Bucur
Philips Research, High Tech Campus 37, 5656 AE, Eindhoven, The Netherlands
Keywords:
High performance computing, GRID computing, Medical imaging, Brain imaging, Decision support.
Abstract:
The grid carries the promise of seamless access to vast amounts of various resources (e.g. computational,
data, special instruments, human, etc.) in a reliable and secure manner and at low costs, at any time and from
anywhere. In this context, an increasing body of research focuses on enabling complex healthcare applications
to make efficient use of grid technologies and remote resources in clusters and grids, while satisfying the high
requirements in the healthcare domain with respect to performance, reliability, cost-effectiveness, privacy and
security. Our research aims at developing an architecture that enables computationally intensive healthcare
applications to transparently use powerful remote resources for significant performance improvement, while
being used in actual clinical environments. In this paper we apply our grid-enabled architecture to High Angu-
lar Fiber Tracking (HAFT), an imaging application with very high computational requirements. We parallelize
the HAFT application and evaluate its performance in terms of response time and scalability. Finally, we de-
ploy the application at the Amsterdam Medical Centre, in The Netherlands, and validate it (and the underlying
architecture) together with clinical users and on real patient data.
1 INTRODUCTION
The grid offers the possibility of transparently access-
ing resources, irrespective of the location of those re-
sources. It has the potential to allow easy access to
large amounts of resources without needing to own
powerful computers. This lowers the financial barrier
typically associated with the execution of computa-
tional intensive applications, enabling a large number
of users from various domains (such as high energy
physics, bio-informatics, etc) to exploit them. Typi-
cally the resources are not under centralized control
and not (fully) owned, and mechanisms (based on
open standards) are provided to integrate and coor-
dinate those resources. This provides the opportunity
of accessing powerful resources, possibly not avail-
able in the residing administrative domain. Beside
extending the capabilities of current applications, this
infrastructure also enables the development of novel
applications previously not possible due to the lack of
powerful resources on which these applications could
be deployed.
In our current research, we focus on applications
in the medical domain and on sharing of computa-
tional resources. We propose a service-oriented archi-
tecture for computationally intensive medical applica-
tions, enabling the exploitation of resources possibly
located outside the administrative domain (e.g. typi-
cally the hospital). Several medical applications have
been examined and typical decomposition patterns
have been described in (Bucur et al., 2005). For the
first decomposition pattern — computational decom-
position — white matter fiber tracking was selected
as a first use case in (Bucur et al., 2006). High angu-
lar fiber tracking (described in detail in (Hoogenraad
et al., 2005)), which is the topic of this paper,has been
selected as use case for the second decomposition pat-
tern — domain decomposition —, but this application
is suitable for computational and functional decompo-
sition as well.
High angular fiber tracking (HAFT) uses a novel
approach in order to track fibers, which achieves in-
creased accuracy compared to the standard, single-
tensor fiber tracking used as our first case study.
The most computationally intensive part of HAFT
is not the actual tracking of the fibers, but the pre-
calculation of the data—determining the double fiber
content for each voxel in the domain. The sequential
version cannot be applied in a clinical setting due to
the very large computation time.
In this paper, our Grid Architecture for Medical
168
van Leeuwen J. and Bucur A. (2009).
HIGH ANGULAR FIBER TRACKING ON THE GRID.
In Proceedings of the International Conference on Health Informatics, pages 168-174
DOI: 10.5220/0001512901680174
Copyright
c
SciTePress

Applications (GAMA) is applied to high angular fiber
tracking, employing domain decomposition for the
parallelization of the application. Our results show
that the application is very suitable for paralleliza-
tion and execution on a grid, bringing the applica-
tion within reach for clinical usage. In fact, the part
of the application parallelized in this work scales lin-
early with the number of nodes.
We have deployed the grid-based HAFT applica-
tion in an actual clinical setting at the Amsterdam
Medical Centre, where its accuracy, performance and
usability were evaluated on real patient studies.
2 GAMA OVERVIEW
In this section, we describe the context of the appli-
cations and of the domain targeted by the GAMA ar-
chitecture. After introducing the main needs we want
to address, we describe the devised architecture and
motivate our choices.
2.1 Context
The arena for our work is the medical domain. Appli-
cations in this domain become increasingly complex,
operating with high resolution images, large amounts
of heterogeneous distributed data (e.g. clinical, im-
ages, genomic, etc.) and making use of significant
computational power, while maintaining their high re-
quirements with respect to interactivity, low response
times, reliability, privacy and security, but also low
costs. While parallel computing becomes a must for
many such applications, the inherently distributed na-
ture of the data and the need to maintain low costs
motivate an increasing body of research in this area
to focus on enabling applications to make use of grid
technologies and resources. In (Breton et al., 2004)
the need for research addressing the deployment of
grid nodes in healthcare organizations and the con-
nection of healthcare professionals to the grid in or-
der to allow the deployment of grid solutions in real
settings has been identified. We circumvent this issue
with an innovative approach. With our architecture
the applications are able to make use of external grid
resources in a seamless way for the clinical user and
without the need to deploy grid nodes in the hospi-
tal domain. Through a thin interface, the applications
can securely connect to a (remote) service (described
in detail in the next section), which transparently ini-
tiates the execution of the computational part of the
application on available grid nodes or computer clus-
ters and returns the results to the user.
While other research, such as (Frate et al., 2006),
focuses on the use of the grid for enabling access
to large amounts of distributed data, our work tar-
gets computationally intensive applications that can
be efficiently parallelized. The GAMA architecture
enables medical applications to use external, power-
ful resources transparently for the clinical user, and it
is scalable for increasing problem sizes and number
of users. The clinical user does not need to have any
grid-related knowledge to use the applications built
according to this architecture and does not need to be
aware of the use of remote resources.
In (Bucur et al., 2005), a number of medical appli-
cations are analysed which currently cannot be used
in a clinical setting due to the high computational
demands. Three distinct decomposition patterns are
suggested by which the applications can be efficiently
parallelized through decomposition: functional, com-
putational and domain decomposition.
In a functional decomposition, the system is di-
vided into functional components. A performanceim-
provement can be obtained when the execution archi-
tecture of the system allows pipelining of the com-
ponents or when components can exploit previously
not available resources. Computational and domain
decomposition focuses on decomposing a functional
component. In a domain decomposition, the data do-
main (denoted by A) is decomposed into (usually dis-
joint) parts (say n parts, named a
i
with 0 ≤ i < n).
Performance improvements can be obtained when
(F(A) = ⊕
a
i
∈A
F(a
i
)), as the F(a
i
) components can
be executed in parallel. In a computational decom-
position, the computation domain (C) is decomposed
into parts (say n parts, named c
i
with 0 ≤ i < n)
and performanceimprovementscan be obtained when
C(A) = ⊕
c
i
∈C
c
i
(A), as the c
i
(A) parts can be executed
in parallel. A real-world application can display a
structure suitable for one or a combination of the three
strategies. The benefit gained with the parallelization
is a trade-off between the execution time achieved by
parallel execution versus the overhead in communica-
tion.
2.2 Architecture
As previouslymentioned, the GAMA architecture tar-
gets the medical domain and has the aim to enable
a wide range of medical applications to access (re-
mote) grid resources. The three decomposition pat-
terns introduced in the previous section are simulta-
neously supported to ensure the facilitation of a wide
range of medical applications. At the same time, the
use of grid resources needs to be minimally inva-
sive to the (clinical) user and to the associated work-
flow. This is achieved by maintaining a (thin) user
HIGH ANGULAR FIBER TRACKING ON THE GRID
169
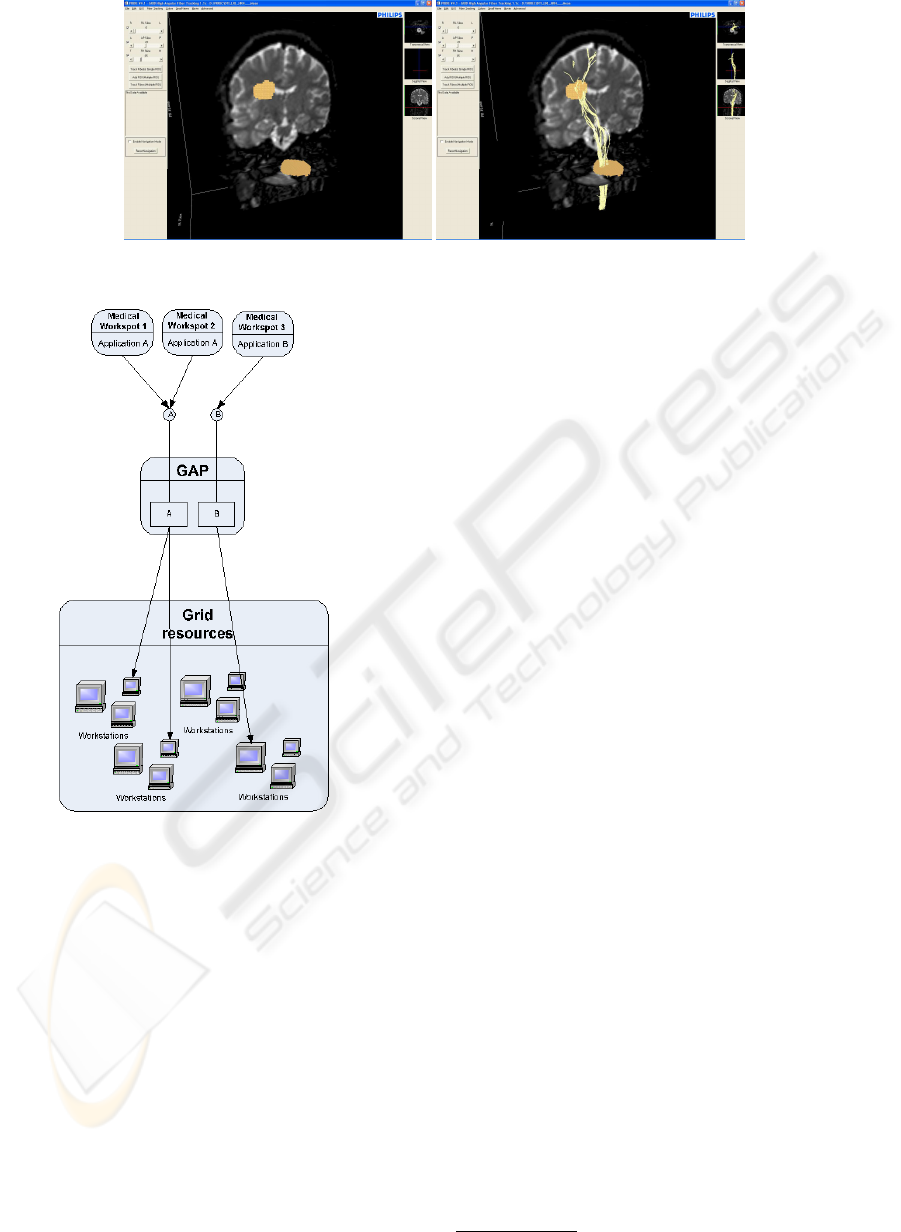
Figure 1: Visualization of HAFT output. Left: the scan with the selected ROIs, right: the resulting fibers.
Figure 2: Overview of the GAMA architecture.
interface at the hospital side. The application com-
ponents which form the bottleneck, preventing the
system from reaching the required performance, are
moved away from the hospital side to the grid-side,
and modified in order to enable good exploitation of
the available resources (see Figure 2).
In order to access grid resources from within a
hospital, a system component called Grid Access
Point (GAP) is introduced. This component acts as
a bridge to the grid resources and offers applica-
tion/computational services to workstations located in
the hospital. In this way, the GAP also encapsulates
the grid mechanisms (e.g. job-submission) of the spe-
cific grid implementation to which it is connected.
This allows for an easy switch between different grid
implementations. In the medical domain, there is also
the need for interactivity. The GAP enables interac-
tivity by relaying data streams between the hospital
side and the grid side.
Besides providing benefits from an application
(computational) point of view, the architecture also
provides benefits from a business point of view. In-
stead of offering applications, services can be offered
via the GAP. This allows for instance for a pay-per-
use business model (e.g. compared to a pay-per-
application model). In addition, different service im-
plementations can offer the same application service,
allowing for trade-offs between (for example) cost,
performance, accuracy.
2.3 The Grid Access Point
The GAP offers multiple application services to mul-
tiple users and hides grid technology details from the
(clinical) user. Via a plug-in mechanism, application
service implementations can be provided to the GAP,
that can run on the resources available to the GAP.
Interactivity is enabled by relaying data streams be-
tween the hospital side and the grid side. The security
of the datastreams between the hospital side and the
grid side is ensured by the use of ssh tunnels
1
.
The GAP can be seen as a single logical compo-
nent, but it is designed as a distributed component in
order to prevent it from becoming a bottleneck. Mul-
tiple GAPs can form a network and they can moni-
tor each other’s load.When a service is requested, an
overloaded GAP can refer a user to a less loaded GAP.
An alternative is to precede the GAP service by a
GAP-discovery service that would transparently redi-
rect the user request to the least loaded GAP. In the
current implementation the load is based on the avail-
able network bandwidth for the GAP, since the band-
width is the first bottleneck that would be reached by
a GAP component. As the GAP hides grid technology
from the user, it can be used to exploit resources avail-
able in multiple (disjoint) grids. This also includes
1
http://www.openssh.com/
HEALTHINF 2009 - International Conference on Health Informatics
170

the possibility of exploiting a locally available clus-
ter, providing a smooth transition path from locally
owned resources to shared resources. In the current
setup, globus
2
is used as grid fabric.
3 HIGH ANGULAR
FIBERTRACKING
3.0.1 Fibertracking Introduction
Fiber tracking is an indirect medical imaging tech-
nique (see (Beaulieu, 2002; Mori and Zijl, 2002)).
It uses diffusion-tensor magnetic resonance imaging
and has as goal to reconstruct axonal tracts in the cen-
tral nervous system that connect brain structures. Ex-
amples of the usage of fiber tracking are in the area
of studying brain development, multiple scleroses,
stroke and schizophrenia.
Fiber tracking relies on the observation that wa-
ter molecules exhibit Brownian motion, i.e. random
movement of molecules in a fluid or gas. The free-
dom of moving can however be restricted by, for in-
stance, the underlying cellular microstructure of tis-
sue. When molecules are in a pure liquid, the diffu-
sion is the same in all directions (so-called isotropic
diffusion). This is not the case with anisotropic diffu-
sion (i.e. when barriers such as communication tracts
connecting different brain areas exist). Diffusion Ten-
sor Imaging (DTI) shows the extent and orientation of
diffusion anisotropy or the averaged diffusion proper-
ties of the water molecules in a volume (typically a
voxel with dimensions in the order of 1 to 5 mm). The
amount of anisotropy is directly related to the cellu-
lar microstructure. This resolution is high enough to
distinguish white matter tracts in the brain. A tract
(called fiber) consists of a collection of axons (the ex-
tension of a nerve cell used to propagate information).
There are multiple ways to track the fibers. The
first category of algorithms is based on line propaga-
tion. DTI provides a 3D tensor field, which is used
to propagate a line from a seeding point. The second
category is based on global energy minimization to
find the least costly path between two points (energy-
wise). The algorithm used in our application is a line
propagation algorithm.
A common approach for tracking fibers is to cre-
ate one or more regions of interest in the dataset in
order to select fibers of interest. The purpose is to se-
lect those fibers that will go through all the regions of
interest. Commonly, the voxels in a region of inter-
est are used as seeding points for the line propagation
2
http://www.globus.org/
algorithm. The extent of the anisotropy and the an-
gle change are used as termination criteria. The line
propagation algorithm is terminated when the angle
change becomes too big, as the diffusion process is
assumed to be Gaussian, or when the anisotropy be-
comes too low (as fibers are assumed to end).
The standard single-tensor algorithm assumes that
there is clearly a principal axis in the voxel when
fibers are present. That algorithm fails however when
fibers branch or cross in a voxel (e.g. two large eigen-
values, which show two predominant directions of
propagation). This can be countered by using every
voxel as a seeding point for tracking and afterwards
selecting only those fibers that intersect the regions of
interest. This is however a time consuming approach
and in (Bucur et al., 2006) we show a successful per-
formance improvement by gridifying the algorithm
and performing a computational decomposition.
In this paper fiber branching and fiber crossing are
handled in a different way. Diffusion weighted data
sets with many gradient encoding directions are used
as input and instead of a single fiber model, a dou-
ble fiber model is used. Each voxel can be described
by a double fiber content, in terms of directions and
volume fraction. In order to get the double fiber con-
tent, a double fiber model is fitted with the apparent
diffusion coefficients for every voxel of the dataset
(Hoogenraad et al., 2005). With the obtained double
fiber content per voxel, branching and crossing fibers
can be handled successfully during tracking. This cal-
culation takes place when the data is loaded into the
application. As the solution space for the fitting pro-
cess is big, it is time consuming to determine the dou-
ble fiber content. Therefore, this is the part of the ap-
plication that we have chosen for efficient paralleliza-
tion and grid execution.
3.1 Application Design
In the workflow of HAFT, first a dataset (a DTI
scan) is selected and the double fiber content is com-
puted for the complete dataset (so-called dataload-
ing). Next, the user can interactively select regions
of interest in the application. The fibers crossing all
the regions of interest will be subsequently tracked.
Figure 1 shows the visual output of the applica-
tion with a DTI scan loaded. Regions of interest are
selected on the left side and the right side shows the
output of the application with the resulting fibers, af-
ter the tracking.
The most computationally challenging part of
HAFT is the calculation of the double fiber content.
This calculation has to be performed for each voxel of
the DTI scan. As there are no (computational) depen-
HIGH ANGULAR FIBER TRACKING ON THE GRID
171
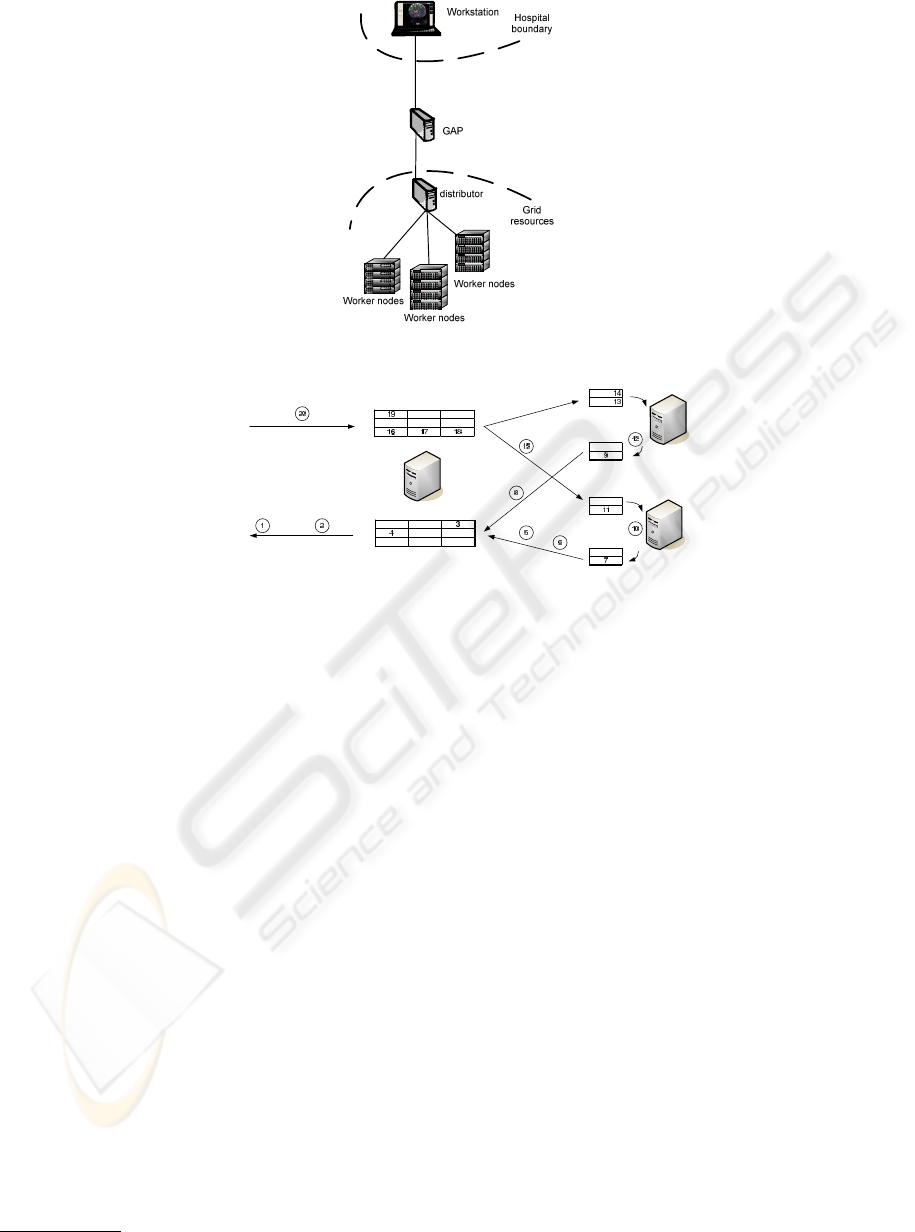
Figure 3: Deployment scenario of the grid-enabled HAFT application.
Figure 4: Topology of the grid-enabled HAFT application.
dencies between the voxels, a domain decomposition
can be performed. This means that the entire dataset
is split and distributed over the available worker nodes
and each worker node will calculate the double fiber
content for the part of the dataset assigned to it.
As grid resources may be used to deploy the appli-
cation, it should be taken into account that the avail-
able resources can be heterogeneous. This implies
that the calculation speed of the resources can differ.
Therefore, we implement a dynamic load balancing
approach where a distributor dynamically distributes
the load over the available workers. The implementa-
tion uses MPI
3
as communication library. In our im-
plementation (see Figure 3), the hospital-side work-
station will still host a light-weight client and the vi-
sual interface of the original sequential application.
The computational part of the application is extracted
and its most computationally intensive component,
which is in this case the dataloading), is parallelized
with a distributor-workers approach. In the first stage
of dataloading, the settings are sent to all the worker
nodes. The client part of the application running on
the workstation sends this data via the GAP to the dis-
tributor, which broadcasts it to all the worker nodes.
In the second stage, the dataset (the apparent dif-
fusion coefficients) is streamed from the client to the
3
http://www-unix.mcs.anl.gov/mpi/mpich2/
distributor, via the GAP. The distributor forms on-the-
fly work packages (consisting of the content of a spec-
ified number of voxels) out of the stream and sends
the work packages to the workers. The workers calcu-
late the results and send them back to the distributor.
The worker nodes use asynchronous communication
and buffering in order to hide as much (data trans-
fer) latency as possible. The distributor sends a new
workpackageto a worker as soon as it receives a result
package from that worker. This approach (depicted in
Figure 4) ensures that the workers are kept busy as
long as there is still work to be distributed, even when
the computational power of the worker nodes differs.
The distributor receives the results in a buffer, indexed
to preserve the order of the result items. The results
may arrive out of order,as the workers might not work
equally fast, and the size of the buffer dictates how
out-of-sync workers can be. When the distributor re-
ceives a set of results, these are ordered and streamed
back via the GAP to the client application.
HEALTHINF 2009 - International Conference on Health Informatics
172
4 EVALUATION
4.1 Scalability
In this section, the scalability of the algorithm is as-
sessed. Experiments were performed on a cluster of
computers. The cluster consisted of 35 nodes, having
4 3.0 GHz Intel Xeon CPU’s processors each.
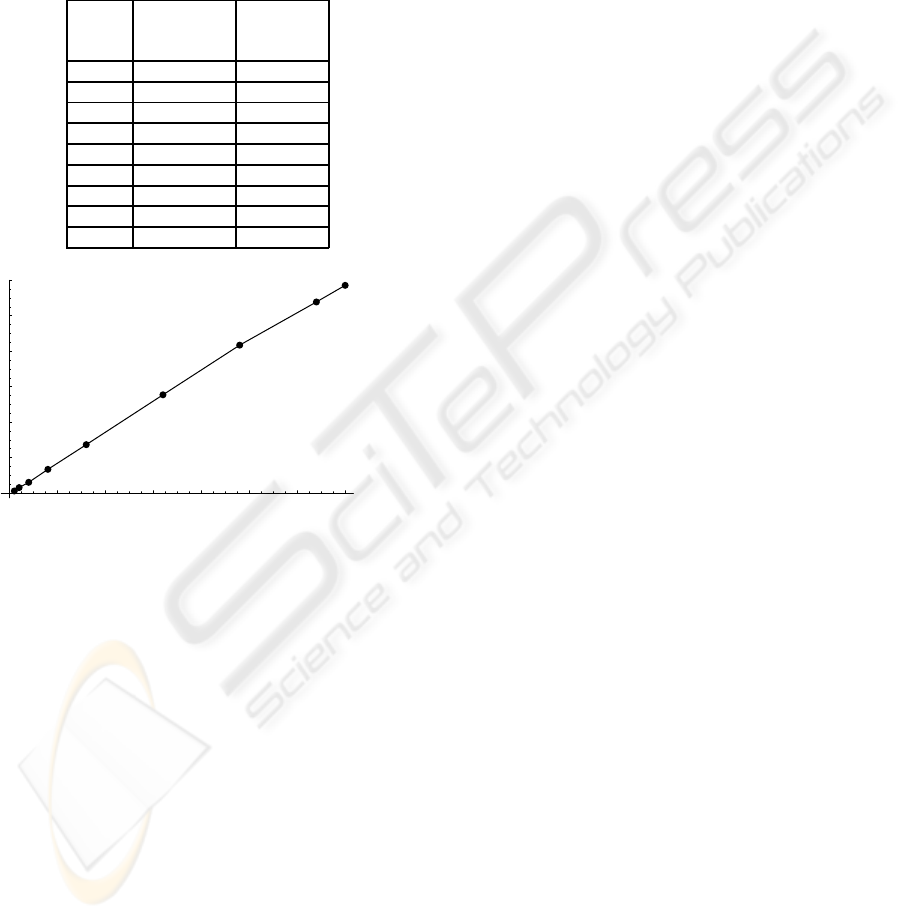
Nr resource execution
of reservation time (s)
nodes time (s)
2 77 22321
4 104 7675
8 81 3817
16 121 1720
32 128 857
64 137 439
96 159 304
128 188 246
140 175 227
20 40 60 80 100 120 140
Processes
20
40
60
80
100
120
Speedup
Figure 5: Measured response times and speedup of the
HAFT application for 1 to 140 processing nodes
As can be seen in Figure 5, the speedup with re-
spect to the number of nodes is very linear. Starting at
a calculation time of 6 hours and 12 minutes, the ex-
ecution time is reduced to 3 minutes and 47 seconds,
bringing the application within clinical reach. Sig-
nificantly larger scale-up is not desirable due to the
incurred cost of adding nodes and little (noticeable)
performance gain (as the steps with constant execu-
tion time and not parallelized, such as visualization,
increasingly dominate the total execution time).
It is expected that eventually the distributor will
become the bottleneck and will cause the speedup to
flatten, as the distributor cannot provide the workers
with enough work while gathering the results. The
computation/communication ratio of the data load-
ing phase is high and the latency is hidden (by using
buffering and asynchronous communication), which
yields that the flattening of the speedup will only hap-
pen for a very large number of nodes. At that point,
the execution time gained by using more nodes will
be spent in extra communication between distributor
and worker nodes, and the number or sizes of work
packages will be too small relatively to the number of
worker nodes.
Table 5 shows the number of nodes versus the
resource reservation time (sec.) and execution time
(sec.). In the setup, a first-come first-served was used
with respect to scheduling of jobs on the available
resources, explaining the variations in the resource
reservation times.
4.2 Requirements in the Healthcare
Domain
The domain that triggered the development of grid
middleware was high energy physics. Of course,
also other domains saw the promises. Different do-
mains may however bring in different requirements.
Currently deployed grid middleware is very focused
on long running jobs, with no interactivity or quick re-
sponse time requirements, scheduled in a batch man-
ner. The main goal of the administrators of the com-
putational resources is to keep the load of the re-
sources as high as possible, in order to maximize (de-
pending on the ownership of the resources) the cost-
effectiveness or the profit.
The medical domain brings in a whole range of
applications with very different requirements. The
requirement that is seriously hampering the effec-
tiveness of applying currently available grid technol-
ogy to the medical domain is predictability. Appli-
cations need to fit into the clinical workflow of the
user. For interactive applications, this implies that
the timespan between a request for execution and
the actual execution and returning of the results is
both short and predictable. For non-interactive (and
mostly batch-oriented) applications, this implies that
the time by which the computation will be finished
is predictable (and short enough to be clinically rele-
vant). Clinical applications may also have hard-time
requirements and it is not always the case that the
need for resources can be identified well in advance,
which means that introducing reservations may not al-
ways solve the problem. Critical applications need
to be served first - so the support of priorities may
be needed, and the alternative to extend the num-
ber of available resources may need to be supported
as well, as the load of the system is not even and
it may unpredictably peak. Currently, this matter is
resolved either by having dedicated resources avail-
able or by over-dimensioning the available resources.
Clearly, this is not a cost-effective approach. Once
Quality of Service guarantees (e.g. on scheduling
HIGH ANGULAR FIBER TRACKING ON THE GRID
173

times) become commonly available, application ser-
vice providers can provide service level agreements
suitable for the medical domain while having cost
benefits compared to dedicated solutions.
5 CONCLUSIONS AND FUTURE
WORK
In this paper we have proposed an architecture
enabling computationally intensive applications to
transparently access remote powerful resources. Our
case study was High Angular Fiber Tracking, an ap-
plication relevant in the healthcare domain, with very
high resource requirements, too high for its deploy-
ment and its use in a real healthcare environment.
Our parallelized version of the application, compli-
ant with the GAMA architecture, shows linear speed-
up, yielding excellent performance during its execu-
tion on a remote cluster. The application was brought
this way within the reach of the clinical practice, and
was deployed and validated in a clinical setting.
This work shows the potential for using grid tech-
nology in the medical domain. It has been demon-
strated that grid resources can be accessed from a clin-
ical environment transparently for the (clinical) user.
The benefits are clear, cost-effective access to a large
amount of shared resources. Technically, the main
bottleneck for accessing grid resources from within
hospital boundaries is the lack of quality of service
guarantees.
Several research issues are still to be addressed.
As future work we foresee the use of the third de-
composition pattern - the functional decomposition,
resulting in an example in each of the decomposition
patterns identified. On the GAP side, several issues
are to be explored, such as incorporating quality-of-
service guarantees. Another hot topic in the medi-
cal domain is privacy. The responsibility of the GAP
plugins could be extended with ensuring that the data
sent is anonymous, and to anonymise the data prior to
sending it to the grid resources if this is not the case.
ACKNOWLEDGEMENTS
Part of this work was carried out in the context of
the Virtual Laboratory for e-Science project
4
. This
project is supported by a BSIK grant from the Dutch
Ministry of Education, Culture and Science (OC and
W) and is part of the ICT innovation program of the
Ministry of Economic Affairs (EZ). Philips Medical
4
http://www.vl-e.nl/
Systems provided the initial data sets used in our
experiments and the sequential High angular Fiber-
tracking application that constitutes the basis for our
grid-enabled case study application. The validation
of our HAFT application was carried out at the Ams-
terdam Medical Centre, The Netherlands. AMC Re-
search has performed a clinical evaluation of the grid-
enabled HAFT application.
REFERENCES
A.I.D. Bucur, R. Kootstra and R. Belleman. A Grid Archi-
tecture for Medical Applications. Healthgrid Confer-
ence, 2005.
A.I.D. Bucur, R. Kootstra, J. van Leeuwen and H.Obbink. A
Service-oriented Architecture for Grid-enabling Med-
ical Applications. Healthgrid Conference, 2006.
F. Hoogenraad, R. Holthuizen, R. Brijder. High angular res-
olution diffusion weighted MRI. International Patent,
WO2005076030, 2005.
V. Breton, A.E. Solomonides and R.H. McClatchey. A per-
spective on the Healthgrid initiative. IEEE Int. Symp.
on Cluster Computing and the Grid, 434-439, 2004.
C. Del Frate, J. Galvez, T. Hauer, D. Manset, R. Mc-
Clatchey, M. Odeh, D. Rogulin, T. Solomonides, R.
Warren. Final Results from and Exploitation Plans for
MammoGrid. Studies in Health Technology and Infor-
matics, 120:305-315, 2006.
C. Beaulieu. The basis of anisotropic water diffusion
in the nervous system - a technical review. NMR
Biomed,15:435-455,2002.
S. Mori and P. van Zijl. Fiber tracling: principles and
strategies - a technical review. NMR Biomed,15:468-
480,2002.
HEALTHINF 2009 - International Conference on Health Informatics
174
