
POA_S@UDE
A New Collaborative Tele-ultrasonography System over PLC
Alécio Pedro Delazari Binotto
1,2
, Valter Roesler
1
, Cirano Iochpe
1,3
, André Campos da Cunha
4
Ronaldo Husemann
1
and Carlos Eduardo Pereira
1,2
1
Informatics Institute, UFRGS - Federal University of Rio Grande do Sul, Av. Bento Gonçalves 9500, Porto Alegre, Brazil
2
CETA - Center of Excellence in Advanced Technologies SENAI, Av. Assis Brasil 8450, Porto Alegre, Brazil
3
PROCEMPA - Information Technology Company of Porto Alegre, Av.Ipiranga 1200, Porto Alegre, Brazil
4
Maternal-Infant Hospital Presidente Vargas, Porto Alegre, Brazil
Keywords: Telemedicine, Ultrasonography Images/Videos, Real-time Collaboration, Multimedia.
Abstract: Access to medical care is sometimes difficult to be reached by citizens living in distant and underserved
areas. The problem increases on high complexity medical cases that are not preventively identified. The
recent advance of broadband communication, like Power Line (PLC), combined with state-of-the-art
multimedia compression methods allowed reaching isolated areas that lacks of intra/internet connections.
This paper presents the results of the POA_S@UDE Project, a research that aimed the improvement of
patient quality of life in distant urban communities from high-complexity hospitals, focusing on obstetric
ultrasonography (U/S) examinations during prenatal period. Statistics show an obstetric examination miss
rate higher 60% at the Restinga peripheral district (100,000 inhabitants) in Brazil. The main reason is the
time and financial difficulties to go to central hospitals to perform regular examinations; added with the
time gap of 4 months between an exam request and its realization by the referral hospital. Based on that, we
introduce a collaborative tele-U/S system over a PLC hybrid network based on multimedia data. The
specialist doctor assists, guides, and interacts in real-time with the remote doctor who operates the U/S
equipment. At Restinga, during a pilot of 3 months, the examination waiting time was decreased to 1 month
and the miss rate of prenatal examinations to 30%.
1 INTRODUCTION
Telemedicine represents a multidisciplinary research
area. It integrates not only efforts of various fields
from Computer Science, but also different
disciplines from medicine and other health areas. In
addition, it can involve public health policies,
government strategies and public organizations. This
way, telemedicine is currently growing as a complex
research topic for the improvement of health
services, of population quality of life, and also for
remote medical training, including resident
physicians. Based on this advance, the qualified
health care of excellence medical centres is extended
to remote and underserved areas with the
indispensible government support.
Therefore, most telemedicine applications are
massively video/image-based (data from U/S, CT,
X-ray, resonance, etc.), being used not just for
teleconsultation, but also for a simple second or third
opinion, repository research or remote training
through the Internet. Those are applications that aim,
chiefly, to provide technical support on decision-
making of non-specialist doctors, who often work in
places distant from medical excellence centers.
However, this strategy depends completely on
Internet bandwidth and its reliability and data
security. Thus, due to the precarious scenario of
poor regions, the mentioned telemedicine
applications present features that originally do not
require synchronous and real-time communication
nor need to deal with large data transferences, like
video, images, textual, and voice.
Regarding U/S examinations (the focus of our
research), it must be performed by doctors
specialized at the medical discipline related to the
exam (e.g., obstetrics, fetal medicine) and
experienced with the equipment. Particularly in
Brazil, other professionals besides doctors cannot
222
Delazari Binotto A., Roesler V., Iochpe C., da Cunha A., Husemann R. and Pereira C. (2009).
POA_S@UDE - A New Collaborative Tele-ultrasonography System over PLC.
In Proceedings of the International Conference on Health Informatics, pages 222-229
DOI: 10.5220/0001541902220229
Copyright
c
SciTePress

operate the equipment. When the local physician
lacks the knowledge or experience at the medical
discipline to perform the exams in order to acquire
meaningful videos for interpretation, the local doctor
must take the responsibility for the final exam
diagnosis, communicating with the specialist
physician who guides all the examination and
together can generate the final diagnosis. In this
case, it is suitable that both doctors have a
synchronously data communication in real-time,
mainly at the data acquiring phase, i.e., videos
generation.
When synchronous communication of images
with good quality and real-time is required, many
factors related to network and multimedia areas must
be taken into consideration, such as bandwidth,
audio and video codification, processing capability
of the involved equipments, and the end-to-end
communication delay. Usually, these factors
determine the final video quality.
In tele-U/S, real-time applications present
specific features that demand more resources from
the computer system. In this paper, real-time means
both sides communicating and not feeling
uncomfortable with the delay. According to (Bartoli,
2007), this time should be less than 400ms in IP
videoconferences to meet ITU (International
Telecommunication Union) standards. In order to
accomplish this, our research is based on MPEG-4
video codification, offering real-time
collaborative point-to-point tools.
Regarding communication, our case study is
deployed over the power lines, designated PLC
(Power Line Communication) in Europe and BPL
(Broadband Power Line) in the United States. The
data communication through electric power nets is
already an alternative that competes and/or
complements the wireless communication systems,
satellite and wired applications, like cable TVs
(Opera, 2007). We choose that type of
communication, since it is a distinct parallel project
developed by part of the authors in the same region
of the presented case study.
Based on that, this paper presents the results of
an innovative telemedicine pilot service over PLC,
named POA_S@UDE, performed at the city of
Porto Alegre (Rio Grande do Sul State, Brazil) and
its poor and remote district called Restinga. The
paper is organized as follows. It starts in Section 2
with a brief motivation and description of the
medical scenario, followed with previous and
parallel work on projects in the telemedicine and
PLC areas in Section 3. The proposed platform is
detailed on Section 4, emphasizing U/S obstetric
examinations over a hybrid PLC network. Finally,
on Section 5, we present medical, technical, and
social results achieved during the pilot and
discussions about its benefits and future directions.
2 MOTIVATION
At Porto Alegre (1.5 million inhabitants), the
Maternal-Infantile Hospital Presidente Vargas
(HPV) is a medical referral center focusing
pregnancy. The public hospital assists a vast part of
the population who lacks of specialized maternal
infrastructure. Most of its patients come from remote
districts just for the accomplishment of routinely
U/S examinations and for accompaniment of
pregnancy evaluation.
Restinga is the poorest and most remote district
of Porto Alegre, having more than 100.000
inhabitants with a population density of 23
inhabitants/ha, occupying more than 20.000 homes.
The growth tax between 1991 and 2004 was 5.6%
per year and the average monthly income of the
answerable for the domiciles is 3.03 minimum
wages. The district counts just with a small health
center and lacks of specialist physicians and basic
medical devices, which sums up an average of 300
patient transfers to HPV per month for basic
ultrasound examinations, being more than the half in
the field of obstetric/gynaecologic. In this manner, it
overflows the HPV capacity with patients that, in the
majority of the cases, could be assisted in their own
district by available General Practitioners, the
residents, whom could be guided by an expert doctor
using a basic structure with U/S and internet
connection. In fact, most of the cities have a basic
structure of general doctors who, very often, cannot
give a final and correct diagnosis without a second
medical opinion or assistance/discussion.
According to the WHO - World Health
Organisation (WHO, 2008), women need to visit a
hospital at least 4 times during the pregnancy for
periodically accompaniment. However, at Restinga
there are cases where the patient visits the hospital
for the first time just to give birth. To better illustrate
the precarious scenario from that region, there is an
obstetric examination miss rate higher that 30% in
U/S exams for pregnant woman at Porto Alegre and
more than 60% at Restinga. In addition, Restinga
presents a time gap of more than 4 months between
an exam request, by the periphery health center
generalist physician, and its realization by the
specialist doctor of the HPV.
POA_S@UDE - A New Collaborative Tele-ultrasonography System over PLC
223

3 PREVIOUS EXPERIENCES
In the recent past and at present, some technological
projects aiming social inclusion were developed at
the Rio Grande do Sul State. Two of them,
T@lemed and PLCRestinga, are the infrastructure
basis for the presented system. The first deployed an
image-based telemedicine system over the State,
while the second integrated Restinga’s public
buildings using PLC, since there was no fast internet
connection until the year of 2006. The next sub-
sections go in detail over these projects, as well as
give an overview about other related work.
3.1 Related Work
The Brazilian Government, through the RUTE
(University Telemedicine Network) initiative -
(Rute, 2008), (Simões, 2006) - has been investing at
the development and online availability of
knowledge databases related to health. The goal is to
subsidize the decision-making of health
professionals who act far from the reference medical
centers. It is a try to improve decision quality and
reduce the "ambulance-therapy" phenomenon.
Another situation was presented by (Sibert,
2008), which performed an experiment of U/S
laryngoscopy images and video transmission in rural
emergency situations. The images were transmitted
from the ambulance through mobile phones 3G
connection, but in low quality. Results showed good
system acceptance by the doctors, but with remarks
regarding image quality.
In the work of (Yee, 2005), an experience
similar to the one presented here, two hospitals in
Australia made transmissions of the ultrasonography
device screen aiming a third medical opinion. They
tested over several network rates and came to a
conclusion about the best cost-benefit rate for a good
video quality. It was a bandwidth around 1Mbps.
The work of (Reddy et al., 2000) proposed a
solution for fetal tele-U/S in remote canadian
communities, where 49 patients were observed in
remote obstetric ultrasound examinations. The
practical environment comprised two personal
computers linked via 19.2 kbps modem over an
analog telephone line.
In addition, (Chan et al., 2000) proposed a real-
time transmission of fetal ultrasound images over
long distances via ISDN lines. A link of up to 2
Mb/s was established. The proposed system
incorporated built-in interactive two-way
microphones, allowing direct communication
between both sites. Examination video has been
captured by dedicated video boards and transmitted
in rates of 30 frames per second. Over a 3-month
pilot period, 24 tele-U/S examinations were carried
out. Overall, the consultations resulted in
modifications compared to clinical diagnosis in
45.8% of the cases and modifications to the
management plan in 33.3% of the cases.
3.2 T@lemed
Following the telemedicine concepts, the T@lemed
Project (T@lemed, 2007) was based on a
teleconsultation platform, named TeleConsult,
which was developed by MedCom GmbH and the
Fraunhofer IGD and allows store-and-forward
DICOM image-based tele-diagnosis in on-line mode
or either off-line.
The TeleConsult software platform is based on
TeleInViVo (Kontaxakis et al., 2000), which is a
telemedicine workstation used in isolated areas such
as islands, rural, and crisis situation areas. The
system integrates in one custom-made device a
portable PC with telecommunication capabilities and
a light and portable 3D ultrasound station,
combining low price, low weight, mobility and a
wide range of non-radiating examinations. The
integrated workstation used advanced techniques
able to collect 3D U/S data, which were presented
on (Sakas, 1993) and (Sakas et al., 2000).
For T@lemed and for this research, the reason to
work with ultrasound data is based on its support to
a very large range of applications (Ferrer-Roca et al.,
2001), varying from gynaecology and abdominal
scans to cardiological examinations. Currently, it is
the only economically and practically affordable
imaging modality.
Figure 1: TeleConsult collaborative annotations.
As an example of its functionalities, after the
data transferring, interaction can be made in real-
HEALTHINF 2009 - International Conference on Health Informatics
224
time. Digital annotations in the medical images can
be made by the generalist and sent to the specialist
physician, aiming to delineate some region of
interest to be argued. The data sending can be
carried through an off-line connection, where
messages (images + annotations + first opinion +
other crucial region of interest) are sent in
determined moment (at night, for example) and later
on, at another moment, the specialist performs the
diagnosis or opinion; or through an on-line
connection. In this last way, depending on the
bandwidth, the data are transmitted in few seconds
and collaborative discussion (annotations + chat +
voice + measurements + interaction), is carried in
real-time. Figure 1 depicts an annotation interaction.
In the scope of T@lemed, doctors from four
remote cities of the Rio Grande do Sul State were
connected over wired internet (512Kbps) with a
referral hospital located at Porto Alegre.
3.3.1 PLC Restinga
The PLC Restinga Project, PLC network at
Restinga, arises to supply an economical gap
promoted by wire telecommunication companies to
attend deprived communities. Concerning the work
of (Borges, 2005), the digital inclusion goal in Brazil
is to look for the population (or at least its great
majority), to be able to receive access to tools,
services, and necessary technological abilities in the
new economy. The PLC technology implementation
cost and installation, using the medium tension net
for data transmission, could be cheaper than the
costs of available technologies.
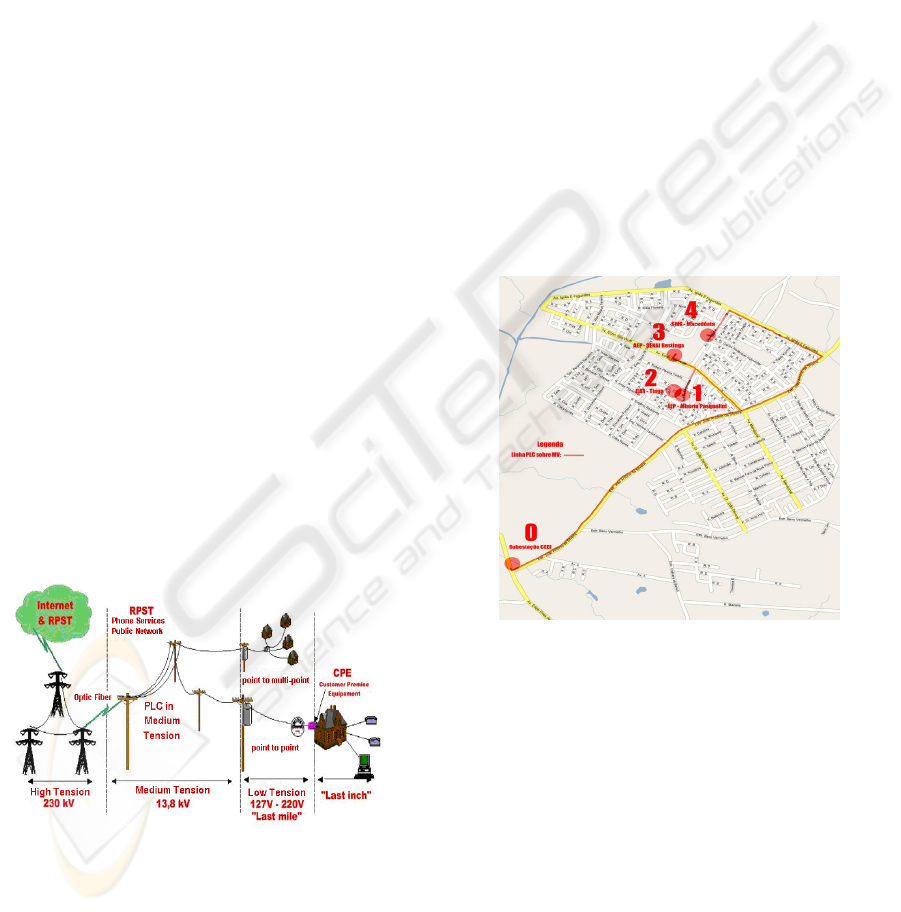
Figure 2: The PLC network at a whole.
With further technological details, we can
basically classify the segments of communication
networks via PLC in 4 areas, but the following 3
were used in our work (see Figure 2):
Medium Tension: interval between the electric
power company substation and the
transformer of low tension that serves the final
consumers;
Last Mile: interval of electric net in between
the transformer of low tension and the
consumer's residence;
Last Inch: interval of electric low tension net
located in the consumer's dependences.
Taking advantage of the fiber optic network from
the Information and Communication Technology
Company of Porto Alegre (Procempa), which is
interlinked to the optic ring from the State Company
of Electric Energy, a PLC network was deployed,
beginning from the substation, located in one of the
extremities of the Restinga neighborhood (point 0 in
Figure 3). In addition, four different points are
connected, chosen from its geographical position
and lack of digital services: (1) public primary
school; (2) district administrative center; (3)
professional primary school; (4) the previous cited
Resting health center.
Figure 3: PLC medium tension map at Restinga.
The pilot reaches a linear extension of
approximately 3.5 kilometers of PLC, transmitting
data in high-speed (45Mbps, since we use the first
generation of equipments) on the electric network of
energized medium tension (13.8 kV). The project
foresees several services, taking maximum
advantage of the communication speed. Thus, its
importance for telemedicine applications that needs
normally high bandwidth when dealing with
multimodal (large image/video data, voice, etc.) high
quality data.
The network implementation was only possible
due to the optic fiber channel located at the
substation (point 0), i.e., it is a hybrid network
topology and the PLC phase accomplishes the “red”
POA_S@UDE - A New Collaborative Tele-ultrasonography System over PLC
225
lines of the figure. At a glance, starting from this
point, the sign from the optic fiber is injected in the
medium tension net throughout capacitive couplers
and goes direct trough the electrical line, with
acceptable losses, in distances of up to 1200 meters,
where regenerators modems are installed aiming the
system sign losses reconstitution. Repeating
modems are also installed in these points to overlap
the maneuver keys and the derivations in the
medium tension net. In the extremities, special
modems are used and receive the PLC signal from
the medium tension and re-inject this signal in the
electric net of low tension (127V/220V). The signal
that arrives in the assisted points through the low
tension is extracted from the power plug using a
modem for low tension.
4 THE POA_S@UDE PLATFORM
Based on physician needs, the proposed system
should compromise with the following concerns:
• Good Ultrasound Video Quality: show
details in the ultrasonographies. This
demand is subjective and the adequate
quality is determined by the doctor when he
can distinguish the meaningful regions of
the fetus needed to perform the correct
diagnosis and taking responsibility for it;
• Perceptible Movements: should show
matters as mainly the fetus heartbeats and
the respiratory system. This demand is
also subjective and also determined by the
doctor;
• Audio Communication: between the
specialist doctor and the support resident
physician;
• Remote Pointer: the specialist doctor can
show details to the patient and the resident
physician (who is with the patient). It uses
its mouse inside the ultrasound area and the
mouse movements are send to the remote
place, showing specific areas which the
doctor wants more attention;
• Hand Probe Position: video showing the
hand of the remote resident physician,
which shows the transducer position on the
patient's abdomen.
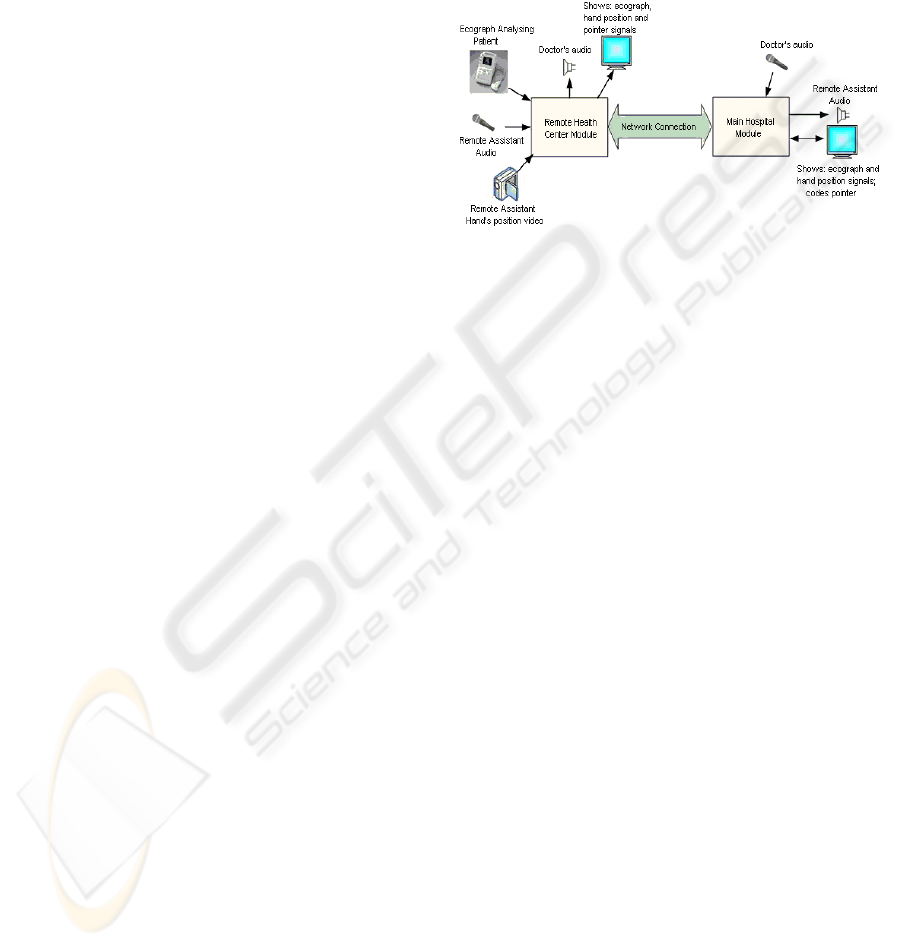
Figure 4 shows a schematic of the developed
solution. At both ends, there is audio coding and
transmission. In the remote module, the system
receives the video signal from the U/S and the hand
position of the attendant, composing both videos on
the same screen. The attendant hand is in PIP
(Picture in Picture) form, generating a small
resolution video. This signal is coded in MPEG-4
and transmitted live, being received by the doctor,
who analyses it and communicates by audio and
through the remote pointer, giving instructions.
Figure 4: System Overview.
The TeleConsult was used to capture the U/S
signal that is sent through the PLC hybrid network
from the remote health center to the referral hospital.
In our case, there is a non-specialist physician (a 4th
year resident) who performs the exam. At the main
hospital (HPV), the specialist doctor is responsible
to assist, guide, and interact with the non-specialist
in order to perform the final diagnosis.
The system internal structure, placed at the
health center, is shown on Figure 5. A short
description of each module is presented bellow:
• Capture: responsible for receiving the
audio and video signals generated by
external equipment, such as camera and
microphone, independent from the
communication interface (DV, acquisition
card or USB). In the specific case of tele-
ultrasonography system, the capture
module received four simultaneous
captures: a) the U/S video signal; b) the
video signal showing the attendant’s hand
position; c) the attendant audio; d) the
video monitor image;
• Audio and Video Coding: responsible for
compressing the audio and video streams,
captured for later transmission. The generic
interface allows working with different
coding algorithms. The available video
coding algorithms are MPEG-2, MPEG-4 e
H.264 protocols, and the audio coders are
G.711 and AAC (Advanced Audio Coding)
protocols. In this case, the coding was
HEALTHINF 2009 - International Conference on Health Informatics
226

compressing the audio and image from the
video monitor;
• Network: implements the point-to-point
communication between the local and the
remote locations.
• Audio and Pointer Decoder: decodes the
audio that comes from the main hospital, as
well as the pointer signal controlled by the
doctor;
• View: shows at the video monitor: a) small-
sized image of the attendant hand position;
b) large-sized ultrasound image; c) remote
pointer image, controlled by the doctor.
Besides that, it decodes the doctor's audio
and presents it on the speakers.
Figure 5: The remote health center system modules.
The system diagram placed at the referral
hospital is complementary to the previous one and
illustrated by Figure 6. The main differences are that
the system codes only audio and pointer. Besides,
decodes the remote audio and video, presenting
them on the computer screen.
Figure 6: The referral hospital system modules.
5 RESULTS
According to (LeRouge, 2002), any application
related to telemedicine with videoconference ought
to study the effectiveness of practical requirements
in order to reach the aimed system quality. To reach
the concern of quality for perceptible fetus
movements, some preliminary experiments were
performed on 2 CPUs (Dual core Pentium 3.4GHz, 2
GB RAM). The evaluated parameters were:
• Video compression using the codecs
MPEG-4 part 2, H.264 and MPEG-2;
• Resolutions of 720x480 and 320x240
pixels;
• 15, 20 and 30 frames per second;
• Bandwidth (bitrate) of 500 kbps, 1 Mbps,
1.5 Mbps and 2 Mbps;
• Audio AAC (Advanced Audio Coding) 64
kbps and 128 kbps.
The H.264 encoder produced good video quality,
but demanded high processing power from the
computers during video encoding process. Besides
that, it increased the total delay to around 1 second
and in some condition caused application freeze.
MPEG-2 and MPEG-4 encoders resulted small delay
(lower than 300 ms). MPEG-4 provided better video
quality compared to MPEG-2, being chosen.
Any resolution below 720x480 was considered
improper according to the specialist doctor, mainly
because of artifacts and pixel interpolation problems
detected in the reconstructed video, which could
invalidate a correct medical interpretation.
Some experiments changing the number of
frame per seconds were also performed in order to
define the better relation between frame rate and
visual movement video requirements. With 20
frames per second, the result was acceptable, but
was better using 30 frames per seconds. Regarding
audio, the tests showed to use the AAC codec with
128 kbps, providing a better audio quality.
The experiments were performed changing the
overall connection bitrate for audio and video, and
the system was tested with 500 kbps, 1 Mbps, 1.5
Mbps and 2 Mbps via PLC. The increasing of the
total multimedia (audio and video) bitrate produces
better quality; however, it is a limited resource. The
best cost-benefit was obtained using 1 Mbps, which
was the rate established to the system.
The mean transmission delay was measured with
the help of a clock, which was filmed while
transmitted, and the overall one-way delay was
about 300ms, meeting with communication needs
between doctors and being considered real-time
according to previous definition.
With these parameters, the case study could
accomplish the fetus movements and meet the
original need of verifying the heartbeats and
breathing movements.
POA_S@UDE - A New Collaborative Tele-ultrasonography System over PLC
227

Regarding the pilot at the remote health center,
about 40 monthly tele-ultrasonographies were made
during a 3-month pilot and the forecast is to increase
this number to 600 monthly exams, covering other
health centers spread over Porto Alegre. Figure 7
presents the environment at the remote health center,
where the resident physician positions the U/S probe
according to the doctor's remote guidance. Besides
that, it shows the U/S equipment (white, on the
table), the video monitor attached to the acquisition
computer (behind the U/S), and the video camera
that records the transducer and hand of the local
physician (behind the patient).
Figure 7: Exam being held at the remote health center.
Figure 8 presents the referral side, showing the
specialist doctor at the HPV watching the
transmission and guiding the resident physician
through audio and using his mouse pointer. From the
figure, it is possible to note the U/S screen as well as
the small image showing the hand position of the
remote physician. The doctor has also a "remote
pointer", which uses to show regions of interest
commenting by audio.
Figure 8: Remote attendance by the specialist doctor.
During the first month of use, 40 patients were
interviewed to collect subjective opinions about their
experience. The major advantages mentioned were
related to being close to home and the decrease of
waiting time to perform the exam (from the original
4 months to actual 1 month). However, this time
should decrease, since the statistics considers a
number of exams requested before the system started
working, i.e., there is a repressed demand which is
being minimized at each new exam session at the
remote health center.
In addition, the patients reported that did not feel
the attendance was impersonal for the fact of
interacting also with a doctor located in another
place. It is also interesting to mention that the
consultations identified, up to now, four cases that
required immediate treatment and patient transfer
due to bad fetus formation, i.e., it was detected
preventively and the forwarding could be well
planned.
6 CONCLUSIONS
This paper presented a new tele-U/S system being
used not just as pilot project, but it is in continuous
use as a pilot service. It connects a poor, distant, and
very populated district with a referral hospital
located at the city via a hybrid PLC network. The
platform was developed by a multidisciplinary team
and was submitted to several technological and
medical experiments. Final results pointed to the use
of MPEG-4 video codec, AAC audio codec, and
resolution of 720x480 pixels to achieve the real-time
interaction of 30 frames per second. The obtained
delay was 300ms, which is better than the 400ms of
worst case in the standard of IP videoconferences.
The directly benefited by POA_S@UDE can
be sorted in two groups: pregnant patients residing
in the peripheral areas of Porto Alegre, i.e., Restinga
up to now; and non-specialist or resident physicians,
who act in health centers distant from the central
area. The benefit for the first group is the reduction
of the absences in prenatal exams and the
consequent early diagnosis of pregnancy problems.
The second group is benefited by the training and
constant contact with the specialist doctors from the
reference center.
It is important to mention that the number of
patients who submitted to the prenatal obstetric
exams through the new telemedicine system is still
small. However, all the patients who already made
the U/S examinations via the platform manifested
their contentment about being able to perform the
HEALTHINF 2009 - International Conference on Health Informatics
228

prenatal exams close to their homes, saving transport
and being able even to take their other children to
the health center. Even more important, the spatial
distribution of the exams reduced their waiting time
(from 4 months to 1 month) and could now
accomplish with the WHO recommendation of 4
medical visits over the pregnancy time. According to
the Porto Alegre Health Ministry statistics, this will
guarantee an increase at the average
ultrasonographies per pregnancy that today, at
Restinga, is between 0 and 1, to at least 3 or 4, until
the end of 2008.
As future directions, the telemedicine service is
expected to be deployed in other neighborhoods or
regions distant from the downtown, such as the
regions of Guaíba Islands and Lomba do Pinheiro. A
"mobile unit" will be equipped with the system,
which will be connected to HPV through network
points at the health care centers of the covered
regions. The unit will be able to transport a resident
physician and a computer technician and each new
health care center is planned to be attended in one
day of the week, reducing the system costs.
ACKNOWLEDGEMENTS
We would like to thank Porto Alegre City Hall at a
glance, HPV and Restinga health center physicians,
and CEEE (State Company of Electric Energy).
REFERENCES
Bartoli, I., Iacovoni, G., Ubaldi, F., 2007. A
Synchronization Control Scheme for Videoconferencing
Services. In Journal of Multimedia, v.2.
Borges, A. A., 2005. Tecnologia PLC. In
http://www.teleco.com.br/emdebate/aderbal01.asp.
Access in November 2006.
Chan, F.Y. et al., 2000. Clinical value of realtime tertiary
fetal ultrasound consultation by telemedicine. Telemed
Journal, v.6, pp.237–242.
Ferrer-Roca, O., Vilarchao-Cavia, J., Troyano-Luque, J.
M., Clavijo, M., 2001. Virtual Sonography through the
Internet: volume compression issues. In Journal of
Medical Internet Research.
http://www.jmir.org/2001/2/e21/.
Kontaxakis, G., Walter, S., Sakas, G., 2000. EU-
TeleInViVo: an integrated portable telemedicine
workstation featuring acquisition, processing and
transmission over low-bandwidth lines of 3D
ultrasound volume images. In Proceedings of IEEE
EMBS International Conference, pp. 158 – 163.
LeRouge, C., Garfield, M. J., Hevner, A. R., 2002. Quality
Attributes in Telemedicine Video Conferencing. In
Proceedings of the 35th Hawaii International
Conference on System Sciences, pp. 1435-1439.
Opera, 2007. Open PLC European Research Alliance. In
http://www.ist-opera.org. Access in May 2007.
Reddy, E. R., Bartlett, J. P., Harnett, J. D.M.,
McManamon, P. J., Snelgrove, C., 2000. Telemedicine
and fetal ultrasonography in a remote Newfoundland
community. In the CMAJ Journal, v.2, n.162, pp.206–
207.
RUTE, 2008. In http://www.rute.rnp.br. Access in June
2008.
Sakas, G., 1993. Interactive volume rendering of large
fields. In Visual Computing, n.9, v.8, p.425-438.
Sakas, G., Walter, S., Grimm, M., Richtscheid, M., 2000.
Free hand acquisition, reconstruction and visualization
of 3D and 4D ultrasound. In Radiologe, v40, p.295-
303.
Sibert, K. et al., 2008. The Feasibility of Using Ultrasound
and Video Laryngoscopy in a Mobile Telemedicine
Consult. In Telemedicine and e-Health Journal, v.3,
n.14, pp.266-272.
Simoes, N., Coury, W., Ribeiro Filho, J. L., Messina, L.
A., 2006. RUTE – Tele-Medicine University Network.
In Tele-Health – Permanent Social and Educational
Support, UFMG Press.
T@lemed, 2007. In http://www.alis-telemed.net. Access in
June 2007.
Yee, C. F., Soong, B., 2005. Telemedicine in Advanced
Fetal Diagnosis and Therapy. In Telepediatrics:
Telemedicine and child health, RSM Press, p.345.
WHO, 2008. In
http://www.euro.who.int/HEN/Syntheses/antenatal/20
031223_2. Access in June 2008.
POA_S@UDE - A New Collaborative Tele-ultrasonography System over PLC
229
