
TOWARDS AN AUTOMATED NOSOCOMIAL INFECTION
CASE REPORTING
Framework to Build a Computer-aided Detection of Nosocomial Infection
Jimison Iavindrasana, Gilles Cohen, Adrien Depeursinge
Medical Informatics Department, University and Hospitals of Geneva, rue Micheli-du-Crest, 24, Geneva, Switzerland
Henning Müeller
Medical Informatics Department, University and Hospitals of Geneva, rue Micheli-du-Crest, 24, Geneva, Switzerland
University of Applied Sciences Western Switzerland, Sierre, Switzerland
Rodolphe Meyer, Antoine Geissbuhler
Medical Informatics Department, University and Hospitals of Geneva, rue Micheli-du-Crest, 24, Geneva, Switzerland
Keywords: Nosocomial infection, Machine learning, Feature selection, Fisher's linear discriminant.
Abstract: The prevalence survey is a valid and realistic surveillance strategy for nosocomial infection surveillance but
it is resource and labor-consuming. Querying the hospital data warehouse with a set of relevant features and
applying a classification algorithm on the results can reduce the amount of cases to be evaluated by the
infection control practitioners. The objective of this work is to provide a framework to build a nosocomial
infection model with a set of pre-selected features with Fisher’s linear discriminant algorithm. Application
of the methodology to two datasets provides promising results. It permits to predict respectively an average
of 41.5% and 43.54% positive cases including respectively 65.37% and 82.56% true positive cases. The
proposed framework can be applied to other classification algorithms, which are planned as future work.
1 INTRODUCTION
1.1 Context
Nosocomial infections (NI) are infections acquired
in a hospital. In Switzerland, 70000 hospitalized
patients per year are infected and 2000 deaths per
year are caused by NI. A hospital aware of the
quality of the patient care should have an infection
prevention, control and surveillance program. The
surveillance is the process of detecting these
infections. Prevalence surveys are recognized as
valid and realistic approaches of nosocomial
infection (NI) surveillance strategies (French et al,
1983). Prevalence of NI is presented as prevalence
of infected patients, defined as the number of
infected patients divided by the total number of
patients hospitalized at the time of study, and
prevalence of infections, defined as the number of
NIs divided by the total number of patients
hospitalized at the time of study (Sax et al, 2002).
However, a prevalence survey is resource and labor-
consuming, as it requires assembling a wide range of
data gathered from multiple sources. The medical
record of all patients hospitalized for more than 48
hours at the time of the survey are reviewed by
infection control practitioners. During this first
process they extract information related to each
patient and store them in a database specially
developed for this purpose. The prevalence database
contains 83 attributes ranging from administrative
information, demographic characteristics, admission
diagnoses, comorbidities and severity of illness
scores, type of admission, and exposure to various
risks of infection, clinical and paraclinical
information, and data related to infection when
present. This database is analyzed to sort out the
prevalence official report.
The hospital data warehouse contains all the data
in the operational system except the data of the day.
Querying the hospital data warehouse and apply data
mining techniques in order to report “potential
cases” to be reviewed by the infection control
317
Iavindrasana J., Cohen G., Depeursinge A., Müeller H., Meyer R. and Geissbuhler A. (2009).
TOWARDS AN AUTOMATED NOSOCOMIAL INFECTION CASE REPORTING - Framework to Build a Computer-aided Detection of Nosocomial
Infection .
In Proceedings of the International Conference on Health Informatics, pages 317-322
DOI: 10.5220/0001553103170322
Copyright
c
SciTePress

practitioners will reduce their workload and will
allow them to focus on the content of the patient
record and evaluate the presence of NI.
Some of the 83 attributes of the prevalence
database are acquired for administrative purposes
only. The majority of these attributes are the
synthesis of information from the patient records
emanating from laboratory, radiology, nursing, and
clinical databases. A more realistic approach to
report potential cases is to find a subset of N most
relevant features (N<83) and query the hospital
databases on the basis of these N features. The
results obtained are then classified and ranked with a
classification algorithm, and only predicted positive
cases i.e. lists of infected patients are reviewed by
the infection control practitioners. The classification
is based on a model build with the N features.
We present in this paper a framework to build a
computer-aided detection of NI based on a set of N
pre-selected features using Fisher’s linear
discriminant algorithm. For this purpose, we analyze
a previous prevalence database to optimize the
classification process. The retrieval of the data from
the hospital data warehouse is not presented in this
paper. The Fisher’s linear discriminant (FLD) was
chosen for its “simplicity” as it only has one
parameter to optimize. One challenging
characteristic of NI prevalence data is the imbalance
between the positive and negative cases
(respectively 11% and 89%) (Cohen et al, 2006).
This important characteristic is taken into account in
the proposed methodology. An application is
developed to automate all the process.
1.2 NI Prevalence Data
The prevalence data we analyzed in this work is data
collected at the hospitals during the 2006 survey.
The dataset contains 5 data categories: 1)
demographic information, 2) admission diagnosis
(classified according to McCabe5 (McCabe and
Jackson, 1962) and the Charlson index (Charlson et
al, 1987) classifications); 3) patient information at
the study date (ward type and name, status of
Methicillin-Resistant Staphylococcus Aureus
portage, etc); 4) information at the study date and
the 6 days before (clinical data, central venous
catheter carriage, workload, infection status, etc) and
5) those related to the infections i.e. for infected
patients (infection type, clinical data, etc.).
In this study, we are interested in the 4 first
categories of data as they are related to patient
infection, which comprises 45 attributes. Most of
these data are categorical except for date information
(year of birth, admission date and study date) and
the workload value. The dataset contains 1573 cases.
The year of birth was converted into age and
discretized into 3 categories (0-60; 60-75; >75) as in
(Sax et al, 2002), and a new variable “hospitalization
duration” was created. A Mann-Whitney-Wilcoxon
statistical test on the workload value provides a
significant difference between infected and non-
infected patients. As it is the unique attribute having
missing values (91 cases including 2 positive cases),
all cases having no workload value were removed.
The latter and the hospitalization duration were
discretized afterwards using the minimum
description length principle (Kononenko, 1995).
Patients admitted for less than 48 hours at the time
of the study and not transferred from another
hospital were also removed. The final dataset
contains 1384 cases containing 166 positive cases
(11.99%). Let us denote this dataset S.
The ratio of positive cases in the dataset S is very
low compared to the negative ones. The class
imbalance is an important issue in machine learning
since the class of interest is represented with a small
number of examples (Japkowicz and Stephen, 2002).
In the presence of imbalanced datasets, classification
algorithms tend to classify the larger class accurately
while generating more errors in the minority class. If
a positive class has a ratio of 10%, a classification
accuracy of 90% may be meaningless if the
classification is not sensitive at all.
The class imbalance problem induces specific
approaches to train classifiers and evaluate their
performance. Two approaches were proposed to deal
with the class imbalance problem in (Cohen et al,
2006, Estabrooks, 2004). The first one is to modify
the classification algorithm or at least use an
algorithm able to deal with imbalanced data. The
second resamples the data to reduce the imbalance
effect. The latter has the advantage of being
independent of any classification algorithm.
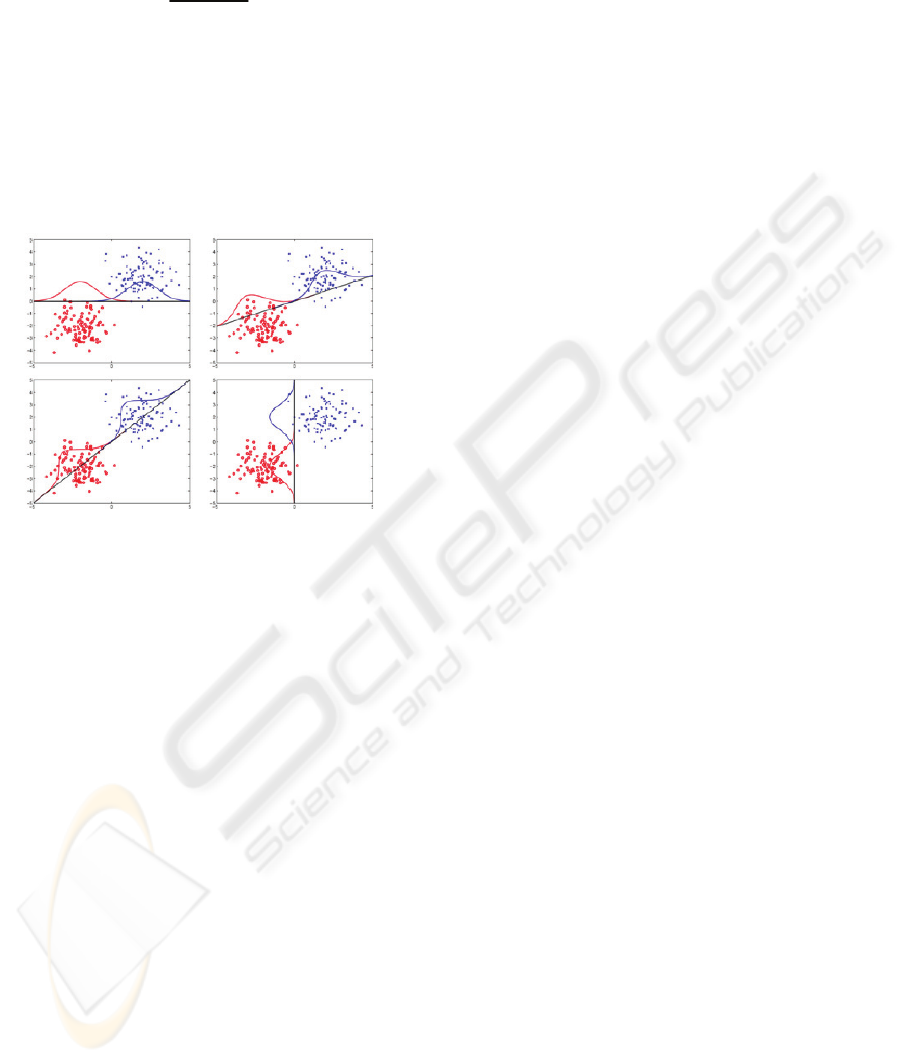
1.3 Fisher’s Linear Discriminant
The basic idea behind linear discriminant algorithms
is to find a linear function providing the best
separation of instances from 2 classes. Fisher’s
linear discriminant is looking for a hyperplane
directed by w, which (i) maximizes the distance
between the mean of the classes when projected on
the line directed by w and (ii) minimizes the
variance around these means (Fisher, 1936). An
illustration of this algorithm is highlighted on the
figure below (Figure 1).
HEALTHINF 2009 - International Conference on Health Informatics
318
Formally, Fisher’s linear discriminant aims at
maximizing the function:
T
B
T
W
wSw
J(w)
wS w
=
(1)
where S
B
is the scatter matrix between classes and
S
W
the scatter matrix within classes. This equation
permits to formulate Fisher’s linear discriminant as
an algorithm aiming at minimizing the variance
within the classes and maximizing the variance
between classes. An unknown case will be classified
into the nearest class centroid when projected onto a
hyperplane directed by w.
Figure 1: Illustration of Fisher’s linear discriminant. The
algorithm is looking for the direction providing the best
separation of the classes when projected upon. In this
figure, the third image (bottom left) provides the best
separation of the datasets.
In a classification task, an object is member of
exactly one class and an error occurs if the object is
classified into the wrong one. The objective is then
to minimize the misclassification rate. With Fisher’s
linear discriminant algorithm, the scatter matrix
within classes SW is evaluated on the training
datasets. To minimize the misclassification rate on
unseen test sets (generalization error), a
regularization factor r (0 ≤ r ≤ 1) is introduced into
the computation of S
W
(Hastie et al, 2001). The
regularization factor r has to be optimized to
minimize the misclassification error.
2 MATERIAL AND METHODS
The attributes from the dataset S were ranked
according to the information gain. Afterwards, a
Chi-square statistic test was applied to filter the
discriminative features to be retained for an
evaluation with the classification algorithm. Let us
denote S1 the new dataset created with this feature
selection. The dataset S1 may contain attributes
which are not always documented or at least not
documented in a machine readable format in the
clinical database. We will remove them from the
dataset S1 to obtain a second dataset S2.
We have taken the two datasets S1 and S2
described above to evaluate the discriminative
power of the selected features. For classification
purposes, we use the open-source toolbox
MATLABArsenal. This MATLAB package contains
many classification algorithms and in particular the
regularized Fisher linear discriminant algorithm as
described above. The MATLAB software is invoked
from the java application developed for the process
automation. This application also uses the WEKA
api for other routine tasks such as the training/testing
set splitting.
The evaluation of the predictive power of the
selected features is inspired by the experimental
setup described in (Rätsch et al, 2001). One hundred
(100) partitions of training and testing sets were
generated with the data source S1 and S2 having
respectively a ratio of 60% and 40%. The original
data distribution is kept in both partitions. A grid
search algorithm is then applied to the first five
under-sampled training sets using a 5-folds cross-
validation to find the best parameters of the
classification algorithm. In the five under-sampled
training sets, the classes are equally distributed (50%
positive cases and 50% negative cases).
The regularization factor r takes 41 values from 2-20
to 220 during this process. The best parameter of
each training set was the one providing the highest
recall (i.e. the parameter permitting to predict
highest rate of true positive cases). The best value
selected for the classification algorithm is the
median of the 5 best parameters. The 100 training
sets (having the original class distribution) are then
used to train Fisher’s linear discriminant models
with this best parameter. This process allows us to
build 100 models and to validate each of them on the
corresponding testing set. The general performance
of the classifier is computed as the mean of the 100
classification performances on the test sets. The
performance of the classification algorithm with the
2 datasets (S1 and S2) is also compared with respect
to the Mann-Whitney-Wilcoxon statistical test.
TOWARDS AN AUTOMATED NOSOCOMIAL INFECTION CASE REPORTING - Framework to Build a
Computer-aided Detection of Nosocomial Infection
319

Table 1: List and rank of features obtained with information gain followed by a Chi-square filtering. The first column
provides the rank of each attributes.
Rank Selected attributes
1
Antibiotic therapy
2
Fever
3
Mechanical ventilation
4
Urinary tract
5
Workload value > 91.5
6
Workload value <=45.5
7
Stay at the intensive care unit during hospitalization
8
Central vein catheter
9
Hospitalization duration up to 7.5 days
10
Intensive care unit ward
11
Obstetrical ward
12
Surgery
13
McCabe score fatal < 6 months
14
No MRSA colonization
15
Actual MRSA colonization
16
McCabe score non fatal
17
Workload value between 45.5 and 91.5
18
Diabetes with organ affected
19
Transfer from another hospital as admission
20
Congestive cardiomiopathy
Figure 2: The mean of each performance measure on the datasets S1 and S2.
HEALTHINF 2009 - International Conference on Health Informatics
320

3 RESULTS
3.1 Feature Selection
Twenty (20) attributes were retained from the
feature selection process as summarized in the table
1. Let S1 denote the name of this subset. Two (2)
clinical attributes are not always documented or at
least not documented in a machine readable format
in the clinical database: fever and workload value.
These attributes were removed to create a second
data source denoted S2 even if the information gain
ranked these attributes at the fourth and sixth
position.
3.2 Model Selection
The grid search algorithm applied on the two
datasets S1 and S2 returned respectively r =0.5 and 1
as the best parameter. The figure 2 summarizes the
performance metrics (accuracy, precision, recall, f-
measure and the ratio of positive predictions)
obtained with the 2 datasets in terms of their mean.
3.3 Classification Performances
Dataset S1 and S2 permit to obtain respectively a
mean recall (±standard deviation) of 65.37% (±6.76)
and 82.56 (±4.22), a precision (±SD) of 41.50%
(±3.9) and 43.54% (±4.59), a f-measure (±SD) of
50.58(±3.83) and 56.87(±4.29) over the 100
training/testing split realizations. The mean accuracy
(±SD) for S1 and S2 are 84.83%(±1.04) and
85.04%(±1.65) and the positive prediction ratios are
respectively 18.82% (±1.72) and 22.73% (±1.55).
According to the results above, querying the
hospital data warehouse with the features present in
the dataset S1 and S2 and classify the results with
the FLD algorithm, we can expect retrieving an
average of (±SD) 65.37% (±6.76) and 82.56 (±4.22)
of the infected patients. The mean numbers of
potential cases (±SD) to be submitted to the ICP are
respectively 18.82% (±1.72) and 22.73% (±1.55) of
the hospitalized patients.
A Mann-Whitney-Wilcoxon statistic test
provided a p value < 0.001 for accuracy, precision,
f-measures and the positive prediction ratio.
According to this test, there is a statistically
significant difference between the accuracy,
precision, f-measure and the ratio of positive
prediction. The removal of the temperature and the
workload features improved significantly the
performance of the FLD.
4 DISCUSSION AND
CONCLUSIONS
In this paper we present a framework to build a NI
model based on a small number of clinical features
permitting to report NI cases to be reviewed by
infection control practitioners. Fisher’s linear
discriminant was chosen as detection algorithm. The
removal of the attributes characterizing fever and
workload value is not affecting the sensitivity of the
classifier. This may be explained by the strong
correlation between these attributes with some
important features such as the antibiotherapy for the
fever and surgery, stay at the intensive care unit
during the hospitalization, a presence of artificial
ventilation, urinary tract, and central venous catheter
for the workvalue. The automation of the process
needs integration of data from laboratory, radiology,
nursing, and clinical databases.
Limits of this Work. The evaluation of the
discriminative power of the selected features was
carried out using Fisher’s linear discriminant
algorithm. A comparison with other classification
algorithms such as Support Vector Machines (SVM)
and the Kernel Fisher’s linear discriminant could be
a good option to improve the classification
performance. The framework could also be extended
with an evaluation of the best classifiers. The grid
search algorithm for optimal parameters has high
computational cost especially for classification
algorithms with more than one parameter to
optimize such as SVMs of the Kernel Fisher
discriminant. A gradient descent method can be used
to find the best parameter and can improve the
generalization performance as described in
(Chapelle et al, 2002).
Future Work. The framework introduced in this
paper permits to evaluate the discriminative power
of a subset of important features from the NI
database. The feature selection method we have
chosen in this work is based on the information gain
combined with a Chi-square statistic test. More
experiments with other feature selection techniques
are required (Guyon, 2003). The discriminative
power of the selected features will be evaluated with
more than one classification algorithm. The result of
these evaluations i.e. the minimal attributes required
to predict most of the positive NI cases will be
retained to build queries for the hospital databases in
order to automatically report potential cases for the
prevalence surveys. This automated nosocomial
TOWARDS AN AUTOMATED NOSOCOMIAL INFECTION CASE REPORTING - Framework to Build a
Computer-aided Detection of Nosocomial Infection
321

infection reporting will permit to conduct more
prevalence surveys with less cost.
ACKNOWLEDGEMENTS
The authors are grateful for the dataset provided by
the infection control team at the Geneva University
Hospital.
REFERENCES
Chapelle, O, Vapnik, V, Bousquet, O, Mukherjee, S, 2002.
Choosing multiple parameters for support vector
machines. Mach. Learning.
Charlson, ME, Pompei, P, Ales, KL, MacKenzie, CR,
1987. A new method of classifying prognostic
comorbidity in longitudinal studies: development and
validation. J Chronic Dis.
Cohen, G, Hilario, M, Sax, H, Hugonnet, S, Geissbuhler,
A, 2006. Learning from imbalanced data in
surveillance of nosocomial infection. Artificial
Intelligence in Medicine.
Estabrooks, A, 2004. A multiple resampling method for
learning from imbalanced datasets. Comput Intell.
Fisher, RA, 1936. The use of multiple measurements in
taxonomic problems. Annals of Eugenics.
French, GG, Cheng, AF, Wong, SL, Donnan, S, 1983.
Repeated prevalence surveys for monitoring
effectiveness of hospital infection control. Lancet.
Guyon, I, Elisseeff, A, 2003. An Introduction to variable
and feature selection. Mach. Learning Res J.
Hastie, T, Tibshirani, R, Friedman, J, 2001. The elements
of statistical learning: data mining, inference, and
prediction. Springer.
Japkowicz, N, Stephen, S, 2002. The class imbalance
problem: a systematic study. Intell Data Anal J.
Kononenko, I, 1995. On biases in estimating multi-valued
attributes. Eds.: Morgan Kaufmann. In Proceedings of
the 14th International Joint Conference on Artificial
Intelligence.
McCabe, WR, Jackson, GG, 1962. Gram-negative
bacteremia, I: etiology and ecology. Arch Intern Med.
Rätsch, G, Onoda, T, Müller, KR, 2001. Soft margin for
AdaBoost. Mach.Learning.
Sax, H, Pittet, D, 2002. Swiss-NOSO Network.
Interhospital Differences in nosocomial infection
rates: importance of case-mix adjustment. Arch Intern
Med.
HEALTHINF 2009 - International Conference on Health Informatics
322
