ICT SUPPORTED COMMUNICATION IN HEALTHCARE
Benefits and Risks
Herman Lodder and Bertie Zwetsloot-Schonk
Clinical Informatics, Leiden University Medical Center, The Netherlands
Keywords: Communication, Semantic interoperability, Decoupling, Electronic health record, Context.
Abstract: Supporting communication in healthcare by ICT enables actors (healthcare professionals and patients) to
“decouple” on the place/time context of the communication process. On the one hand decoupling makes a
more flexible and efficient organization of care processes possible, on the other hand it imposes
preconditions to a number of features of the communication process and also to the standards being adopted.
1 INTRODUCTION
Communication plays a crucial role in healthcare. A
health professional is communicating about 60% of
his working day (Coiera, 2000), not only to share
data with colleagues but also to inform the patient
about his illness, ordering diagnostic tests and to
coordinate different activities. In an ideal situation
all caregivers would be standing around the bed of
one patient at the same time with all data at hand,
with no external interrupts, all contacts being face-
to-face, and a patient answering all upcoming
questions. Daily practice shows a complete other
picture in which communication in healthcare is
highly interruptive, often asynchronic, using a
variety of messages, languages, media and coding
systems, and has to deal with incomplete
documentation distributed over different sources.
And due to more co morbidity, more fragmentation
of care, more part-time workers, but also patients
who want to be more informed and involved, the so-
called ‘communication space’ will grow even more.
The examples from literature showing that
communication errors are the main lead cause for
unintended harm and errors within hospitals are
numerous.
Because the quality of healthcare delivery is
highly determined by the efficiency and
effectiveness of the underlying communication
process, we have to improve that communication
process in order to keep the quality of healthcare at
an acceptable level. In this paper, we describe how
ICT can and should be used as means to improve the
communication in healthcare.
2 ANALYSIS OF THE
COMMUNICATION PROCESS
Decomposition of the communication process into
its constituting components can reveal the features
that characterize the communication process.
social context
task/joint activity
C - process
Message
exchange
C - session
content structure
focus magnitude
capacity
interactivity
simultaneity
evanescence
Message
Medium
Partici-
pants
knowledge role
goal time/place context
Te’eni (2001)
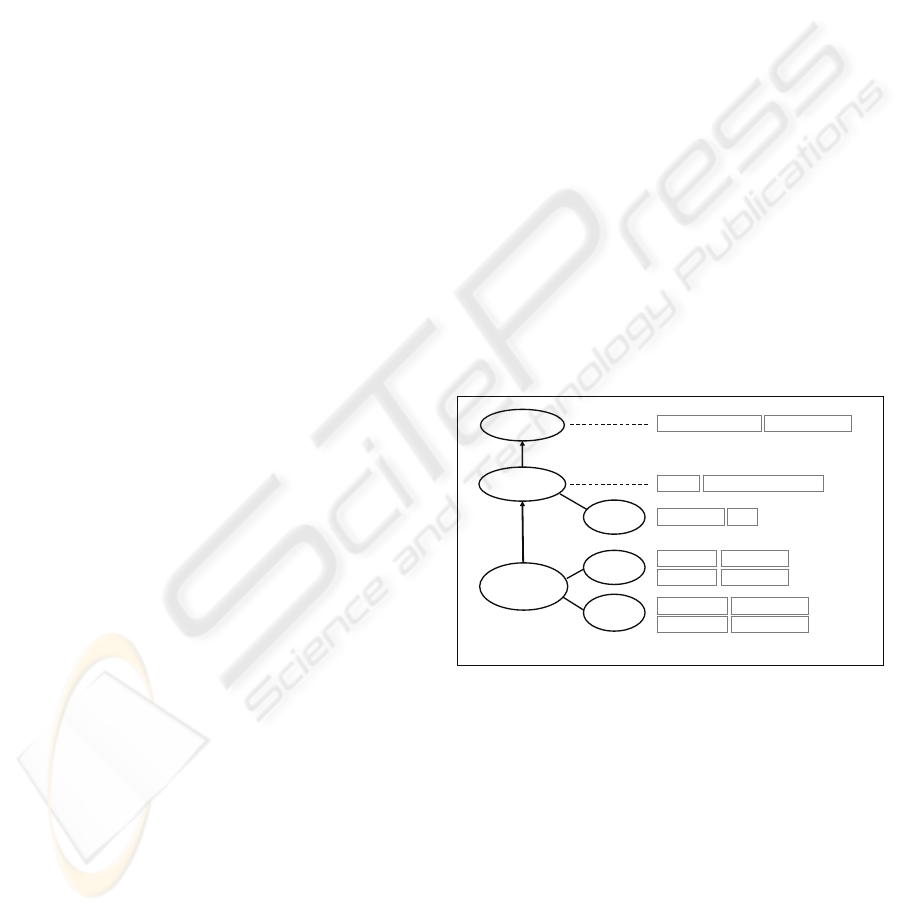
Figure 1: Decomposition of a communication process into
its constituting components and their features.
According to the theoretical communication
framework (Te’eni, 2001), a communication process
can be decomposed into one or more sessions.
Within each session one or more messages are
exchanged between participants using a medium.
Each of the component-levels can be characterized
by a number of features (see figure 1). For example,
a communication session has a specific goal and
takes place within a specific time/place context, and
a message can be defined by its structure, content,
focus and magnitude. And because of the partitive
relation between the components a message is
495
Lodder H. and Zwetsloot-Schonk B. (2009).
ICT SUPPORTED COMMUNICATION IN HEALTHCARE - Benefits and Risks .
In Proceedings of the International Conference on Health Informatics, pages 495-498
DOI: 10.5220/0001776404950498
Copyright
c
SciTePress
always exchanged within the context of a session’s
goal and time/place context between participants
having a specific cognitive distance and (emotional)
relation. This also implies that changing a feature of
a component will have impact to one or more
features of the underlying component(s).
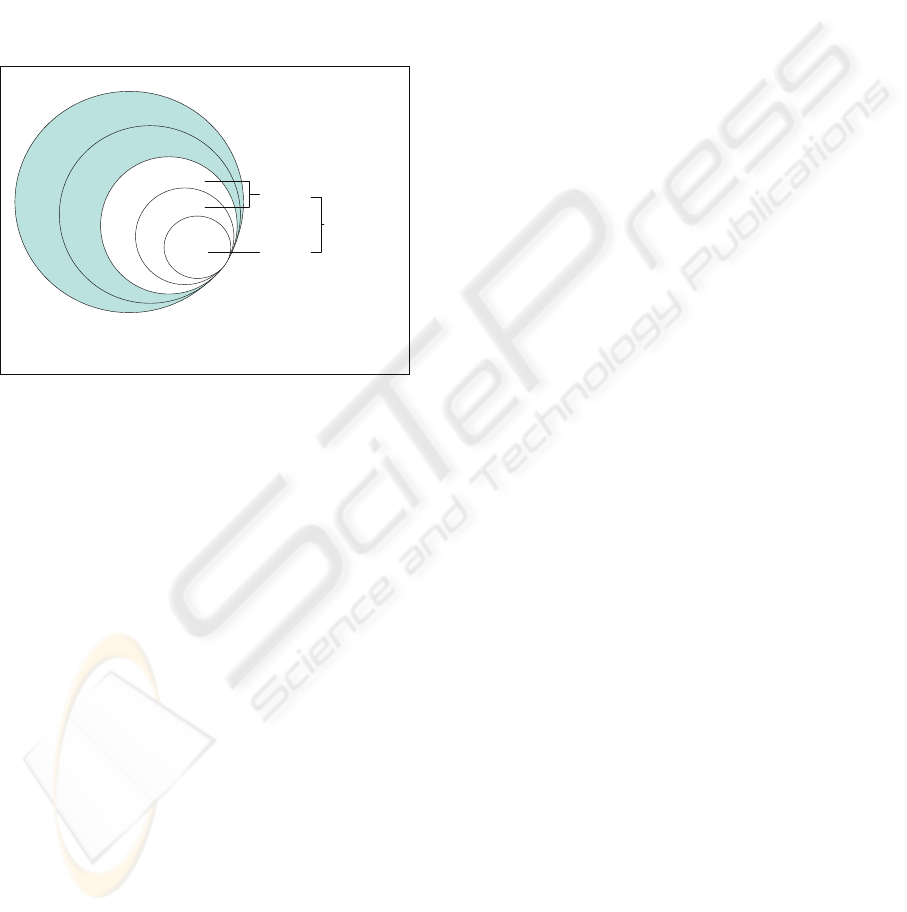
Another way to show that communication always
functions within a context - or in other words that
communication can only be understood in relation to
the context in which it is used – is by using co-
tangential circles (Halliday and Martin, 1993). In
this representation each circle can be seen as
realisation of the outer circle(s), see figure 2.
Communication in context
After: Halliday & Martin, 1993
Context of Domain
Context of Situation
Semantics
Structure
Expression
Content
Channel
Communi-
cation
Figure 2: Communication in relation to its context.
By taking the clinical domain as an example, the
context of domain includes the ‘medical language’,
the ‘clinical setting’, the way of medical reasoning,
etc. For the medical research domain the context of
domain will include knowledge of design and
analysis of e.g. Randomized Control Trials, together
with the medical language and epidemiology.
Within any context of situation – comparable to
the session component in the Te’eni model – one can
distinguish three variables that largely determine the
communication choices to be made. These variables,
just like the features in the Te’eni model, refer to:
the time-place context, who is taking part and in
what role, and the goal of the communication.
In the next section we will introduce ICT as an
intervention to the communication process and we
will look for the effects of this intervention on a
number of communication process features.
3 ICT SUPPORTED
COMMUNICATION
The introduction of ICT enables participants of a
communication session to ‘decouple’ on time/place
context in a very flexible way. In other words, the
participants can choose for: same time/same place,
same time/other place, other time/same place, or
other time/other place. Note that decoupling can also
be realised by using the traditional letter.
3.1 Benefits and Risks
The main benefit of decoupling is that participants in
a joint activity become less interdependent, which
enables them to organize their part of the joint
activity more efficiently. In literature there are
several examples of reorganizations of care
processes that were facilitated by a more efficient
organisation of the communication process, e.g. in
(Toussaint, 2004). Apart from the benefits to be
gained with respect to more efficient
communication, decoupling also implies loosing
context which can lead to misunderstanding and a
possible decrease of the effectiveness of the joint
activity. Because a message can only be interpreted
correctly by knowing the original context, we must
be aware that any loss of context has to be repaired
somehow. In this reparation process, ICT can also
play a crucial role, as can be illustrated by the
following projects carried out by our group:
SeniorGezond project
A website has been developed for elderly to inform
them about risks and prevention of fall incidences.
The effectiveness of the communication is shown to
improve significantly by providing extra contextual
information depending on the cognitive distance (i.e.
the difference in knowledge between the user and
the website) (Alpay, 2007).
SuperAssist project:
Electronic personal assistants supporting distributed
supervision of complex task environments are being
developed. With respect to the support of
communication personal assistants are able to filter,
provide and enrich information, and can even
express emphatic behaviour (Blanson Henkemans,
2008).
RAP project:
The effectiveness of the interdisciplinary team
conferences at the Rheumatologic Rehabilitation
Clinic in LUMC improved significantly by
introducing ICT for decoupling on time/place
context for the information session. For
optimalisation reasons both message structure and
content (registration of more structured information
items) had to be adjusted (Verhoef, 2007).
In the next two sections we will elaborate on two
scenarios by describing both the benefits and the
HEALTHINF 2009 - International Conference on Health Informatics
496
risks of applying decoupling by ICT. For both
scenarios a suggestion is made how to repair
possible negative effects on other communication
features.
3.2 Scenario 1: e-Consult
The electronic consult or e-Consult can be regarded
as an additional way of communicating between a
patient and his physician alongside the regular face-
to-face consultation. By decoupling on time/place
context the patient can ask questions that were not
addressed during the normal consultation or ask for
extra explanation or details for treatment, while the
general practitioner can reply to patient questions
outside the hectic office-hours.
Despite of these advantages, the e-Consult is still
offered by a minority of primary care doctors.
Literature (van Gemert, 2006) shows that for most
general practitioners the disadvantages of
introducing the e-Consult clearly outrange the
advantages (see table 1).
General practitioners mainly regard the e-
Consult as a replacement for the consult by
telephone and not as a contribution to a better
quality of healthcare. This will probably be the
reason that one of the main negative effects of
decoupling on time/place context - i.e. the lack of
personal contact – is mentioned only after arguments
regarding higher workload and incompatibility with
the information system. A closer look at the effects
of decoupling gives support to the opinion that an e-
Consult is a replacement for a consult by telephone
rather than a substitute for a regular face-to-face
consult.
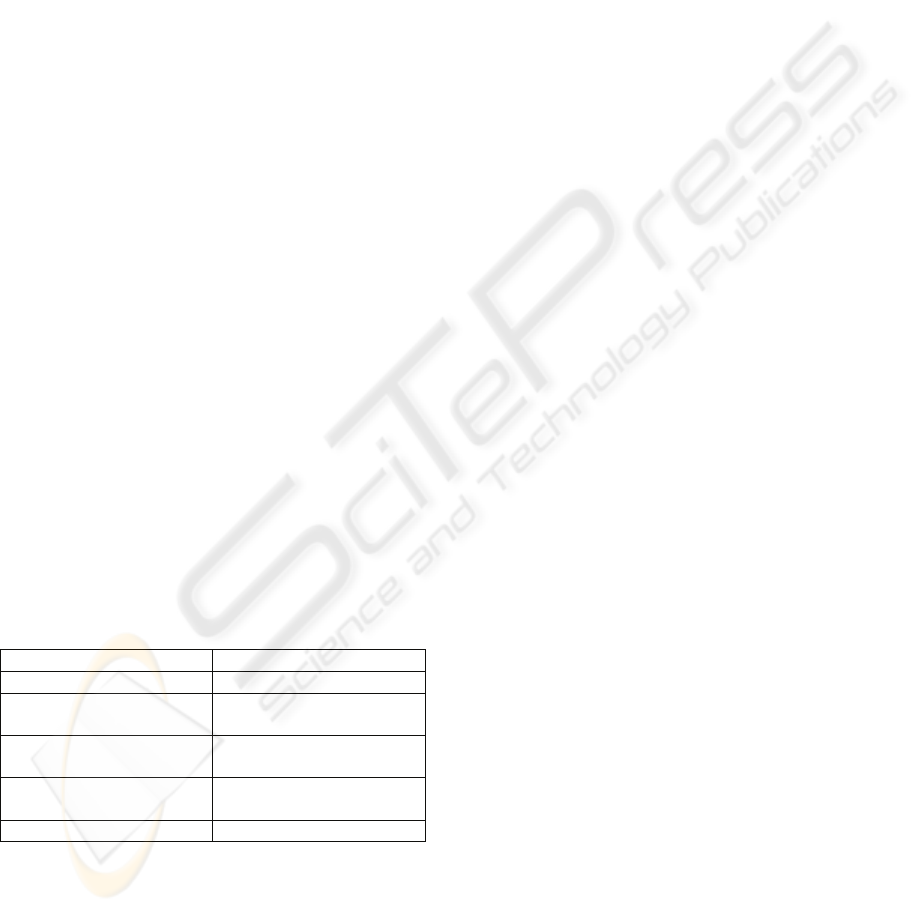
Table 1: Advantages and disadvantages of using the e-
Consult (questionnaire filled in by 654 Dutch general
practitioners).
Advantages Disadvantages
Meeting the patients wishes Higher workload
Outside office hours No reduction of regular
consultations
Reduction of number of
consults by telephone
No financial compensation
Incompatibility with the
Information system
Lack of personal contact
Decoupling on time-place context directly has
effect on other features of the communication
process and in particular the message exchange
component. Compared to the face-to-face consult,
the interactivity will decrease, the structure of the
content will increase, the capacity of the medium
(i.e. the number of supported modalities) will
decrease and the evanescence will become low.
Because modifications of features such as
interactivity and capacity - that are essential for a
regular consult – cannot be repaired, an e-Consult
will never be a good replacement for a regular
consult. A related consequence is that the use of e-
Consults is only limited to non-urgent
communication and between actors already having
an established patient-doctor relation.
3.3 Scenario 2: Clinical Research based
on Clinical Patient Data
In scenario 1, decoupling on time/place context only
effects a number of features of the message
exchange component, but the context of domain (i.e.
the clinical care setting) remains the same. In this
scenario 2, we will look at decoupling on time/place
context accompanied by a changing context of
domain (i.e. from clinical care to clinical research).
The clinical researcher wants to reuse the clinical
patient data that were captured by the clinician
within the context of patient care. Reuse of data that
were registered for another purpose is only feasible
when a number of preconditions are met. Let us first
assume that the cognitive distance between the
researcher and the clinician will be limited when
they are working within the same field. But their
needs with respect to the granularity of the data and
the number of parameters will diverge. The most
important precondition however is that sufficient
context information is available to the researcher to
determine whether the data meets the requirements
for research. As a first step towards semantic
interoperability the clinician should use controlled
terminologies during the registration of his findings.
But apart from using non-ambiguous codes for
findings or diagnoses the correct interpretation is
always dependent on (part of) the original context
that usually gets lost by the decoupling process (e.g.
reasons for visit, medication history, co morbidity).
Therefore a prerequisite to make reuse of clinical
data possible is an electronic patient record system
facilitating capturing and communicating both the
data and their context.
4 DISCUSSION
Transformation of a communication scenario as
described in the introduction to a communication
scenario supported by ICT may imply that both the
clinical data and their original context are available
to all authorized users any time and any place. It
may also imply that additional measures must be
ICT SUPPORTED COMMUNICATION IN HEALTHCARE - Benefits and Risks
497

taken to repair what gets lost by decoupling on time
and place. In daily practice no clinician can be
convinced why he should record the complete
context of each patient encounter because of
possible future reuse of the data in another domain.
Even within the same domain it will always be a
trade-off between costs related to the time-
consuming recording process and the new
opportunities that become feasible by reusing data.
Within the clinical care domain, the continuity of
care should always be the leading factor. And of
course only a small part of the complete patient
record is suited for being shared.
A practical consequence of decoupling on
time/place that was not mentioned before can be
loosing information that always ‘automatically’
came to the healthcare professional as part of his
routine (participation in a working meeting, picking
up the lab results when walking along the lab, etc.).
For each of these situations the lost information
should be provided in another way.
In order to achieve real semantic interoperability
we have to standardize both the content and the way
of communication. For standardizing the
communication many standards are already
available. The content can be standardized by
describing the structure (using a reference
information model) and the semantics (using a
terminology system). Next to a reference
information model and a terminology system a third
component is needed to act as mediator between
data and terminology and to define the clinically
relevant domain content together with its context.
The Archetype concept from the (ISO/CEN)
EN13606 standard on communication of EHR
information seems to be a promising candidate for
this third component.
5 CONCLUSIONS
Supporting communication in healthcare by ICT can
give rise to more flexibility and efficiency of care
processes. However, in most cases these benefits can
only be realized if the original context of the
information to be communicated is registered
explicitly and if negative effects of decoupling on
time/place context on other features of the
communication process can be repaired. As future
work, we plan to explore how the archetype
approach can be used to tackle these interoperability
problems.
REFERENCES
Alpay L, Toussaint P, Ezendam N, Rövekamp T,
Westendorp R, Verhoef J, Zwetsloot-Schonk JHM,
2007. The Dutch Website ‘SeniorGezond’: An
illustration of a road map for the informed patient.
Managed Care 2
Blanson Henkemans OA, Boog PJM van der, Lindenberg
J, Mast CAPG van der, Neerincx MA, Zwetsloot-
Schonk JHM, 2008. An Online Lifestyle Diary with
Persuasive Computer Assistant for Support of Self-
Management. Submitted.
Coiera E, 2000, When Conversation is better than
computation, Journal American Medical Informatics
Association, 7, 277-286.
Gemert-Pijnen, JEWC van, Nijland N, Tije S ten, Mol R,
Hennemann G. 2006. E-consult 2006, Een onderzoek
naar het gebruik van e-consult onder huisartsen. Ned.
Vereniging voor E-Health, University. Twente.
Halliday MAK,.Martin JR. 1993. Writing science:Literacy
and discursive power. London: The Falmer Press.
Te’eni D, 2001. Review: A cognitive-affective model of
organizational communication for designing IT, MIS
Quarterly, Vol. 25 No.2, pp. 251-312
Toussaint PJ, Verhoef J, Vliet Vlieland TPM, Zwetsloot-
Schonk JHM, 2004. The impact of ICT on
communication in healthcare. Stud Health Technol
Inform. 2004;107(Pt 2):988-91.
Verhoef J, Toussaint PJ, Putter H, Zwetsloot-Schonk Vliet
Vlieland TPM, 2007, The impact of the
implementation of a rehabilitation tool on the contents
of the communication during multidisciplinary team
conferences in rheumatology. Int J Med Inform. 2007
Nov-Dec;76(11-12):856-63.
HEALTHINF 2009 - International Conference on Health Informatics
498
