
AN AGENT-BASED ARCHITECTURE FOR CANCER STAGING
Miguel Miranda, Ant
´
onio Abelha, Manuel Santos, Jos
´
e Machado and Jos
´
e Neves
Uiversidade do Minho, Departamento de Inform
´
atica, Campus de Gualtar, Braga, Portugal
Keywords:
Group Decision Support Systems, Artificial Intelligence and Medicine.
Abstract:
Cancer staging is the process by which physicians evaluate the spread of cancer. This is important, once in
a good cancer staging system, the stage of disease helps to determine prognosis and assists in selecting ther-
apies. A combination of physical examination, blood tests, and medical imaging is used to determine the
clinical stage; if tissue is obtained via biopsy or surgery, examination of the tissue under a microscope can
provide pathologic staging. On the other hand, good patient education may help to reduce health service costs
and improve the quality of life of people with chronic or terminal conditions. In this paper it is endorsed a
theoretical based model to support the provision of computer based information on cancer patients, and the
computational techniques used to implement it. One’s goal is to develop an interactive agent based computa-
tional system which may provide physicians with the right information, on time, that is adapted to the situation
and process-based aspects of the patients’s illness and treatment.
1 INTRODUCTION
A healthcare unit may be approached as a distributed
computational environment, where different services
(here conceived as agents or multi-agent systems),
and people, need to communicate, exchanging data
and knowledge (e.g., cirurgical experiencies). Indeed,
whenever one is faced with a problem, the use of a
multidisciplinary team presents in itself as a solution
for the extension and complexity of the intersecting
medical specifies. Such a team, acting as a group
decision supported one, built on the base of human
beings and software agents, will intertwine all health-
care related areas. Its role will be crucial on the em-
ulation of expert behavior and to ease of the intricacy
of the diagnose process.
The explained architecture depends on the devel-
opment of key cornerstones which make the system
possible and with meaning, once a scheduled system
has no utility in a distributed environment. First of all,
in an healthcare unit one cannot allow the heterogene-
ity of the methodologies for problem solving and pro-
cedurals inherent to each medical speciality act to dis-
turb the flow of data and information among the dif-
ferent partners. Therefore, a platform for integration,
archiving and diffusing of information is required,
making all resources accessible to everyone and from
elsewhere in the environment, while not requiring any
considerable alteration of any of the medical area
specificities. The next phase on the development of
the architecture referred to above is concerned with
the use of web based interfaces as means towards ho-
mogeneity and platform independency when storing,
accessing, communicating and displaying medical in-
formation. The Electronic Health Record (EHR) is
such an application which presents the information
of the patient according to their particular problems
and manages the front-end interaction and inputs with
the specific end-user (e.g., physician, nurse, auxil-
iary personnel). The modularity inherent to the men-
tioned EHR interface is essential in order to prop-
erly integrate and establish a Group Decision Sup-
port System (GDSS), enabling workflows, scheduling
and structured patient information, leading towards
a better quality of service. The integration platform
as well as the GDSS architecture considered in this
work are designed based on an agent or multi-agent
based approach to problem solving, taking into con-
sideration not only the intricacy and heterogeneity of
both healthcare software solutions and human interac-
tion, but also the scalability and integration of differ-
ent technologies and methodologies for problem solv-
ing.
Due to the arising need for such an environment
313
Miranda M., Abelha A., Santos M., Machado J. and Neves J. (2009).
AN AGENT-BASED ARCHITECTURE FOR CANCER STAGING.
In Proceedings of the 11th International Conference on Enterprise Information Systems - Artificial Intelligence and Decision Support Systems, pages
313-316
DOI: 10.5220/0001863503130316
Copyright
c
SciTePress

in cancer staging, the intricacy of the staging itself,
and the fact that it is usually performed by none ex-
perts in the area cancer, staging was the chosen field
to start implementing such an architecture. The pro-
posed architecture is in production at an healthcare
unit and stands as a stepping-stone influence process
towards a platform which will allow distinct and tech-
nology independent decision support systems to be
fully adapted to the healthcare environment through
the use of EHR technologies.
It was under this assumption that an Agency for
the Integration, Archive and Diffusion of Medical In-
formation (AIDA) was developed, using new com-
putational paradigms and methodologies for problem
solving, which have been based based on the concept
of agent (Machado et al., 2008).
2 THE AJCC STAGING NORM
In information sharing, an understanding of the con-
cepts and vocabulary involved is paramount. Anal-
ogously, in a healthcare environment, a firm knowl-
edge on specialized areas and their uniform lexicon
is required, from physicians and other staff, in order
to normalize information communication and the pro-
cess of their dissemination among healthcare units,
in performing a group decision meeting, or even on
a peers exchange on routine practices, where the ex-
istence of different thesaurus associated to particular
backgrounds may result in dubious or mistaken as-
sumptions and culminate in misjudgments with com-
plex complications. For this reasons, several the-
saurus have been created, trying to establish an uni-
form syntactic and semantic indexation of medical in-
formation, such as SNOMED CT or even more spe-
cific normalization, like the American Joint Commis-
sion on cancer staging norms (Andrews et al., 2008).
This norm consists of a structure of uniform staging
variables within every area where there may be can-
cer, keeping however many specialized variables on
specific cancer areas (Greene et al., 1998). The speci-
ficity of the staging of each particular area increases
the difficulty of following this normalization without
any kind of help or, at least, any mean of consulta-
tion. Furthermore, case specific information or more
detailed information not presented on the form itself,
but presented in other sources, may be of great impor-
tance for a better understanding and compliancy of the
norm defined by the AJCC (Greene et al., 2003).
3 AN IMPLEMENTATION OF A
HEALTHCARE GROUP
DECISION SUPPORT SYSTEM
The system was developed with prospects of future
implementation in a particular healthcare environ-
ment. This fact greatly affected the design and soft-
ware used, resulting in a custom tool, for this spe-
cific healthcare environment. Moreover, its adaptabil-
ity towards the necessities of this particular institu-
tion and its already well designed information system,
greatly enriched the tool, giving it a broader applica-
bility when integrated with services, while at the same
time enabling a seamless area adapted service. In the
design of this system, a multi-layer architecture was
used in order to increase its reliability and scalability,
as well as to improve the results in providing the fi-
nal service as a whole, i.e., enabling a fully working
group decision platform.
In a more specific description, the GDSS follows
a client-server hierarchy and can be decomposed into
four individual layers (Figure 1). The database layer,
the cornerstone of this implementation, is the one re-
sponsible for the messaging system, which allow the
communication between human agents and software
based ones. As well as this role, it is responsible
for containing structured information for the agents
to extract and analyze. At the present time, it stores
information concerning the AJCC cancer staging sys-
tem, being this informations structured in areas and
staging variables. The application server and the user
layer are responsible for the web interface available
to human agents. The users, through web browsers,
and mediated by software agents, converse and ne-
gotiate with other agents (human or software ones)
that are able to help the user in a particular area of in-
terest or related with the problem. This communica-
tion is achieved through conveyed messages between
users and agents, stored and managed by relational
databases.
Holding the software agents, the agent layer in-
cludes several types of services that go beyond system
management, being able to interact with both human
and software agents, as well as integrating the GDSS
with the already established information system of the
healthcare institution. The human agents can com-
municate among themselves or even with other agent
systems as long as the other layers are still functional.
Within the agent system platform, each agent respon-
sible for interaction with human agents has an in-
dividual role and can interact with the user through
the messaging system, answering questions and es-
tablishing a dialogue aimed towards the problem so-
lution.
ICEIS 2009 - International Conference on Enterprise Information Systems
314
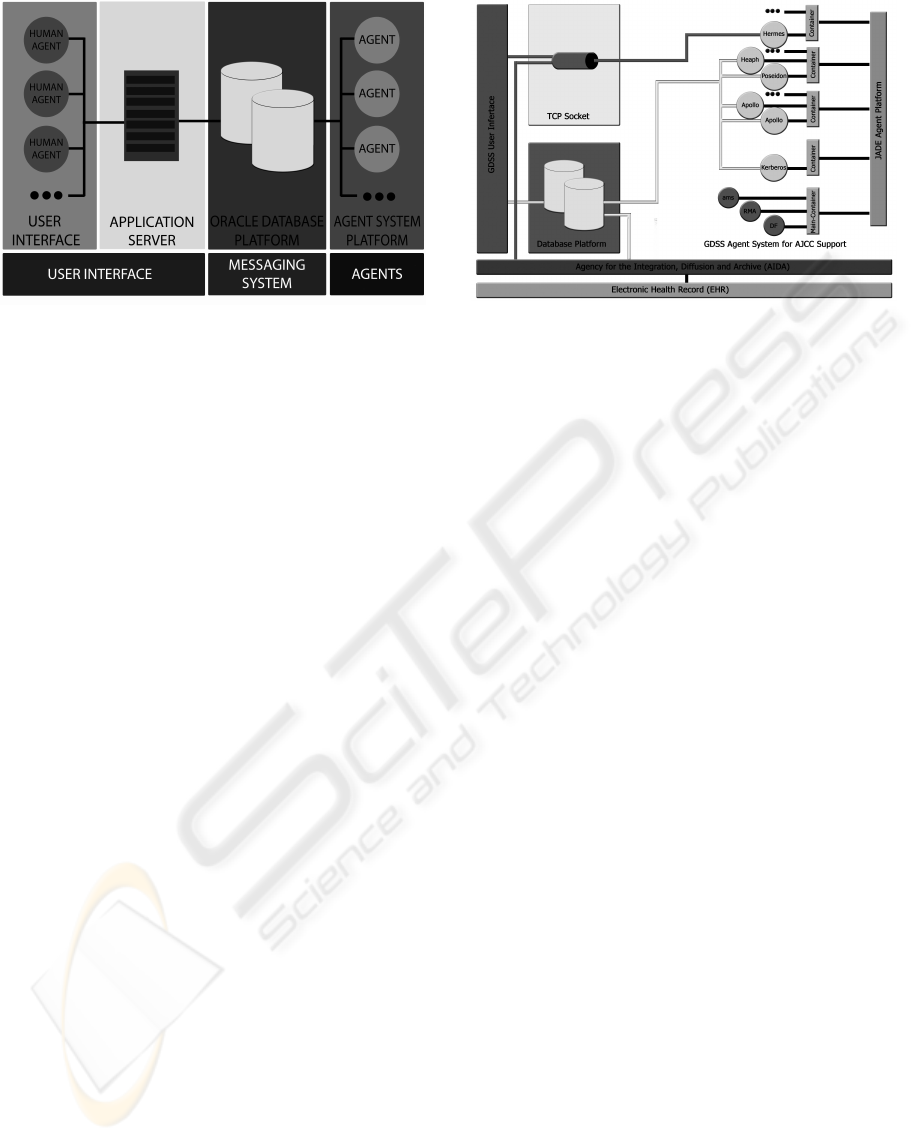
Figure 1: The GDSS Architecture.
3.1 The User Interface
The user interface is a web application that is both
based on Asynchronous Javascript and XML (AJAX)
and Hypertext Preprocessor (PHP). With the use of
AJAX, the human agent is faced with a much more
interactive environment similar to usual desktop ap-
plications, where events and other variables can be
updated on request or need without full page refresh.
The use of area specific or case specific chat
rooms is extremely important in this implementation,
as it has a vital role in enabling a specialized group de-
cision platform. In these rooms, physicians and other
healthcare personal can discuss matters, being medi-
ated or not, depending of its specific objective. The
GDSS has a great potential when integrated within a
healthcare facility, not only just with the possibility of
intercommunication within this institution on simple
work related subjects, just like any intern messaging
system, but as well as a mean of storing and easy shar-
ing of information provided by both human and soft-
ware agents. In this specific case users have a fully
functional and user friendly platform with which they
can actively interact with the information system it-
self through software agents.
The GDSS system is as well integrated with the
web application used by the same institution to ac-
cess the Electronic Health Record (EHR). In this way
agents, both human and software can generate events
when intending to interact with an user when he/she is
in any of the interface systems. As a result the system
can widely interact with users and be fully integrated
with the institutions information infrastructure. Other
functions played by other agent systems can be added
into this architecture fulfilling the continuous need to
scalability within this system.
Figure 2: GDSS Integration Platform.
3.2 Agent System
The problem addressed in this agent based system
is concerned with the AJCC’s cancer staging forms,
more concretely with the intricacy it presents to non
oncologist when staging a cancer. The need for a spe-
cialized agent may guide a physician in solving a par-
ticular staging problem, supporting the decision mak-
ing process and presenting the final staging score in a
normalized form, and then integrated it with the EHR
of the patient, make the difference and set our goals.
Indeed, the agents share decision support procedures
and resulting intents, presenting themselves as the so-
lution for the complex proceedings that may occur at
the institutional level.
In the GDSS, agent system interaction with hu-
man agents is based mainly on messages sent by
means of the database platform; there exists, how-
ever, communication agents listening at specific ports
using socket connections that can receive informa-
tion directly from an auxiliary interface. From a
brief conversation with the user, a best fitted agent is
called in order to successfully help in solving the pre-
sented problem. The data respective to cancer stag-
ing was extracted from the forms, and the supplemen-
tary guidance presented by other AJCC releases ex-
plaining the norm(Greene et al., 1998) (Greene et al.,
2003). There exists 45 forms out of the 48 chapters
of the AJJC norm, being the data in each form repre-
sented in different relations of the relational database,
distinguishing each staging variable and the relevant
information involved in the staging procedure.
3.3 The Technology
Among the possible tools to the analysis and devel-
opment of our system, the JADE framework (Java
Agent DEvelopment Framework) stands as a promis-
ingly one for GDSS. Once it was developed on top
AN AGENT-BASED ARCHITECTURE FOR CANCER STAGING
315

of the cross-platform technology Java, allows for a
strong connection among two similar computational
paradigms, such as The Agent and The Object Ori-
ented Programming ones, as well as the possibility to
easily integrate the rich Java libraries into the agent’s
behaviours. However, developed under an object ori-
ented paradigm, the difference between objects and
agents is fully secured in JADE, so that agents can
have the autonomy to choose their own actions and re-
act according to their inherent behaviour(Bellifemine
et al., 2007).
JADE is according to FIPA ( Foundation for In-
telligent Physical Agents) specifications, allowing for
a standard communication procedure, which can be
used to interact with other FIPA compliant agent
systems. With JADE, different performatives asso-
ciated with the intent on the interaction are easily
differentiated, allowing for a better comprehension
of the communication contents and objective by the
agent(Bellifemine and Rimassa, 2001). In the de-
velopment of a MAS, in order to be able to com-
municate in a rich manner, presents a potential nor-
malized infrastructure of openness, autonomy, ro-
bustness, scaleability and flexibility(Charlton et al.,
2000). The coordination among agents was success-
fully implemented following this norm, though when
integrating with the institutions proprietary agent sys-
tems, the HL7 norm was used in order to ensure that
both platforms were compliant with the same stan-
dard(Machado et al., 2008).
4 CONCLUSIONS
Modern science utilizes some basic approaches to the
study of how nature works, namely Observational
Science, Experimental Science, Theoretical Science,
and Computational Science. However, Computa-
tional Science is the newest, made possible by the
tremendous improvements in both computer hard-
ware and software over the past thirty years. Com-
putational Science, sometimes known as Modeling
and Simulation or Scientific Computing, is used in
Medicine, and benefits from knowledge in a large
amount or scale. On the other hand, staging, a key
word in our work, refers to a clinical process that
is based on knowledge and on the way cancer de-
velops, with some staging systems covering different
types of cancer, when others focus on a particular type
of cancer (e.g., distinctive staging systems are used
for countless cancers of the blood or bone marrow
such as lymphoma). Indeed, doctors gather dissim-
ilar types of information about cancer to determine
its stage. The various tests used for staging depend
on the type of cancer, and may include physical ex-
ams, imaging tests (e.g., XR, CT or MRI), laboratory
tests (e.g., blood, urine, uids or tissues), or pathol-
ogy and surgical reports, i.e., in terms of the algo-
rithm, in Computational Science, the scientific prob-
lem must be expressed mathematically, known as the
Algorithm. In terms of the architecture, once a suit-
able algorithm has been determined, that algorithm is
translated into one or more computer programs and
implemented on one or more types of hardware. In
our work, the combination of software and hardware
is referred to as the Computational Architecture, the
AIDA agency referred to above.
REFERENCES
Andrews, J. E., Patrick, T. B., Richesson, R. L., Brown, H.,
and Krischer, J. P. (2008). Comparing heterogeneous
snomed ct coding of clinical research concepts by ex-
amining normalized expressions. J. of Biomedical In-
formatics, 41(6):1062–1069.
Bellifemine, F. and Rimassa, G. (2001). Developing multi-
agent systems with a fipa-compliant agent framework.
Softw. Pract. Exper., 31(2):103–128.
Bellifemine, F. L., Caire, G., and Greenwood, D. (2007).
Developing Multi-Agent Systems with JADE (Wiley
Series in Agent Technology). John Wiley & Sons.
Charlton, P., Mamdani, E., Cattoni, R., and Potrich, A.
(2000). Evaluating the fipa standards and its role
in achieving cooperation in multi-agent systems. In
HICSS ’00: Proceedings of the 33rd Hawaii Interna-
tional Conference on System Sciences-Volume 8, page
8034, Washington, DC, USA. IEEE Computer Soci-
ety.
Greene, F., Page, D., Fleming, I., Fritz, A., Balch, C.,
Haller, D., and Morrow, M. E. (1998). AJCC Can-
cer Staging Forms for Microsoft Word). Lippincott
Williams & Wilkins.
Greene, F. L., Page, D. L., (Editor), I. D. F., Fritz, A., and
Balch, C. M. (2003). AJCC Cancer Staging Handbook
- From the AJCC Cancer Staging Manual. Springer-
Verlag, sixth edition edition.
Machado, J., Abelha, A., Novais, P., ao Neves, J., and
Neves, J. (2008). Improving patient assistance and
medical practices through intelligent agents. In Pro-
ceedings of the Workshop in Agents Applied in Health-
care, AAMAS 2008.
ICEIS 2009 - International Conference on Enterprise Information Systems
316
