
On the Automatic Classification of Reading Disorders
Andreas Maier
1
, Caroline Parchmann
2
, Tobias Bocklet
1
, Florian H¨onig
1
Oliver Kratz
2
, Stefanie Horndasch
2
, Elmar N¨oth
1
and Gunther Moll
2
1
Lehrstuhl f¨ur Mustererkennung (Informatik 5)
Friedrich-Alexander Universit¨at Erlangen N¨urnberg
Martensstr.3, 91058 Erlangen, Germany
2
Kinder- und Jugendabteilung f¨ur Psychische Gesundheit, Universit¨atsklinikum Erlangen
Schwabachanlage 6 und 10, 91054 Erlangen, Germany
Abstract. In this paper, we present an automatic classification approach to iden-
tify reading disorders in children. This identification is based on a standardized
test. In the original setup the test is performed by a human supervisor who mea-
sures the reading duration and notes down all reading errors of the child at the
same time. In this manner we recorded tests of 38 children who were suspected
to have reading disorders. The data was confronted to an automatic system which
employs speech recognition to identify the reading errors. In a subsequent classi-
fication experiment — based on the speech recognizer’s output and the duration
of the test — 94.7% of the children could be classified correctly.
1 Introduction
The state-of-the-art approach to examine children for reading disorders is a perceptual
evaluation of the children’s reading abilities. In all of these reading tests, a list of words
or sentences is presented to the child. The child has to read all of the material as fast and
as accurate as possible. In order to determine whether the child has a reading disorder
two variables are investigated by a human supervisor during the test procedure:
– The duration of the test, i.e. the fluency, and
– The number of reading errors during the reading of the test material, i.e., the accu-
racy.
Both variables, however, are dependent on the age of the child and related to each other.
If a child tries to read very fast, the number of reading errors will increase and vice
versa [1]. Furthermore, with increasing age the reading ability of children increases.
Hence, appropriate test material has to be chosen according to the age and reading
ability of the child. Therefore, reading tests often consist of different sub-tests. While
younger children are tested with really existing words and only short sentences, the
older children have to be tested with more difficult tasks, such as long complex sen-
tences and pseudo words which may or may not resemble real words. Appropriate sub-
tests are then selected for each tested child. Often this is linked to the child’s progress
in school.
One major drawback of the testing procedure is the intra-rater variablity in the per-
ceptual evaluation procedure. Although the test manual often defines how to differen-
tiate reading errors from normal disfluencies and “allowed” pronunciation alternatives,
Maier A., Parchmann C., Bocklet T., Hönig F., Kratz O., Horndasch S., Nöth E. and Moll G. (2009).
On the Automatic Classification of Reading Disorders.
In Proceedings of the 9th International Workshop on Pattern Recognition in Information Systems, pages 18-27
DOI: 10.5220/0002174700180027
Copyright
c
SciTePress

there is no exact definition of a reading error in terms of its acoustical representation.
In order to solve this problem, we propose the use of a speech recognition system to
detect the reading errors. This procedure has two major advantages:
– The intra-rater variability of the speech recognizer is zero because it will always
produce the same result given the same input.
– The definition of reading errors is standardized by the parameters of the speech
recognition system, i.e., the reading ability test can also be performed by lay per-
sons with only little experience in the judgment of readings disorders.
In the literature, different automatic approaches to determine the “reading level” of a
child exist. Often the reading level is linked to the perceptual evaluation of expert listen-
ers using five to seven classes. In [2] Black et al. estimate a reading level between 1 and
7 using pronunciation verification methods based on Bayesian Networks. Compared to
the human evaluation they achieve correlations between their automatic predictions and
the human experts of up to 0.91 on 13 speakers. In [3] the use of finite-state-transducers
is proposed to obtain a “reading level” between “A” (best) and “E” (worst). For this
five-class problem absolute recognition rates of up to 73.4% for real words and 62.8%
for pseudo words are reported. In order to remove age-dependent effects from the data,
80 children in the 2nd grade were investigated. Both papers focus on the creation of a
“reading tutor” in order to improve children’s reading abilities.
In contrast to these studies, we are interested in the diagnosis of reading disorders
as they are relevant in a clinical point of view. Currently, we are developing PEAKS
(Program for the Evaluation of All Kinds of Speech Disorders [4]) — a client-server-
based speech evaluation framework — which was already used to evaluate speech in-
telligibility in children with cleft lip and palate [5], patients after removal of laryngeal
cancer [6], and patients after the removal of oral cancer [7]. PEAKS features interfaces
and tools to integrate standardized speech tests easily. After integration of a new test,
PEAKS can be used for recording from any PC which is connected to the Internet if
Java Runtime Environment version 1.6 or higher is installed. All analyses performed by
PEAKS are fully automatic and independent of the supervising person. Hence, it is an
ideal framework to integrate an automatic reading disorder classification system.
The paper is organized as follows. First the test material, the recorded speech data
and its annotation is described and discussed. Next, the automatic evaluation methods,
i.e., the speech recognizer and the classifiers, are reported. In the results section the clas-
sification accuracy is presented in detail. The subsequent section discusses the outcome
of the experiments. The paper is concluded by a summary.
2 Speech Data
In order to be able to interpret the results and to compare them to other studies’ test
material, speech data, and its annotation is described in detail here. Special attention is
given to the annotation procedure since the automatic evaluation algorithm aims to be
used for clinical diagnosis. Therefore, the annotation should meet clinical standards.
19

Table 1. Structure of the SLRT test: Thetable reports all sub-tests of the SLRT with their contents,
their number of words, and the school grades in which the respective sub-test is suitable.
sub-test content # of words grade
SLRT1 A short list of bisyllabic, single, real words to introduce the test.
This part is not analyzed according to the protocol of the test.
8 1–4
SLRT2 A list of mono- and bisyllabic real words 30 1–4
SLRT3 A list of compound words with two to three compounds each 11 3–4
SLRT4 A short story with only mono- and bisyllabic words 30 1–2
SLRT5 A longer story with mainly mono- and bisyllabic words but also
a few compound words
57 3–4
SLRT6 A short list of pseudo words with two to three syllables to intro-
duce the pseudo words. This part is not analyzed according to
the protocol of the test.
6 3–4
SLRT7 A list of pseudo words with two to three syllables 24 1–4
SLRT8 A list of mono- and bisyllabic pseudo words which resemble
real words
30 2–4
2.1 Test Material
The recorded test data is based on a German standardized reading disorder test — the
“Salzburger Lese-Rechtschreib-Test” (SLRT, [8]). In total the SLRT consists of eight
sub-tests (cf. Table 1). All sub-tests contain 196 words of which 170 are disjoint.
The test is standardized according to the instructions and the evaluation. The test is
presented in form of a small book, which is handed to the children to read in. They get
the instruction to read the text as fast as possible while doing as little reading mistakes
as possible.
In the original setup the supervisor of the test has to measure the time for all sub-
tests separately while noting down the reading errors of the child.
We will only report the results obtained for the SLRT7 and SLRT8 sub-tests in the
following.
On the one hand, the setup of the perceptual evaluation for all sub-tests is very
similar. Therefore, it is not necessary to report the results of all sub-tests. On the other
hand, the investigation of pseudo words using automatic systems is described as the
most challenging task in the literature [2]. The sub-test SLRT6 also contains pseudo
words, but no perceptual evaluations are conducted according to the test manual.
2.2 Recording Setup
In order to be able to collect the data directly at the PC, the test had to be modified. In-
stead of a book, the text was presented as a slide on the screen of a PC. The instructions
to the child were the same as in the original setup.
All children were recorded with a head-mounted microphone (Plantronics USB
510) at the University Clinic Erlangen. The recordings took place in a separate quiet
room without background noises. Hence, appropriate audio quality was achieved in all
recordings.
20
Table 2. 38 Children were recorded with the SLRT: The table shows mean value, standard de-
viation, minimum, and maximum of the age of the children and the count (#) in the respective
group.
group # mean std. dev. min max
all 38 9.7 0.9 7.8 11.3
girls 12 10.2 0.7 9.0 11.3
boys 26 9.5 0.9 7.8 11.3
Table 3. Overview on the limits of pathology for the SLRT7 and SLRT8 sub-tests
SLRT 7 SLRT 8
grade # of errors duration [s] # of errors duration [s]
1st 8 144 - -
2nd 7 113 6 100
3rd 6 78 5 70
4th 5 62 4 55
In total 38 children (26 boys and 12 girls) were recorded. The average age of the
children was 10.2 ± 0.9 years. A detailed overview regarding the statistics of the chil-
dren’s ages is given in Table 2. All of the children were speculated to have a reading
disorder.
2.3 Perceptual Evaluation
For each child the decision whether its reading ability was pathologic or not was de-
termined according to the manual of the SLRT [8]. A child’s reading ability is deemed
pathologic
– if the duration of the test is longer than an age-dependent standard value or
– if the number of reading errors exceeds an age-dependent standard value.
These limits differ for each sub-test according to the SLRT. Table 3 reports these limits
for the sub-tests SLRT7 and SLRT8. In the SLRT7 and the SLRT8 sub-test 30 children
were above the time limit.
We assigned each child two different labels: “reading error/normal”and “pathologic/non-
pathologic”. If only the number of misread words is exceeded, the child is assigned the
label “reading error”, otherwise “normal”. Reading errors are regarded as soon as a sin-
gle phonemic deviation is found. Errors of the accentuation of the word are also counted
as reading errors as described in the manual of the test [8]. For the case of the SLRT7
data, 12 children exceeded the limit of reading errors while 14 children were above the
error limit in the SLRT8 data.
If either of these two boundaries is exceeded by the child, the child is assigned
the label “pathologic”. In both sub-tests 32 of the 38 children were diagnosed to have
pathologic reading.
3 Automatic Evaluation System
The automatic evaluation is based on three information sources:
21

– The total duration of the test
– The reading error and duration limits (cf. Table 3)
– The word accuracy computed by a speech recognition system
The test duration can be easily accessed as PEAKS tracks this information automati-
cally during the recording. Prior information about the child — namely the child’s age
and the respective duration and error limits — can also easily be obtained (cf. Table 3).
3.1 Speech Recognition Engine
For the objective measurement of the reading accuracy, we use an automatic speech
recognition system based on Hidden Markov Models (HMM). It is a word recognition
system developed at the Chair of Pattern Recognition (Lehrstuhl f¨ur Mustererkennung)
of the University of Erlangen-Nuremberg. In this study, the latest version as described
in detail in [9] and [10] was used.
As features we use 11 Mel-Frequency Cepstrum Coefficients (MFCCs) and the en-
ergy of the signal plus their first-order derivatives. The short-time analysis applies a
Hamming window with a length of 16ms, the frame rate is 10ms. The filter bank for
the Mel-spectrum consists of 25 triangular filters. The 12 delta coefficients are com-
puted over a context of 2 time frames to the left and the right side (56 ms in total).
The recognition is performed with semi-continuous HMMs. The codebook con-
tains 500 full covariance Gaussian densities which are shared by all HMM states. The
elementary recognition units are polyphones [11], a generalization of triphones. Poly-
phones use phones in a context as large as possible which can still statistically be mod-
eled well, i.e., the context appears more often than 50 times in the training data. The
HMMs for the polyphones have three to four states.
We used a unigram language model to weigh the outcome of each word model. It
was trained with the reference of the tests. For our purpose it was necessary to em-
phasize the acoustic features in the decoding process. In [12] a comparison between
unigram and zerogram language models was conducted. It was shown that intelligibil-
ity can be predicted using word recognition accuracies computed using either zero- or
unigram language models. The unigram, however,is computationally more efficient be-
cause it can be used to reduce the search space. The use of higher n-gram models was
not beneficial.
The result of the recognition is a word lattice. In order to get an estimate of the
quality of the recognition, the word accuracy (WA) is computed. Based on the number
of correctly recognized words C and the number of words R in the reference, the WA
is further dependent on the number or wrongly inserted words I:
WA =
C − I
R
· 100 %
Hence, the WA can take values between minus infinity and 100%.
The speech recognition system had been trained with acoustic information from 23
male and 30 female children from a local school who were between 10 and 14 years
old (6.9 hours of speech). To make the recognizer more robust, we added data from 85
male and 47 female adult speakers from all over Germany (2.3 hours of spontaneous
22

speech from the VERBMOBIL project, [13]). The data were recorded with a close-talk
microphone with 16 kHz sampling frequency and 16 bit resolution. The adult speakers
were from all over Germany and thus covered most dialect regions. However, they were
asked to speak standard German. The adults’ data were adapted by vocal tract length
normalization as proposed in [14]. During training an evaluation set was used that only
contained children’s speech. MLLR adaptation (cf. [15,16]) with the patients’ test data
led to further improvement of the speech recognition system.
3.2 Classification System
Classification was performed in a leave-one-speaker-out (LOO) manner since there was
only little training and test data available. We chose three popular measures in order to
report the classification accuracy.
– CL: The class-wise-averaged recognition rate, or so-called average recall. It is de-
termined as
CL =
1
K
K
X
k
recall(k)
!
· 100 % (1)
where K is the number of classes. The CL is useful if the distribution of the classes
is biased.
– RR: The total recognition rate determined as the fraction of correctly identified
samples c divided by the number of samples n:
RR =
c
n
· 100 % (2)
The RR reports the overall performance of the classifier including the class distri-
bution of the data.
– ROC denotes the area under the Receiver-Operating-Characteristic (ROC) curve
[17]. A random classifier yields an area of 0.5 while the perfect classifier would
yield an area of 1.0.
As classification system we decided for Ada-Boost [18] in combination with an LDA-
Classifier as simple classifier as it was already successfully applied in [19].
4 Results
Table 4 shows the results of the classification experiment “reading error”. The task
was to determine automatically whether the age-dependent limit of reading errors was
exceeded or not. For both sub-tests, the classification performance using duration infor-
mation and WA only is moderate. If the age-dependent limit which is dependent on the
school grade of the child is also provided to the classifier, the performance increases for
both sub-tests (90.1 % CL for SLRT7 and 68.2% CL for SLRT8). The actual age —
defined by the date of birth of the child and the date and time of recording — did not
yield any improvement for this classification task.
As a second experiment, the use of the classification system to automatically de-
termine reading disorders was investigated. Now, the task was to classify whether the
23
Table 4. Overview on the classification results for the task “reading error”. CL is the average
recall, RR the absolute recognition rate and ROC the area under the ROC curve.
SLRT 7 SLRT 8
feature set CL [%] RR [%] ROC CL [%] RR [%] ROC
duration and accuracy 59.5 65.8 0.74 61.6 68.4 0.74
+ age-dependent limits 90.1 89.5 0.97 68.2 71.1 0.62
+ actual age 77.6 81.6 0.81 50.3 57.9 0.56
Table 5. Overview on the classification results for the task “pathologic”. CL is the average recall,
RR the absolute recognition rate and ROC the area under the ROC curve.
SLRT 7 SLRT 8
feature set CL [%] RR [%] ROC CL [%] RR [%] ROC
duration and accuracy 90.1 94.7 0.99 68.7 81.6 0.66
+ age-dependent limits 83.3 84.7 0.99 70.3 84.2 0.76
+ actual age 81.8 91.1 0.99 88.5 92.1 0.83
child has a reading disorder or not. Table 5 reports the results. Using only duration and
WA, high recognition rates can already be obtained for the SLRT7 sub-test. For the
case of the SLRT8 sub-test, more information is required to obtain such high classifica-
tion rates. If the age-dependent limits of the SLRT8 and the actual age of the child are
supplied to the classifier, a CL of 88.5% is achieved.
5 Discussion
The scope of this paper was the automatic detection and classification of reading disor-
ders in children. Therefore, we chose a clinical standard test and recorded 38 children
who were speculated to have reading disorders.
In order to diagnose a reading disorder,the time of the test has to be investigated and
the number of reading errors has to be determined because both variables are related.
This was performed according to the manual of the SLRT test.
Next, these data were confronted to an automatic evaluation routine based on an
automatic speech recognition system. For the SLRT7 test, using the test duration, the
WA, and the age-dependent limits of the test, the automatic system could already deter-
mine whether the child exceeded the number of reading errors or not at a CL of 90.1%
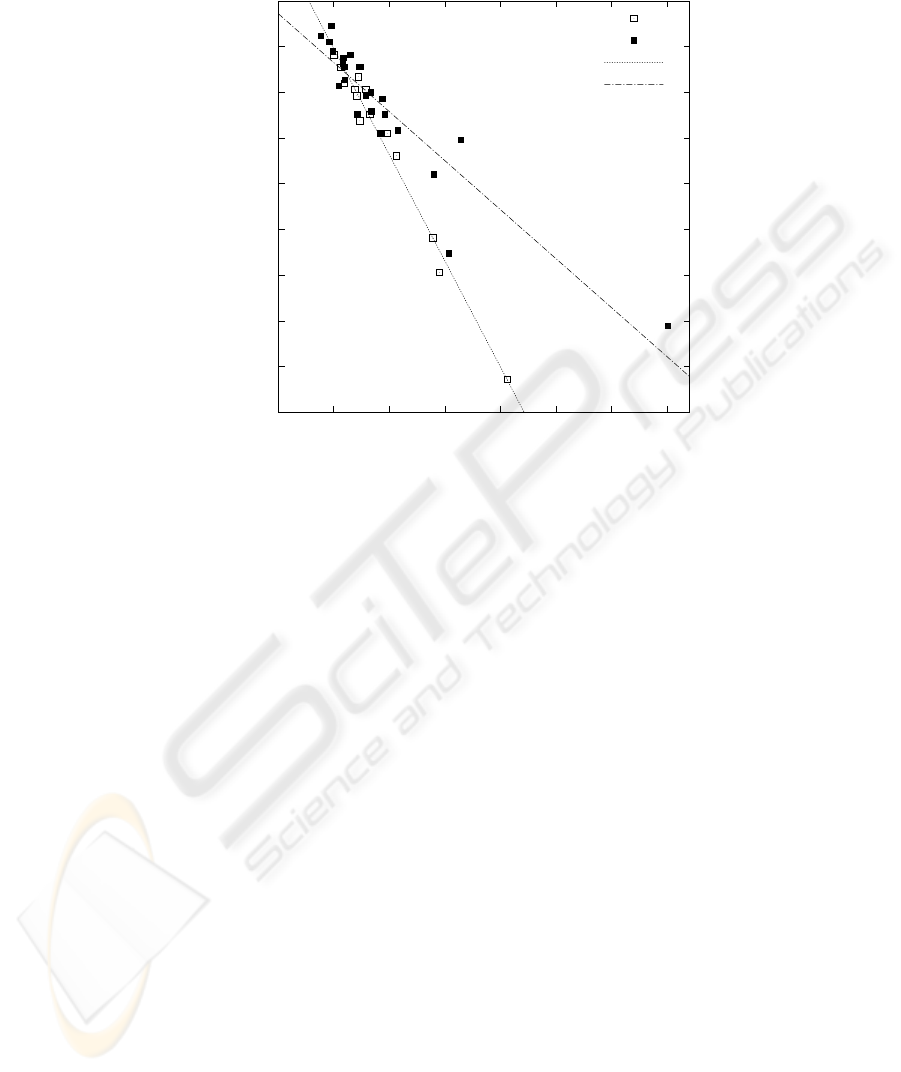
(89.5% RR). For the SLRT8, however, only 68.2% accuracy were achieved. Figure 1
shows the relation between WA and the duration for the SLRT8 sub-test. Although both
are correlated, duration and WA can be used to distinguish children with many reading
errors from children with only few reading errors. However, both clusters are scattered
into each other. If the reading error limit is also supplied the performance of the clas-
sification system increases. The actual age of the children did not contribute. This may
be related to the boosting algorithm. It emphazises the wrong features and classifies
according to the age instead of the grade.
In a second experiment we investigated whether these classification rates were al-
ready enough to determine a reading pathology automatically. In the SLRT7 sub-test,
24
-350
-300
-250
-200
-150
-100
-50
0
50
100
0 50 100 150 200 250 300 350
word accuracy [%]
duration [s]
X (reading error)
O (normal)
regression line X
regression line O
Fig.1. The plot shows the children of the SLRT8 sub-test: The regression lines show that the
additional use of speech recognition helps to differentiate between the children with many reading
errors and the ones with few reading errors.
90.1% CL (94.7% RR) were achieved.Investigationof the SLRT8 sub-test showed that
a high classification rate of 88.5 % CL (92.1% RR) could also be achieved. Hence, the
proposed system is suitable for the automatic classification of reading disorders, even
though the classification of the reading errors is not perfect. Figure 2 shows this pro-
cess: If duration and reading errors are taken into account the group of non-pathologic
children can be found on the top left of the plot. However,both groups still overlap. Fur-
ther prior information helps to distinguish them from each other. In this experiment the
limits and the true age of the child improve the classification further. In further experi-
ments using the other sub-tests and a control group of non-pathologic school children,
we will investigate this effect in more detail.
In the future this procedure will help in the diagnosis of reading disorders in chil-
dren. The system can also be used by lay persons with only little understanding of read-
ing disorders. Screening of reading disorders is also within the reach of the proposed
system.
6 Summary
In this paper we presented an automatic approach for the classification of reading disor-
ders based on automatic speech recognition. The evaluation is performed on a standard-
ized German reading capability test that contains pseudo words. To our knowledge such
25

-350
-300
-250
-200
-150
-100
-50
0
50
100
0 50 100 150 200 250 300 350
word accuracy [%]
duration [s]
pathologic
non-pathologic
Fig.2. The plot shows the children of the SLRT8 sub-test: The non-pathologic children can be
found in the upper left corner of the diagram. The data points of the pathologic children are scat-
tered to the bottom right. Duration and word accuracy (WA) alone are not sufficient to separate
both clusters.
a system has not been published before. The system is web-based and can be accessed
from any PC which is connected to the Internet.
Using a database with 38 children classification rates of up to 94.7% (RR) could be
achieved. The system is suitable for the automatic classification of reading disorders.
References
1. I. Dennis and J. St. B. T. Evans, “The speed-error trade-off problem in psychometric testing,”
British Journal of Psychology, vol. 87, pp. 105–129, 1996.
2. M. Black, J. Tepperman, S. Lee, and S. Narayanan, “Estimation of children’s reading ability
by fusion of automatic pronunciation verification and fluency detection,” in Interspeech 2008
– Proc. Int. Conf. on Spoken Language Processing, 11th International Conference on Spoken
Language Processing, September 25-28, 2008, Brisbane, Australia, Proceedings, 2008, pp.
2779–2782.
3. J. Duchateau, L. Cleuren, H. Van Hamme, and P. Ghesquiere, “Automatic assessment of
children’s reading level,” in Interspeech 2007 – Proc. Int. Conf. on Spoken Language Pro-
cessing, 10th European Conference on Spoken Language Processing, August 27-31, 2007,
Antwerp, Belgium, Proceedings, 2007, pp. 1210–1213.
4. A. Maier, T. Haderlein, U. Eysholdt, F. Rosanowski, A. Batliner, M. Schuster, and E. N¨oth,
“PEAKS – A System for the Automatic Evaluation of Voice and Speech Disorders,” Speech
Communication, vol. 51, no. 5, pp. 425–437, 2009.
26

5. A. Maier, E. N¨oth, A. Batliner, E. Nkenke, and M. Schuster, “Fully Automatic Assessment
of Speech of Children with Cleft Lip and Palate,” Informatica, vol. 30, no. 4, pp. 477–482,
2006.
6. M. Schuster, T. Haderlein, E. N¨oth, J. Lohscheller, U. Eysholdt, and F. Rosanowski, “Intel-
ligibility of laryngectomees’ substitute speech: automatic speech recognition and subjective
rating,” Eur Arch Otorhinolaryngol, vol. 263, no. 2, pp. 188–193, 2006.
7. M. Windrich, A. Maier, R. Kohler, E.N¨oth, E. Nkenke, U. Eysholdt, and M. Schuster, “Au-
tomatic Quantification of Speech Intelligibility of Adults with Oral Squamous Cell Carci-
noma,” Folia Phoniatr Logop, vol. 60, pp. 151–156, 2008.
8. K. Landerl, H. Wimmer, and E. Moser, Salzburger Lese- und Rechtschreibtest. Verfahren zur
Differentialdiagnose von St¨orungen des Lesens und des Schreibens f¨ur die 1. bis 4. Schul-
stufe, Huber, Bern, 1997.
9. F. Gallwitz, Integrated Stochastic Models for Spontaneous Speech Recognition, vol. 6 of
Studien zur Mustererkennung, Logos Verlag, Berlin (Germany), 2002.
10. G. Stemmer, Modeling Variability in Speech Recognition, vol. 19 of Studien zur Muster-
erkennung, Logos Verlag, Berlin (Germany), 2005.
11. E.G. Schukat-Talamazzini, H. Niemann, W. Eckert, T. Kuhn, and S. Rieck, “Automatic
Speech Recognition without Phonemes,” in Proc. European Conf. on Speech Communication
and Technology (Eurospeech), Berlin (Germany), 1993, vol. 1, pp. 129–132.
12. K. Riedhammer, G. Stemmer, T. Haderlein, M. Schuster, F. Rosanowski, E. N¨oth, and
A. Maier, “Towards Robust Automatic Evaluation of Pathologic Telephone Speech,” in
Proceedings of the Automatic Speech Recognition and Understanding Workshop (ASRU),
Kyoto, Japan, 2007, pp. 717–722, IEEE Computer Society Press.
13. W. Wahlster, Ed., Verbmobil: Foundations of Speech-to-Speech Translation, Springer, Berlin
(Germany), 2000.
14. G. Stemmer, C. Hacker, S. Steidl, and E. N¨oth, “Acoustic Normalization of Children’s
Speech,” in Proc. European Conf. on Speech Communication and Technology, Geneva,
Switzerland, 2003, vol. 2, pp. 1313–1316.
15. M. Gales, D. Pye, and P. Woodland, “Variance compensation within the MLLR framework
for robust speech recognition and speaker adaptation,” in Proceedings of the International
Conference on Speech Communication and Technology (Interspeech), Philadelphia, USA,
1996, vol. 3, pp. 1832–1835, ISCA.
16. A. Maier, T. Haderlein, and E. N¨oth, “Environmental Adaptation with a Small Data Set of the
Target Domain,” in 9th International Conf. on Text, Speech and Dialogue (TSD), P. Sojka,
I. Kopeˇcek, and K. Pala, Eds., Berlin, Heidelberg, New York, 2006, vol. 4188 of Lecture
Notes in Artificial Intelligence, pp. 431–437, Springer.
17. A. Fawcett, “An introduction to ROC analysis,” Pattern Recognition Letters, vol. 27, pp.
861–874, 2006.
18. Yoav Freund and Robert E. Schapire, “Experiments with a new boosting algorithm,” in
Thirteenth International Conference on Machine Learning, San Francisco, 1996, pp. 148–
156, Morgan Kaufmann.
19. C. Hacker, T. Cincarek, A. Maier, A. Heßler, and E. N¨oth, “Boosting of Prosodic and Pronun-
ciation Features to Detect Mispronunciations of Non-Native Children,” in Proceedings of the
International Conference on Acoustics, Speech, and Signal Processing (ICASSP), Hawaii,
USA, 2007, vol. 4, pp. 197–200, IEEE Computer Society Press.
27
