
DIAGNOSIS
A Global Alignment and Fusion Medical System
E. Faliagka, V. N. Syrimpeis, A.Tsakalidis
Computer Engineering and Informatics Department, University of Patras, Greece
G. K. Matsopoulos
School of Electrical and Computer Engineering, National Technical University of Athens, Greece
J. Tsaknakis, G. Tzimas
Department of Applied Informatics in Administration and Economy, National Technical University of Messolonghi, Greece
Keywords: Medical systems, Image processing, Registration, Fusion.
Abstract: In this paper, a global registration-fusion system of medical data is presented in detail. The system is
comprised by the following basic subsystems: (1) the multimodal medical image archiving and
communication subsystem, (2) the image processing subsystem, and (3) the multimodal registration and
fusion subsystem. The system offers various capabilities such as storage, retrieval, distribution and
presentation of images from different medical modalities in DICOM format, supports multiple examinations
of a patient and uses parallel processing threads to perform the processing of the acquired three-dimensional
(3D) data in almost real time. The paper discusses the basic features of the proposed system, analyzes the
proposed algorithms for image preprocessing, registration and fusion and presents the results of an
experimental study that was carried out for evaluating its performance. The innovation of the proposed work
is multilayered. It provides automatic matching based on both segmented surfaces and on different levels of
gray and it allows comparison of registration accuracy for the different techniques based on specific criteria
to quantify registration. Finally, it improves the registration when there is movement and / or distortion in
the data collection of the patient from different imaging systems.
1 INTRODUCTION
Medical imaging is a vital component of diagnostic
medicine, and it also has a significant role in the
areas of surgical planning and radiotherapy (Maintz,
1998). Often, medical images acquired in the clinical
track are using different imaging technologies.
Integrating these images, which are often
complementary in nature, is a challenging problem.
The first step in the integration process is bringing
the tomographic images into spatial registration, so
that the same anatomical regions coincide, a
procedure referred to as registration (Hajnal, 2001).
After registration, a fusion step is required in order
to combine information from different modalities, or
from the same modalities at different examination
periods (
Hawks, 1992).
A prominent example where the fusion of
registered images maximizes the available
diagnostic information is tumor diagnosis and
radiotherapy treatment. The Magnetic Resonance
(MR) imaging system, the SPECT medical imaging
and the Positron Emission Tomography (PET)
provide functional information even at very early
stages of cancerous tumors, but they do not reliably
depict the anatomical characteristics of the tested
organs. On the other hand, tomographic imaging
techniques such as Computer Tomography (CT) and
magnetic (MR) scanners, the ultrasound and X-rays
provide anatomical information, but usually
determine the existence of a cancer tumor only when
it is in a later stage compared to the functional
techniques. Thus, the combined use of different
modalities that offers complementary clinical
information is much more effective, allowing early
21
Faliagka E., Syrimpeis V., Tsakalidis A., Matsopoulos G., Tsaknakis J. and Tzimas G. (2010).
DIAGNOSIS - A Global Alignment and Fusion Medical System.
In Proceedings of the Third International Conference on Health Informatics, pages 21-28
DOI: 10.5220/0002695500210028
Copyright
c
SciTePress
diagnosis and accurate identification of a cancer
tumor and hence the effective planning of the
radiotherapy treatment.
It is often necessary to align medical data to
illustrate the changes between the data retrieved at
different times so as to assess the progress of a
disease, or to assess the effectiveness of the
treatment. In this case the fusion of data is
implemented to illustrate the changes, as in the
measurement of bone support for implants using
dental radiographs. Moreover, the data registration
applies to cases where data from anatomical atlases
in conjunction with real clinical data and studies on
patient populations are used.
In this work, a global alignment-fusion system of
medical data was developed, which was named
«dIaGnosis». Comparable software systems for
processing and visualization of medical data are also
implemented by Philips Medical Systems Inc.,
Siemens Medical Systems Inc and others. Medical
data in commercial systems are represented in
DICOM format, which is the prominent medical
data protocol. Most commercial software provide
semi-automatic and automatic registration options,
as well as possibilities for data fusion after
registration alignment, either on sections base (2D
problem) or on surfaces base (3D problem). The
proposed system overbalances the existing
registration techniques. Specifically, it provides
automatic matching based on both segmented
surfaces and on different levels of gray, while
algorithms are applied directly to three-dimensional
(3D) data. In addition, it allows the application of
different geometric transformations, including an
elastic transformation to improve the registration
when there is movement and / or distortion in the
data collection of the patient from different imaging
systems. Finally, it allows comparison of registration
accuracy for the different techniques based on
specific criteria to quantify registration.
This paper is organized as follows. Section 2
outlines the architecture of the system proposed and
presents the algorithms used for image
preprocessing, registration and fusion. Section 3
describes the working environment of the
implemented system. Section 4 presents the baseline
scenario where most of the procedures supported by
the system are shown. The efficiency of registration
techniques was tested during the pilot study on skull
patient data collected from CT and MR scanners.
2 SYSTEM ARCHITECTURE
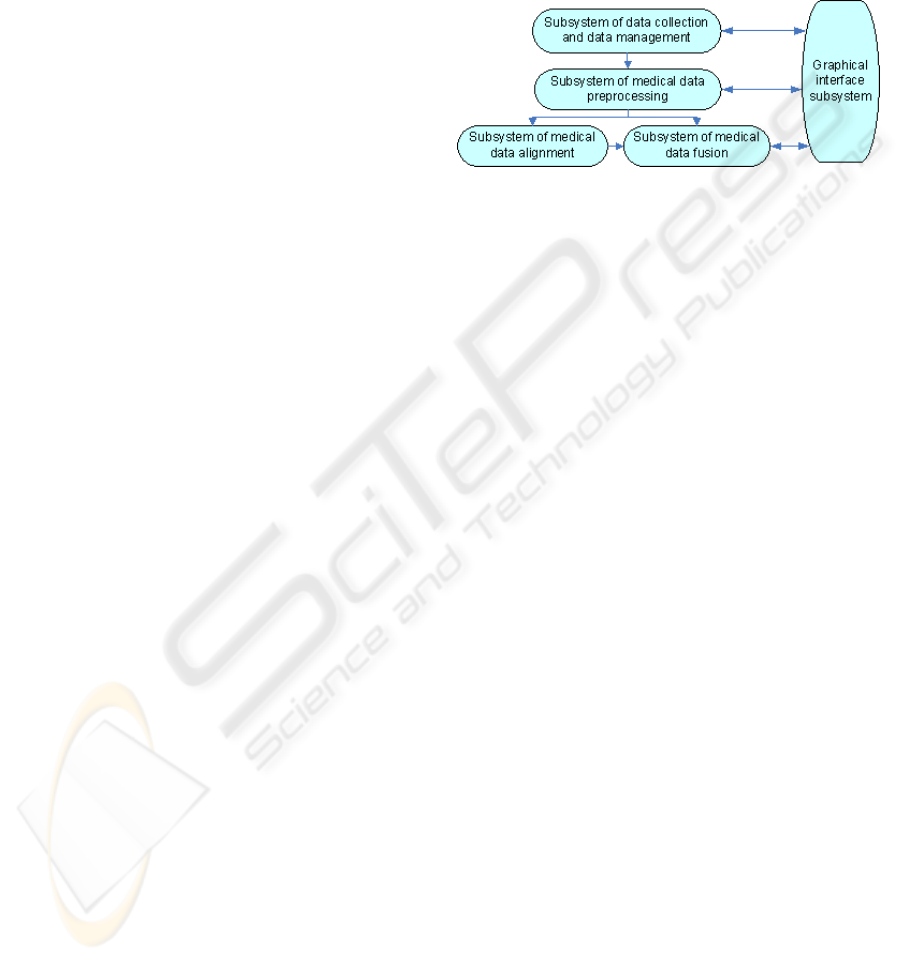
In Figure 1 the overall system architecture is
depicted. The system consists of five complementary
layers-subsystems, managing the registration and
fusion of the medical data, as well as the interaction
with the final user.
Figure 1: The system architecture.
According to the proposed architecture, the
system consists of the following five subsystems.
2.1 Data Collection and Data
Management Subsystem
The subsystem of data collection and management
allows the storage, retrieval, distribution and
presentation of medical images:
Using Magneto-optical instrument, and
Data transfer via network from the diagnostic
consoles of the CT and MR scanners, or a
workstation where digital medical data are
acquired.
The medical data collected are a series of sections
from the same patient from different imaging
modalities (CT and MR scanners) and correspond to
a specific region of the human body. In the pilot
version of the system the data correspond to the
region of the skull as acquired from both CT and
MR scanners.
As mentioned earlier, DICOM format is the
prominent international protocol for medical data.
Thus, the medical data acquired by the scanners are
compatible with this format. The entry, management
and export data are in DICOM format too. (NEMA,
2006)
In this subsystem we implemented a function
that reads the header of the DICOM file (DICOM
header) and includes automatically the following
technical characteristics of the system: the number
of sections, the number of pixels per section, a data
analysis per section (mm/pixel), the interval sections
(mm), the number of bits/pixel and the patient data
(patient code, DATE examination, etc.), if available.
The basic technical capabilities of the subsystem
HEALTHINF 2010 - International Conference on Health Informatics
22

include:
Patient (code) correspondence with the initial
data of his/her examination.
Multiple examinations per patient (through
appropriate code).
Data display with multiple horizontal sections
in icon size.
Data storage after their process (in DICOM or
other format) in the hard disk of the computer
system.
Determination of reference data from the user.
Ability to support multiple data to align
common reference data.
2.2 Medical Data Preprocessing
Subsystem
The data preprocessing is an optional step. It applies
to data which are characterized by high levels of
noise and the containment is achieved by using the
appropriate filters. So, it is usual that before the
registration a re-sampling of one or both data sets
that have the same discretionary analysis is needed.
Thus in the subsystem an appropriate technique for
re-sampling is incorporated (
Unser, 1993). The data
pre-processing subsystem includes the segmentation
technique as developed. In this case, anatomical
information is extracted from the two data sets (for
example the external surfaces of the skull from both
CT and MR scanners), which is then used to perform
the registration.
2.2.1 Pre-processing Techniques
The acquired 3D data may include noise and/or
characterized by heterogeneous background. This
noise is undesirable and should be removed, without
the loss of significant anatomical information
contained in images. For noise reduction, suitable
filters are implemented to improve the quality of
images, which are applied on section based (two-
dimensional problem - 2D) (Gonzalez, 1993).
Specifically, within the subsystem the following
filters have been implemented to improve image
quality:
Mean filter: It is a low-pass filter which reduces
high-frequency noise in an image.
Median filter: it is another filter for noise
containment.
Gamma correction: The factor γ determines the
function which distributes the values of pixels,
according to the intensity of brightness of the
screen. The factor γ is equal to one when there
is a linear relationship between pixel values
and intensity of brightness. Images that appear
darker usually require the factor γ have values
larger than one, while those which appear
bright usually require the factor γ have values
smaller than one.
Histogram Equalization filter: it is a commonly
used technique for better visualization of the
diagnostic information of an image. In cases
where the biological tissue of interest shows
rates (different levels of gray), which vary
between certain limits in the digital image, the
visualization of the tissue is significantly
enhanced if the function which corresponds
the values of pixels in the image with
brightness in screen changes.
Adjust brightness and contrast: It is one of the
most basic functions for image editing. The
implementation of this subsystem provides the
opportunity to change the brightness and
contrast of images by the simple linear
transformation:
(
)
(
)
byxaIyxI +
=
,,'
(1)
Where I(x,y) is the pixel of the initial image with
coordinates (x,y) and I’(x,y) is the pixel of the
adjusted image.
2.3 Medical Data Alignment Subsystem
In many cases in the current clinical practice it is
desirable to combine information provided by two or
more imaging modalities or to monitor the
development of a treatment based on data collected
at different times by the same modality. In
particular, when monitoring the development of a
treatment, it is very often the imaging anatomical
structures displayed in two sets of data that have
been collected at different times to be characterized
by geometrical movements, revolutions, etc. It is
necessary to find an appropriate geometric
transformation, which achieves the spatial
coincidence of anatomical structures of the two
images. This process of finding the transformation is
called registration.
The medical data alignment subsystem consists
of a set of techniques for 3D registration of brain
data on surface based or using the levels of gray
(gray-based). Particular attention has been given to
the design of the automatic registration techniques.
Alternatively, there is the option of manual
registration using appropriate surface driving points
as selected by the expert.
Within the design of this subsystem three
registration techniques were implemented:
Automatic registration based on surfaces,
Automatic registration based on gray levels and
DIAGNOSIS - A Global Alignment and Fusion Medical System
23

Manual registration.
2.3.1 Surface-based Registration Technique
This technique is automatic and based on the spatial
matching of segmented anatomical structures of data
from different imaging modalities (Matsopoulos,
2003).
The basic stages of the automatic method for
surfaces registration include:
Surface Pre-alignment. The stage of pre-
alignment includes the spatial displacement of
two triangulated surfaces, so that the centres
of mass coincide. Also, a transformation of
scale in each axis is done separately, based on
the voxel sizes of the two images
(Matsopoulos, 2000).
Geometric transformation application. The
second phase implements an overall geometric
transformation. Its parameters are calculated
by optimizing a function that quantifies the
spatial matching of a triangulated surface of
the reference image (computer tomography -
CT) and the modified image (MRI - MRI).
Four models of geometric transformation in
three dimensions, are explored and evaluated
based on the final results of the registration
(Van den Elsen, 1993).
Matching function definition. The registration
can be seen as the optimization of a Measure
of Match - MOM according to the variables of
the selected transformation. At the case of
surfaces matching an appropriate matching
function is the average of the geometric
distance between the transformed points of the
magnetic scanner data and the corresponding
closest points of computer scanner data.
2.3.2 Registration Based on Gray Levels
This data registration technique is based on the
automatic spatial identification of data from
different imaging systems and is applied on image
values directly, without the prior requirement for
segmenting common anatomical structures (Kagadis,
2002).
2.3.3 Manual Registration
In the case of the manual registration method, the
expert selects points in the respective sections of the
two imaging modalities and the registration of the
data is based on the selection of a particular
geometric transformation (Maurer, 1997). This
method has been developed so that its performance
can be compared to the performance of the proposed
automatic registration methods.
2.4 Medical Data Fusion Subsystem
Medical data fusions scope is to combine
information from different modalities, after the
application of the medical image registration
process. The fusion subsystem is designed
appropriately to allow the composition of anatomical
information from the aligned medical data using
techniques such as the pseudo-colour scale, logic
functions for the diverse overlay of image parts on
another image and change the degree of
transparency in the overlay of anatomical structures
(Matsopoulos, 2008).
2.4.1 Fusion Techniques
Within the proposed system, the following
techniques for medical data fusion, were developed
and applied after registration:
Implementation of logical functions for the
diverse parts overlay of one image on the
other. Specifically, after the data registration,
the anatomical information derived from data
of the CT Scanner overlays on the respective
aligned sections of the MR scanner in order to
fuse the information from the two imaging
systems. This process is mathematically
standardized with the logical operator
Exclusive Or (XOR), which is implemented as
follows:
(
)
(
)
(
)
(
)()()
yxMyxIyxMyxIyxI
BA
,,,1,, +−=
(2)
where Ι
Α
and Ι
Β
the reference image and the
image to align respectively and Μ is the mask
that has value 1 at the pixels that overlay from
both the Ι
Β
to the Ι
Α
. The mask Μ may be the
segmented structure of interest of the Ι
Β
image
that has to be visualized from the reference
system of Ι
Α
, or repeated normalized
geometric shapes, where the aim is to visually
confirm the accuracy of the registration of Ι
Β
relatively to Ι
Α
.
In the pilot study, information from the CT
scanner was isolated and was inserted in the
aligned data of the magnetic scanner using
logic functions (XOR). This fusion method
allows the expert – a doctor to assess the
accuracy of the registration method, while it
gives information on the position of the bones
from the computer tomography in comparison
with other soft tissues or tumors, as shown in
MR.
HEALTHINF 2010 - International Conference on Health Informatics
24

Ability to change the degree of transparency ‘a’
during the overlay of anatomical structures in
order to achieve a combination of information
and assess the quality of the registration result.
This technique was implemented on the basis
of the relationship:
() ()( ) ()
yxaIayxIyxI
BA
,1,, +
−
=
(3)
Fusion of data in 3D is a particularly difficult
problem because the extra dimension makes
the data display difficult even without the
extra complexity of the data fusion. In this
work, a simultaneous demonstration of
common anatomical structures - surfaces
before and after the registration is achieved
using the proposed representation techniques
in the form of VRML.
The results are visualized using pseudo-
coloring according to the medical system used
(e.g. red for the visualization of the anatomical
structure of the axial scanner and blue for the
magnet scanner), to make clear to the expert
the relative position of the two surfaces and
the change before and after the registration
(
Gomes, 1998).
2.5 Graphical Interface Subsystem
The graphical interface subsystem is an important
part of the developed system, as it allows the final
user use the necessary functions of the registration
software. The subsystem was developed having in
mind the following requirements:
Ease of use and user friendliness,
Speed enforcement functions and
Reliable performance of the software’s
individual applications
(a)
(b)
Figure 2: (a) Selection of registration parameters (b)
Selection of the fusion parameters and implementation of
the fusion settings.
The key features of the graphical interface
subsystem include:
Creation of an appropriate graphical
environment: This feature concerns the design
and development of an appropriate interface
that offers: a) easy navigation to the
software’s menus, b) easy access to medical
data and c) a clear definition of the integrated
techniques – algorithms.
Visualization of the medical information: An
important feature of the software is the ability
to visualize data and present the results of the
applications and techniques applied in an
comprehensible manner. It provides: a)
visualization of the original medical data, b)
visualization of the data processing results,
particularly the results of automatic
registration methods and c) visualization of
the fusion of information from the registration.
In particular it allows simultaneous display of
relevant medical data (e.g. CT and MR
sections) before and after the registration and
presentation of the fusion results.
Quantification of the registration results:
Beyond the visualization of the registration
and fusion results another important feature is
the presentation of quantitative data. The data
are related to registration results based on
a)specific success criteria and b) on
geometrical differences (displacements and
rotations) of the data to align from the
reference data.
3 WORKING ENVIRONMENT
The user can use the basic components and navigate
to the input and output data using a tree structure
(Figure 3). The tree structure starts from the node of
the project. The project is the main component of the
system. A project consists of source images,
processing settings and output images and can be
saved and retrieved at will without losing the
settings of the user. It is the root of the tree that
represents, while the intermediate nodes and leaves
of the tree represent individual project data or
processing information.
Figure 3: System information data.
DIAGNOSIS - A Global Alignment and Fusion Medical System
25
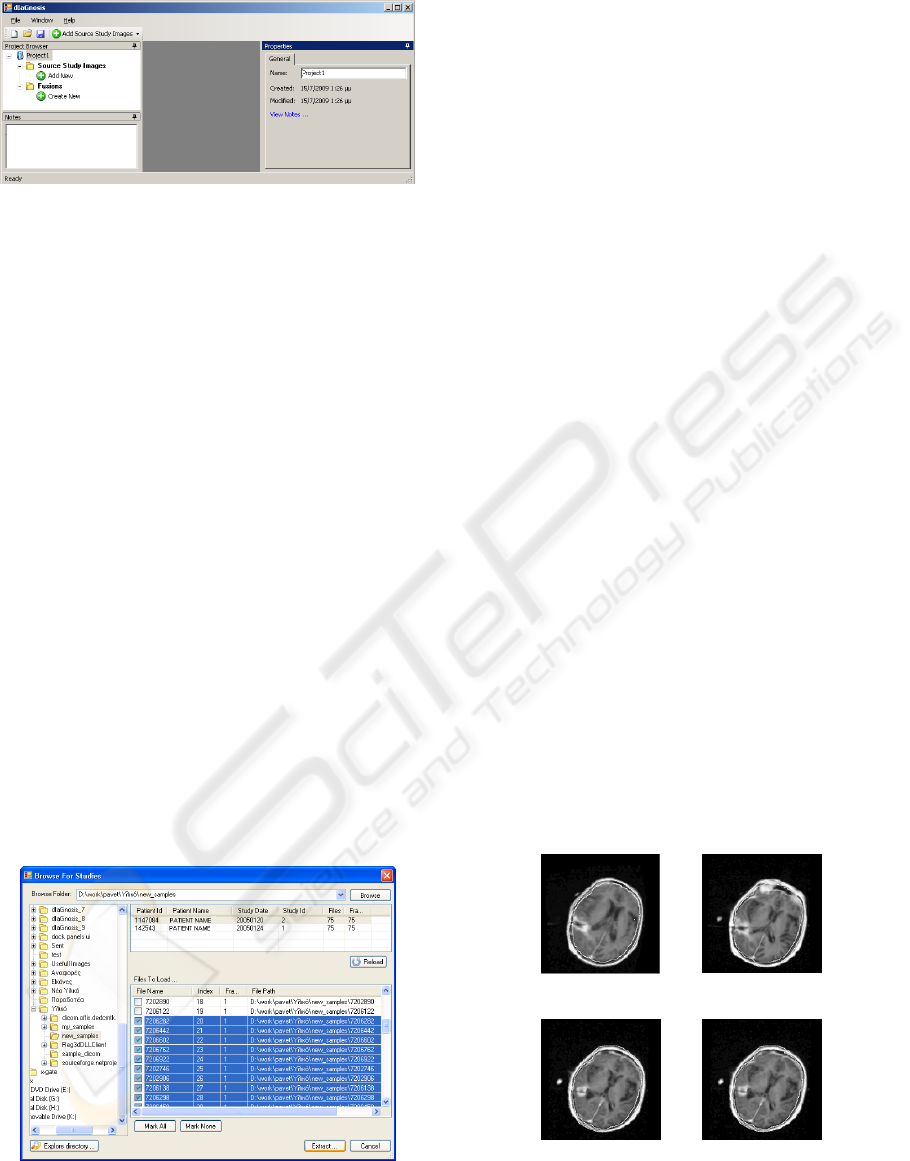
Figure 4: Starting the application.
There are also collection nodes, which group
different snapshots of similar information existing in
each project. Each node, depending on the
information that represents may correspond to a
dynamic description, have associated notes, contain
interfaces presenting information and have
properties that are processed by the user and others.
New nodes can be created by the user and added to
the project while some existing may be removed.
In Figure 4 the general working environment of
the application is shown. The working environment
is dynamic. The user interfaces can be aggregated
into tabs, to activate the automatic concealment
within the window, to match them all together and
more. The user options are saved by closing the
application, and retrieved the next time booted. Also
some templates of the user interface are created and
the user can easily select the one he likes.
The images can be loaded either from an existing
list or with the process of surveying examination
(Figure 5).
As the recovery process of the examining image
from DICOM files may be slow, the system makes
the process to use parallel processing threads.
During the information retrieval the system notifies
the user about the status of recovery and does not
allow access to the node’s data.
Figure 5: Image loading with the process of surveying
examination.
4 PILOT SCENARIO
In order to have an exhaustive testing of the system
a testing scenario was defined. This scenario uses all
the processes supported.
Specifically, the system was installed and
evaluated by an expert-radiologist on the credibility
of the operation and performance of the registration
techniques.
Data sets from axial (CT) and magnetic
tomography (MRI) from 5 patients from
Strahlenklinik of the Stadtische Kliniken Offenbach
of Germany were used. The axial tomography data
were the «Reference data», while the magnetic
tomography data were the «Data to align».
After any registration technique an overlay -
fusion of the CT data on the corresponding sections
of the MRI data took place. In this way, the expert
assessed optically the performance of the
registration techniques.
Figure 6 shows characteristic results of the
registration-fusion techniques using real medical
data. Based on an analysis of these results we came
to the following conclusions:
The performance of the automatic registration
techniques is much better compared to the
semi-automatic alignment technique.
Among the automatic registration techniques
based on gray levels, the technique of mutual
information has better performance compared
to the technique using the correlation
coefficient.
The technique of surface registration is worse
compared to the technique using mutual
information and is almost equivalent to the
technique using the correlation coefficient.
(a)
(b)
(c)
(d)
Figure 6: Registration results using (a) Automatic
registration using correlation coefficient. (b) Automatic
surfaces registration (c) Automatic registration using
mutual data coefficient. (d) Semi-automatic registration
technique.
HEALTHINF 2010 - International Conference on Health Informatics
26
4.1 Quantitative Analysis of
Registration Results
The four registration techniques implemented within
the proposed system were further quantitatively
evaluated in terms of accuracy. Towards this
direction, five patients were used forming five pairs
of sets, each set consisting of CT and MRI head data
of the same patient. The accuracy of each
registration technique was measured as the mean
distance of the centers of all the external markers for
each data set before and after registration (in pixels).
The centers of the external markers were obtained
manually by an experienced radiotherapist.
Comparisons on the performance of these
registration techniques based on this criterion are
shown in Table 1.
From the quantitative result in Table 1 it is shown
that all automatic techniques were performed better
than the semi-automatic technique. Furthermore, the
mutual information registration technique was
outperformed from the other two automatic
registration techniques. Finally, the surface and the
correlation coefficient registration techniques were
performed equivalently.
4.2 Three-dimensional Display of
Anatomic Structures
An important factor in the process of medical data
fusion is the ability of the system to visualize the
results of the registration. Specifically, the system
supports the display of the exported external.
Table 1: Registration Techniques comparison.
Data Sets
Registration Techniques
Automatic
Mutual
Information
Automatic
Correlation
Coefficient
Set 1 0.27 ± 0.01 0.59 ± 0.02
Set 2 0.28 ± 0.02 0.67 ± 0.03
Set 3
0.32 ± 0.01
0.80 ± 0.02
Set 4
0.31 ± 0.01
0.61 ± 0.05
Set 5
0.29 ± 0.01 0.46 ± 0.02
Data Sets
Registration Techniques
Automatic –
Surface
Registration
Semi-
automatic
Registration
Set 1 0.60 ± 0.03 1.89 ± 0.37
Set 2
0.63 ± 0.01 1.87 ± 1.21
Set 3
0.49 ± 0.07 1.33 ± 0.07
Set 4
0.50 ± 0.01 0.47 ± 0.00
Set 5 0.43 ± 0.00
0.53 ± 0.04
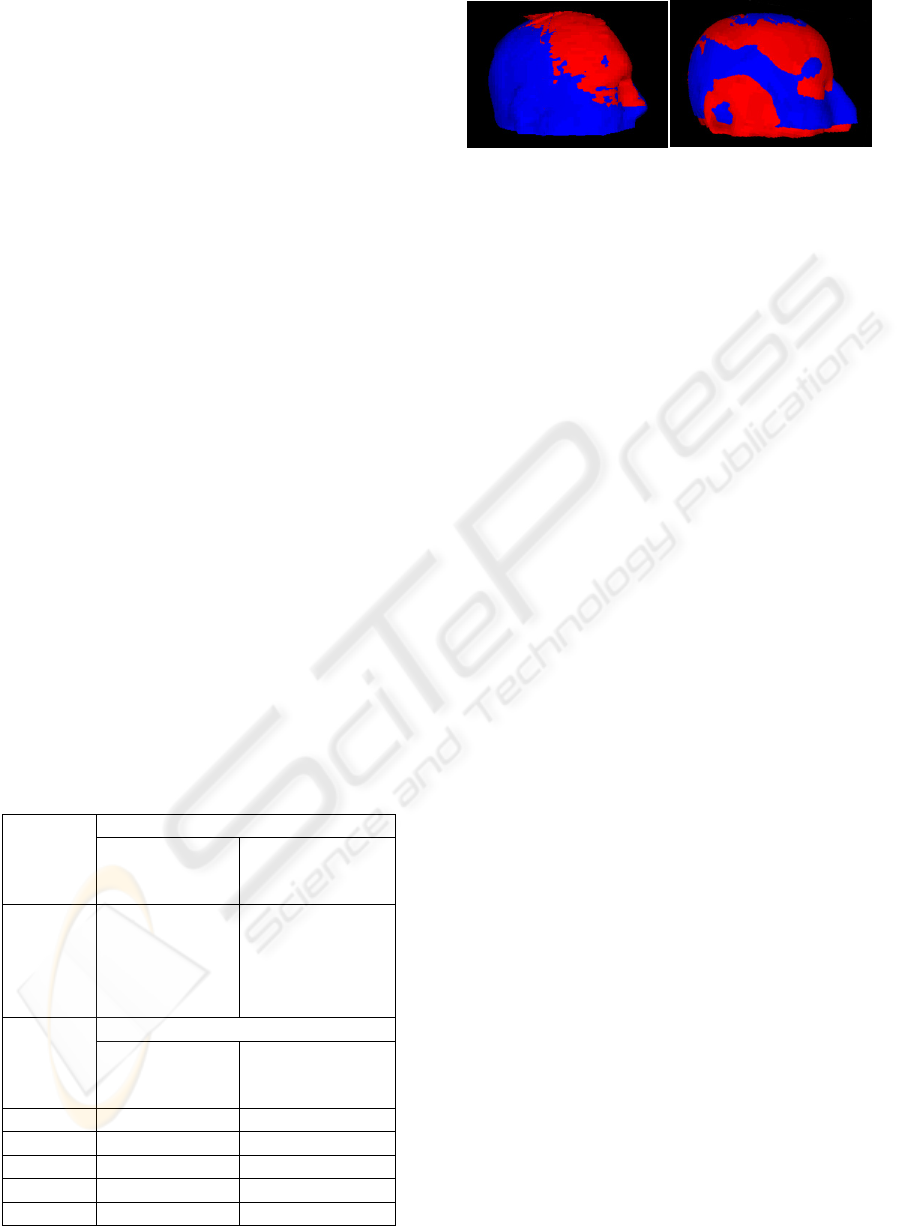
Figure 7: (a) Before registration (b) Registration using the
surface registration method.
anatomical structures - three-dimensional surfaces -
before and after the registration
Furthermore, an indicative visual result of the
overlay of the axial and magnetic scanner surfaces is
presented using VRML and a surface representation
algorithm.
It may be noted that the pre-aligned skin surfaces
are different and the area of the axial tomography is
external and above the area of the MRI. With the
method of surfaces registration the registration
between two surfaces is enhanced, as shown by the
alternation of the two colours of the surfaces.
In Figure 7 we can see the overlay of the skin
surface of the axial tomography (red colour) on the
corresponding surface of the magnetic tomography
(blue colour) for a specific couple using the
algorithm for surface representation in VRML
format.
5 CONCLUSIONS
In this paper we have illustrated our registration-
fusion system in detail, described the algorithms
used and shown the basic scenario of the
application’s usage. Diagnosis is an integrated
environment that facilitates the automatic matching
based on both segmented surfaces and on different
levels of gray and it allows comparison of
registration accuracy for the different techniques
based on specific criteria to quantify registration. It
also improves the registration in case of movement
and / or distortion in the data collection of the
patient from different imaging systems.
After the implementation of the system, a
number of tests were performed for evaluating the
developed registration techniques both qualitatively
and quantitatively in order to test the stability and
accuracy of the techniques. As for future work, we
plan to extend our system by developing further
fusion and registration techniques. Additionally,
more tests will be conducted to support the
efficiency of the implemented system.
DIAGNOSIS - A Global Alignment and Fusion Medical System
27

REFERENCES
J. B. A. Maintz and M. A. Viergever, 1998. A survey of
medical image registration, Medical Image Analysis,
vol. 2, no. 1, pp.1–36,
J.V. Hajnal, D.L.G. Hill, and D.J. Hawkes, 2001. Medical
image registration, CRC Press.
D.J. Hawks, D.L.G. Hill, and E.C.M.L. Bracey, 1992.
Multi-modal data fusion to combine anatomical and
physiological information in the head and the heart, in
J.H.C. Reiber and E.E. Van der Wall (Eds.):
Cardiovascular Nuclear Medicine and MRI, Kluwer
Academic Publishers, Dordrecht, The Netherlands, pp.
113-130.
2006, Digital Imaging and Communications in Medicine
(DICOM) Part 1: Introduction and Overview. National
Electrical Manufacturers Association.
Unser M, Aldroubi, Eden M. B-Spline, 1993. Signal
processing: Part II – Efficient design and applications.
IEEE Trans. Signal Proc.; 2: 834-83-1000.
Gonzalez RC, and Woods RE, 1993. Digital image
processing, Addison Wesley, Second Edition,
G.K. Matsopoulos, K.K. Delibasis, N.A. Mouravliansky,
P.A. Asvestas, K.S. Nikita, V.E. Kouloulias, N.K.
Uzunoglu, 2003. CT-MRI Automatic Surface-based
Registration Schemes Combining Global and Local
Optimization Techniques, Technology and Health
Care: Official Journal of the European Society for
Engineering and Medicine, vol. 11, no. 4, pp. 219-232.
Matsopoulos G.K., Delibasis K.K., Mouravliansky N.,
Nikita K.S, 2000. A Combination of Global and
Elastic Transformations for the Automatic Medical
Surface Registration. Scattering Theory and
Biomedical Technology: Modelling and Applications.
C.V. Massalas, G. Dassios, K. Kiriaki, D. Fotiades, A.
Payatakes (Eds.), pp. 250-264, World Scientific
Publishing Co., Inc., River Edge, NJ, USA (ISBN 981-
02-4391-X).
Van den Elsen PA, Pol EJD, Viergever MA. 1993.
Medical image matching—a review with
classification. IEEE Engng Med Biol; 12: 26-39.
G.C. Kagadis, K.K. Delibasis, G.K. Matsopoulos, N.A.
Mouravliansky, P.A. Asvestas, G.C. Nikiforidis, 2002.
A Comparative Study of Surface- and Volume-based
Techniques for the Automatic Registration between
CT and SPECT Brain Images, Medical Physics, vol.
29, no. 2, pp.201-213
Maurer C. R., Fitzpatrick J. M., Wang M. Y., Galloway R.
L., Maciunas R. J. and Allen G. G., 1997. Registration
of head volume images using implentable fiducial
markers, IEEE Trans. Med. Imag.; 16: 447-462.
G.K. Matsopoulos, 2008. Automatic Correspondence
Methods Towards Point-based Medical Image
Registration: An Evaluation Study, Chapter 26, in
“Handbook of Research on Advanced Techniques in
Diagnostic Imaging and Biomedical Applications”,
edited by T. Exarchos, IGI Global publication, pp.
407-425, (ISBN (ISBN 978-3-540-78870-6).
J. Gomes, L. Darsa, B. Costa, and L. Velho, 1998.
Warping and Morphing of Graphical Objects, in Computer
Graphics, The Morgan Kaufman Series.
HEALTHINF 2010 - International Conference on Health Informatics
28
