
A NOVEL EVALUATION MODEL OF USER ACCEPTANCE OF
SOFTWARE TECHNOLOGY IN HEALTHCARE SECTOR
Noor Azizah K. S. Mohamadali and Jonathan M. Garibaldi
Intelligent Modelling and Analysis (IMA) Research Group
School of Computer Science, University of Nottingham, NG8 1BB, U.K.
Keywords:
Evaluation model, User acceptance, IS success model, UTAUT model, Task-technology fit.
Abstract:
Effective evaluation of healthcare information systems is necessary in order to ensure systems adequately
meet the requirements and information processing needs of the users and healthcare organisations. A number
of studies have proposed evaluation frameworks to aid in evaluation work. However, some of them can be
improved upon. This paper proposes a novel evaluation model to evaluate user acceptance of software tech-
nology within the healthcare sector. It describes the theoretical basis behind the development of the research
model and methodology being employed to validate the model.
1 INTRODUCTION
Information systems play an increasingly important
role in developing the structure and functions of
healthcare industry. Almost a billion dollars are be-
ing spent on the procurement of new technology with
the aim to improve organization performance as well
as the quality of service delivered to the patient. Any
new system implemented is estimated to take approx-
imately 18 months to be fully operationalized (Lee
et al., 2008). Although technology often brings ben-
efits to an organization, sometimes implementations
do fail due to low levels of user acceptance (Southon
et al., 1999). Since the success or failure of system
implementation largely depends on user acceptance
of technology, much research has been carried out to
identify those critical factors that influence user ac-
ceptance (Yusof et al., 2008; Shaw, 2002; Despont-
Gros et al., 2005; Schaper and Pervan, 2007). Some
authors have proposed frameworks to assist evalua-
tion. However, we believe most of these frameworks
can be improved upon. In this paper, we propose a
novel evaluation model to evaluate user acceptance of
technology. The theoretical significance of this work
is that it will use well-established theory in informa-
tion systems to inform the proposed model.
2 THEORETICAL BACKGROUND
In order to build the evaluation model, the following
three-step methodology was adopted:
• A general review of existing information system
models to provide a theoretical basis to the key di-
mension of user satisfaction or acceptance of tech-
nology.
• A general review of existing evaluation frame-
works to identify strengths and limitations of each
framework, if any, to identify improvements.
• A general review of information system evalua-
tion studies in healthcare to highlight studied vari-
ables on user acceptance of technology.
2.1 Review of Theories of User
Acceptance of Technology
There are a number of theories that focus on user ac-
ceptance of technology such as the technology accep-
tance model (Davis, 1989), the theory of reasoned
action, the IS Success Model (DeLone and McLean,
2003), the diffusion of innovation theory, the Unified
Theory of Technology Acceptance and Use of Tech-
nology (Venkatesh et al., 2003) and many other re-
lated theories. Here, we discuss three theories that we
believe are relevant to our research problem.
392
Azizah K. S. Mohamadali N. and Garibaldi J. (2010).
A NOVEL EVALUATION MODEL OF USER ACCEPTANCE OF SOFTWARE TECHNOLOGY IN HEALTHCARE SECTOR.
In Proceedings of the Third International Conference on Health Informatics, pages 392-397
DOI: 10.5220/0002695703920397
Copyright
c
SciTePress

2.1.1 DeLone and McLean IS Success Model
Since its introduction by (Delone and McLean, 1992),
the model has been widely used, evaluated, validated
and extended in various studies. In 2003, the IS Suc-
cess Model was updated by inclusion of net bene-
fits derived from intention to use and user satisfac-
tion (DeLone and McLean, 2003). The IS Success
Model illustrates clear, specific dimensions of success
or effectiveness and the relationships between the fac-
tors. Dimensions suggested are system quality, infor-
mation quality, service quality, intention to use, ac-
tual use, user satisfaction and net benefits. (Petter and
McLean, 2009) in his paper has given a detailed de-
scription of each of the constructs. However, the lim-
itation of this model is that it cannot provide expla-
nation as to why the same IT system can be adopted
in different ways, with different effects in various set-
tings (Tsiknakis and Kouroubali, 2008).
2.1.2 Unified Theory of Technology Acceptance
and Use of Technology (UTAUT)
(Venkatesh et al., 2003) proposed a more complete
model for understanding the acceptance and adoption
of information technology. The UTAUT model con-
tains four core determinants of intention and usage,
while also incorporating moderating variables, gen-
der, age, experience and voluntariness of use, which
may or may not have an influence on user acceptance
of technology. A description of the constructs defined
by the model are as follows:
• Performance expectancy — “The degree to which
an individual believes that using the system will
help him or her to attain gains in job performance.
Measured such as accomplish task quickly, im-
prove job performance, increase productivity, en-
hance effectiveness.”
• Effort expectancy — “The degree of ease associ-
ated with the use of system. Measured such as
interaction with system clear and understandable,
flexible to iteract, easy to use, etc.”
• Social influence — “The degree to which an indi-
vidual perceive that important others believe he or
she should use the new system.”
• Facilitating condition — “The degree to which an
individual believes than an organization and tech-
nical infrastructure exist to support the use of a
system.”
The UTAUT model is a relatively new model and
to our knowledge it has not been widely used in the
healthcare domain. Thus, this model will be utilized
in understanding user acceptance of technology in
healthcare domain.
2.1.3 Task-technology Fit (TTF)
Task-technology fit model was developed by (Good-
hue, 1995). TTF theory holds that information tech-
nology is more likely to have a positive impact on its
individual performance and be used if the capabilities
of the technology match the tasks that the user must
perform. The importance of task fit and technology
has been highlighted in many studies (Ammenwerth
et al., 2006; Goodhue et al., 2000; Goodhue, 1995).
The fit between attributes to accomplish certain tasks
is more important that the individual attributes them-
selves. For example, a user with certain IT skills is not
a sufficient requirement for the use of a new system;
rather their skills must be match with the requirement
of the IT system itself (system complexity). In addi-
tion to the fit defined by the model, we believe there
must exist also a fit between the individual and the
organisation. For example, if a particular individual
does not possess the skill to use a new technology,
the organisation needs to provide necessary training.
This will eventually influence the user to accept the
technology. Thus, other than the fit between individ-
ual and organisation, the fit between organisation and
technology is also equally important and we include
this additional fit in our model.
2.1.4 Observation and Recommendation
Both the IS Success Model and the UTAUT model by
itself is an excellent model. Each is internally sound
and based directly on well-tested attitude/ behaviour
models. Both models define almost similar depen-
dant constructs, where in IS Success Model it is called
‘intention to use’ or ‘use’, whereas in the UTATUT
model it is called ‘behavioural intention’. However,
for this dependant construct, each model defines dif-
ferent independent constructs. For example, in the
UTAUT model, behavioural intentions are determined
by performance expectancy, effort expectancy and so-
cial influence. In the IS Success Model, intention to
use or use is determined by information quality, sys-
tem quality and service quality. We believe that, by
combining all these independent factors, we can bet-
ter represent factors that determine intention to use
or behavioral intention of the user of the system. As
observed also, the weakness of the existing models
is in their lack of task focus (fit) between various
constructs, which contributes to the mixed results in
information technology evaluations studies (Dishaw
and Strong, 1999). Thus, instead of proposing TTF
as an alternative to the IS Success Model or UTAUT
model, we propose to add the strengths of TTF mod-
els to the IS Success Model and UTAUT model to
produce an integrated model which incorporate both
A NOVEL EVALUATION MODEL OF USER ACCEPTANCE OF SOFTWARE TECHNOLOGY IN HEALTHCARE
SECTOR
393

attitudes toward information technology and the fit
between technology functionality and the character-
istics of the tasks that users need to accomplish with
the technology. We believe that these three models
overlap in a significant way and, if integrated, it could
provide a better explanation of information technol-
ogy utilization by the users and also a stronger model
than any stand alone model.
2.2 Observation on Early Study of
Existing Evaluation Frameworks
In this section, we briefly analyze several existing
evaluation frameworks. Most of the frameworks were
developed based on influences from other disciplines
(Chiasson et al., 2007).
• ICT and OTs: A model of information and com-
munication technology acceptance and utilisation
by occupational therapists (Schaper and Pervan,
2007). The framework was developed to exam-
ine acceptance and utilisation issues among health
professionals and was based on the UTAUT model
by (Venkatesh et al., 2003) and ‘Technology Ac-
ceptance (TAM)’ by (Davis, 1989). However, de-
scription of task charateristics is lacking in this
model. We believe on the importance of task char-
acteristics and skills that user possess will eventu-
ally influence users’ usage of the technology and
this must be evaluated when we address user ac-
ceptance of technology.
• Understanding IT: acceptance by individual pro-
fessional: Towards an integrating view (Yi et al.,
2006). The framework was based on the TAM
model by (Davis, 1989), planned behavior and
innovation diffusion. This research model was
tested in the context of personal digital assistance
acceptance by healthcare processionals. We be-
lieve that the important factor which is the fit be-
tween the technology and the task that the user
needs to perform is important and this fit is lack-
ing in this model.
• HOT-fit: An evaluation framework for health
information systems: human, organization and
technology-fit factors (Yusof et al., 2008). The
proposed framework is constructed so that it is
capable of being useful in conducting a thorough
evaluation study and to help researcher and practi-
tioners to understand the perceived complexity of
health information system evaluation. The model
was developed based on the IS Success Model
and the ‘IT-Organization fit model’. The strength
of this model is inclusion of fit element. How-
ever, we believe more constructs from the UTAUT
model can be incorporated into this model to bet-
ter explain user acceptance of technology.
• FIIT: Fit between Individual, technology and
Task by (Ammenwerth et al., 2006). This pro-
posed framework was believed to provide better
analyses on socio-organizational-technical factors
that influence IT adoption during implementation.
The model referred to the IS Success Model, the
TAM model and the IT adoption model. Inclusion
of several constructs from UTAUT model, includ-
ing moderating factor, can (we believe) further en-
hance the applicability of this model.
Based on our early observations, we believe each of
these frameworks can be improved upon to address
the issue of user acceptance of technology.
3 THE PROPOSED INTEGRATED
EVALUATION MODEL
The following proposed evaluation framework is de-
veloped after studying the existing models and theory
of user acceptance of technology, and following crit-
ical appraisal of the existing evaluation frameworks.
Three models were integrated to build this model as
shown in Figure 1. The features of this integrated
model are:
• Categorisation of all the independent constructs
under Individual, Organizational and Technology
context.
• The individual factors and their dimensions are
performance expectancy, effort expectancy and
social influence. These are constructs defined in
the UTAUT model.
• The organisational factor and its dimension is fa-
cilitating condition, from the UTAUT Model.
• The technology factors and their dimensions are
system quality, information quality and service
quality. These are constructs defined in the IS
Success Model
• Incorporation of fit between individual, organi-
sational and technology context. In the original
TTF model, the fit is between task (individual)
and technology. In addition to this, we include
fit between individual and organisation, and be-
tween technology and organisation, which we be-
lieve are also equally important.
HEALTHINF 2010 - International Conference on Health Informatics
394

Table 1: Classification of the Factors Associated with the Adoption of New Technology.
Factors/Constructs Measurement Variable Sources
Performance
Expectancy
Work Quicker, Improve Quality of work, Improve communication,
will use if offer advantages, save time, information exchange, clear
interaction and understandable, easy to use, multi-tasking, improved
work effectiveness, etc.
1, 2, 3, 4, 6,
11
Effort Expectancy Clear, easy to remember, always available, easy to use, usability, has
knowledge to use, improve job performance, enhance job effective-
ness, increase job productivity, user-friendly etc.
3, 4, 5,6, 7, 8,
9, 10
Social Influence Perception of other, usage benefits social factors, social words, at-
mosphere, etc.
7, 11
Information Quality Relevance and usefulness, efficiency, conciseness and completeness,
reliability, observability and result demonstrability, accurate infor-
mation, content, format
10,11, 12
Service Quality Helpdesk support, user documentation, quality of hotline, support,
speed to repair
5, 7
System Quality Speed, response time, provide security, downtime, response time,
require multiple update, stability and usability, data accuracy, data
availability, flexibility, reliability, functionality, connection time, sys-
tem function, content design and device accessibility, etc.
3, 5, 6, 8, 9,
11, 12, 13
Facilitating
Condition
Management support, training, provision of computer support (hard-
ware, software), system availability, network infrastructure, security,
compatibility of technology or technical issues/ appropriateness of
technology implemented, helpdesk, maintenance, support from IS
department, support from vendor, technical support, induction, etc.
2, 5, 6, 7, 8, 9,
13, 14, 15
User Satisfaction Task-support satisfaction, quality of work-life satisfaction, interface
satisfaction, decision-making satisfaction, software satisfaction, sat-
isfaction with system components
2, 12
Net Benefits Improve task performance, efficiency and effectiveness (goal
achievement), error reduction
12
Moderating Factors Experience, age and gender 2, 6, 9, 11, 14,
15
3.1 Classification of Factors: Individual,
Organizational, Technology
According to (Chau and Hu, 2002), technology ac-
ceptance has three dimensions:
1. characteristics of the individual;
2. characteristics of the technology; and
3. characteristics of organisational context.
Several evaluation frameworks categorise factors un-
der these three wide categories (Schaper and Pervan,
2007; Yusof et al., 2008; Lorenzi, 1999). Organisa-
tion factors need to be evaluated because introduction
of new information technology changes the services,
operation and also the structure of the organisation it-
self. Technology needs to be evaluated because it be-
comes part of the system within the organisation in
which it operates. The user or individual is mainly
subjective because they imply how people conceive
their relationship with the technology, and individual
also needs to be evaluated (Southon, 1999).
3.2 Validation of Proposed Evaluation
Model: Phase 1 (Literature Review)
In phase one of our research, in order to validate the
proposed model, we conducted a literature review to
identify factors associated with the adoption of new
technology. All these factors are collected and classi-
fied according to the constructs defined in our model
to test if our defined constructs can incorporate these
factors and we managed to classify the identified fac-
tors. Table 1 shows the classification of the factors
identified from this review. This indicates that most
of the factors associated with user acceptance of tech-
nology can be represented by our model. This demon-
strates the strength and applicability of our proposed
model.
A NOVEL EVALUATION MODEL OF USER ACCEPTANCE OF SOFTWARE TECHNOLOGY IN HEALTHCARE
SECTOR
395
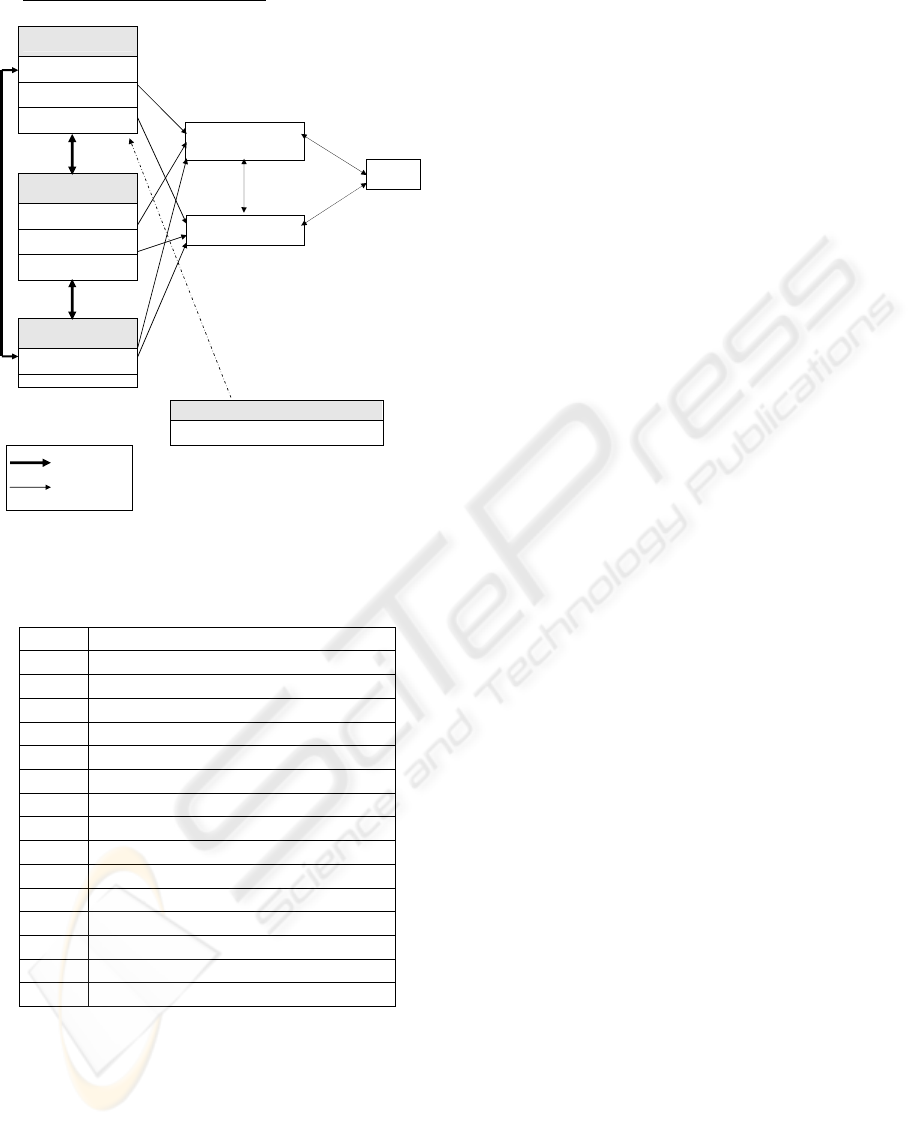
1
Integrated Model of User Acceptance of Technology
Individual/ People
Factor
Performance Expectancy
Effort Expectancy
Social Influence
Technology Context
Information Quality
Service Quality
System Quality
Organizational Context
Facilitating Condition
Culture /newly added
Moderating Factors
Age, Gender, Experiences and Voluntariness
Behavioural Intention /
Intention to Use / Use
Behaviour
Net
Benefits
User Satisfaction
Fit
Influence
Figure 1: Proposed Evaluation Model of User Acceptance
of Technology.
Table 2: Reference to Sources.
Key Sources
1 (Otieno et al., 2008)
2 (Despont-Gros et al., 2005)
3 (Tsiknakis and Kouroubali, 2008)
4 (Yi et al., 2006)
5 (Shaw, 2002)
6 (Garfield, 2005)
7 (Martens et al., 2008)
8 (Sicotte et al., 2006)
9 (Ammenwerth et al., 2006)
10 (Chiasson et al., 2007)
11 (Lee et al., 2008)
12 (Yusof et al., 2008)
13 (Heeks, 2006)
14 (Mahmood et al., 2000)
15 (Goodhue et al., 2000)
3.3 Validation of Proposed Model:
Phase 2 (Case Study Strategy)
In phase two of our study, in future, a case study strat-
egy will be employed. The case study will serve two
purposes:
1. to evaluate the adoption factor of new technology
in the context of the phenomena under study;
2. to validate the proposed evaluation model.
A case study will be conducted within the clinical
setting with research students from the Breast Can-
cer Pathology Research Group, based in the Queen’s
Medical Centre, Nottingham. This research centre
has recently purchased a new piece of software known
as Distiller (SlidePath, 2008). The model will be
used as a guideline in the evaluation of this software.
During the evaluation process, we will interview the
users, observe their use of the system and also per-
form document analysis.
4 CONCLUSIONS AND FUTURE
WORK
In this paper, we have proposed an evaluation model
to evaluate user acceptance of software technology
in the healthcare sector. Our proposed model in-
tegrates three very well-known theories of informa-
tion systems to represent factors that influence user
acceptance of software technology. In first phase
of the study, we conducted a literature review to
identified factors associated with the user acceptance
of the technology. These factors were then clas-
sified according to the constructs proposed in our
model. Through this process, we demonstrated that
our model can better represent factors associated with
technology acceptance. As future work, in order to
further validate our model, we will test the model in
clinical settings with research students by means of a
case study. Findings from fieldwork will (hopefully)
be used to further improve and refine the model. Iden-
tifying what are the factors that influence successful
implementation of new software technology among
the users is vital since the success and failure of any
new systems to operate in a new environment depends
largely on the acceptance of the users of the system.
ACKNOWLEDGEMENTS
Noor Azizah KS Mohamadali would like to grate-
fully acknowledge the funding received from both the
Public Service Department of Malaysia and from the
International Islamic University of Malaysia that is
helping to sponsor this research.
REFERENCES
Ammenwerth, E., Iller, C., and Mahler, C. (2006). It-
adoption and the interaction of task, technology and
HEALTHINF 2010 - International Conference on Health Informatics
396

individuals: a fit framework and a case study. BMC
Medical Informatics and Decision Making, 6:1–13.
Chau, P. Y. K. and Hu, P. J.-H. (2002). Investigating helath-
care professionals’ decisons to accept telemedicine
technology: an empirical test of competing theories.
Information and Management, 39:297–311.
Chiasson, M., Reddy, M., Kaplan, B., and Davidson, E.
(2007). Expanding multi-disciplinary approaches to
healthcare information technologies: What does infor-
mation systems offer medical informatics? Interna-
tional Journal of Medical Informatics, 76s:S89–S97.
Davis, F. D. (1989). Perceived usefulness, perceived ease of
use, and user acceptance of information technology.
MIS Quarterly, 13:319–339.
Delone, W. H. and McLean, E. R. (1992). Information sys-
tems success: The quest for the dependent variable.
Information Systems Research, 3:60–95.
DeLone, W. H. and McLean, E. R. (2003). The delone
and mclean model of information systems success: A
ten year update. Management Information Systems,
19(4):9–30.
Despont-Gros, C., Mueller, H., and Lovis, C. (2005). Eval-
uating user interactions with clinical information sys-
tems: A model based on human-computer interaction
models. Journal of Biomedical Informatics, 38:244–
255.
Dishaw, M. T. and Strong, D. M. (1999). Extending the
technology acceptance model with task-technilogy fit
constructs. Information and Management, 36:9–21.
Garfield, M. J. (2005). Acceptance of ubiquitous comput-
ing. Information Systems Management, 22:24–31.
Goodhue, D. L. (1995). Understanding user evaluation of
information systems. Management Science, 41:1827–
1844.
Goodhue, D. L., Klein, B. D., and March, S. T. (2000).
User evaluation of is as surrogates for objective per-
formance. Information and Management, 38:87–101.
Heeks, R. (2006). Health information systems: Failure, suc-
cess and improvisation. International Journal of Med-
ical Informatics, 75:125–137.
Lee, T.-T., Mills, M. E., Bausell, B., and Lu, M.-H. (2008).
Two-stage evaluation of the impact of a nursing in-
formation system in taiwan. International Journal of
Medical Informatics, 77:698–707.
Lorenzi, N. M. (1999). Imia working group 13: organi-
zational impact of medical informatics. International
Journal of Medical Informatics, 56:5–8.
Mahmood, M. A., Burn, J. M., Gemoets, L. A., and
Jacquez, C. (2000). Variables affecting information
technology end-user satisfaction: a meta-analysis of
the empirical literature. International Journal of Hu-
man Computer Studies, 52:751–771.
Martens, J. D., van der Weijden, T., Winkes, R. A. G.,
Kester, A. D. M., Geerts, P. J. H., Evers, S. M. A. A.,
and Severens, J. L. (2008). Feasibility and accept-
ability of a computerised system with automated re-
minders for perscribing behaviour in primary care. In-
ternationa Journal of Medical Informatics, 77:199–
207.
Otieno, G. O., Hinako, T., Motohiro, A., Daisuke, K., and
Keiko, N. (2008). Measuring effectiveness of elec-
tronic medical records systems: Towards buidling a
composite index for benchmarking hospitals. Interna-
tional Journal of Medical Informatics, 77:657–669.
Petter, S. and McLean, E. R. (2009). A meta-analytic as-
sessment of the delone and mclean is success model:
An examination of is success at the individual level.
Information and Management, 46:159–166.
Schaper, L. K. and Pervan, G. P. (2007). Ict and ots:
A model of information and communication technol-
ogy acceptance and utilisation by occupational thera-
pists. International Journal of Medical Informatics,
76s:S212–S221.
Shaw, N. T. (2002). Cheats: a generic information commu-
nication technology (ict) evaluation framework. Com-
puters in Biology and Medicine, 32:209–220.
Sicotte, C., Pare, G., Marie-Pierre, and Paccioni, A. (2006).
A risk assessment of two interorganizational clinical
information systems. Journal of the American Medi-
cal Informatics Association, 13:557–566.
SlidePath (2008). Distiller. Available from
http://www.slidepath.com.
Southon, G. (1999). It, change and evaluation: an overview
of the role of evaluation in health services:. Interna-
tional Journal of Medical Informatics, 56:125–133.
Southon, G., Sauer, C., and Dampney, K. (1999). Lesson
from a failed information system initiative: issues for
complex organisations. International Journal of Med-
ical Informatics, 55:33–46.
Tsiknakis, M. and Kouroubali, A. (2008). Organizational
factors affecting successful adoption of innovative
ehelath services: A case study employing the fitt
framework. International Journal of Medical Infor-
matics.
Venkatesh, V., Morris, M. G., Davis, G. B., and Davis, F. D.
(2003). User acceptance of information technology:
toward a unified views. MIS Quarterly, 27:425–478.
Yi, M. Y., Jackson, J. D., Park, J. S., and Probst, J. C.
(2006). Understanding information technology accep-
tance by individual professionals: Towards an integra-
tive view. Information and Management, 43:350–363.
Yusof, M. M., Kuljis, J., Papzafeiropoulou, A., and Ster-
gioulas, L. K. (2008). An evaluation framework for
health information systems: human, organization and
technology-fit factors (hot-fit). International Journal
of Medical Informatics, 77:386–398.
A NOVEL EVALUATION MODEL OF USER ACCEPTANCE OF SOFTWARE TECHNOLOGY IN HEALTHCARE
SECTOR
397
