MENTAL CLONING BASE VIRTUAL DIAGNOSTICIAN
SYSTEM
Virtual Medical Doctor System (VDS) Reasoning
Hamido Fujita, Jun Hakura and Masaki Kurematsu
Iwate Prefectural University, Iwate, 020-0193, Japan
Keywords: Emotional mental reasoning, Human user interaction, Intelligent interface, Ontology integration, UMLS.
Abstract: Human computer Interaction based on emotional modelling and physical views, collectively; has been
investigated and reported in this paper. Two types of ontology have been presented to formalize a patient
state: mental ontology reflecting the patient mental behaviour due to certain disorder and physical ontology
reflecting the observed consequences of such disorder. These two types of ontology have been mapped and
aligned for reasoning purposes. We have constructed an integrated computerized model which reflects a
human diagnostician as computer model and through it, an integrated interaction between that model and
the real human user (patient) is utilized for 1
st
stage diagnosis purposes. The diagnostician knowledge has
been utilized through UMLS for testing, and the integrated mapping of the two views been represented
through OWL framework. The reasoning instantiation is done using Description logic. We have
implemented the system and empirically, examining it, for revision and evaluation.
1 INTRODUCTION
There have been extensive move towards changing
the way health care is delivered, financed and
regulated (Smith, 20009) Medical innovations have
become an important lever inquest of improving
efficiency. The main purpose is to improve the
efficiency so that more patients could receive
treatment more quickly without reducing the quality
of care (Mikkola, 2003). How to cope with a rise in
the need for the elderly care services is a formidable
issue facing all the industrialized countries.
Unfortunately, Japan's health care system has not
been prepared enough to respond to the needs ahead.
Particularly Japan's home care services have heavily
been relying on voluntary labour of family members
with little social services available. The proportion
of the population 65 and over has doubled from 10%
in 1985 to 20% in 2005, and is projected to be 30%
in 2023 (2006, NIPSSR).
In June 2006, the Diet (Japanese Congress)
passed a comprehensive package of reform to make
the delivery system more efficient. First, the average
length of stay in hospitals is to be decreased. To
achieve this goal, the number of long term care
(LTC) hospital beds will be reduced from the 2006
level of 380,000 to 150,000 by the end of fiscal year
2011 and converted to LTC Insurance facility beds
and assisted living (Leflar, 2005). The system
proposed in this paper participates in helping
physicians to manage the diagnosis procedure using
the same knowledge that that physicians have by
copying (mimic) his/her style, mentality, diagnosis
routines and medicine recipes. It is not replacing the
physicians but it would participate to utilize his/her
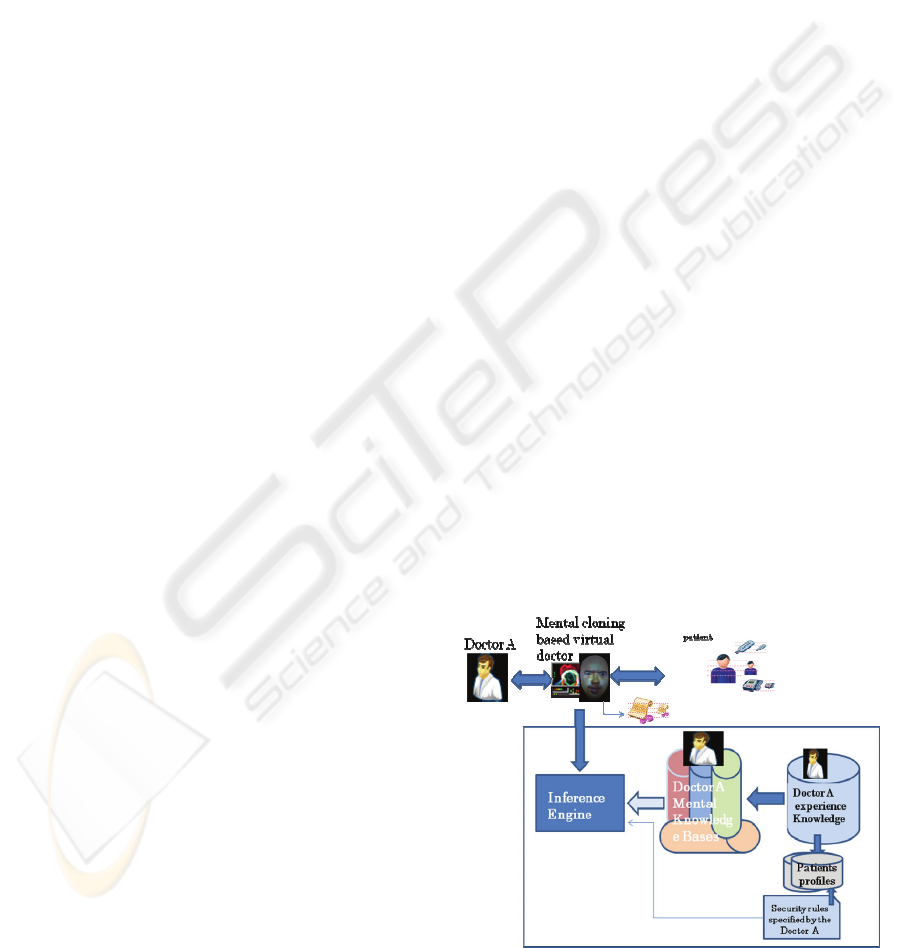
Figure 1: Simple outline of the VDS.
250
Fujita H., Hakura J. and Kurematsu M. (2010).
MENTAL CLONING BASE VIRTUAL DIAGNOSTICIAN SYSTEM - Virtual Medical Doctor System (VDS) Reasoning.
In Proceedings of the Third International Conference on Health Informatics, pages 250-256
DOI: 10.5220/0002717102500256
Copyright
c
SciTePress

Figure 2: The VDS outline.
knowledge for preliminary diagnosis and health care
services for patient for efficiency purpose.
This paper contributes to present part of our
experimental work on building a virtual system
based or what we called as Virtual doctor System
(VDS) Fig.2, to act as a physical or medicinal doctor
for diagnosis purposes. In other paper we have
presented the outline of the interface, and in this
complementary part we are presenting the inference
engine and the ontological integration as in Fig.5.
1.1 System Conceptual Outline
The system we called here as VDS (Virtual Medical
Doctor) (Fig.2) is to work together with the
corresponding medical doctor. So the system (VDS)
and the MD are working together in comprehensive
coherency; the former is complementary to the latter
but not vice versa. The former is to diagnose
outpatient 1
st
and classify these diagnosis into
classes. Simple cases classes that the VDS would
take conclusion and set the diagnosis procedure and
accordingly take action (e.g., issue drugs to the
patient). The overall procedure is supervised by the
medical doctor later on in a report. There are other
cases which the system concludes to have the MD to
participate in the final decision. In such cases, the
system sends the diagnosis reports to the MD and
provides an appointment to the patient in the
Figure 3: VD avatar.
Figure 4: VDS experiment style.
hospital queue. The system reads the queue data at
the management centre of the hospital reception.
And assign the patient to the queue. If the Doctor
found the assignment is appropriate (check mark
OK) then the system learned that the decision is
appropriate, however, by certain feedback from the
doctor the system can learn from the doctor’s
feedback. We provide a window at the doctor office
Bodyweight ・ Temp ・
BloodP
Case and scenario a
cold (92%)
Influenza (83%)
bronchitis (64%)
pneumonia (42%)
A moon-faced woman
cold (38%)
Voice Input
Processing
Image
Processing
Output
Ego gram &
Profile DB
A
sync
h
ronous
management
Emotion
Estimate Processor
Emotion
Transmission
Processor:
From Keywords a
related scenario would
Keywor
Feel Heavy
Fever 38.6℃
Keywords
with
annotated
Wei
g
ht
Emotion Processor
Emotional
Emotion
Scenario Catch Cold
A1:Since when?(92%)
A2:Stomach-ache(83%)
A3:Phlegm?(64%)
Patient
Sensor
Touch Panel
MIC
Camera
Image Processing
Voice Input
Profile Processor
profile management
Mental
Knowledge Base
Action Processor
The decision of the next
behaviour based on the
observed emotion and
Reasonin
Diagnosis Processor
MD Scenario
DB
カ
ルテ
カ
ルテ
Carte
MD-
Personalit
y
Extraction
MENTAL CLONING BASE VIRTUAL DIAGNOSTICIAN SYSTEM - Virtual Medical Doctor System (VDS) Reasoning
251
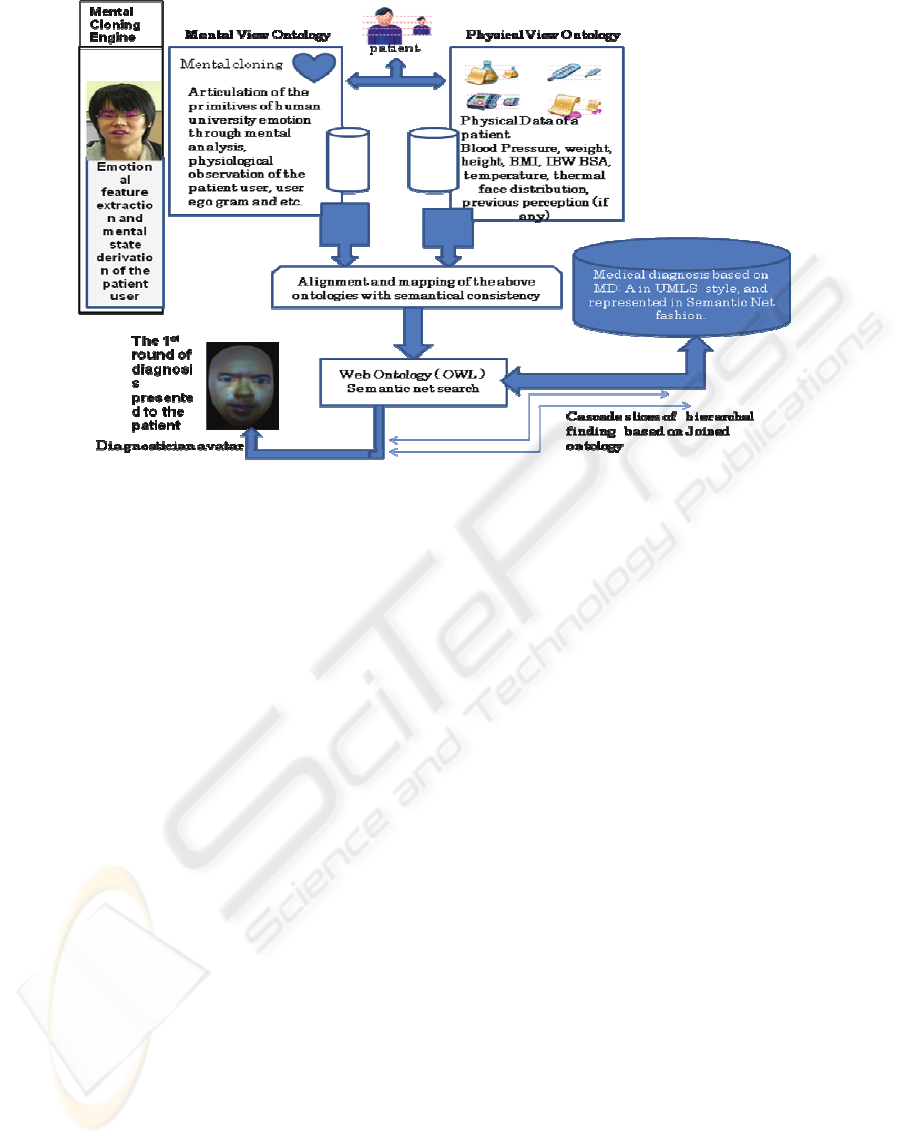
Figure 5: System architecture of the inference engine.
to fill a sheet of evaluation to enforce the learning
procedure for the system. Such evaluation sheet
would provide a learning mechanism to increase the
reasoning procedure for the diagnosis. However
such knowledge management would be based (i.e.,
mimic) on Medical Doctor A, therefore, it would be
stored in knowledge management on the top of the
management system. So when another doctor is
doing the outpatient diagnosis then the profile of
decision making related to that Doctor would be
used (i.e., recalled). So there is a general diagnosis
and on top of it there are diagnosis categorized on
physicians actual practices.
The paper is showing the state of art in making a
system that can interact with human user based on
new concept named as mental cloning at (Fujita
2009). The cloning is based on analysis of human
medical doctor (HMD). The analysis is projected
using his/her observed styles as a person and also as
expert in medical diagnosis related practices. So
there are different style of categorized knowledge
reflecting such representation and related reasoning.
As shown in Fig.2 and Fig.3. The system would
create a virtual face (i.e., screen mask) of an actual
doctor that through it the patient communicates with
pre-assigned virtual version of that medical doctor.
Physical doctor face is masked copied and attached
on manikin (as shown in Fig 4). Inside it there is a
projector that reflects the 3 dimensional generated
images on the mask screen that reflects the actual
facial real-time created images and voices of the
medical doctor namely, Doctor A (Fig. 4). These
animated facial image synchronized with a spoken
language in the same manner as the actual physical
doctor is doing diagnosis practices in Japanese
hospital. The style mimics the actual doctor
emotional expression as well his/her diagnosis Case
and scenario a cold (92%) influenza (83%)
bronchitis (64%) pneumonia (42%) a moon-faced
woman cold (38%) style (Fig.2). Also, the MD
would speak in natural accent with emotions based
on the patient mental mode, estimated by the patient
profile (age, gender, ego data), and his/her situation
automatically measured by data resembles (blood
pressure, body weight, body temperature, and
thermal analyzer).
These devices (equipments) are assembled to a
patient desk chair that the patient would sit on, and
automatically these measurements are collected
and transferred through serial connection to the
virtual doctor system. These physical data are all
measured and send online to the VDS together with
the mental status data (situation) of the user
(patient), with estimated ego state retrieved from
the databases.
This system is been built by a support from
Ministry of Interiors affairs and communications of
Japan under SCOPE project.
2 VIRTUAL DOCTOR SYSTEM
REASONING ENGINE
The paper reports here, part of our project outcome
HEALTHINF 2010 - International Conference on Health Informatics
252

that is related to interaction between VDS avatar and
Patient. The voice recognition issues is been also,
discussed in (Kurematsu, 2009). The action scenario
is to create a diagnosis based on the guidelines given
by the Doctor A. Doctor A is a nominated Doctor
which is the object system would mimic to interact
with patient through VDS avatar. Implementing
medical guidelines of Doctor A in active computer-
based decision participates to enhance the best
practices of medical services on behalf of Doctor A.
Our system reported here briefly, participates to
provide cognitive interaction between real patient
and specialized doctor A (avatar) through computer
interpretable guidelines (CIGs). We have used
UMLS Metathesaurus® for testing purposes (Fig.5).
The contextualization of the two ontologies
specified namely, by the mental ontology and
physical ontology annotated mapping alignment,
that produce annotated search profiling in the
medical knowledge base Unified Medical Language
System (e.g.,UMLS) semantic net. We think this is
compatible with vocabularies and classification used
in patient diagnosis. The combined usage of the two
ontologies is intended (Fig. 5) to derive semantically
appropriate reference to the patient’s status and
correspondingly the appropriate concluded aligned
key words for relative diagnosis search. The
diagnosis retrieval from the knowledge base (i.e.,
UMLS) would be related to the specialization of the
patient case through the combined ontology. This in
turn would lead to derive the validated
correspondence related to patient condition.
We define the structure of classes that are to be used
in the hospital Class patient: as the class that specify
all types of patient in hospital class and can be
attributed by their: Unique assigned number; The
number can have a structure representing a form that
store the profile of that patient and retrieve it when
necessary, and to update it is content. This code
represents the hierarchy of the data structure of
patient ID.
The patient ID file would have information related
to the, personal information, like name, gender, age,
employment type, tallness, address, marital status,
special information and other type of personal
related medical information. This also would
represent the patient module that would have related
information to the mental state of that patient,
his/her physiological state definition (Fujita, 2009).
This would to establish a template that also stored as
part of the patient module structure. Templates
related to mental cloning issues. Like the user ego
gram, his/her universal templates, and six basic
templates of Ekman emotion and the neutral state
(no emotion recognized state) (Fujita, 2008). As part
of the language issues we have defined other modes
that are needed during the diagnosis procedure.
These types of emotional modes are related to the
effect produced due to a certain combination that the
patient would have as a result of disorder or sickness
of different cause or nature. These states can be
specified as pain(x), x would be a percentage values
that to be extracted from the combination of other
observed cognitive state. We have six primitives’
cognitive states. {Happy, sad, disgust, fear, surprise,
anger}. Each state can be attributed with a value
represents the grades among high, low medium.
These are primitive’s states, due to their
characteristic nature to express human emotion,
universally. Albeit, the degree of exposing these
states are different among people due to several
factors. These factors can be predicated and
estimated (i.e., computed) based on specialization
and symmetrical projection through people
characteristic, observed through other disciplinary,
like Type_Age, Type_Gender, Type_Ego-gram and
so (Hakura, 2009). In this paper, we call these as
stereo data as typed meta data related to complex
representation for emotional states. [Such
presentation would be useful to use object orientated
technology in the implementation.] For example:
TypeFear:(Type_Age:20th, Type_Gender:male,
Meta_Type_perosnality). This is a stereo type (i.e.,
class definition) on Class:fear be characterized. For
sickness related issues, the pain (user) can be a
stereo type of a combination of {disgust (medium),
(sad (low)), neutral}. The combinations of the
emotional related states can be extracted in real-time
from the frame video collected from user images
labeled on the spoken sentences that he/she
articulate to present his/her condition. This
articulation representation would be to express user
physical status or/and mental status using informal
representation in spoken language. This time the
spoken language is Japanese. As a spoken language
it would be arbitrary set of sound words (spoken
words). The sound is a stereotype collecting the
emotional feature of the patient (i.e., user).
(Kurematsu, 2009). The facial and related situational
information collected by the system would reflect
the status of the patient. Here, is the stereotype of
the emotion of the user. So the user status is a
combination of the pair: {StereoType_Voice(pitch,
power), Stereotype_ (face(happy, sad,..), situation
(gender(Boolean), temperature(integer), blood
pressure(integer,integer), BMI(integer))}. These two
different ontology stereotype information represent
the mental cloning of the user for reasoning purpose.
The wording (key word extraction by the mapping
alignment between the two view schemata related to
MENTAL CLONING BASE VIRTUAL DIAGNOSTICIAN SYSTEM - Virtual Medical Doctor System (VDS) Reasoning
253

the two ontologies), are to be concluded by the
system. These wording would construct the situation
related abstraction useful to be articulated to
construct the schema needed to establish the
conceptual view of the user diagnostic situation.
Words collected from user (i.e., patient) and
conceptualized. For example Headache; as a concept
is conceptualized into mental view, and physical
view. Each view would have a set of condition and
assertion to be fulfilled collectively as assertions.
This is a temporal order related situational reasoning
based on integrated views of reasoning. It is sequent
cascade incremental reasoning, based on
regenerative schema at the functional
correspondence mapping. It is cyclic iterative
reasoning based on the same schema’s structure for
diagnosis. The 1
st
schema structure would be used to
collect the best response, and accordingly the related
diagnosis is fetch and customized with diagnostician
template to readout, to the patient with emotion
mimicking the MD namely A. The response from
the patient would lead to another incremental
schema that is semantically consistent with the
previous schema with similar partial set semantically
consistent fragmented diagnosis outcome, with extra
key word, extracted from the patient response
derived from patient performance due to the readout,
role-act diagnosis initiated by the schema of the
alignment of the two ontologies. The incremental
schema generation from the mapping alignment
constructed through the patient and computed by
system due to the VDS generated scenarios derived
from the semantic net (UMLS), and shown in Fig. 5,
is cascading and incremented schema type
generation, in nature. This would provide structured
interoperability through such integration.
Medical diagnosis process is built by merging a set
of fragments instances of the mental views instances
with the corresponding physical views instances.
These mappings are expressed with various
relationships between classes in the two different
ontology fragments, for machine executable medical
diagnosis purposes.
The VDS final conclusion on the diagnosing
situational reasoning process would also be part of
the readout to validate the patient performance if
he/she is satisfied with the outcome. This validation
process is essential to help the patient be more
interacted with the VDS on basis on collective
engagement for best practices. All diagnosis reports
are also sent to the MD for conformance checking.
Above we have expressed the stereotype
emotion, and below we integrate it with the
stereotype voice. The stereotypes voice is also used
by the VDS to express the question and related
responses for information extraction from the patient
user. The VDS doctor would express these
synchronized stereo types using avatar which is 3D
generated graphics and synchronized voice sounds
as shown in Fig. 2 and Fig.3. The 1
st
response would
be presented through the avatar using the
representation of the stereotypes (emotion and
voice) mentioned above. Then the collected
information for the patient user is also represented in
the next cycle of diagnosis hierarchy, for another
round of reasoning in the search engine. The
information knowledge is represented as semantic
net and based on the stereotype representation. The
domain knowledge is specified by automatic
retrieval in establishing a link between the ontology
and the patient database.
The word selection is specified through the
keywords. The schemata outline (as above) would
construct the conceptual schema that would be used
to do search in the semantic net based on the
situational abstract articulated on the tow views,
namely the mental and physical views.
The semantic net is constructed based on Object
Web ontology (OWL). The data base is constructed
such that the diagnosis would be articulated on
structural hierarchy. For example pain, with fever,
specify the diagnosis of pain fever class hierarchy,
then pain would be specified as location by the user
answer.
We establish a process of finding the reasoning
of the system using these two types of ontology.
Also this problem is called as ontology mapping
(Kalfoglou,2003), to establish the semantical
relation between procedures and entities among the
mapped ontologies based on the previously
explained stereotype views. We align the properties
of physical diagnosis specified by the medical doctor
with those related to cognitive reasoning based on
the patient mental cloning articulation. Features
expressed by stereotype Meta data definition
mentioned above are used to make such alignment.
The mapping is an abstraction that encapsulate the
features (properties) related to certain abstraction in
an ontology and reflect or map that feature into other
ontology such that to qualify the related features
through such mappings. This semantic level
mapping based on conceptual schema related to each
ontology. The mapping feature would provide
coordination among different schema such that to
establish semantic correspondence for reasoning
purposes, in semantic web bases reasoning fashion.
This would enhance and smooth the interoperability
on service through different schema reflected on
different type ontologies. As shown in Fig.2 and
Fig.5., This mapping is incremental process as the
HEALTHINF 2010 - International Conference on Health Informatics
254

patient produce new schema and also the VDS
consume this schema to produce another request by
which the patient user would correspond to produce
another schemata to be correspondingly, consumed
again by the diagnostician (the system). This
procedure is recalled based on mutual induction
mapping discovery through conceptual schemata.
This is incremental indexing schema because the
process is qualitative driven by the diagnostician. It
represents incremental diagnostic refinement by
including new collected purified information.
2.1 Implementation Aspects
Ontologies used in semantic web consist of
hierarchical description of concepts and their
properties in a domain (nest of concepts organized
due to the nature of the situation instantiated from
the integrated ontologies). Fig. 2 shows the details of
the system implementation.
OWL (web ontology language), is knowledge
representation scheme in semantic web exploiting
web standards (XML, RDF). OWL is suitable to
specify medical knowledge. We think OWL is more
suitable for us than OBO as the later is mostly
suitable for biological application, and its format
does not include all the feature of OWL.
Deductive inference is used based on explicit
given knowledge, represented by description logic,
like RACER www.racer-systems.com/ We envisage
using the OWL axioms and class constructors as
descriptive logic for explicit inference from medical
knowledge base.
For example, there is a correspondence relation
between the medical process integration “drugs” and
“medical decisions” domains. Consequently, there is
semantics alignment integration among the instances
semantic selection between, process decision and
process of selecting the best match instances of drug
property that fit to the decision to be expressed to
the patient. (as shown in Fig.2).
We envisage templates that can be used by the
diagnostician for matching diagnosis use cases to the
drug prescription databases impeded in the
knowledge base. This would be a sub ontology
derived from the aligned two ontologies, (mental
and physical). We envisage using a sequence
diagram with association rules to examine
interactions arising in various patient scenarios to
establish the validity of diagnosis procedure as
approved by the diagnostician.
Discovering association rules is an important data
mining problem. For example patient who has
running nose can be either allergenic side effect or a
side effect of cold sickness. Therefore, the main
purpose of implementing relationships in the
knowledge base is by analyzing the data as reference
during decision making.
Protégé UMLS plugin supports browsing and be
use to query the UMLS knowledge base for medical
keywords and retrieve them in terminological format.
We construct domain ontologies by entering
diagnosis related data and storing them in formats
standards like OWL. The formal of OWL is
provided by description logics (DLs). DLs are used
to describe structured objects whose parts are
interconnected in complex ways, such as medical
diagnosis. OWL facilitates greater machine
interpretability of Web style content than that
supported by XML, RDF, and RDF Schema (RDF-
S) by providing additional vocabulary along with a
formal semantics. Instance data pertaining to the two
view mapped ontology is making the assertion in
terms of DL using Ontomat. OntoMat
http://annotation.semanticweb.org/ontomat Public
annotation tool is used to build OWL instances, and
attribute relations, participate in the logical part of
DL.
MD doctor diagnosis routines, as well as the MD
personality (mental view) are added to the action
scenario related to diagnosis (Fi.g.2). All these
knowledge based are to be represented as a concept
in DL in structural formal way using the stereotype
based views mentioned above. The reasoning would
be reflected through what we called as diagnosis
map: reflects the clustering of different knowledge
map articulated through the mapping of the two
previously mentioned views (mental and physical)
shown in Fig.5.
Also, there is a correspondence to the patient
pattern: behavioural pattern that is reflected by the
mental view ontology along with the attributed
values of the physical view. Recall that the physical
view is values reflecting by the physical status of the
patient. This all resembled in profile processor
shown in Fig.2. The strategy of changing
diagnostician (i.e., MD) routines would be affected
by specified instances of patient observation, these
related observation would be categorized in a region
that to be confirmed by actual MD, like blood or else
physical collected data analysis. In most cases MD
chose from limited evoked set of drugs which comes
up in their minds, given a certain health problem of a
patient. This evoked service is influenced by MD
mental states, background and other local
parameters. MD usually does not consider all
possible treatment options, but chose approximately
among two to 5 different options reflected to his/her
experiences. This is resembled by the Emotion
Estimate processor in Fig.2.
The knowledge base diagnoses scenarios can be
revised and updated based on new diagnosis
MENTAL CLONING BASE VIRTUAL DIAGNOSTICIAN SYSTEM - Virtual Medical Doctor System (VDS) Reasoning
255

scenarios and participate to revise this efficiency
related issue. However, it is still be approved by the
MD in order to be used by the system. We currently
are collecting these action scenarios from a hospital
case study in Iwate region, in Japan. We would
report on this in another paper.
3 CONCLUSIONS
This paper is reporting a progress status of our
project related to mental cloning based concept on
how to reason and represent human emotion in
scientific way and use that emotion to reason with
human user. We articulate such realization to
establish a virtual medical doctor for diagnosis
purpose. The MD is a real person that based on
interviews, we extract her/his personality that is to
be used into the system and act on his/her behalf on
mental basis using her/his routine diagnosis
procedure (knowledge and scenarios). Using this
with other related information we created a system
that interacts with the patient user based on
Transaction analysis protocol. The system would
be examined in Beta space at a hospital where that
MD is working. We have represented the patient
mental view and physical view. We have aligned
and mapped these two views to discover the best
integrated correspondence that resulted in a set of
key words that would be used in searching the best
action scenario relative to patient case. The
discovery is incremental and cascade. The
implementation outline of our system is presented
in this paper. All diagnosis knowledge of MD is
stored in the knowledge base as semantic net and in
OWL. For testing purpose we have used UMLS for
knowledge based, as it is based on semantic net.
The mapping is based on DL. The system is under
construction and to be installed in a hospital in
Iwate region in Japan by 2010.
ACKNOWLEDGEMENTS
This research is supported by the Ministry of
Internal Affairs and Communications of Japan under
the Strategic Information and Communications R&D
Promotion Programme (SCOPE).
REFERENCES
Annette ten Teije (ed). 2008 Computer-Based Medical
Guidelines and Protocols: A Primer and Current Trends
(Studies in Health Technology and Informatics, IOS press,
ISBN: 978-1-58603-873-1
Fujita, H., Hakura, J, Kurematsu, M., 2009 “Intelligent
human interface based on mental cloning-based
software” International Journal on Knowledge-Based
Systems, Elsevier, 22 (3), pp. 216-234, April.
Fujita, H., Hakura, J. Kurematsu, M. Chida, S. and
Arakawa, Y.:2008 “Empirical based Techniques for
Human Cognitive Interaction Analysis: Universal
Template Design”,the 7th New Trends in Software
Methodologies, tools and Techniques (Proceedings of
SoMeT_08), pp.257-277. IOS press, ISBN: 978-1-
158603-916-5
Hakura, J., Kurematsu, M., Fujita, H., 2008 An
Exploration toward Emotion Estimation from Facial
Expressions for Systems with Quasi-Personality,
INTERNATIONAL JOURNAL of CIRCUITS,
SYSTEMS and SIGNAL PROCESSING, Vol. 1, No. 2,
137-144.
Hakura, J., Kurematsu, M., Fujita, H 2009 «Facial
Expression Invariants for Estimating Mental States of
Person» Frontiers in Artificial Intelligence and
application series, Volume 199, New Trends in
Software Methodologies, tools and Techniques
(SoMeT_09),. IOS press, ISBN: 978-1-60750-049-0.
Kurematsu, M., Ohashi, M. Kinoshita,O. Hakura, J. And
Fujita, H., 2009: “An Approach to implement
Listeners Estimate Emotion in Speech” Frontiers in
Artificial Intelligence and application series, Volume
199, New Trends in Software Methodologies, tools and
Techniques (SoMeT_09),. IOS press, ISBN: 978-1-
60750-049-0.
Leflar,2005: Leflar, R.B and F. Iwata, “Medical Error as
Reportable Event, as Tort, as Crime: A Transpacific
Comparison,” Widener Law Review 189, no. 25
(2005)
Mikkola, 2003, Hospital Pricing reform in the public
health care system- an empirical case study from
Finland, International journal of Health Care Finance
and Economics, 3 (4) 267-286.
NIPSSR, 2006; National Institute of Population and Social
Security Research, “Population Statistics of Japan,”
2006; Tokyo: NIPSSR.
Horowitz: 1988 Introduction to Psychodynamics. A New
Synthesis: By Mardi J. Horowitz. New York: Basic
Books, Inc.
Kalfoglou, Y., and Scholermmer, 2003 “Ontology
Mapping: the state of the art,” The knowledge
Engineering review, 2003.
Tanaka, M., Noguchi, M 2000: Concept Retrieval of
Medical Text using UMLS, Japan Journal of Medical
Informatics, Vol.20, pp.934-935.
Smith, 2000, Reforming Markets in Health Care-An
Economic Perspective, Open University Press,
Buckingham, 2000.]
Trautmann, R. L. & Erskine, R. G. 1981: Ego state
analysis: A comparative view Transactional Analysis
Journal, 11, 178-185.
Weizenbaum, J., 1966: "ELIZA - A Computer Program
for the Study of Natural Language Communication
Between Man and Machine", Communications of the
Association for Computing Machinery, Vol.9, pp.36-
45.
HEALTHINF 2010 - International Conference on Health Informatics
256
