
MICROCOMPUTERIZED RESPIRATORY SOUND RECORDER
A Low Cost Device
Daniel F. Ponte, Raimes Moraes
Electrical Engineering Department, Federal University of Santa Catarina, 88040-900, Florian´opolis, SC, Brazil
Federal Institute of Education in Science and Technology, 64000-040, Teresina, PI, Brazil
Leila J. M. Steidle, Renata Cristina T. P. Viana
Medical School Hospital Department, Federal University of Santa Catarina, 88080-350, Florian´opolis, SC, Brazil
Deborah C. Hizume, Adriano M. Alencar
Physiotherapy Department, State University of Santa Catarina, 88080-350, Florian´opolis, SC, Brazil
Pathology Department, Medical School of University of S˜ao Paulo, 01246-903, S˜ao Paulo, SP, Brazil
Keywords:
Respiratory sounds, CORSA, Flow waveform, Respiratory diseases.
Abstract:
Auscultation of breathing sounds is a common practice since the antiquity. In 1819, La¨ennec invented the
stethoscope and published the first work on pulmonary disorders and their associated sounds. Since then, the
auscultation was incorporated into medicine. The first electronic device to record and analyze physiological
sounds was built in 1955, being followed by many other developments. In 2000, a task force of the European
Respiratory Society established guidelines for computerized respiratory sound analysis (CORSA). Our work
describes a low cost microcomputerized system, based on the CORSA guidelines, developed to acquire and
record breathing sounds as well as respiratory flow waveforms. It consists of a four channel micro-controlled
device that can simultaneously record sounds from three different sources and flow waveform. These signals
are transmitted to a microcomputer running dedicated software that shows the waveforms on the screen and
stores them into the hard disk. The developed device was tested in patients with heart failure, idiopathic
pulmonary fibrosis, pneumonia and asthma. Examples of the registered signals and results of a qualitative
assessment of the developed system are presented.
1 INTRODUCTION
In 1819, La¨ennec developed a noninvasive diagnostic
tool for the assessment of pulmonary diseases named
stethoscope (La¨ennec, 1819). Based on necropsies,
he associated respiratory sounds auscultated on the
thorax to pathologies, such as: edema, pneumo-
nia, tuberculosis, bronchitis and emphysemas. How-
ever, lung sound auscultation carried out with the
stethoscope is a subjective procedure, since it de-
pends on the experience and hearing acuity of the
examiner (Garcia, 2002). Besides, the human au-
ditory system is not very sensitive to the frequency
response of stethoscopes that attenuate components
above 120Hz (Sovij¨arvi et al., 2000).
In 1955, the first electronic device to record and
analyze biological sounds was developed (McKusic
et al., 1955), being followed by other projects in the
decades of 60 and 70 (Forgacs, 1969; Weiss and Carl-
son, 1972). In 1987, the International Lung Sounds
Association proposed a common nomenclature that
has been used internationally (Mikami et al., 1987).
Computerized methods to record and analyze respi-
ratory sounds may overcome many limitations of the
auscultation. Nevertheless, the conclusive character-
ization of the sounds belonging to different respira-
tory disorders was being hampered by the fact that
researchers were employing systems with different
technical specifications for the sound acquisition. To
circumvent that, the European community promoted
the CORSA (Computerized Respiratory Sound Anal-
ysis) project that established guidelines for the inves-
tigation of lung sounds (Sovij¨arvi et al., 2000).
The adventitious respiratory sounds are classi-
fied in discontinuous or continuous (Sovij¨arvi et al.,
2000). Pulmonary crackles are discontinuous, be-
21
F. Ponte D., Moraes R., J. M. Steidle L., Cristina T. P. Viana R., C. Hizume D. and M. Alencar A. (2010).
MICROCOMPUTERIZED RESPIRATORY SOUND RECORDER - A Low Cost Device.
In Proceedings of the Third International Conference on Biomedical Electronics and Devices, pages 21-27
DOI: 10.5220/0002721900210027
Copyright
c
SciTePress

Figure 1: Microcomputerized system for acquisition of breathing sounds and flow waveforms. There are three channels to
record sounds and one channel to register the flow signal.
(a) (b) (c)
Figure 2: (a) Microphones and acoustic coupler manufactured in nylon; (b) Connections of the pressure transducer to the
pneumotacograph (PT); (c) View of the PT resistance that provides pressure drop proportional to the flow velocity.
ing described as short, explosive and transient sound
waves, characterized by a rapid initial pressure deflec-
tion, called a spike, followed by a short duration ring-
ing and are usually associated with recruitment of ob-
structed airways (Alencar et al., 2001; Hantos et al.,
2004). They occur in heart failure, fibrosis, pneumo-
nia and others. The wheezes and rhonchi are contin-
uous adventitious sounds and are caused by narrowed
upper airways and secretion in bronchial airways, re-
spectively. Wheezes are periodic, containing a single
tone (monophonic) or many related harmonic tones
(polyphonic).
This work presents a low cost system to record
breathing sounds that was developed according to the
CORSA recommendations. It also records flow wave-
form simultaneously.
To assess the developed system, sounds and flow
waveforms were recorded from patients with heart
failure, fibrosis alveolitis, pneumonia and asthma.
The quality of the recorded sounds was analyzed by
specialists. The recorded waveforms as well as the
results of the qualitative assessment of the developed
system are presented.
2 MATERIALS AND METHODS
Figure 1 depicts the block diagram of the developed
system. It consists of a conditioning module (micro-
phones, pressure sensor, amplifiers and filters), a con-
BIODEVICES 2010 - International Conference on Biomedical Electronics and Devices
22

Figure 3: Screen of the software showing four acquired waveforms. On the top, left to right, lung sounds of the channels 1
and 2, respectively. On the bottom left, lung sound of the channel 3. On the bottom right, the flow waveform.
trol module (microcontroller and communication in-
terface) and software for Windows
R
OS. The next
subsections describe each module of the developed
system.
2.1 Conditioning Module
The breathing sounds are acquired on the thorax using
3 electret microphones (MD9745APA-1 – Knowles
Acoustics) that are housed by acoustic couplers man-
ufactured in nylon (Fig. 2) according to the dimen-
sions recommended by previous studies (Kraman
et al., 1995). This microphone model has small di-
mensions (9.7 × 4.5 mm), low weight (about 1g), a
flat frequency response from 100 to 3000 Hz, signal
to noise ratio of 55 dB, output impedance of 2.2 kΩ,
and sensitivity of 9 mV/Pa.
2.1.1 Flow Transducer
To sample the flow waveform, the volunteer breaths
through an acrylic tube containing a pneumotaco-
graph (PT). The pressure drop across the pneumo-
tacograph resistance is proportional to the flow veloc-
ity (Doeblin, 1990). The transducer (DC030NDC4
– Honeywell) measures the differential pressure
through the obstacle in a range of ±76.2 cmH
2
O. It
has a sensitivity of 52.36 mV/cmH
2
O, generating a
voltage output of 2.25±2.0 V. Figure 2 shows how the
transducer inputs are connected to the PT apertures as
well as the flow resistor. The pressure drop is negative
for inspiratory flow and positive for expiratory flow.
Electrical signals generated by the microphones
have low amplitude, requiring amplification and fil-
tering (anti-aliasing) before being sampled. The sig-
nal generated by each microphone is applied to a
preamplifier with a gain of 2 that also accomplishes
impedance matching to the next circuit stage (Sedra
and Smith, 2004). The amplified signal has its band-
width limited from 60 to 2500Hz by two second or-
der Butterworth filters in cascade. The high pass fil-
ter attenuates the low frequency sounds produced by
the heart that may saturate the circuit, distorting the
sampled signal. The low pass one attenuates sounds
that are above the expected frequency content of the
crackles. These respiratory sounds have the highest
frequency components that may achieve up to 2000
Hz (Sovij¨arvi et al., 2000). The filtered signal is
further amplified to 600 times by the inherent filters
gains and by software programmable gain amplifier
(IC AD526 – Analog Devices).
The output voltage signal of the pressure trans-
MICROCOMPUTERIZED RESPIRATORY SOUND RECORDER - A Low Cost Device
23

ducer is filtered by a second order Butterworth low
pass filter with a cut-off frequency of 40Hz. The sig-
nal amplitude is adjusted to the maximum value of the
acquisition module (0 to 2.5V), considering the max-
imum expected flow range (-70 to +70ℓ/min). For
that, it is amplified and summed to a dc offset to
achieve positive values. The obtained resolution is
17.9mV(ℓ/min)
−1
.
2.2 Control Module
The main IC of the control module is the ADuC841
microcontroller (Analog Devices), an optimized
single-cycle 20 MHz 8052 core. It has a 12-bit analog
to digital converter (ADC) fed by an 8-channel ana-
log input multiplexer, four different memory blocks
(62 kiB of flash for code, 4 kiB of flash for data, 256
bytes of general-purpose RAM and 2 kiB of internal
XRAM), 3 timers, serial communication interfaces
(UART, SPI, I2C) and 2 digital to analog converter
(DAC) of 12 bits.
After being filtered and amplified, the three respi-
ratory signals and the flow waveform are simultane-
ously sampled at 10 kSPS by a sample - and - hold (IC
SMP04 - Analog Devices). The ADuC841 gets, one
by one, the sampled voltage values and converts them
to digital. It carries out the conversion in 8 µs with a
voltage resolution of 0.61mV (1LSB=2.5 V/4096 ).
The digital samples are sent to the data-transfer
device (IC FT245BM – Future Technology Devices
Intl.) that establishes the USB communication with
a notebook, transferring data at the rate of 1MiB/sec
(Axelson, 2005).
2.3 PC Software
Software developed in C++ Builder establishes the
communication between the computer and the control
module. For that, USB driver made available by the
FT245BM manufacturer is employed.
The received data contain multiplexed samples of
each channel. The samples have a header with the
number of the channel to which they belong.
The software demultiplexes the received data and
shows them on the screen in real time. To achieve
that, a scientific chart library for plotting multiple
curves (Scope) is used (Scientific Plotting Library)
since the native C++ Builder library is quite slow for
real time applications. Each sampled waveform is
stored into the hard disk in individual wave files. Fig-
ure 3 shows the screen of the developed software.
3 RESULTS
To assess the qualitative performance of the devel-
oped system, adventitious sounds were recorded from
patients of a Medical School Hospital (Federal Uni-
versity of Santa Catarina) after the approval by its Re-
search Ethics Committee (Process number:181/2007).
The patients were in a room without noise level
control (infirmary). Based on the medical records,
clinical signs, chest x-rays and lung function studies,
the patients were diagnosed with the following pul-
monary conditions: heart failure (2 men), idiopathic
pulmonary fibrosis (3 men), pneumonia (2 men) and
asthma (5 women).
Figures 3 and 4 show examples of sound curves
as well as flow waveforms that were simultaneously
recorded using the developed system.
The sounds collected from twelve patients (with-
out any post-processing) were reproduced to seven
respiratory sound specialists of the Therapeutic Labo-
ratory in the Medical School of the University of S˜ao
Paulo (LTFMUSP). The specialists filled up a ques-
tionnaire on the quality of the recorded sounds. 42
opinions were obtained (Table 1). Besides the sound
quality, the questionnaire aimed to evaluate the need
for further processing of the sounds to improve the
diagnosis.
4 DISCUSSION
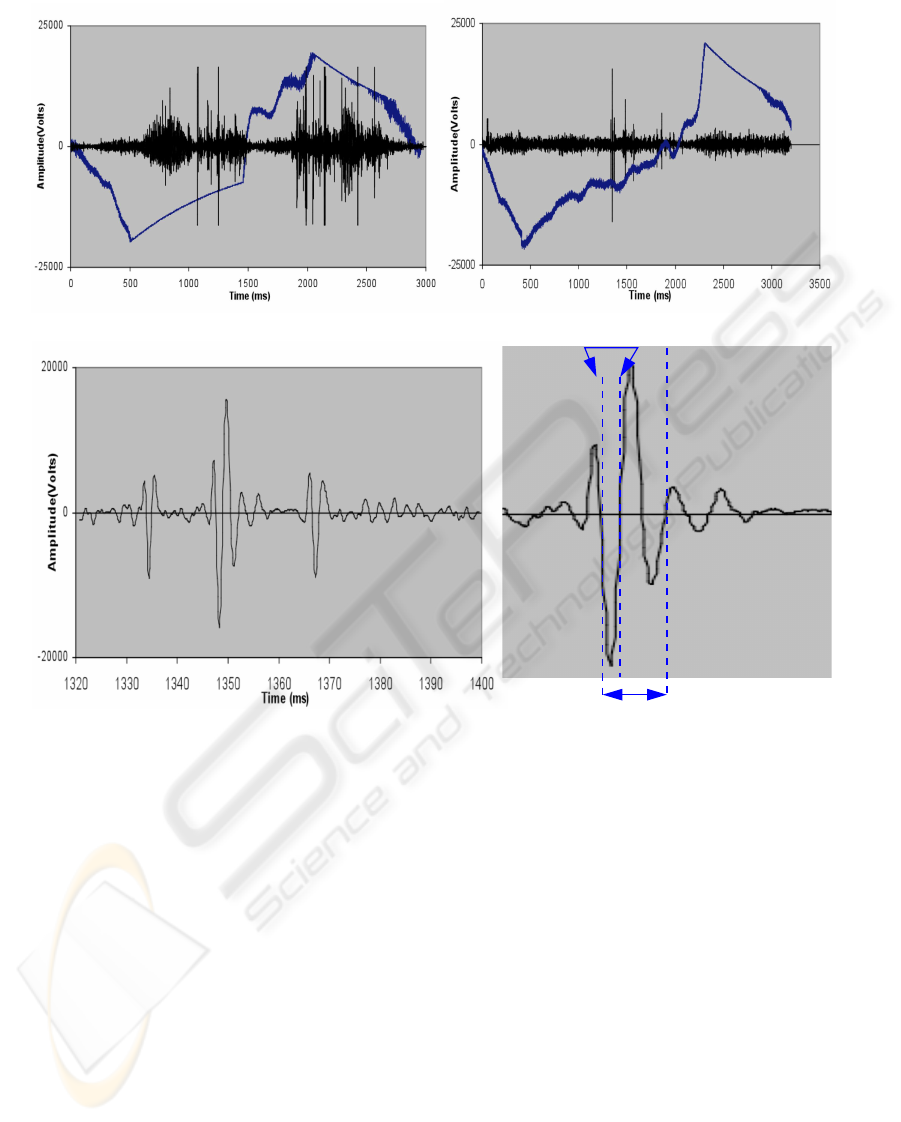
Figure 4a shows that crackles occurred during the in-
spiration and expiration for a fibrosis patient. Patient
with heart failure had crackles only at the end of the
inspiration (Figure 4b). It should be noted that this
condition may generate crackles during expiration as
well (Piiril¨a et al., 1991; Vyshedskiy et al., 2009).
Figure 4c and d shows an expanded crackle wave-
form. The American Thoracic Society (ATS) uses
time intervals of the expanded crackle waveforms
(initial deflection width (IDW) and two-cycle dura-
tion (2CD)) to classify the crackles in two classes:
fine, or high pitched crackles, and coarse, or low
pitched crackles (American Thoracic Society, 1977).
Figure 5a shows crackles and wheezes acquired from
a patient with pneumonia. Figure 5b shows the ex-
panded wheezes also known as squawks (Paciej et al.,
2004).
Figure 6 shows a short acoustic interval contain-
ing wheezes (and its sonogram) acquired from a pa-
tient with acute asthma. It is possible to see that the
recorded sound has more than one tone, being named,
therefore, polyphonic wheezes.
BIODEVICES 2010 - International Conference on Biomedical Electronics and Devices
24
IDW
2CD
(b)(a)
(d)(c)
Figure 4: Crackles and flow waveforms recorded from patients with idiopathic pulmonary fibrosis (a) and heart failure (b).
The sound and flow waveforms are shown by the black and blue lines, respectively. (c) Zooming of the crackles shown in (b).
(d) The waveforms, initial deflection width (IDW) and two-cycle duration (2CD) waveforms of the strongest crackle shown
in (b).
Table 1 summarizes the answers of the 42 ques-
tions posed to specialists on the quality of the sounds
recorded with the developed system. The specialists
heard background noise interference in nearly 15% of
the recordings. They reported heart sounds superim-
posed to the adventitious sounds in about 27% of the
recordings. The majority of the specialists considered
that the noise level contained in the recordings was
low enough to allow the sound classification.
In the infirmary, background noise is always
present and it will be also heard when using a stetho-
scope. When the sound is recorded, digital signal pro-
cessing techniques may be applied to reduce the inter-
ferences due to the background noise and due to the
heart sounds.
5 CONCLUSIONS
Auscultation of breathing sounds using stethoscopes
is a relevant medical practice. Nevertheless, it does
not allow the information to be quantified, stored, re-
produced, visualized or processed. Therefore, it is
difficult for the specialists to exchange information
and educate new professionals.
Breathing sounds acquired with microphones and
recorded with eletronic devices contain information
of a given patient lung condition that can be stored
and does not depend on the specialist subjectivity.
The application of digital signal processing tech-
niques to these signals may allow the development of
quantitative methods to assist the diagnosis.
This work presented a low cost system that is able
to acquire and store respiratory sounds and flow wave-
MICROCOMPUTERIZED RESPIRATORY SOUND RECORDER - A Low Cost Device
25
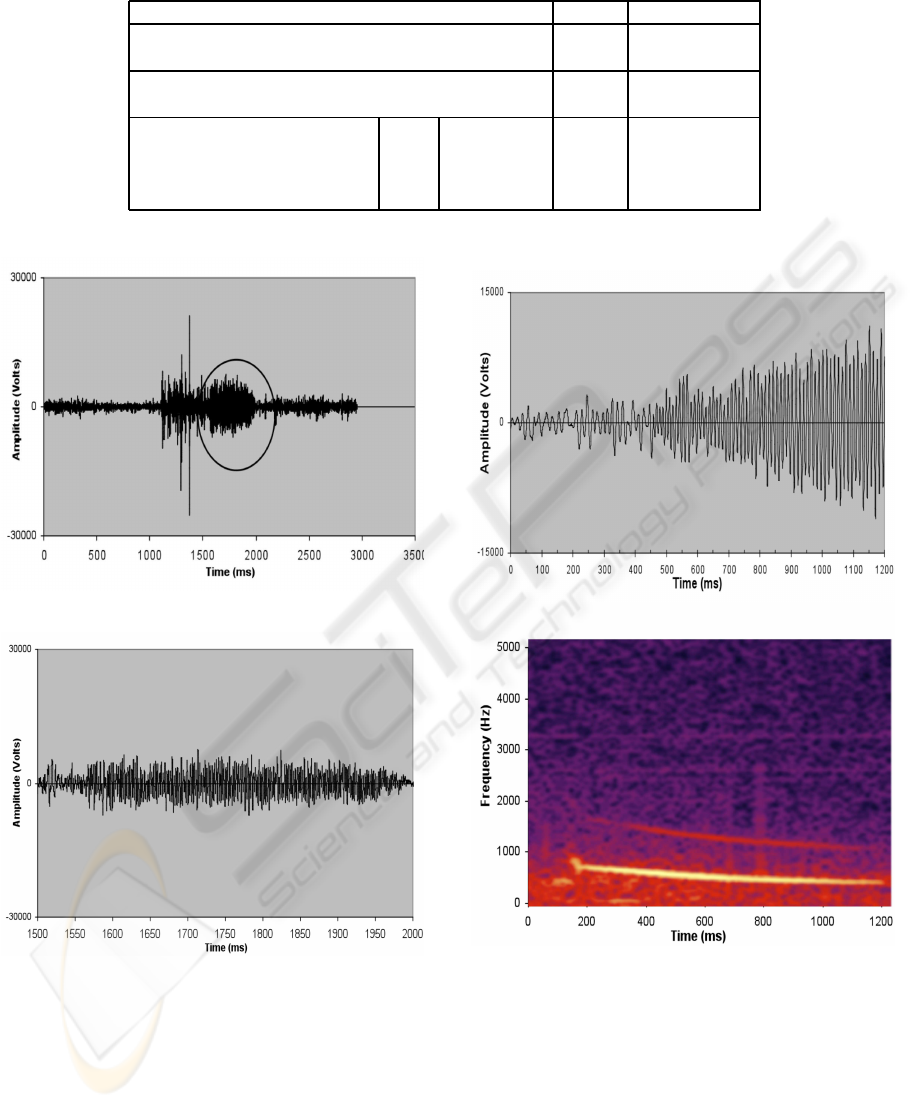
Table 1: Specialists answers about the respiratory sounds recorded with the developed system.
No Yes
Is there environmental noise
in the respiratory sounds? 85.7% 14.3%
Is there heart sounds mixed
with the respiratory sounds? 73.8% 26.2%
Low Acceptable High Unacceptable
Classify the level of the
intrinsic system noise added 31% 47.5% 21.5% 0%
to the respiratory sounds.
(b)
(a)
Figure 5: Crackles recorded from patient with pneumonia
followed by wheezes (squawks - encircled region) (a) and
the zoomed view of the squawks (b).
forms. The system presented a good performance.
It was possible to record different respiratory sounds
with a good quality (crackles, wheezes and others).
The development of such low cost systems may allow
the dissemination of computerized respiratory sound
analyzes, contributing to a more objective diagnosis
of pulmonary disorders in the clinical practice.
(a)
(b)
Figure 6: Wheezes from patient with acute asthma (a) and
its sonogram using Hamming window (b).
ACKNOWLEDGEMENTS
The authors are thankful to the seven specialists
that answered the questions about the lung sounds
recorded. The authors acknowledge Dr. Henrique T.
Moriya, and Jo˜ao R. Baggio, MSc for many valuable
discussions related to technical aspects of the acqui-
BIODEVICES 2010 - International Conference on Biomedical Electronics and Devices
26

sition system as well as the patients of the HU/UFSC
that allowed the recordings. A. M. Alencar acknowl-
edge FAPESP (Fundac¸˜ao de Amparo a Pesquisa do
Estado de S˜ao Paulo).
REFERENCES
Alencar, A. M., Buldyrev, S. V., Majumdar, A., Stanley,
H. E., and Suki, B. (2001). Avalanche dynamics of
crackle sound. Phys. Rev. Lett., 87:088101.
American Thoracic Society (1977). Uptated nomenclature
for membership reaction. reports of the ats – accp ad
hoc committee. Am. Thorac. Soc., 3:5–6.
Axelson, J. (2005). USB Complete. Lakeview Research
LLC, 5310 Chinook Ln., Madison, USA.
Doeblin, E. O. (1990). Measurement Systems: application
and design, Chapter 7. McGraw-Hill, Singapore.
Forgacs, P. (1969). Lung sounds. Br. J. Dis. Chest, 63:1–2.
Garcia, E. A. C. (2002). Biof´ısica. Sarvier, S˜ao Paulo,
Brazil, 2nd edition.
Hantos, Z., Tolnai, J., Alencar, A. M., Majumdar, A., and
Suki, B. (2004). Acoustic evidence of airway open-
ing during recruitment in excised dog lungs. J. Appl.
Physiol., 97(2):592–598.
Kraman, S. S., Wodicka, G. R., Oh, Y., and Pasterkamp,
H. (1995). Measurement of respiratory acoustic sig-
nals: Effect of microphone air cavity width, shape and
venting. Chest, 108:1004–1008.
La¨ennec, R. T. H. (1819). De l’auscultation m´ediate ou
trait´e du diagnostic de maladies des poumons et du
coeur, fond´e principalement sur ce nouveau moyen
d’exploration. Brosson et Chaud´e, Paris.
McKusic, V. A., Jenkins, J. T., and Webb, G. N. (1955).
The acoustic basis of the chest examination: Studies
by means of sound spectrography. Am. Rev. Tuberc.,
72:12–34.
Mikami, R., Murao, M., Cugell, D. W., Chretien, J., Cole,
P., Meier-Sydow, J., Murphy, R. L., and Loudon, R. G.
(1987). International symposium on lung sounds. syn-
opsis of proceedings. Chest, 92(2):342–345.
Paciej, R., Vyshedskiy, A., Bana, D., and Murphy, R.
(2004). Squawks in pnemonia. Thorax, 59:177–179.
Piiril¨a, P., Sovij¨arvi, A. R. A., Kaisla, T., Rajala, H. M.,
and Katila, T. (1991). Crackle in patients with fibros-
ing alveolitis, bronchiectasis, copd, and heart failure.
Chest, 99:1076–1083.
Sedra, A. S. and Smith, K. C. (2004). Microeletronics Cir-
cuits. Oxford University Press, Ney York.
Sovij¨arvi, A. R. A., Vanderschoot, J., and Earis, J. E.
(2000). Standardization of computerized respiratory
sound analysis – corsa. Eur. Respir. Rev., 10(77):585.
Vyshedskiy, A., Alhashem, R. M., Paciej, R., Ebril, M.,
Rudman, I., Fredberg, J. J., and Murphy, R. (2009).
Mechanism of inspiratory and expiratory crackles.
Chest, 135(1):156–164.
Weiss, E. B. and Carlson, C. J. (1972). Recording of breath
sounds. Am Rev Respir Dis., 105:835–939.
MICROCOMPUTERIZED RESPIRATORY SOUND RECORDER - A Low Cost Device
27
