
A NEED FOR AN INTEROPERABLE OPEN SOURCE
MIDDLEWARE FOR AMBIENT ASSISTED LIVING APPLICATIONS
A Position Paper
Sten Hanke, Christopher Mayer, Johannes Kropf and Andreas Hochgatterer
AIT Austrian Institute of Technology GmbH, Biomedical Systems, Viktor Kaplan Strasse 2, A-2700 Wiener Neustadt, Austria
Keywords:
Ambient assisted living, AAL, Middleware, Open source, Interoperability, Standardisation.
Abstract:
Recent European population projections underlined demographic developments towards an ”ageing society”.
A challenge of the future is ”ageing well at home” assisted by technology, while maintaining a high degree
of independence, autonomy and dignity. Ambient Assisted Living technologies try to follow this objective
by integrating intelligent assistance-systems in people’s homes. So in future there will be a high demand on
AAL applications which should fulfil different needs of user groups and daily living scenarios. To speed up
the development process and to make the applications more adaptive and flexible to special user needs a com-
mon middleware with standardised interfaces would be desirable. This should be an open-source middleware,
which operates as an interconnection layer to the operating system and as basis for applications and services.
Furthermore the implementation of different frameworks and standards is preferable to ensure the interoper-
ability of different systems and overlapping domains in AAL. The open source approach can be essential to
initiate a community of different stakeholders and to reuse software components with a common understand-
ing on the implemented standards. The paper shows the need of such an interoperable middleware and gives
recommendations of standards and frameworks to follow. The paper explains why the open source approach
is a chance to fulfil the mentioned motivations. As a first approach the EU IST FP6 project MPOWER is
introduced, which could be the basic fundament of such a middleware approach. It is an example for an open
source service oriented platform providing encapsulated AAL and health related services.
1 INTRODUCTION
Within the next decades the European society will
face serious demographic changes. Recent European
population projections for 2008-2060 published by
the European Office for Statistics underlined demo-
graphic developments towards an ”ageing society”. It
is projected that from 2015 onwards, births will not
outnumber deaths and hence population growth due
to natural increase will cease. For this reason posi-
tive net migration will be the only population growth
factor (Giannakouris, 2008).
The old age dependency ratio, which is defined as
the population aged 65 years or older related to the
population aged between 15 and 64 years, will be a
particularly dynamic indicator. It is a reasonable pro-
jection that, on average for the EU-27 and if current
trends prevail, the old age dependency ratio will ap-
proximately double during the next 50 years. This
means that in 2050 a person of working age might
have to provide for up to twice as many retired people
as is usual today (Eurostat, 2008).
The social behaviour and lifestyles as well as the
identity of the individual older person will change
if current trends continue. With higher expectancies
of life and rising retirement ages in European coun-
tries, the proportion of older people at work will in-
crease as well as the number of elderly people partic-
ipating actively in social life. Furthermore the num-
ber of elderly people living alone and of those who
live under the average subsistence level will increase
(AALIANCE, 2008). Although older people in the
future will remain self-sufficient for a longer time,
more people will need high intensity care in the end-
of-life period and more people will need support in
daily life operations prior to this phase due to more
or less intense disabilities (European Commission,
2005).
517
Hanke S., Mayer C., Kropf J. and Hochgatterer A. (2010).
A NEED FOR AN INTEROPERABLE OPEN SOURCE MIDDLEWARE FOR AMBIENT ASSISTED LIVING APPLICATIONS - A Position Paper.
In Proceedings of the Third International Conference on Health Informatics, pages 517-524
DOI: 10.5220/0002767105170524
Copyright
c
SciTePress

2 MOTIVATION
These demographic changes will lead to different
challenges and opportunities of ageing society in
Europe such as a growing number of older people
who live by themselves and who are in need of
care and a growing number of older people lacking
basic financial and social resources who will have
difficulties to obtain a minimum of health and care
services. Facing these challenges and opportunities
there exist opportunities, where technological and
socioeconomic innovation can enhance the quality
of life for older and impaired people. It is assumed
that Ambient Assisted Living (AAL) technologies
and services for elderly people can play an important
role to solve some of the increasing future problems
(AALIANCE, 2008). Information and communica-
tion technology (ICT) is believed to play a major role
in order to help older individuals to improve their
quality of life.
The following three areas of user needs are to be
addressed as stated in (European Commission, 2007):
• Ageing well at work or ”active ageing at work”:
staying active and productive for longer, with bet-
ter quality of work and work-life balance with the
help of easy-to-access ICT, innovative practices
for adaptable, flexible workplaces, ICT skills and
competencies and ICT enhanced learning (resp. e-
skills and e-learning).
• Ageing well in the community: staying socially
active and creative, through ICT solutions for so-
cial networking, as well as access to public and
commercial services, thus improving quality of
life and reducing social isolation (one of the main
problems of older people in rural, scarcely pop-
ulated areas, as well as urban areas with limited
family support).
• Ageing well at home: enjoying a healthier and
higher quality of daily life for longer, assisted by
technology, while maintaining a high degree of in-
dependence, autonomy and dignity.
As can be seen there is a need for the devel-
opment of AAL technologies to support elderly
people in their daily life activities to enable them
to live an independent life in the privacy of one’s
home as long as possible. This could help to cut
the sharp increase in social costs caused by the
ongoing demographic change. Ambient Assisted
Living (AAL) technologies try to follow this ob-
jective by integrating intelligent assistance-systems
in people’s homes. Modern sensor-techniques and
IT-based evaluation of data, i.e. behaviour pattern
recognition algorithms, should support the safety of
the inhabitants. In other words, current sensor events
are compared to predefined or learned patterns and
if the situation differs from normality alarms are
triggered by the AAL-system at different levels (i.e.
as a feedback to the care receiver, as an information
for relatives or as an alarm to a nurse and/or a doctor).
AAL applications respectively technologies
should be based on a middleware, which is open
to the public and works as an intermediate layer
between the operating system and the application
itself. The middleware has to be adaptable in terms
of services that can be implemented. Furthermore it
should be flexible and freely configurable to satisfy
user needs regarding the development of applications
and user interfaces. Moreover it would be a good
starting point for rapid development of applications
and services. As a consequence the development
process would be more cost- and time-efficient. A
realisation as an open source project would help to
spread it in a big community and a benefit would be
more reliability and security in further development
stages.
To ensure an interoperability and interaction of
different AAL applications and systems standards
should be the basis of all technologies. Furthermore
the idea of open source software can enhance the
coalescence of different approaches. Following
ideas about standarization principles, open source
approaches and generalization of interfaces and their
interoperability are presented.
3 ONE MIDDLEWARE FOR
APPLICATION DEVELOPER
There are a number of architectural characteristics
that can be used as basis for reasoning about what
might be considered appropriate quality attributes that
can be measured. These include interfaces and lay-
ers, standards and data interoperability. Middleware
provides an example of the layering principle. It sep-
arates the applications from the operating systems on
which the applications run. As outlined in figure 1,
middleware services are sets of distributed software
that exist between the application and the operating
system and network services on a system node in the
network (Kasunic and Anderson, 2004).
An essential aspect of architecture is the establish-
ment of technical standards. In general, standards de-
fine common elements, such as user interfaces, sys-
tem interfaces, representations of data, protocols for
the exchange of data, and interfaces accessing data
HEALTHINF 2010 - International Conference on Health Informatics
518

Figure 1: Middleware.
or system functions. Technical standards provide a
number of advantages for the systems architect. With
regard to interoperability, standards are important be-
cause they are accepted by multiple vendors, thereby
increasing the likelihood that a collection of systems
from diverse sources will be able to interoperate. It
has become generally accepted by now that although
standards are certainly beneficial, simple adherence
to standards is not sufficient to guarantee interoper-
ability. Even when there are accepted standards and
compliant products, interoperability is facilitated but
not assured as there are options within standards and
different releases and versions of products.
4 INTEROPERABILITY IN AAL
APPLICATIONS
Interoperability is the ability of different information
technology systems and software applications to com-
municate, to exchange data accurately, effectively and
consistently, and to use the information that has been
exchanged. Important for interoperability is not only
the syntactical interoperability of simply connecting
devices and modules through sharing and exchang-
ing. Specified data formats, communication protocols
and the like are therefore fundamental. But also the
semantic interoperability and therefore the ability to
use and understand the exchanged information is im-
portant. Beyond the ability of two or more computer
systems to exchange information, semantic interoper-
ability is the ability to automatically interpret the in-
formation exchanged meaningfully and accurately in
order to produce useful results as defined by the end
users of both systems. To achieve semantic interoper-
ability, both sides must defer to a common informa-
tion exchange reference model.
Services for the ageing and cognitively disabled
do not and will not exist in isolation. The AAL do-
main consists of a large set of independently devel-
oped systems and services in existing environments.
On top of the value of these individual systems addi-
tional value could be created by exchanging data be-
tween these systems or even aggregate the data in a
system for analysis and to give proper feedback or
alerts to relevant systems or users. These systems
and services should be able to communicate with each
other not only by exchanging data but also under-
standing each other’s data. This can only be achieved
by agreeing on a lot of issues in other words by using
standards (AALIANCE, 2009).
The ageing society’s conditions require that we re-
think traditional models of care. One prominent as-
pect of new care models for this target group is the co-
operation of different stakeholders in the care process.
Stakeholders include the patient himself, his relatives
and caregivers such as the general practitioner, hospi-
tal personnel, homecare personnel and insurance and
social security departments as well. Healthcare sys-
tems are expected to maintain the continuity of care,
shared care and the empowerment of patients in the
management process. Many relevant systems and ap-
plications exist, that AAL services might need to in-
teroperate with. Healthcare applications built around
Europe use proprietary data formats and some sys-
tems are designed to interoperate with others based
on standardized data formats, such as HL7 and CEN
standards. Consequently an interoperability solution
needs to be able to communicate with external parties
in an agreed upon format, even though the internal
system is based on proprietary formats.
So far we have experienced in many projects in the
AAL domain that within one after the other project
different proprietary solutions are developed. A lot
of funded projects are like reinventing the wheel and
so far no common sense on even some universal used
modules or components with open and described in-
terfaces can be found. Many working and already
implemented solutions in residential house or smart
home applications are generally proprietary solutions
in the case of sensor networks, middleware imple-
mentations and even data formats and records. Of
course interoperability and standardisation is already
mentioned in every project proposal but a real guide-
line or state of the art for practical use is still missing.
It seems like there is nowadays a situation in the AAL
domain like in the eHealth domain years ago. Impor-
tant will be to learn from this domain and to speed
up the process of using interoperable and standard-
ized systems and frameworks. Of course AAL is an
A NEED FOR AN INTEROPERABLE OPEN SOURCE MIDDLEWARE FOR AMBIENT ASSISTED LIVING
APPLICATIONS - A Position Paper
519
application domain with a lot of overlapping subdo-
mains where so far there has not been a real need for
interoperability. In the AAL domain there must be a
interchanging of the e.g. eHealth domain, the home
entertainment domain, the home automation domain,
the household appliance domain and many more. The
status quo in the AAL operation are conflicting ver-
sions of standards as well as conflicting implementa-
tions thereof. This is also caused by the fact that so
far the existing standards, like the ISO/IEEE 11073
standards for domotic sensors, have not been used and
implemented in many applications and cases. Thus
there is no experience of e.g. missing parts or any
other lessons learned from usage. There are not many
examples to show how to implement these standards
in practice. Of course there is also a lack of standards
in some fields of AAL applications like for remote
maintenance, terminology and ontology, emergency
and alarming calls and procedures and in some extend
middleware etc. And there is a lack of certification
and also labelling processes of devices and modules
in the AAL domain.
4.1 Using Standards and Frameworks
The structure shown in figure 2 presents four cate-
gories of standards relevant for AAL (AALIANCE,
2009). Starting from the bottom:
• Equipment and environmental standards (EES):
these are standards agreed on in a large domain
and sometimes imposed by regulation. Quite of-
ten they have to be followed if one wants to en-
ter the market and processes to change them are
very difficult. These standards are usually not ICT
related but relate to environmental (e.g. EMC),
quality (ISO 9001), safety, physical product prop-
erties (e.g. CE norms), manufacturing and instal-
lation processes. AAL products however have to
comply with these standards but they will hardly
be influenced by the AAL community. Some
specific standards exist e.g. EN 50134 for so-
cial alarm systems, CENELEC Smart House and
CENELEC TC 205 (HBES) for home and build-
ing electronic systems. A number of standards in
this area will be mentioned but not explored in
greater detail.
• Generic technology standards (GTS): these stan-
dards have often been developed by standard
development organisations or industrial associa-
tions, which are either very broad associations like
IEEE or more closed ones like W3C or UPnP,
Bluetooth, or USB. Often multiple alternatives for
certain technologies exist like Bluetooth, Zigbee,
Z-wave for personal area or local area networks.
For AAL one or sometimes more than one should
be selected. If more than one is selected it might
be necessary that an aggregating device supports
more than one option at the same time. The influ-
ence of the AAL community on these standards
might be in communicating specific needs from
the AAL domain either on the standard itself or
on profiles on top of these standards.
• Domain specific standards (DSS): these are stan-
dards for sub domains that are important for an
integrated AAL solution. Examples of relevant
sub domains are healthcare (with sub groups like:
tele-monitoring, medication registries, electronic
health records, personal health records), home
control, home safety, home security, remote pay-
ment systems, etc. Sometimes generic technolo-
gies have specialisations for certain domains like
the Bluetooth medical profile and the USB device
class definition for personal healthcare devices. In
this category the AAL community might give in-
put to the standard development organisation for
extensions.
• Specific AAL standards (SAS): these are stan-
dards specific to the AAL domain. There are very
limited potential candidates available at the mo-
ment: data exchange standards and ontologies to
enable the exchange and understanding of data be-
tween different subsystems for reasoning on this
data and interacting with the users. Some of these
standards might exist or are evolving in specific
domains as e.g. healthcare.
AALintegration like:
Eh
f
E
xc
h
ange
f
ormats
Ontology‘s
Domainspecific like:
Healthcare:teleͲmonitoring,medication management,care organisation
Homecontrol
,
safet
y
and securit
y
,
y
y
Infotainmentand social connectedness
Electronicshopping,orderning and payment
Generic technologies like:
Connectivity:PAN,LAN,WAN
Webbased services
Distributedsystems,middleware
Equipmentand environment standards like:
Homeand building electronics
Safety,EMC,Connectors,material
Figure 2: Standards relevant for AAL (AALIANCE, 2009).
Although the ”Integrating the Health Care Enter-
prise” (IHE) (IHE - Integrating the Health Care En-
terprise, 2008) started to implement the framework
for health applications, the communication structure
could be used as well for homecare applications for
elderly and persons with dementia. This could be
easily done because there are already structures for
HEALTHINF 2010 - International Conference on Health Informatics
520

point-of-care devices. The benefit would be the ac-
cordance to established standards and standard frame-
works. It is obvious that there is a benefit because
of already established point-of-care communications
from the medical field (blood pressure, temperature
etc.), which can be adapted. Of course the whole IT
structure and the cross-enterprise-document sharing
(XDS) defined in the IHE framework could handle
personal health data and information, which could be,
depending on the use cases, even important for medi-
cal help.
The ISO 11073 offers plug-and-play and a func-
tional as well as a semantic interoperability between
sensor systems and aggregation systems. In this stan-
dard all functions and use cases, which are defined
for patient oriented health care and of course in some
aspects for smart home for elderly, are already ob-
ject orientated modelled. That means a so called
domain information model is constructed where the
device, the functionality, the measured data, set-
tings, alarm functions, patient information and in-
terfaces are defined. Furthermore there are codes
for all information elements defined as ”nomencla-
ture” (ISO/IEEE 11073-10101) and ”data dictionary”
(ISO/IEEE 11073-10201). The communication stan-
dard POCT-1A is implemented in the ISO 11073.9
and is specialised for patient near point of care. In
principle the functionality of POCT1-A could be re-
alised by HL7, but the functional range of the HL7
structure is in some cases (single sensors) too high
dimensioned. So it depends on the special functions
to realize what should be realised on the sensor (ac-
cording sensor often have a restricted hardware) and
the local controller. Because of a clear defined mes-
sage communication the unique interpretation of the
standard is guaranteed. POCT1-A is a flaring of HL7
not a competition standard. The advantage of the
CEN/ISO/IEEE 11073 is that it is the only compre-
hensive system of point-of-care medical device com-
munication standards. The modality categories range
from real-time operating medical equipment to point-
of-care test devices. Wired as well as wireless IR and
RF network technologies are supported. If healthcare
providers and management organizations want point-
of-care to record transparency of information, they
must demand medical device interoperability. In ad-
dition the activity is regularly coordinated with other
health information activities (HL7, NCCLS, IHE and
DICOM) by the core development bodies.
The Continua Health Alliance can help to over-
come the barriers of using standards. The Continua
Health Alliance is a non-profit, open industry coali-
tion of healthcare and technology companies join-
ing together in collaboration to improve the quality
of personal healthcare. With more than 200 compa-
nies around the world, Continua is dedicated to es-
tablish a system of interoperable personal health so-
lutions with the knowledge that extending those so-
lutions into the home fosters independence, empow-
ers individuals and provides the opportunity to truly
personalized health and wellness management (Con-
tinua Health Alliance, 2009). It is important to know
that Continua is not developing standards but is rec-
ommending standards like the ISO/IEEE 11073 and is
also providing a certification process to make the ben-
efit of devices visible to the user. The benefit for AAL
applications is that Continua has beside the scope on
managing chronic diseases and fitness a scope on ag-
ing independently what could be used as a standard-
isation process for devices and applications in the
AAL domain. Therefore more and more companies
and technology providers but also research institu-
tions from the AAL domain are joining the Alliance.
The implementation of standards and interoper-
ability by using frameworks is not only a major is-
sue concerning the usage of the open source ser-
vices, it is also a major issue on private data pro-
tection. Recommendable are the frameworks pro-
vided by IHE (Integrating the Healthcare Enterprise)
and HIMSS (Healthcare Information and Manage-
ment System Society). As an example IHE provides
a Basic Patient Privacy Consents (BPPC) mechanism
to record the patient privacy consent(s), a method to
mark documents published by XDS with the patient
privacy consent that was used to authorize the pub-
lication and a method for XDS consumers to use to
enforce the privacy consent appropriate to the use.
The leadership of HIMSS, Health Level Seven (HL7),
Integrating the Healthcare Enterprise (IHE) and the
HIMSS EHR Vendors Association (EHRVA) have be-
gun to work on this effort by establishing a coordi-
nated set of activities that would provide an HL7 im-
plementation guide and launch this new IHE domain
called Patient Care Coordination with demonstrated
interoperability of medical summary documents by
January 2006.
4.2 The MPOWER Project
MPOWER has been an EU IST FP6 project (fin-
ished June 2009) with the objective to create a mid-
dleware platform that enables rapid development of
novel smart house systems and applications. This
platform should simplify and speed up the task of de-
veloping and deploying services for persons with cog-
nitive disabilities and elderly. The approach has been
to encapsulate the functionality by a service oriented
architecture (SOA) and by using the model driven ar-
A NEED FOR AN INTEROPERABLE OPEN SOURCE MIDDLEWARE FOR AMBIENT ASSISTED LIVING
APPLICATIONS - A Position Paper
521
chitecture approach (MDA). To enable adaptivity and
the possibility to integrate the middleware with ex-
ternal systems a requirement has been the implemen-
tation of existing standards and frameworks (HL7,
ISO, CEN, IHE etc.). For demonstration purposes the
implemented services are containing communication
services, information services, management services,
sensor services as well as security services.
As already mentioned MPOWER is based on SOA
by using the web services WSDL and SOAP. Thus it
is an interoperability enabler, as the web service front
ends allows heterogeneous platforms to interoperate
(e.g. .NET and Java). This is not enough as the mes-
sages, which can be exchanged by applications and
systems, can be very different and there can be appli-
cation policies (such as security) which need special
interoperability requirements. To this end, we have
designed a reusable interoperability architecture that
encapsulates the interoperability components in such
a way that changes in these components or the exter-
nal systems they relate to are hidden from the rest of
the MPOWER framework. For other MPOWER ser-
vices the interoperability services look just like any
other MPOWER service. The mechanism is to use
a design pattern known as the message translation.
We are not the first ones facing interoperability chal-
lenges. It is a reoccurring problem and therefore pat-
terns exist that explain how one should design middle-
ware components in order to achieve interoperability.
We provide this pattern with its subpatterns and ex-
plain their relevance to MPOWER.
To see this middlware, which is implemented,
used, maintained and expanded by different stake-
holders, the MPOWER consortium provides all im-
plemented services as open source (MIT license) un-
der the Free-mpower project. It is hosted on Source-
Forge under http://sourceforge.net/projects/free-
mpower/. Everyone is able and also invited to browse
and acquire the source code, basic documentation
to several services and the toolchain as well as the
service deployment process, the handbooks as well
as the open source toolchain itself and to submit re-
quests. Members of the sourceforge project can also
post code, make documentation and post pictures of
e.g. running application GUIs. Provided services are
for example security services, database management
service (with init data), patient manager service,
calendar service with reminder (HL7v3), patient
information message board service, localisation
service, frame sensor service (ISO/IEEE 11073) as
well as alarming and notification services and many
others. Of course documentation is provided for
these services and the overall architecture.
As short term projects the usage of the free-
mpower setup is thinkable for any student project,
any proof of concept application or rapid prototyp-
ing. As long term projects the free-mpower project
could be the basis for following European projects
any commercial solutions or any application provider.
For community building purpose, which is obviously
a very important point for an open source project,
a growing framework by using and adding service
would be desirable.
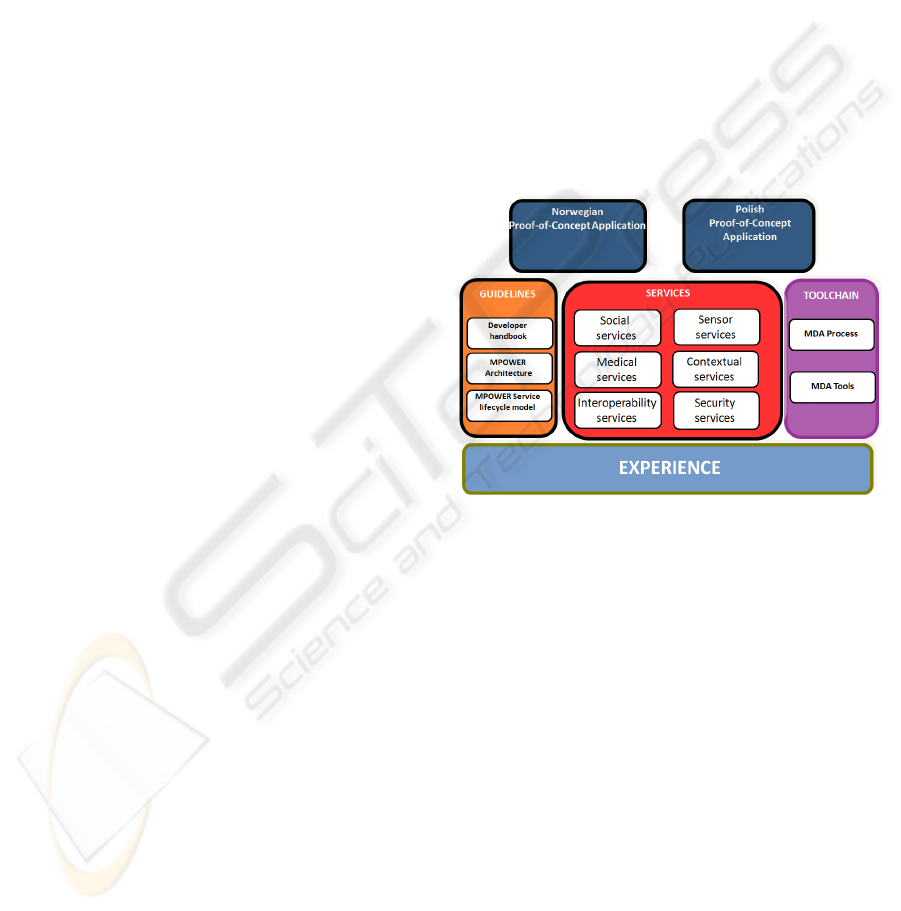
MPOWER is an open source service oriented plat-
form providing encapsulated AAL and health related
services. It includes standardised smart house sensor
interfaces (ISO/IEEE 11073), interoperable interfac-
ing for legacy systems (CDA, HL7-HSSP) and exter-
nal service connection (mobile alarming / reminding
/ communication), security services, social and infor-
mation services (HL7). All results are shown in figure
3.
Figure 3: Results from the MPOWER project.
5 THE CHANCE OF OPEN
SOURCE
To provide the services of a middleware and also soft-
ware application modules as open source to the com-
munity, is a big advantage for projects and a subse-
quent use of the project results as well as it may en-
sure the usage of the platform and the consistency of
the developments beyond the project runtime. On the
other side it is important to be aware of the challenges
and requirements of open source for the project and
application developers.
At first the MIT License states explicitly the rights
given to the end-user, including the right to use, copy,
modify, merge, publish, distribute, sublicense, and/or
sell the software. In detail the end-user are on the one
hand the application developer, which may want to
build applications based on the services, and on the
other hand the care receiver who wants to use the ser-
HEALTHINF 2010 - International Conference on Health Informatics
522

vice including the application. In comparison to the
GPL license the application developer is allowed to
redistribute the modified software and an application
which is an incentive for the professional application
developer and can expand the usage of the services
itself.
Another big advantage of open source services in
the AAL context, which should be taken into account
when talking about ethical issues, is the advantage
of the transparency of the services and the code it-
self. Transparency is inherent to every release of open
source code. The customers can see it and thus the
vendor has no secrets.
But transparency also applies to vendor’s opera-
tions. Vendors who are opaque on their strategy gain
fewer benefits from a open source release of code.
The most successful open source vendors are trans-
parent on their strategies and the most successful open
source customers are transparent in turn, being frank
about their needs. Transparency, the need for it, the
desire for it, extends outward from there. The advan-
tage of the usage of open source in eHealth and AAL
projects concerning the support of standards has been
pointed out as a need by the member states of the Eu-
ropean Union. There is a need to support actions that
cover the development of standards addressing the in-
teroperability of diverse systems and services and to
explore in particular the possibilities of open source
applications to achieve this objective. In this context,
the need for future standards is clearly emphasized
to solve interoperability concerns in a way that all
stakeholders will benefit from the possible adoption
of Open Source reference implementations for care
services. In addition, an open and more free access
to future and existing e-Health and general interop-
erability standards in the AAL and eHealth service
providing should be recommended, taking inspiration
from models such as the World Wide Web Consor-
tium. The exchange of experience in the use of open
standards and open source solutions among health ad-
ministrations in Member States should be promoted
(European Commission, 2004). Success in develop-
ing a European e-Health Area and AAL standard con-
form platform will draw on sharing best practices and
experience across the Union, as systems are deployed
and organizations redesigned. Open source applica-
tions play an important role in achieving interoper-
ability (European Commission, 2004).
Maybe the biggest ethical issue when providing
open source services in the AAL context is the issue
of data privacy and data protection. This is very im-
portant because the services generally developed in
AAL related middleware and application projects use
medical and social relevant data which underlie spe-
cial data privacy regulations.
The advantage of transparency of open source
code and the possibility that any expert has the pos-
sibility to find security leaks and general mistakes in
the code and can fix them, leads also to a high de-
mand on secure software development and the inte-
gration of security services so that the transparency
can not be misused. As a result of the transparency
the application developer can fix and provide special
data security, e.g. in the case of medical data treat-
ment, and provide it as a business to user organization
or private users.
The transparency of open source also gives the
possibility to expand the functionality of the service
or the application, which can be part of a business
strategy, and to learn from the structure and interfaces
of already implemented services.
A very important point concerning the usage of
open source software components is the community,
which uses and kind of maintains the project or at
least can give assistance or support.
A main goal of AAL related projects develop-
ing open source middleware software components
is to build a powerful community of application
developers and users of the open source services
and application. This can be any kind of possible
stakeholders e.g. universities, national organizations,
residential house operator etc. This will be important
to guarantee maintenance of the services to provide
good quality to the user and as well to set up and
include perfect security mechanisms and to close
possible security leaks. The attraction for developers
to provide software components under the MIT
license as open source may be that open source
services under the MIT license are underlying the
international valid copyright law. That means the
provider of the services still holds the international
copyright but is providing the sources as ”it is”.
In the social thinking of the gift economy, where
valuable goods or software modules are given with-
out any explicit agreement for immediate or future
reward, the fact of providing a middleware for AAL
applications makes sense to fulfil the aim of having a
commonly used system. The gift economy is a more
and more desirable thinking in western companies or
by private persons, who are not essentially depending
on a money exchange. Ideally, simultaneous or recur-
ring giving serves to circulate and redistribute valu-
ables within the community. Jordan Hubbard wrote
in his article ”Open Source to the Core” (although
referring to it as a barter economy) and essentially
describes a gift culture, where reciprocity is a broad
community custom, rather than an explicit quid pro
A NEED FOR AN INTEROPERABLE OPEN SOURCE MIDDLEWARE FOR AMBIENT ASSISTED LIVING
APPLICATIONS - A Position Paper
523

quo (Hubbard, 2004): ”The volunteer software engi-
neers in the open source software community are far
more likely to help those who have demonstrated their
commitment to the success of the overall open source
software development process.”
6 CONCLUSIONS
There have been many research projects concerning
a common middleware for AAL applications. There
is a high demand on technical standards in the AAL
domain but their is also a high activity defining stan-
dards going on. For future developments it will be
important to reuse existing developments and to en-
hance or adapt them. In the future it will be important
to have more and more applications with standardised
interfaces and protocols implemented. These experi-
ences can be used by standard organisations to adapt
the documents to users’ and developers’ needs. We
think that the open source approach can help a lot to
spread a common sense a software and standard im-
plementations.
The AAL domain should take the chance of
reusing frameworks and standards from the medical
domain because there is an overlap of this two do-
mains. But more important is the fact that it should
be avoided to make the same experience again and
have an unsatisfying solution for the next years. Even
in the medical domain their is still much to do when
thinking of implemented standards of medical device
communication or data exchange between different
legacy systems. The AAL domain should use the al-
ready existing knowledge and base findings on it.
This will be very important because in the AAL do-
main their are also a lot of other fields where standards
are missing and where the community should work on
like standards for basic user needs evaluation, basic
aspects of layout and designed user interfaces, basic
standards for the demand on usability, standards on
privacy data also for social data and basic standards
for evaluation methodology.
The MPOWER project could be a basis for creat-
ing a community and to start a common implemen-
tation of an AAL middleware. The benefit is that it
is easy adaptable and even some few services can be
used as a standard and maybe integrated in other run-
ning AAL applications, because of its service encap-
sulation.
For the AAL community as a whole it will be a
task to (AALIANCE, 2009):
• Increase the awareness on existing standards
• Demonstrate the advantage of collaborative and
integrated applications and services based on us-
ing standards
• Develop and promote a reference model that gives
guidance to product and service developers.
REFERENCES
AALIANCE (2008). Ageing characterises the demographic
perspectives of the European societies. AAL Policy
Paper, 0.7.
AALIANCE (2009). Policy Paper on Standardisation Re-
quirements for AAL. AAL Policy Paper.
Continua Health Alliance (2009). About the Alliance.
Available from: http://www.continuaalliance.org [Ac-
cessed: February 28th, 2009].
European Commission (2004). e-health - making health-
care better for european citizens: An action plan for a
european e-health area.
European Commission (2005). Confronting demographic
change: a new solidarity between the generations.
Green Paper.
European Commission (2007). Ageing well in the In-
formation Society - An i2010 Initiative. Action Plan
on Information and Communication Technologies and
Ageing.
Eurostat (2008). Eurostat regional yearbook 2008. Euro-
pean Office for Statistics.
Giannakouris, K. (2008). Ageing characterises the demo-
graphic perspectives of the European societies. Statis-
tics in focus, 72.
Hubbard, J. (2004). Open source to the core. Queue maga-
zine.
IHE - Integrating the Health Care Enterprise
(2008). Continua and IHE Collaborate to
Strengthen Outreach and Message. Avail-
able from: http://www.ihe.net/News/ihe-
continua mou release 2008-10-28.cfm [Accessed:
April 8th 2009].
Kasunic, M. and Anderson, W. (2004). Measuring systems
interoperability: Challenges and opportunities, tech-
nical note.
HEALTHINF 2010 - International Conference on Health Informatics
524
