
WIRELESS BODY AREA NETWORKS
Information Dissemination Analysis
Yasir Faheem and Saadi Boudjit
Laboratoire L2TI, Institut Galil
´
ee, Universit
´
e Paris 13, Villetaneuse, France
Keywords:
WBANs, Wearable Sensors, Energy Dissipation, Health Care Computing.
Abstract:
Telemedicine integrated wearable health monitoring system is a novel technology with aiming to support early
detection of abnormal conditions and prevention of its serious consequences. Recent Advances in technology
has led to the development of small, intelligent, wearable sensors capable of remotely performing critical
health monitoring tasks and then transmitting patient’s data back to health care centers over wireless medium.
Patients benefit from continuous ambulatory monitoring as a part of a diagnostic procedure, optimal mainte-
nance of a chronic condition or during supervised recovery from an acute event or surgical procedure. This
requires continuous functioning of the wearable sensor devices. But to the day, energy remains to be a big
constraint in enhancing Wireless Body Area Networks (WBAN) (IEEE 802.15 WPAN Task Group, 2003)
lifetime. Some recent literature on WBANs proposes multi-hop sensor-to-gateway data relay as more energy
efficient than single hop communication. There are studies which argue contrarily. This study analyzes the
single vs multi-hop energy consumption effect for real short range sensor devices.
1 INTRODUCTION
Health cost represents a considerable ratio in the eco-
nomic budget of developed countries, and certain ten-
dency studies are not optimistic about an improve-
ment in the situation. Average age of the population
tends to increase. Number of people requiring more
or less care intensive medical monitoring is not small.
This increases overall cost of medical care. No doubt,
using socio-medical establishments to place people at
risk, under surveillance is impractical for cost rea-
sons, but also for reasons of quality of life. Many
of these people are fully autonomous, though weak-
ened. Their psychological confinement due to pres-
ence nursing staff would be a breach of their free-
dom. Therefore, partially replacing the assistance of
nursing staff by small health surveillance & commu-
nication equipments like sensors, networks, monitor-
ing software could be cost effective and would also
increase life standard. Focusing on this topic, we
are developing a wireless health monitoring platform
which aims to continuously monitor mobile patients
needing permanent surveillance. The objective of this
project is to develop and implement innovative solu-
tions based on information technologies and wireless
communication for the benefit of those needing medi-
cal permanence. In first step, we propose to study the
issues related to the acquisition of medical informa-
tion concerning a patient via a set of wireless sensors
embedded in the patient himself. Secondly, we focus
on treatment and use of this information either by a
local contractor equipment (central device) with a ca-
pacity of calculation or offset after transfer in GPRS
and/or WiFi connection to a data server based at the
attending physician or hospital.
In this project, we will propose and evaluate solu-
tions to some of related problems that can be encoun-
tered in such an environment:
- Information dissemination between wireless sen-
sors and the central device (mobile phone for in-
stance)
- Sensors’ auto-configuration
- Authentication and security
The proposed solutions will be evaluated on an exper-
imental platform. This will be achieved by the help of
our medical partner LIM&Bio laboratory (LIM&Bio,
2009). Although the platform will not be tested on
real patients, but it will be a prototype proof of con-
cept taking into account experimental constraints re-
lated to vital parameters of the human body. Thus,
the diversity of information that can be collected,
their frequency, their importance as, for example, set
thresholds for various measurements and above which
an alert is sent to the doctor, are fixed by our medical
partner.
489
Faheem Y. and Boudjit S. (2010).
WIRELESS BODY AREA NETWORKS - Information Dissemination Analysis.
In Proceedings of the Third International Conference on Health Informatics, pages 489-494
DOI: 10.5220/0002798104890494
Copyright
c
SciTePress
2 ARCHITECTURE AND
POSITIONNING OF THE
PROPOSED PLATFORM
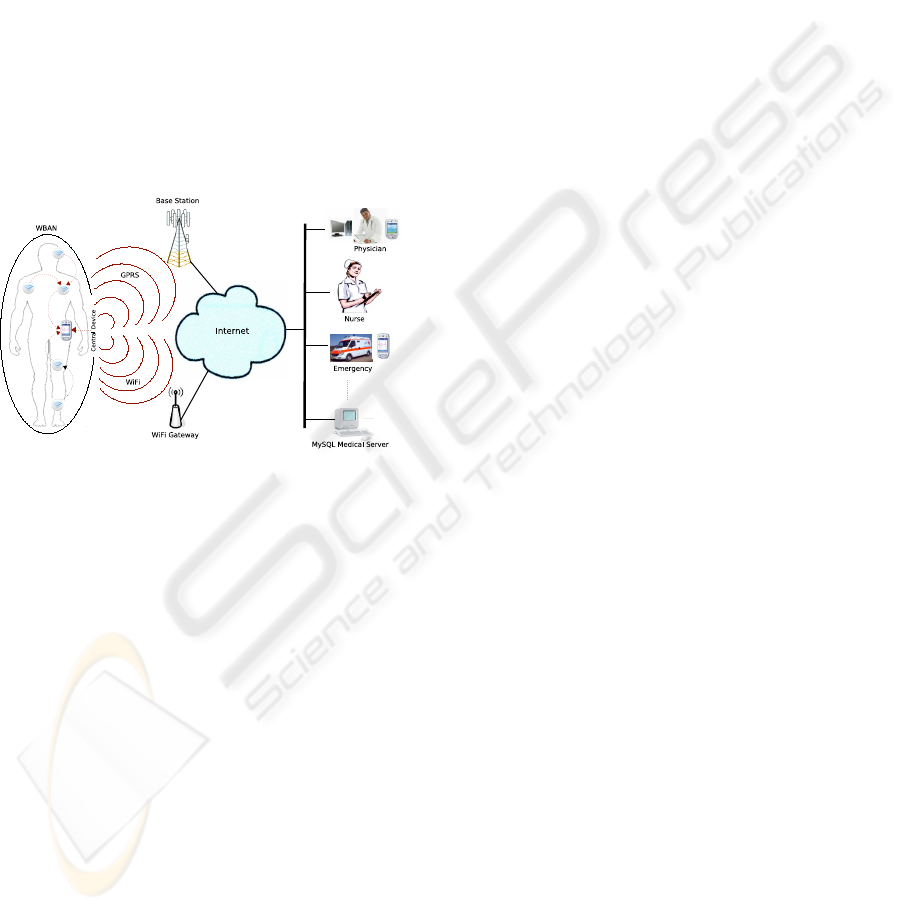
A general multi-tier system architecture is shown in
Figure 1; the lowest level encompasses a set of intel-
ligent sensors, the second level is the personal server
(central device) which could be an Internet enabled
PDA, a cell-phone, or a home computer. The third
level encompasses a remote health care server with
a set of its possible related users (Physician, Clinic,
Emergency). Each level represents a fairly complex
subsystem with a local hierarchy employed to ensure
efficiency, portability, security, and reduced cost. The
personal server, running on a PDA or a 3G cell phone,
provides the human-computer interface and commu-
nicates with the remote server.
Figure 1: Wireless Health Monitoring Platform.
There are several projects implementing platforms
for medical supervision at a distance. BASUMA (BA-
SUMA, 2006) is an example of such a platform of
which Philips is the consortium leader. Another simi-
lar platform called CodeBlue (CodeBlue, 2008) is be-
ing developed at Harvard University. However, these
platforms are typically installed in homes of patients,
and therefore limit patients’ mobility because they
must constantly be close to their Internet connection
for transmitting real time data. Secondly, security is-
sue has not been addressed in these platforms.
Our purpose in this work is to propose an archi-
tecture that combines several wireless technologies
(WiFi, ZigBee, GPRS) allowing patients to transmit
data in a secure manner to the remote health care
server regardless of their location.The proposed plat-
form will address the following issues:
• A Wireless Body Area Network (WBAN) com-
posed of various wireless sensors ultimately con-
nected to a retransmission device and commu-
nicating using wireless technologies like Blue-
tooth (Bluetooth, 2009) and ZigBee (Zigbee Al-
liance, 2009).
• A retransmitter device (central device), which
could be a cell-Phone or a PDA. This compo-
nent will implement the functions of active patient
monitoring, especially in the case of connection
loss with the remote server. It will serve as the
bridge between the WBAN and the global Inter-
net network and will also ensure the security and
confidentiality of that route.
• A remote server that collects all data from various
sources and stores it in database. It will gener-
ate statistics, information for doctors and alarms,
if any, that may be transmitted to a personal care
unit.
• The doctor or, generally speaking, the medical
staff will be the privileged consumer of platform
provided information. Due to this, user can have
multiple interactive interfaces:
– Standard web Interface: interactions with the
platform are done using a conventional web
browser.
– Mobile Interface: this interface will be de-
signed for personal digital assistants (PDAs) or
smartphones.
However, the establishment of such an architec-
ture requires solving certain scientific problems at all
the platform levels. Under this project, we concen-
trate our analyses on the patient side and we focus
on three key issues related to wireless body area net-
works: routing between sensors and the central de-
vice, sensors auto-configuration, and secure transmis-
sions.
3 OUR CONTRIBUTION
Several studies have shown that multi-hop routing
in WBAN result in non-negligible lifetime increase
of sensors as compared to direct communication be-
tween sensors and the central device. In this case, in-
formation dissemination between sensors and the cen-
tral device requires an ad hoc routing protocol.
Some other studies, however, argue contrarily.
They show that direct communication between sen-
sors and the central device considerably increase the
lifetime of a wireless body area network. They show
that executing a multi-hop adhoc routing protocol on
embedded sensors consumes more energy.
In this paper we are exploring both information
dissemination techniques in a WBAN scenario. Our
objectif here is to find a tradeoff between the number
of hops in the network and the energy consumption.
Energy consumption for various scenarios is evalu-
ated through simulations.
HEALTHINF 2010 - International Conference on Health Informatics
490
4 PROBLEM ANALYSES
Power consumption for transceivers is different
in different communication states i.e. transmis-
sion/reception/idle/sleep. Transmission energy de-
pends upon the power with which signal is propa-
gated to attain longer ranges while consumption in
other states is less variable. Unlike other technolo-
gies, reception/idle state consumption for low power,
limited range WSN is not negligible as compared to
transmission state power consumption. Thus global
energy minimization requires optimum selection of
transmission range. Latr
´
e et. al. in (Latre et. al.,
2004) showed that utilizing multi-hop communica-
tion by reducing transmission power in WBAN re-
duces overall energy consumption. This is true but
authors in (Latre et. al., 2004) ignore increased en-
ergy consumption due to multiple receptions. Wang
et. al. in (Wang et. al., 2006) propose a realistic
power consumption model for WSN. (Wang et. al.,
2006) shows that multi-hop communication is more
energy efficient when destination is out of reach. That
is when destination cannot be reached in single hop.
They show that multi-hop communication by control-
ling transmission power does not neccessarily result
in energy gain. This is due to non-negligible energy
consumptions in reception and Idle modes.
In sensor motes energy consumption in reception
and idle mode is relatively high. It can be equal to or
greater than transmission energy consumption for low
power transmissions. For low transmission ranges as
in WBAN, utilizing single hop data delivery to gate-
way node while other sensors are put in idle/sleep
state might be more energy efficient. Real experi-
ments conducted in (Anastasi et. al., 2004) show
that reception and idle listening consume a consider-
able amount of energy. Especially for sensor nodes,
very low power transmissions for ranges as short as
in WBAN consume lesser power than reception. For
micaZ motes (Chipcon AS, 2007), reception energy is
higher than transmission energy even with maximum
power transmission. Above stated variations in liter-
ature, motivated us to better understand this energy
consumption scenario and choose a better communi-
cation strategy for our future test bed implementation
for WBAN.
Figure 2: Simulation scenarios.
Table 1: Simulated scenarios.
Scenario
Hops
Distance
Nodes
1 1 60 n
s
→d
2 2 30 n
s
→n
4
→d
3 3 20 n
s
→n
3
→n
5
→d
4 6 10 n
s
→n
2
→n
3
→n
4
→n
5
→n
6
→d
Table 2: Mica2 Mote Power Consumption and Range Val-
ues.
Tx
power
(dBm)
Power
consumed
(mW)
Rx
power/Idle
power
(mW)
Tx
range
(meter)
05 76.2 30 60
-07 32.4 30 30
-14 27.9 30 20
-20 25.8 30 10
4.1 Channel Model and Energy
Consumption
Let P
t
and P
r
be the transmission and reception sig-
nal power respectively, where P
r
is equal to receive
sensitivity of mica2 node (-98 dBm). Let d be the
communicating nodes’ inter-node distance and, L the
system loss, then our WSN model can be represented
by the well known TwoRayGround radio model (NS2,
n.d.):
P
r
= ReceiveSensitivity =
P
t
G
t
G
r
h
t
h
r
d
4
L
(1)
Where G
t
=G
r
=1.2 are antenna transmission and
reception gains respectively. h
t
=h
r
=16cm are trans-
mission and receptor’s antenna heights. Transmission
power P
t
is varied according to desired range. Equa-
tion (1) can be rearranged to determine d for given
values of P
t
as follows:
d = [
P
t
G
t
G
r
h
t
h
r
P
r
L
]
1
4
(2)
We need minimum P
t
that ensures suc-
cessful reception of packet at destination with
P
r
>ReceiveSensitivity. For given values of P
t
,
approximate range values are obtained from radio
model given in (2). The actual power consumed by
mica2 while transmitting with permissible power P
t
is obtained from CC1000 data sheet (CC1000, 2007).
The range results for given P
t
(Table 2) conform to
WIRELESS BODY AREA NETWORKS - Information Dissemination Analysis
491
the MICA2 data sheet and experimentally obtained
range values.
Energy consumption of sensor nodes in various
states can be obtained by the following equations:
E
tx
= P
tr
× T
tx
E
rx
= P
rec
× T
rx
E
idle
= P
idle
× T
idle
where P
tr
, P
rec
, P
idle
are the powers consumed
by the Mica2 mote’s CC1000 transceiver in transmis-
sion, reception and idle mode respectively, and T
tx
,
T
rx
, T
idle
are times spent in each mode. Time for
transmitting a packet of size b bits is equal to [
b
R
]
where R is the data rate. Total energy consumed by
the network is given by;
E
total
= E
tr
+ E
Rec
+ E
idle
4.2 Simulations
Network Simulator 2 (NS2) is used for performing
simulations. We performed simulations utilizing the
actual power consumption values of sensor motes in
various states. In order to have an insight view of
the energy consumption in various working modes,
the power consumption values of Mica2 (Crossbow,
n.d.) sensor motes have been used. Mica2 has an on-
board CC1000 transceiver for communication. Thus
power consumption values for communication have
been taken from CC1000 data sheet (CC1000, 2007).
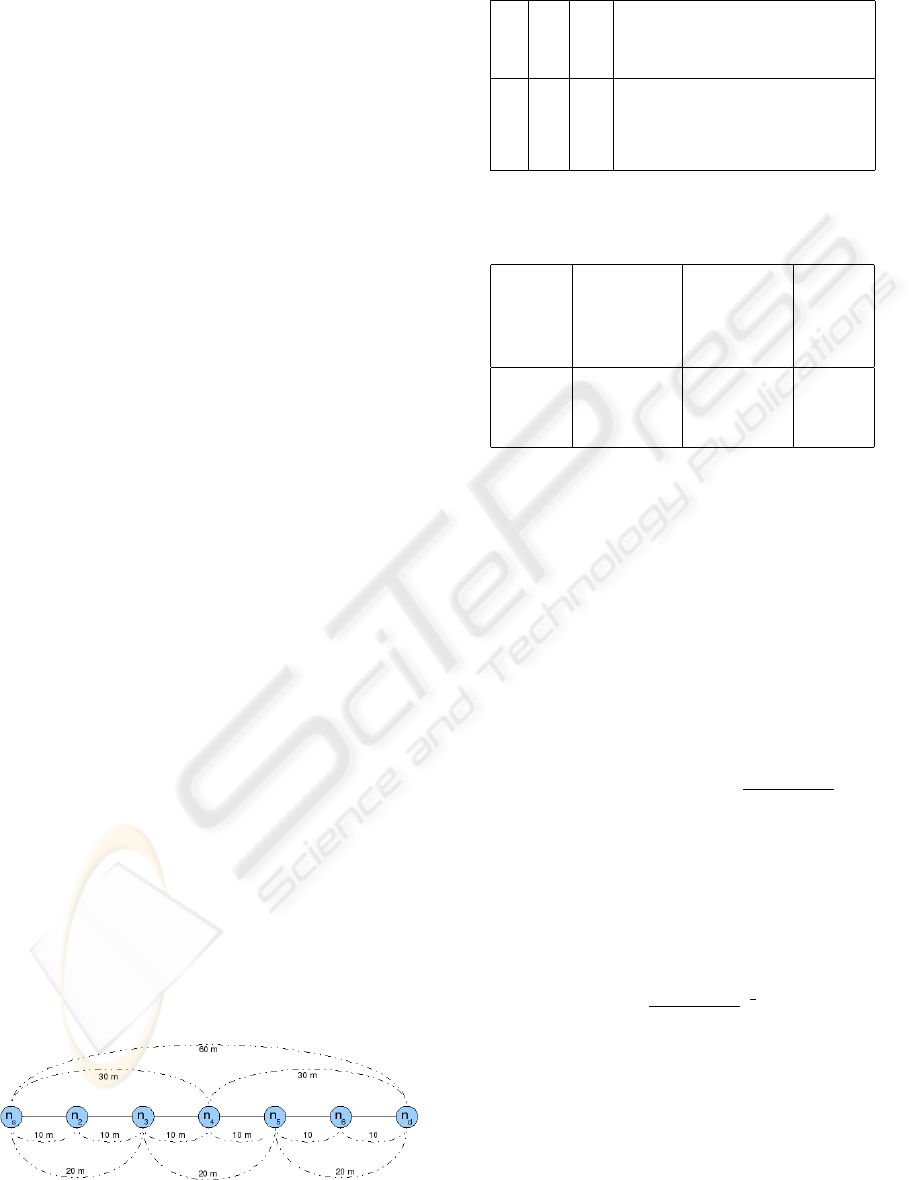
Deployed topology consists of a set of seven
equidistant nodes {n
s
, n
2
, n
3
, n
4
, n
5
, n
6
, n
d
} deployed
linearly with adjacent inter-node distance of 10
meters. This accounts to maximal source-destination
(n
s
→n
d
) distance of 60 meters. Source n
s
generates
packets at regular intervals and transmits them
towards sink n
d
. Simulations are performed with
four different relaying scenarios. Details are given in
figure 2 and in table 1. n
s
→n
d
transmission is varied
from single hop to a maximum of six hops. In all
the scenarios source node n
s
sends 50 bytes packets
towards desination node n
d
. MAC layer issues like
collisions, retransmissions and scheduling are not
taken into account. This is realistic assumption as the
goal here is to analyze only the energy consumption
effect with varying hop distances.
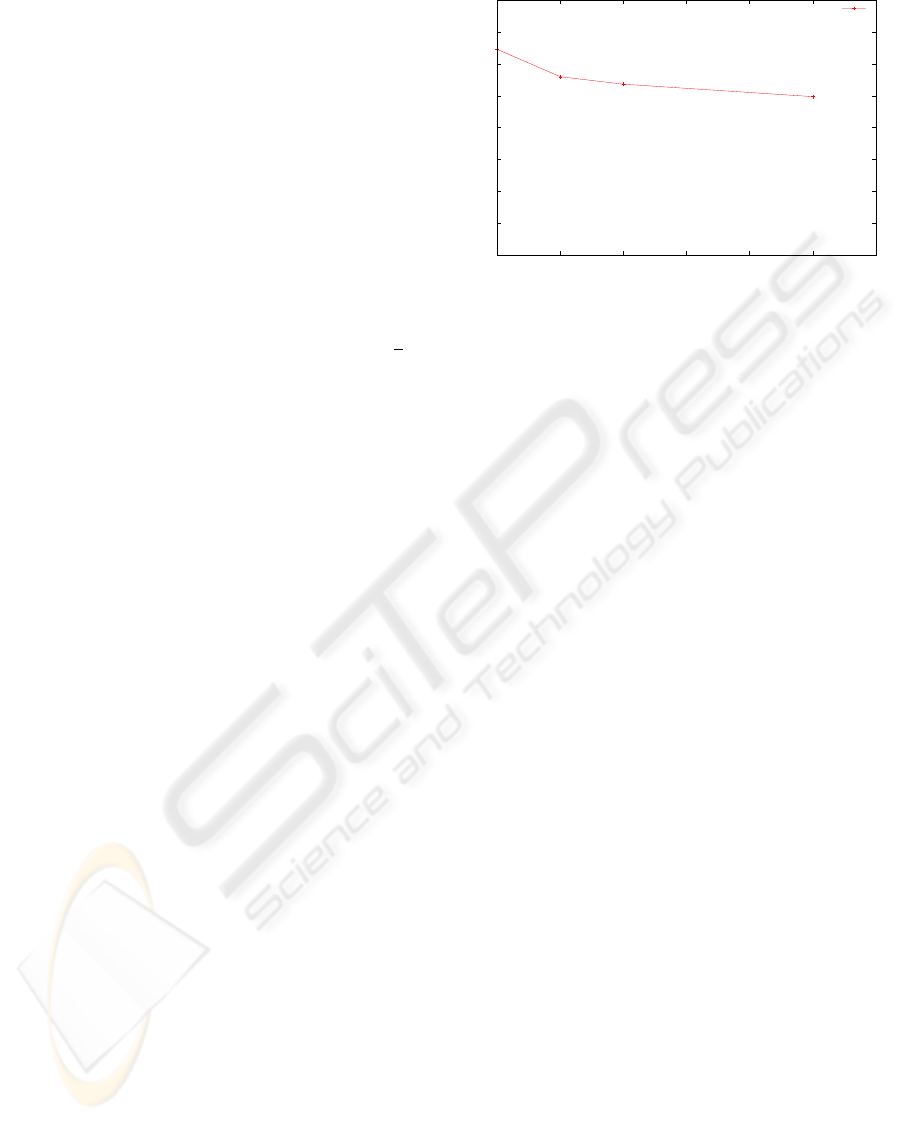
Figure 3 shows total network energy consumption
when radio is always active i.e. either in Tx/Rx state
or in idle state. In this case energy consumption re-
duces a bit with increasing number of hops. Note that
1
1.2
1.4
1.6
1.8
2
2.2
2.4
2.6
1 2 3 4 5 6 7
Energy (J)
Hops
Total Energy Consumption
"Consumption"
Figure 3: Total Energy Consumption when Radio always
ON/IDLE.
for this case P
rec
=P
idle
=30mW. This is because cur-
rent draw through mica2 is same when it is either re-
ceiving a packet or performing idle listening. Power
transmission values P
tr
for each case are obtained
from table 2. Energy consumption for direct n
s
→n
d
communication is 2.29J. For two hops n
s
→n
4
→n
d
and three hops n
s
→n
3
→n
5
→n
d
scenarios total energy
consumption slightly reduces to 2.12J and 2.07J re-
spectively. Results are not very appealing. With least
transmission power of -20dBm, that draws 25.8mW
from mica2, minimum total consumption of 1.99J is
acheived.This accounts to maximum energy saving
of 13% as compared to direct n
s
→n
d
communica-
tion. At -20dBm, power consumed P
tr
<P
rec
(25.8
<30mW). As compared to this, multiple WBAN sen-
sors are very close to each other (tens of centimeters)
and to the gateway node e.g. PDA. In such scenario
further reduction in transmission power will increase
multiple receptions/Listening dominancy over trans-
mission energy. Thus multi-hop option is not practical
in small WBAN. Heinzelman et. al. in (Heinzelman
et. al., 2000) propose a WSN based energy model.
They also conclude that multi-hopping is energy effi-
cient when destination cannot be reached in a single
hop. A contrary argument to this point could be that
transmission range reduction is neccessary to avoid
collisions and large number of overhearings. This is
true, but in small scale WBANs, source to sink syn-
chronized single hop communications while keeping
other nodes’ transceivers off would be more optimal.
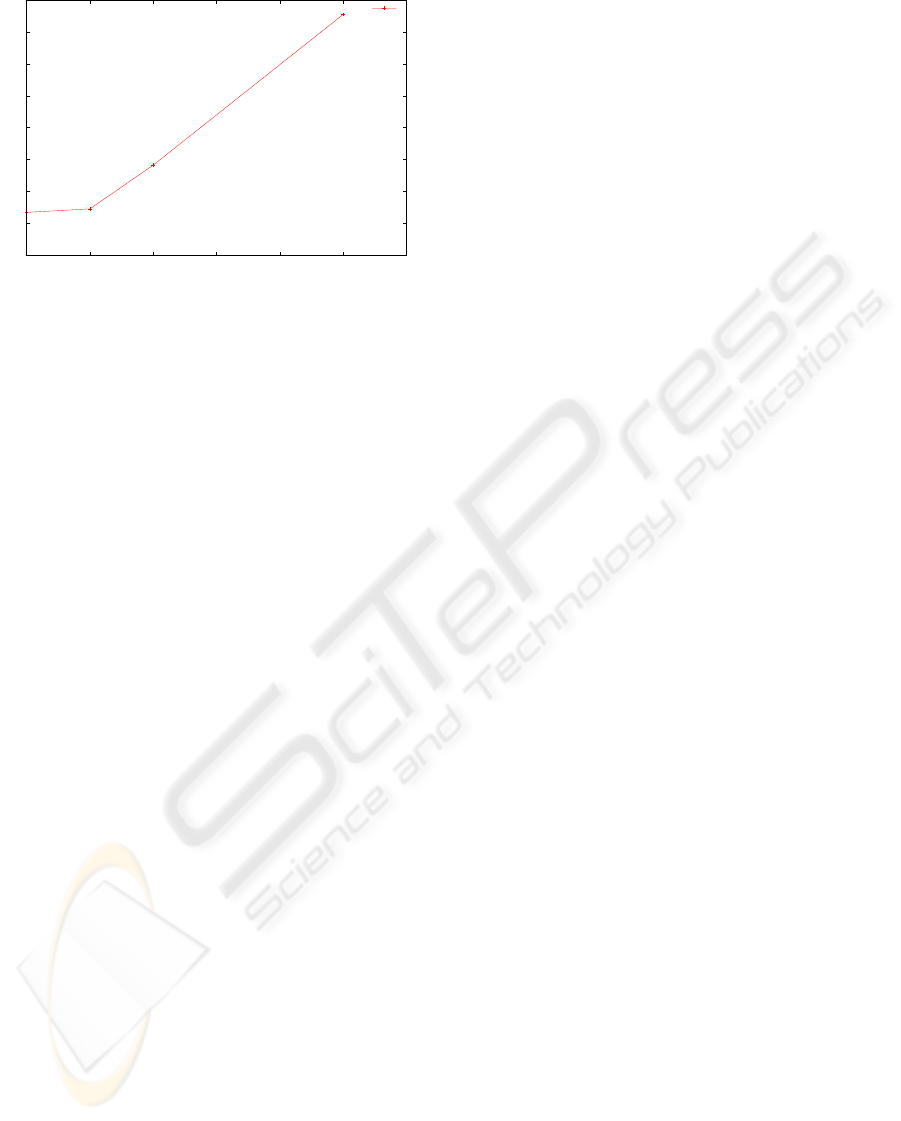
Figure 4 shows network energy consumption
when nodes switch on their radio only when they need
to transmit their information. Energy consumption for
direct n
s
→n
d
communication is 0.93J. For two hops
n
s
→n
4
→n
d
and three hops n
s
→n
3
→n
5
→n
d
scenar-
ios total energy consumption increases to 0.946J and
1.083J respectively. With least transmission power of
-20dBm, that draws 25.8mW from mica2, minimum
HEALTHINF 2010 - International Conference on Health Informatics
492
0.8
0.9
1
1.1
1.2
1.3
1.4
1.5
1.6
1 2 3 4 5 6 7
Energy (J)
Hops
Total Energy Consumption
" "
Figure 4: Total Energy Consumption when sensor node Ra-
dio ”ON” only for transmission.
total consumption of 1.55J is acheived.This accounts
to 40% increase in network’s total energy consump-
tion as compared to direct n
s
→n
d
. Clearly, reduc-
ing transmission range to perform data relaying does
not seem to be good option in WBAN. Energy effi-
ciency gain in WSN is maximum when sensor nodes
periodically go to deep sleep mode. We are not con-
sidering this case here as turning off health sensing
equipment may prove fatal to patient’s life. Patient’s
health needs to be regularly monitered and transmit-
ted to the concerned data center. Although the period-
icity of monitering depends upon the nature of obser-
vation and patients condition. It may not be necessary
to transfer health update to data center. This could be
utilized only under emergency condition to trigger the
call for medical assistance. From this discussion, it is
concluded that, unless really required, unneccessary
relaying should be avoided. Some real experiments
show high path atenuation values in WBAN with α
as high as 5.8. If such condition arrives the deployed
routing mechanism should be able to adapt itself for
multi-hop communication. For this reason, we aim
to adopt a simple routing protocol that uses a smart
neighbour discovery mechanism as in (Jacquet et. al.,
2003). This would allow nodes to communicate with
sinks over two hops, if required.
5 CONCLUSIONS AND FUTURE
WORK
An energy consumption comparison for various com-
munication scenarios has been made. It has been
shown that at very low ranges, transceivers consume
almost equal or more power on reception than trans-
mission. Thus deliberate reduction of transmission
range to induce multi-hop scenario is not efficient.
Though this is device dependent but general charac-
teristics of very low power transceivers seem to show
the same results.
Our future work is to propose an energy efficient, re-
liable routing architecture keeping in view the results
obtained through this study. Auto-configuration for
multi-hop relaying should be added in proposed rout-
ing architecture, in case when direct sensor to gate-
way access is not attainable. Security issues to ensure
patient’s unique identity will be dealt. At the end, we
plan to implement a real working WBAN prototype
on specialized wearable Shimmer sensors (Shimmer
Platform, n.d.).
REFERENCES
IEEE 802.15 WPAN Task Group 6 (TG6) Body Area Net-
works. (2003). 802.15.4 Standard. Retrieved Aug.
2009 from www.ieee802.org/15/pub/TG6.html
LIM&Bio: Laboratoire d’Informatique Medicale & Bio-
Informatique. Retrieved Jul. 2009 from www.limbio-
paris13.org
BASUMA. (2006). Body Area System for Ubiquitous Mul-
timedia Applications Project. Retrieved Sept. 2009
from www.basuma.de
CodeBlue: Wireless Sensors for Medical Care.
(2008). Retrieved 13, November 2009 from
http://fiji.eecs.harvard.edu/CodeBlue
Bluetooth Technology. (2009). Retrieved Oct. 2009 from
www.bluetooth.com
ZigBee Alliance. (2009). Retrieved Oct. 2009 from
www.zigbee.org
B. Latre, I. Moerman, B. Dhoedt, P. Demeester. (2004). Net-
working in Wireless Body Area Networks 5th FTW
PHD Symposium
Q. Wang, M. Hempstead, W. Yang. (2006). A Realistic
Power Consumption Model for Wireless Sensor Net-
work Devices IEEE Comm. Society Conference on
Sensor, Mesh and Ad hoc Communications and Net-
works
G. Anastasi et. al. (2004). Performance Measurements of
Motes Sensor Networks International Workshop on
Modeling Analysis and Simulation of Wireless and
Mobile Systems
Chipcon AS. (2007). CC2420 2.4 GHz IEEE
802.15.4/ZigBee-ready RF Transceiver Retrieved
Oct. 2009 from http://inst.eecs.berkeley.edu/ cs150/
Chipcon AS. (2007). CC1000 Single Chip Very Low Power
RF Transceiver. Retrieved from Oct. 2009 from
http://focus.ti.com/lit/ds/symlink/cc1000.pdf
Crossbow Technology MICA2 Motes Retrieved June, 2009
from www.xbow.com
W. R. Heinzelman, A. Chandrakasan, H. Balakrishnan.
(2000). Energy-efficient communication protocol for
wireless microsensor networks Proceedings of the
WIRELESS BODY AREA NETWORKS - Information Dissemination Analysis
493

33rd Hawaii International Conference on System Sci-
ences
P. Jacquet, P. Muhlethaler, P. Minet, A. Qayyum, A. Laouiti,
T. Clausen, L. Viennot, C. Adjih. (2003). Optimized
Link State Routing Protocol Internet Engineering Task
Force Group, RFC 3626
Shimmer Platform. (n.d.) Oct. 2009 Retrieved from
http://shimmer-research.com
Network Simulator 2 (n.d.). www.isi.edu/nsnam/ns/
HEALTHINF 2010 - International Conference on Health Informatics
494
