
THE ACCEPTANCE OF WIRELESS HEALTHCARE FOR
INDIVIDUALS
An Integrative View
Ing-Long Wu
1
, Jhao-Yin Li
2
, Chu-Ying Fu
3
, and Shwu-Ming Wu
4
1
Department of Information Management, National Chung Cheng University, Chia-Yi, Taiwan
2
Institute of Information Science, Academia Sinica, Taipei, Taiwan
3
Department of Information Management, Wu Feng Institute of Technology, Chia-Yi, Taiwan
4
Department of Human Resource Development, National Kaohsiung University of Applied Science, Kaohsiung, Taiwan
Keywords: Mobile Healthcare, TAM, TPB, Wireless Service, Personal Innovativeness
Abstract: A recent report showed that the adoption rate of mobile healthcare is relatively low. Thus, a study for how
healthcare professionals adopt mobile services to support their work is imperative in practice. An integration
of TAM and TPB has considered both technological and organizational aspects in a complementary manner.
However, while mobile healthcare is considered as an emerging technology with wireless features and often
used in a voluntary motive. The service provision for pervasive usage and individual psychological state are
critical in determining the system use. Accordingly, perceived service availability and personal
innovativeness in IT are the major drivers for the components of TAM and TPB. This study thus proposed
such a research framework for integrating these relevant components from a broader perspective.
Empirical research is further conducted for examining its practical validity.
1 INTRODUCTION
It is only quite recently that a surge of mainstream
popularity has motivated researchers to acknowledge
the value of mobile healthcare. Hospitals are the
places closely related to people’s health and medical
professionals are responsible for patients’ health and
life. Medical professionals always carefully concern
the risk or uncertainty in using new technologies for
helping medical treatments. Hence, medical
professionals usually tend to adopt new technologies
later until they have been growing more mature and
safe in their use. However, wireless technologies can
be widely applied in many ways to help medical
professionals complete their work safely and
efficiently, such as electronic patient record and
real-time monitoring system for heart rate variability.
This creates a great need and importance for mobile
healthcare in the hospitals. However, a recent survey
by the Taiwan government in 2007 indicated a quite
low adoption rate of mobile healthcare.
As technology acceptance model (TAM) focuses
more on technological aspect for its parsimony and
high explained power, however, it lacks considering
the effects of individual and organizational factors in
the adoption process. Theory of planned behavior
(TPB) is indicated with a consideration of these two
factors. Moreover, while mobile devices with
wireless features are portable for personal use and
provide instant supports for medical activities at
anytime and from anywhere, the quality of system
services, such as real-time service availability, is the
major concern for medical professionals to determine
the system use. Many studies have indicated the
same concern for understanding the adoption of
mobile devices, namely perceived service availability
(PSA) (DeLone and McLean, 2003; Venkatesh et al.,
2003; Hong and Tam, 2006). In addition, while
mobile healthcare is an emerging technology for
personal use and often used in a voluntary motive,
the psychological state of medical personnel
specifically plays a critical role in determining the
system use. Many researchers have considered the
same concern for identifying individual difference in
adopting a new technology, namely personal
innovativeness (Thong, 1999; Gallivan, 2003; Tayor,
2007). It is defined as personal innovativeness in IT
(PIIT) for IT context (Agarwal and Prasad, 1998; Yi
et al., 2006).
In sum, while many studies have proposed a
unified model primarily based on TAM and TPB for
various IS settings (Venkatesh et al., 2003; Wu and
124
Wu I., Li J., Fu C. and Wu S. (2010).
THE ACCEPTANCE OF WIRELESS HEALTHCARE FOR INDIVIDUALS - An Integrative View.
In Proceedings of the 12th International Conference on Enterprise Information Systems - Human-Computer Interaction, pages 124-130
DOI: 10.5220/0002864701240130
Copyright
c
SciTePress
Chen, 2005), we first integrated TAM and TPB in a
complementary manner. Moreover, for the
importance of PSA and PIIT in the particular mobile
healthcare, an enhancement of the unified view with
the two antecedents may positively increase the
explained power of a proposed model. Furthermore,
empirical examination is conducted for examining its
practical validity.
2 LITERATURE REVIEW AND
HYPOTHESES DEVELOPMENT
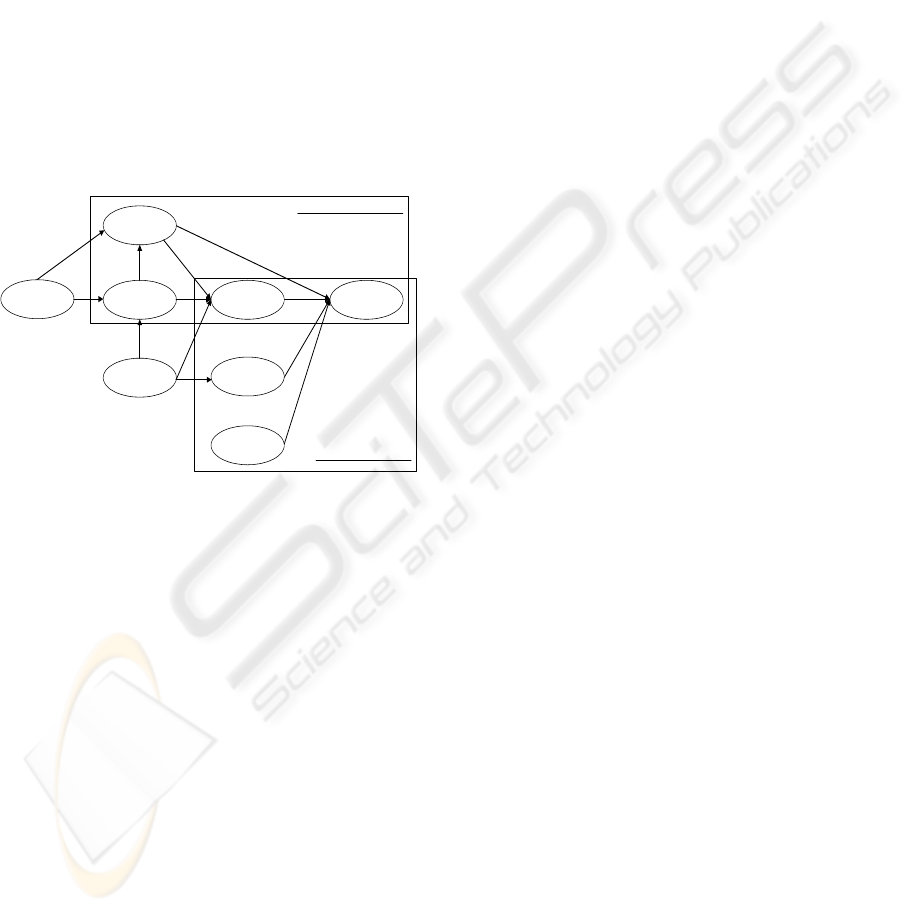
Based on the above discussion, Figure 1 provides a
pictorial depiction of this research framework. The
followings discuss the theoretical bases and
development of relevant hypotheses.
Perceived
Ease of use
Personal
Innovativeness
in IT
Perceived
Behavioral Control
Behavioral
Intention
Subjective
No rm
H1 1
H1 2
H7
H6
Attitude
Perceived
Service
Availability
Perceived
Us ef u l ne ss
H10
H5
H8
H9
H1
H2
H3
H4
Technology Acceptance Model
Theory of Planned Behavior
Figure 1: Research model.
2.1 Mobile Healthcare
Recent report has shown the importance of health
monitoring systems that can reduce the number of
readmissions for the patients suffering from many
chronic health problems (Toledo et al. in press). The
systems can also help in keeping track of patients
with one or more cognitive disabilities, such as the
stray prevention system for the elderly with dementia
(Lin et al. in press). Specifically, examples for
mobile healthcare include an implementation of
infrared and radio-based locator badges (Stanford,
2002), long-term health monitoring by wearable
devices (Jovanov et al. 2002), wireless sensor for
blood oxygen saturation monitoring (Asada, et al.
2003). Moreover, the use of wireless technologies
can also reduce long-term cost of healthcare and
result in an increased productivity of healthcare
providers. (Varshney, 2003).
2.2 TAM and TPB
TAM is designed for modeling user acceptance of
information technology (Davis et al., 1989). This
model hypothesizes these relationships, actual use
toward certain technology directly influenced by a
person’s behavioral intention to use (BI) and in turn,
behavioral intention to use determined by perceived
usefulness (PU) and attitude toward the technology.
Furthermore, perceived usefulness and attitude (ATT)
are affected by perceived ease of use (PEOU). TPB
differs from TAM by adding two components,
subjective norm (SN) and perceived behavioral
control (PBC). SN refers to the perceived social
pressure to perform or not to perform the behavior.
PBC refers to people’s perception of ease or
difficulty in performing the behavior of interest.
Consequently, Behavioral intention to use is jointly
determined by a person's attitude, subjective norm,
and perceived behavioral control toward the
behavior.
Some researchers have applied TAM and TPB
concepts on the use of telemedicine technologies for
healthcare professionals, such as WAP-based
telemedicine systems (Chau and Hu, 2002; Yi, et al.,
2006). The following discusses the development of
relevant hypotheses.
Based on TPB, there are three direct antecedents,
attitude, perceived behavioral control, and subjective
norm, for determining behavioral intention to use.
We can argue that three hypotheses are thus proposed
for them.
H1. Attitude has a positive effect on behavioral
intention to use mobile healthcare.
H2. Perceived behavioral control has a positive effect
on behavioral intention to use mobile healthcare.
H3. Subjective norm has a positive effect on
behavioral intention to use mobile healthcare.
Next, according to the TAM structure, as discussed
previously, we can argue that four hypotheses are
thus proposed for them.
H4. Perceived usefulness has a positive effect on
behavioral intention to use mobile healthcare.
H5. Perceived usefulness has a positive effect on
attitude toward using mobile healthcare.
H6. Perceived ease of use has a positive effect on
attitude toward using mobile healthcare.
H7. Perceived ease of use has a positive effect on
perceived usefulness for mobile healthcare.
THE ACCEPTANCE OF WIRELESS HEALTHCARE FOR INDIVIDUALS - An Integrative View
125

1.3 PIIT and IT Adoption
Personal Innovativeness represents the degree to
which an individual is willing to take a risk by trying
out an innovation (Flynn and Goldsmith 1993).
Personal innovativeness can be classified into five
types: innovators, early adopters, early majority, late
majority, and laggards. Personal innovativeness with
its application in information technology was first
termed personal innovativeness in IT (PIIT)
(Agarwal and Prasad, 1998, 1999). The following
presents the development of relevant hypotheses.
One study analyzed individual’s Internet anxiety, an
attitude toward the Internet use, when they may
experience perceived unreliability, risk, and
vulnerability from using it and suggested a
relationship between PIIT and the Internet anxiety
(Thatcher et al., 2007). Additional study discussed
the relationship between software developers’
innovativeness and their attitude toward a new
development process (Gallivan, 2003). We can posit
that one hypothesis is thus proposed for this.
H8. Personal innovativeness in IT has a positive
effect on attitude toward using mobile healthcare.
In the study of Yi et al. (2006) in terms of the
acceptance of PDA by medical professionals, the
PIIT is posited as a direct antecedent of perceived
behavioral control toward the behavior of adopting
PDA. Another study proposed PIIT as a determinant
of computer self-efficacy with respect to the use of
Window or Lotus software (Agarwal et al., 2000).
Moreover, computer self-efficacy has been indicated
as a determinant of perceived behavioral
control(Taylor and Todd, 1995). Therefore, the PIIT
has the indirect impact on perceived behavioral
control toward the behavior. We can argue that one
hypothesis is thus proposed for this.
H9. Personal innovativeness in IT has a positive
effect on perceived behavior control toward using
mobile healthcare.
A prior study indicated that PIIT is a significant
antecedent of perceived easy of use in terms of
knowledge workers in using IT (Lewis et al., 2003).
Another study indicated that higher PIIT leads to
higher perceived ease of use for financial service
software (Walczuch et al., 2007). We can assume that
one hypothesis is thus proposed for this.
H10. Personal innovativeness in IT has a positive
effect on perceived ease of use for mobile
healthcare.
1.4 PSA and IT Adoption
The use of mobile healthcare is closely related to the
patients’ health and life. Healthcare professionals are
usually hesitant to adopt a new system service, such
as mobile healthcare, while it is still in the early
development stage of its regular use. Among these
concerns regarding the mobile service, there is a
specific perception that relates to the unique features
of this service with wireless devices and its particular
usage context for patient safety. Perceived service
availability (PSA) refers to the degree to which an
innovation is perceived as being able to support
pervasive and timely usage. The following discusses
the development of relevant hypotheses. Many
studies have generally highlighted the importance of
service provision in determining the personal use of a
new mobile service (Islam and Fayad, 2003; Hong
and Tam, 2006). Specifically, one study indicated
that PSA is expected to have a direct effect on
perceived usefulness of a mobile data service (Hong
and Tam, 2006). We can posit that one hypothesis is
thus proposed for this.
H11. Perceived service availability has a positive
effect on perceived usefulness for mobile
healthcare.
The same study, as discussed above, also argued that
PSA has the direct influence on perceived ease of use
for the mobile data service (Hong and Tam, 2006).
The other study proposed that facilitating conditions
is a determinant of perceived ease of use for a new
technology (Venkatesh, 2000). Facilitating
conditions are defined as the provision factors in the
user environment to support the use of a new
technology (Venkatesh et al., 2003). We can argue
that one hypothesis is thus proposed for this.
H12. Perceived service availability has a positive
effect on perceived ease of use for mobile
healthcare.
3 RESEARCH DESIGN
3.1 Instrument
3.1.1 Basic Information
This part collects basic information about
organizational characteristics including hospital type
and bed size as well as respondent characteristics
including position, gender, working experience,
education level, and age.
ICEIS 2010 - 12th International Conference on Enterprise Information Systems
126
3.1.2 TAM and TPB Constructs
The measuring items for TAM constructs, including
PU, PEOU, ATT, and BI, were adapted from the
measurement developed by Venkatesh and Davis
(1996; 2000). They contain 4 items, 4 items, 4 items,
and 3 items respectively. The measuring items for
TPB constructs, including PBC and SN, were
adapted from the measurement developed by Taylor
and Todd (1995). They contain 3 items and 3 items
respectively.
3.1.3 PIIT and PSA
The measuring items for PIIT were based on the
recommendations of Agarwal and Prasad (1998) and
Yi et al. (2006), including 3 items. The measuring
items for PSA were adapted from the measurements
developed by Venkatesh (2000) and Hong and Tam
(2006), including 4 items.
3.2 Sample Design
Mobile healthcare is still in an early stage to use and
is considered to be a new technology for medical
professionals. It was assumed that larger hospitals
would be more likely to have this early experience.
We randomly selected 80 hospitals to be the study
sample from the population of 450 hospitals.
Furthermore, physicians and nurses in the hospitals
would be the major respondents since they are the
major users of mobile healthcare. We first sent an
invitation letter to one designated person in each
selected hospital and ask them for the help in
distributing questionnaires to their colleagues,
including physicians and nurses. After that, 10
questionnaires were sent for each hospital through
the designated person. A total of 800 questionnaires
were sent out to the potential respondents. 140 valid
questionnaires were successfully received. The
response rate was 17.5%.
3.3 Scale Validation
PLS is a structural equation modeling (SEM)
technique that employs a nonparametric and
component-based approach for estimation purposes.
This study uses PLS to analyze the measurement
model. PLS is the best analytical tool available to
fit the requirement of small sample size.
Convergent
validity is assessed by three criteria, factor loading
construct reliability, and average variance extracted
(Fornell and Larcker, 1981). Discriminant validity is
assessed by the measure that AVE for a construct
should be larger than the squared correlation between
the construct and other constructs. The testing results
indicate that convergent and discriminant validities
are all in a high acceptable level.
4 STATISTICAL ANALYSIS
PLS was used to examine the structural model. There
are two steps in evaluating the structural model.
First, we needed to estimate standardized path
coefficients and their statistical significance for
testing the hypotheses. PLS does not provide a
significance test or confidence interval estimation.
We re-sampled 1000 times with Bootstrapping
analysis to obtain a stable result for these analyses.
Second, the coefficient of determination (
2
R
) for
endogenous variables was calculated to assess the
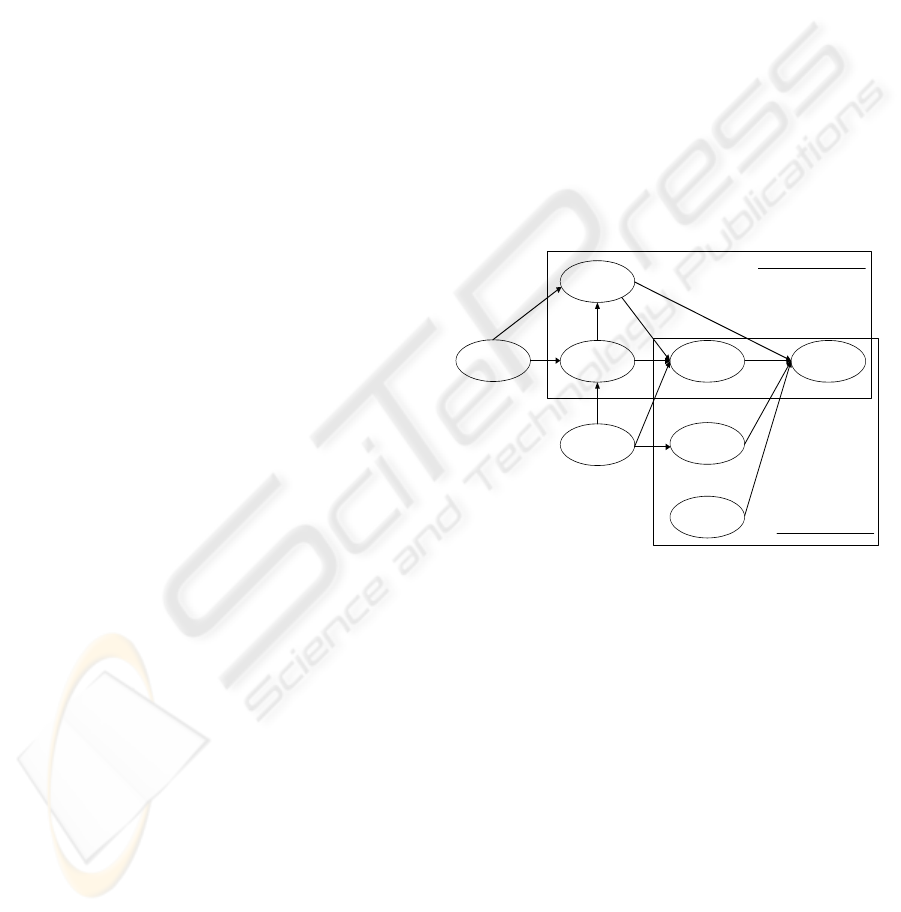
predictive power of this model. Figure 2 shows the
testing results of the structural model.
Percei ved
Ease of use
Personal
Innovativeness
in IT
Percei ved
Behavioral Control
Behavioral
Intention
Subjective
No r m
0.38*
0.13
0.40*
0.16
Attitude
Percei ved
Servi ce
Availability
Percei ved
Us e f ul n e s s
0.33*
0.60*
0.15
0.28*
0.22*
0.25*
0.23*
0.24*
Technology Acceptance Model
Theory of Planned Behavior
R
2
= 0.65
R
2
= 0.62
R
2
= 0.25
R
2
= 0.29
R
2
= 0.69
Value on path: Standardized coefficients (β),
2
R
: Coefficient of
determination, *: p<0.01
Figure 2: Result of the structure model.
For the components of TPB, attitude, perceived
behavior control and subjective norm are all reported
to be the important antecedents of behavioral
intention to use mobile healthcare (β=0.22, 0.25,
0.23). Therefore, Hypotheses 1, 2, and 3 are all
supported. For the components of TAM, perceived
usefulness has a significant positive impact on
behavioral intention to use (β=0.24). Hypothesis 4 is
thus supported. Perceived usefulness is a significant
determinant of attitude toward using mobile
healthcare (β=0.60). Hypothesis 5 is thus supported.
Perceived ease of use reveals no significance in
influencing attitude (β=0.16). Therefore, Hypothesis
6 is not supported. In contrast, perceived ease of use
plays a critical role in determining perceived
usefulness (β=0.40). Hypothesis 7 is thus supported.
THE ACCEPTANCE OF WIRELESS HEALTHCARE FOR INDIVIDUALS - An Integrative View
127

In a brief summary, the four constructs, attitude,
perceived behavior control and subjective norm, and
perceived usefulness, jointly explain 65% variance in
behavioral intention to use mobile healthcare
(
2
R
=0.65).
For the construct of PIIT, it indicates no
significant influence to attitude (β=0.15). Therefore,
Hypothesis 8 is not supported. Conversely, it is the
significant determinant of both perceived behavioral
control and perceived ease of use (β=0.28, 0.33).
Hypotheses 9 and 10 are thus supported. In a brief
summary, the three constructs, perceived usefulness,
perceived ease of use, and PIIT, jointly explain 62%
variance of attitude toward using mobile healthcare
(
2
R
=0.62). Next, PIIT singly explains 25% variance
of perceived behavioral control with respect to using
mobile healthcare. For the construct of PSA, it
indicates as an important antecedent of perceived
usefulness (β=0.38). Hypothesis 11 is thus supported.
In contrast, it is not a significant influencer of
perceived ease of use (β=0.13). Therefore,
Hypothesis 12 is not supported. In a brief summary,
the two constructs, perceived ease of use and PSA,
together explain 69% variance of perceived
usefulness (
2
R
=0.69). Next, the two unique features
for mobile healthcare, PIIT and PSA, jointly explain
29% variance of perceived ease of use (
2
R
=0.29).
5 FINDINGS AND DISCUSSIONS
This current model indicates a high explained power
for behavioral intention to use mobile healthcare with
2
R
=0.65 while compared the previous studies. This
may be because the four antecedents of behavioral
intention to use, that is, perceived usefulness,
attitude,
perceived behavioral control, and subjective norm,
are all significant in their influence. Among these
antecedents, perceived usefulness particularly plays
the same significant role as the three components of
TPB, attitude, perceived behavioral control, and
subjective norm. Research on the issue of integrating
TAM and TPB has shown mixed results for its
impact on behavioral intention to use (Wu and Chen,
2005). Moreover, perceived usefulness has much
greater influence on attitude toward using mobile
healthcare than perceived ease of use, (β=0.60 vs.
0.16). In a brief summary for the two findings,
perceived usefulness can be recognized as a
particularly important determinant for encouraging
the use of mobile healthcare in the hospitals.
Next, this study importantly indicates that PIIT is not
significant in determining attitude, but significant in
influencing perceived behavioral control. This
finding is particularly new for the adoption of mobile
healthcare while attitude is usually reported as the
major produced effect in the literature. This finding
also explains the above indication for the similar role
of perceived behavioral control in affecting
behavioral intention to use. More specifically, the
reasons to explain this are two-fold. First, while
mobile healthcare has been widely advocated and
recognized for healthcare professionals in the
hospital in order to improve healthcare quality
recently, the major problem for determining the use
of mobile healthcare is not the favorable or
unfavorable trait of healthcare professionals in the
psychological state rather than the externally physical
forces or control factors to encourage their usage,
such as the necessity of using this innovation to treat
patients in certain environments. Second, healthcare
professionals with high PIIT enforce their interest or
psychological state in favor of the use of mobile
healthcare and as a result, they perceive better
control or ease in performing the adoption behavior.
Finally, PSA, as an important determinant of
using new technology, significantly reveals the effect
on perceived usefulness and no effect on perceived
ease of use. This finding is particularly critical for the
use of mobile healthcare while most professionals
still thought that mobile healthcare is a type of
emerging technology for posing a difficulty to use.
This may have an indication for encouraging the
professionals to use this technology in the hospitals.
The reasons for these results may be noted as below.
For the former, mobile healthcare is closely related to
the patient life and its usefulness for healthcare
professional is greatly dependent on whether it can
be regularly operated regardless of the time and
places. For the latter, while the design of user
interface for mobile services has been in a stable and
consistent form for users, PSA may not be an
important determinant of perceived ease of use any
more at the current technological level.
6 CONCLUSIONS
AND SUGGESTIONS
The findings have important implications for both
practitioners and researchers. For the practitioners,
PSA initially drives the forces to determining
behavioral intention to use through two layers of
mediators in terms of TAM beliefs, that is, perceived
usefulness and attitude. This description basically
ICEIS 2010 - 12th International Conference on Enterprise Information Systems
128

relates to a particular technological issue in the
adoption of mobile services. This means that to
effectively encourage medical professionals to use
mobile healthcare, the provided service for pervasive
and timely usage without any difficulty should be
well prepared in the hospitals. Next, the TAM
belief (perceived usefulness) and PIIT have indicated
to be the underlying antecedents in determining
behavioral intention to use through the mediators of
attitude and perceived behavioral control respectively.
This means that both technological (perceived
usefulness) and individual issues (PIIT) are
important for overcoming the impediment of using
mobile healthcare.
For the technological aspect, the design of mobile
healthcare needs to carefully examine the functional
requirements of users and further is able to provide
useful information for helping the decision making of
medical professionals. For the individual aspect,
the hospitals may provide incentives for encouraging
medical professionals to be often kept in an
innovative manner with their regular tasks. This will
improve the willingness of an individual to take a
risk by trying out an innovation. Finally, the TPB
components, attitude, perceived behavioral control,
and subjective norm, involve the relevant
organizational and individual issues for indicating
their impact on the adoption of mobile services.
The hospital, as a type of organization’s form, should
be able to provide some training programs for
increasing the skill level of employees and nurturing
their confidence in facing new technologies.
For the researchers, prior research on information
technology acceptance in general and mobile services
in particular has been focused on the general
components of TAM or TPB. This research has
considered the roles of system services and personal
trait in the innovation acceptance. This is because
mobile healthcare with wireless features is an
emerging technology for medical professionals in
terms of high uncertainty in system services, great
change of their work styles, and real belief of its
usefulness. These considerations are particularly
important for the context of mobile healthcare. This
will provide a new thinking/concept for theoretically
defining the antecedents of behavioral intention to
use in the context of mobile healthcare.
Finally, although this research has produced some
interesting results, a number of limitations may be
inherent in it. Many studies have reported that gender
difference plays a moderating role for the
relationship between attitude, perceived behavioral
control, or subjective norm and behavioral intention
to use. Next, the response rate for this survey is lower
than desirable, despite the various efforts to improve
it. One of the reasons for this may be due to
inexperience of the respondents in using mobile
healthcare and reluctant to answer the questionnaire.
Finally, while medical doctors from larger hospitals
are always quite busy, few questionnaires may have
been completed by subordinates and therefore, the
data may have some biases.
REFERENCES
Agarwal, R. and Prasad, J. (1998). A conceptual and
operational definition of personal innovativeness in
the domain of information technology. Information
Systems Research, 9(2), 204–215.
Agarwal, R. and Prasad, J. (1999). Are individual
differences germane to the acceptance of new
information technologies? Decision Sciences, 30(2),
361–391.
Agarwal, R. and Karahanna, E. (2000). Time flies when
you’re having fun: Cognitive absorption and beliefs
about information technology usage. MIS Quarterly,
24(4), 665–694.
Asada, H., Shaltis, P., Reisner, A., Rhee, S., and
Hutchinson, R. (2003). Mobile monitoring with
wearable photoplethysmographic biosensors. IEEE
Engineering in Medical and Biology Magazine,
28–40.
Chau, P. Y. K. and Hu, P. J. (2002). Investigating healthcare
professionals’ decisions to accept telemedicine
technology: an empirical test of competing theories.
Information & Management, 39, 297-311.
Davis, F. D., Bagozzi, R. P., and Warshaw, P. R. (1989).
User acceptance of computer technology: a
comparison of two theoretical models. Management
Science, 35, 982–1002.
DeLone, W.H., and McLean, E.R. (2003). The DeLone and
McLean model of information systems success: a
ten-year update. Journal of Management Information
Systems, 19(4), 9-30.
Flynn, L R. and Goldsmith, R. E. (1993). A validation of
the goldsmith and hofacker innovativeness scale.
Educational and Psychological Measurement, 53,
1105-1116.
Fornell, C., and Larcker, D.F. Structural equation models
with unobservable variables and measurement error:
Algebra and statistics. Journal of Marketing Research,
18, 3 (1981), 382-388.
Gallivan, M. J. (2003). The influence of software
developers’ creative style on their attitudes to and
assimilation of a software process innovation.
Information & Management, 40, 443-465.
Hong, S.-J. and Tam, K. Y. (2006). Understanding the
adoption of multipurpose information appliances: the
case of mobile data services. Information Systems
THE ACCEPTANCE OF WIRELESS HEALTHCARE FOR INDIVIDUALS - An Integrative View
129

Research, 17(2), 162-179.
Islam, N. and Fayad, M. (2003). Toward ubiquitous
acceptance of ubiquitous computing. Communications
of ACM, 46(2), 89-92.
Jovanov, E., O’Donnel, A., Morgan, A., Priddy, B., and
Hormigo, R. (2002). Prolonged telemetric monitoring
of heart rate variability using wireless intelligent
sensors and a mobile gateway. The Second Joint IEEE
EMBS/BMES Conference, 1875–1876.
Lewis, W., Agarwal, R., and Sambamurthy, V. (2003).
Sources of influence on beliefs about information
technology use: An empirical study of knowledge
workers. MIS Quarterly, 27(4), 657–678.
Lin, C., Chiu, M., Hsiao, C., Lee, R., and Tsai, Y. (in
press). A wireless healthcare eservice system for
elderly with dementia. IEEE Transactions on IT in
Biomedicine.
Stanford, V. (2002). Using pervasive computing to deliver
elder care. IEEE Pervasive Computing Magazine,
10–13.
Taylor, S. and Todd, P. A. (1995). Understanding
information technology usage: A test of competing
models. Information Systems Research, 6 (2),
144–176.
Taylor, N. J. (2007). Public grid computing participation:
An exploratory study of determinants. Information &
Management, 44, 12–21.
Thatcher, J. B., Loughry, M. L., Lim, J., and McKnight, D.
H. (2007). Internet anxiety: an empirical study of the
effects of personality, beliefs, and social support.
Information & Management, 44, 353–363.
Thong, J. Y. L. (1999). An integrated model of information
systems adoption in small businesses. Journal of
Management Information Systems, 15(4), 187-214.
Toledo, P., Jimenez, S., Pozo, F., Roca, J., Alonso, A., and
Hernandez, C. (in press). A telemedicine experience
for chronic care in COPD. IEEE Transactions on IT
in Biomedicine.
Varshney, U. (2003). Location management for mobile
commerce applications in wireless internet. ACM
Transactions on Internet Technologies, 3(3) 221-232.
Varshney, U. (2007). Pervasive healthcare and wireless
health monitoring. Mobile Network Applications, 12,
113-127.
Venkatesh, V. (2000). Determinants of perceived ease of
use: integrating control, intrinsic motivation, and
emotion into the technology acceptance model.
Information Systems Research, 11(4), 342–365.
Venkatesh, V. and Davis, F. (1996). A model of the
antecedents of perceived ease of use: development
and test. Decision Sciences, 27(3), 451–481.
Venkatesh, V. and Davis, F. (2000). A theoretical
extension of the technology acceptance model: four
longitudinal field studies. Management Science, 46(2),
186–204.
Venkatesh, V., Morris, M., Davis, G., and Davis, F. (2003).
Use acceptance of information technology: toward a
unified view.
MIS Quarterly, 27(3), 425-478.
Walczuch, R., Lemmink, J., and Streukens, S. (2007). The
effect of service employees’ technology readiness on
technology acceptance. Information & Management,
44, 206–215
Wu, I. L. and Chen, J. L. (2005). An extension of trust and
TAM model with TPB in the initial adoption of
on-line tax: an empirical study. International Journal
of Human-Computer Studies, 62, 784-808.
Yi, M. Y., Jackson, J. D., Park, J. S., and Probst, J. C.
(2006). Understanding information technology
acceptance by individual professionals: toward an
integrative view. Information & Management, 43,
350-363.
ICEIS 2010 - 12th International Conference on Enterprise Information Systems
130
