
UNDERSTANDING ACCESS CONTROL CHALLENGES
IN LOOSELY-COUPLED MULTIDOMAIN ENVIRONMENTS
Yue Zhang and James B. D. Joshi
Information Science Department, University of Pittsburgh, Pittsburgh, PA, U.S.A.
Keywords: Access Control, Loosely-Coupled, Multidomain Environments, Policy Integration, RBAC.
Abstract: Access control to ensure secure interoperation in multidomain environments is a crucial challenge. A
multidomain environment can be categorized as tightly-coupled or loosely-coupled. The specific access
control challenges in loosely-coupled environments have not been studied adequately in the literature. In
this paper, we analyze the access control challenges specific to loosely-coupled environments. Based on our
analysis, we propose a decentralized secure interoperation framework for loosely-coupled environments
based on Role Based Access Control (RBAC). We believe our work takes the first step towards a more
complete secure interoperation solution for loosely-coupled environment.
1 INTRODUCTION
Access control poses a significant challenge to
ensure that data is exchanged and shared in a secure
way in a multidomain environment. We refer to this
as the secure interoperation problem (Gong, 1996).
In a typical scenario, a multidomain environment
may involve a small number of organizations closely
related to each other. They typically collaborate for a
common purpose and interoperations among them
need to be predefined to complete the common task.
We refer to such multidomain environments as
tightly-coupled environments. With the recent
advances in distributed systems and networking
technologies, such small and tightly-coupled
environments can not satisfy the fast growing
interoperation needs. Dynamic interoperations
among very large number of distributed domains
become not only feasible but also increasingly
popular. We refer to such an environment as the
loosely-coupled environment.
In the literature, the access control challenges in
tightly-coupled environments have been studied
extensively and they in general use global policy
based approaches (Gong, 1996; Shafiq, 2005). The
specific access control challenges in a loosely-
coupled environment, however, have not been
studied adequately in the literature. In this paper, we
focus on analyzing and identifying the access control
challenges in loosely-coupled environments. Based
on our analysis, we propose a decentralized secure
interoperation framework for loosely-coupled
environments. We believe this is the first step
towards solving all those challenges we identify.
Assuming that each individual domain employs
RBAC and the hybrid hierarchy, the proposed
framework consists of three components: Domain
Discovery, Trust Management, and Policy
Integration.
The rest of the paper is organized as follows. We
discuss the background of our work in Section 2. We
analyze access control challenges in loosely-coupled
environments in Section 3. The proposed secure
interoperation framework is described in Section 4.
We conclude our work in Section 5.
2 BACKGROUND
2.1 RBAC and Hybrid Hierarchy
In RBAC (Ferraiolo, 2001), users and permissions
are associated through roles. Any user assigned to a
role can acquire the permissions assigned to that
role. One of the most distinguished features of
RBAC is the role hierarchy, defining inheritance
semantics over roles. Joshi et al. have proposed
hybrid hierarchy containing the following three
relations (Joshi, 2002): permission-inheritance-only
(I-relation, ≥
i
), activation-inheritance-only (A-
356
Zhang Y. and B. D. Joshi J. (2010).
UNDERSTANDING ACCESS CONTROL CHALLENGES IN LOOSELY-COUPLED MULTIDOMAIN ENVIRONMENTS.
In Proceedings of the 12th International Conference on Enterprise Information Systems - Information Systems Analysis and Specification, pages
356-361
DOI: 10.5220/0002976903560361
Copyright
c
SciTePress
relation, ≥
a
), and the combined permission-
inheritance and activation hierarchy (IA-relation, ≥).
Semantically, x ≥
i
y means that permissions available
through y are also available through x; x ≥
a
y means
that any user who can activate x can also activate y;
and x ≥
y means that permissions available through j
are available through s and users who can activate s
can also activate j. Figure 1 shows the legend of our
paper. In hybrid hierarchy, if an I-relation precedes
an A-relation in the hierarchy, then there is no
permission acquisition relation between the two end
roles. Consider s ≥
i
r ≥
a
j. Here, the user assigned to
s can neither activate j nor inherit the permissions of
j through the I-relation between s and r.
Lemma 1: Users assigned to r
1
can acquire
permissions of r
2
if and only if there exists at least
one hierarchical path from r
1
to r
2
such that no I-
relation precedes an A-relation in the path.
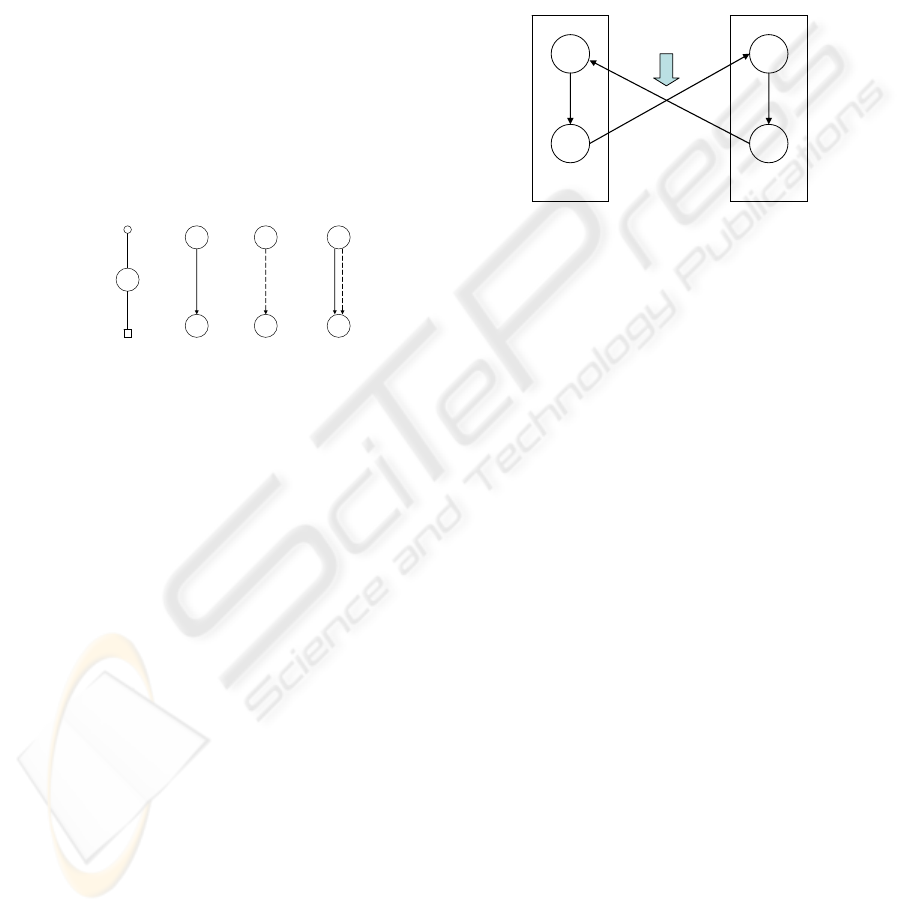
Figure 1: Legend of RBAC with Hybrid Hierarchy.
2.2 Secure Interoperation
Gong et al. (Gong, 1996) has proposed two
principles to the secure interoperation problem:
• Principle of Autonomy: If an access is
permitted within an individual system, it must
also be permitted under secure interoperation.
• Principle of Security: If an access is not
permitted within an individual system, it must
not be permitted under secure interoperation.
Typically, the principle of autonomy is ensured by
not changing the individual policy; and the principle
of security is ensured by detecting and removing the
access cycles. As shown in Figure 2, assume some
interoperation requires r
2
of domain d
1
to be made
senior of r
3
of d
2
, and another interoperation requires
r
4
to be made senior of r
1
. There is an access cycle
(r
1
, r
2
, r
3
, r
4
, r
1
) and the principle of security has
been violated since the users of r
2
are now
authorized to acquire permissions of r
1
in d
1
. In the
literature, many global policy based approaches have
been proposed (Gong, 1996; Shafiq, 2005) to
address the secure interoperation problem in tightly-
coupled environment. A global policy is predefined
by central administrators by integrating all
individual access control policies. And the access
cycles are detected and removed in the global policy.
In a loosely-coupled environment, global policy
cannot be used since the interoperation needs are
dynamic. Several trust management approaches
(Blaze, 1996; Li, 2002) have been proposed to make
dynamic authorization decisions based on trust
policies. However, trust management can only solve
a part of the access control challenges in loosely-
coupled environment, as shown in Section 3.
Figure 2: Example of access cycles during interoperation.
3 LOOSELY-COUPLED
ENVIRONMENTS
3.1 Characteristic
The domains in a loosely-coupled environment are
typically independent to each other and are able to
carry out their major functions themselves. The
interoperation needs are raised dynamically to share
the data whenever needed. Therefore, the
interoperation needs in loosely-coupled
environments are dynamic and cannot be pre-
defined. For example, consider a distributed health
care system (e.g. HL7) that consists of different
hospitals, clinic, health care station, and other
related organizations. Assume Bob travels outside
his hometown and needs to go to an emergency unit.
The local hospital (Hospital A) might need to access
his health information from his home hospital
(Hospital B) to provide him with a proper treatment.
This particular interoperation need is driven by a
specific event (Bob needs to go to the emergency),
and we cannot predefine that Hospital A should
always be authorized to access Bob’s health
information from Hospital B.
3.2 Specific Access Control Challenges
The first challenge is how to locate the domains that
contain the requested permissions in the access
r
s
j
s
j
s
j
user
role
user-role assignment
permission
senior role
junior role
I-hierarchy IA-hierarchyA-hierarchy
role-permission assignment
r
1
r
2
r
3
r
4
Domain d
1
Domain d
2
Interoperation links
UNDERSTANDING ACCESS CONTROL CHALLENGES IN LOOSELY-COUPLED MULTIDOMAIN
ENVIRONMENTS
357

request. Once a particular interoperation need arises,
the requesting domain may not know which domains
contain the requested permissions, and a look-up
mechanism is necessary to locate those domains. For
example, the health care workers in Hospital A
needs to know which hospital or clinic has Bob
registered and contains Bob’s health information.
Although in this example Bob may carry his health
care card that contains the information of his home
hospital, in general we cannot assume that the
requesting domain always knows a priori the
domains containing the requested permissions. One
possible solution is to use a centralized database to
maintain such global information (e.g. the hospitals
a patient has registered in). However, such
centralized database could become very complex
and hard to manage. Moreover, it could also be the
bottleneck and suffer from single point of attack.
Therefore, decentralized look-up approaches are
more desirable in loosely-coupled environments. We
refer to this problem as Domain Discovery problem.
This challenge shows that Domain Discovery is
necessary in loosely-coupled environments.
Figure 3: Access cycles in a loosely-coupled environment.
The second challenge is how to make an access
control decision for a particular interoperation
request. Global policy based approach cannot be
applied here since the interoperation needs cannot be
predefined. For example, at the time when both
Hospital A and Hospital B join the network, the
administrators cannot pre-define that Hospital A can
access Bob’s health information from Hospital B.
This is because such interoperation need is only
necessary when Bob needs to go to the emergency
ward in Hospital A and this may never happen. In
the literature, trust management systems are
typically used to make authorizations among
unknown domains. In a trust management system,
each domain specifies its local trust policy (typically
consists of credentials that is required to access
some resources), and employs some credential
validation and trust negotiation approaches to make
the authorization decisions. For example, when the
healthcare workers in Hospital A request Bob’s
health information from Hospital B, Hospital B may
require that only the users with valid healthcare
licenses be allowed access to Bob’s health
information, and ask healthcare workers in Hospital
A to present their license in order to gain the access.
Once the license has been verified, the access
request is granted and the healthcare workers in
Hospital A can now access Bob’s health information
from Hospital B. This challenge shows that a Trust
Management component is necessary in loosely-
coupled environments.
The third challenge is how to prevent the access
cycle and preserve the principle of security during
the interoperation. The access cycles could be
formed when multiple authorized interoperations co-
exist within the same time period. Consider the
example shown in Figure 3. Assume Bob is
registered and taken cared of at his home hospital
(Hospital B), where both the doctor and resident are
authorized to access his healthcare information. Of
course, doctors have more privileges, such as adding
a new entry to his record, so Doctor role is made
senior to Resident role in Hospital B’s local policy.
In Hospital A located at another city, healthcare
workers are responsible for maintaining normal
health care information. There are specialist doctors
that are all experts of cancer and they may need
special privileges to maintain cancer-related
information. Therefore, SpecialistDoctor is made
senior to HealthCare-Worker in Hospital A. Now
assume that Bob needs to go to the emergency ward
in Hospital A when he travels to that city. To take
care of Bob, the healthcare worker in Hospital A
needs to access Bob’s health care records and also
needs to add a new entry to Bob’s records. So
HealthCareWorker of Hospital A is made senior to
Doctor of Hospital B to facilitate such
interoperation needs (Interoperation 1 in Figure 3).
Assume at the same time, hospital B receives a
cancer patient but is unable to make a proper
treatment plan since they are not experts of cancer.
The doctor in hospital B asks the resident to get
some help from the specialist doctors in Hospital A
(e.g. accessing some cancer-specific information in
Hospital A to learn how to make the proper
treatment). As a result, Resident of Hospital B is
made senior to SpecialistDoctor of Hospital A to
facilitate such interoperation needs (Interoperation 2
in Figure 3).
At this time instant when both
interoperations 1 and 2 in Figure 3 are authorized,
there exists an access cycle (shown by the four
arrows) and the principle of security is violated.
Unlike in a tightly-coupled environment, there
is no static global policy in loosely-coupled
Specialist Doctor
HealthCare Worker
Doctor
Resident
Hospital A Hospital B
Interoperation 1
Interoperation 2
adding entries …
access health
care records…
maintain normal health
care information…
maintain cancer-specific
information …
ICEIS 2010 - 12th International Conference on Enterprise Information Systems
358

Figure 4: Architecture of our decentralized secure interoperation framework.
environments. Therefore, the existing access cycle
detection and removal approaches employed in
global policy based approaches in the literature
cannot be applied here. This challenge shows that
proper mechanisms to ensure principle of security
are necessary in loosely-coupled environments.
4 PROPOSED FRAMEWORK
Figure 4 shows the architecture of our decentralized
secure interoperation framework. The left part shows
the components involved when the domain is
providing resources to other domains’ access
requests, while the right part shows the components
when the domain is requesting resources from other
domains. An interoperation access request (iar) is
the access request such that the requesting domain is
different from the domain containing the requested
permissions, as defined formally below:
Definition 1 (Interoperation Access Request). An
interoperation access request, iar, is defined as a
tuple of <d
req
, P
dest
, r
req
>, where d
req
is the domain
issuing the request, P
dest
is the requested permission
set, and r
req
is the role in d
req
to access P
req
.
Note that users acquire permissions through roles in
RBAC. Therefore, besides the requested
permissions, the requesting domain should also
identify one of its local roles for its users to acquire
the requested permissions through. For example, an
iar= <Hospital A, {add an entry to Bob’s record,
read Bob’s record}, HealthCareWorker> specifies
that Hospital A requests to acquire the permissions
to edit and access Bob’s record through its
HealthCareWorker role. If authorized, all the users
of HealthCareWorker can acquire the requested
permissions.
4.1 Domain Discovery and Role
Mapping
Given an iar, we need to decide which domains
contain the requested permissions. First, the domains
receiving the requested permissions need to decide a
set of roles that contain a subset of the requested
permissions, and we refer to this as the Role
Mapping problem. Second, given the roles written
by the Role Mapping components of other domains,
the requesting domain needs to identify a set of
involved domains that together can provide exactly
the requested permissions.
In (Zhang, 2010), we have proposed a role-
mapping algorithm that can be used for the Role
Mapping component, and propose several domain
discovery protocols that can be used to identify the
involved domains. Based on the output of the Role
Mapping algorithm, we define the answer of iar as
below:
Definition 2 (Answer of iar). The answer of a given
iar=<d
req
, P
dest
, r
req
> by an individual domain d,
denoted by d.answer(iar), is the tuple of <d, P
contain
,
R
contain
>, where P
contain
⊆ iar.P
dest
is the subset of
requested permissions that is contained in d’s local
policy, and can be acquired through R
contain
, which is
a set of d’s local roles.
Role Mapping
interoperation access request: iar
answer to iar
Local Policy
local access
request: lar
answer
to lar
check
Domain
Discovery
check
interoperation access request: iar
answers to iar from other domains
interoperation session request: isr
Interoperation Policy
interoperation session request: isr
Trust NegotiationPolicy Integration
answer to isr: yes
no
update
check
check
yes
no
yes
answer to isr: no
Individual
Domain
modules when the domain
is requesting resources
modules when the domain is providing resources
UNDERSTANDING ACCESS CONTROL CHALLENGES IN LOOSELY-COUPLED MULTIDOMAIN
ENVIRONMENTS
359

Once the set of involved domains have been
identified by the Domain Discovery component, it
sends a session access request sar to each of the
involved domain, as below:
Definition 3 (Session Access Request). A session
access request, sar, is defined as <d
req
, r
req
, d
dest
,
R
dest
>, where d
req
and r
req
are the same as defined in
iar, d
dest
is the destination domain where sar is sent
to, and R
dest
= d
dest
.answer(iar).R
contain
is a set of
roles in d
dest
that the requesting domain wants to
assume.
Compared to iar, sar has a new field d
dest
since now
the requesting domain has identified a set of
involved domains and knows where to send its
request. Moreover, the requested permission set P
req
in iar is replaced by the requested role set R
dest
in
sar. Actually R
dest
is simply R
contain
specified in
d
dest
.answer (iar). For example, after Hospital B
returns the answer <Hospital B, {add an entry to
Bob’s record, read Bob’s record}, {Doctor}>,
Hospital A issues an sar = <Hospital A,
HealthCare-Worker, Hospital B, {Doctor}>
indicating that the users of HealthCareWorker in
Hospital A requests to acquire the permissions of
Doctor in Hospital B.
4.2 Trust Management
The Trust Management component is responsible for
deciding whether an sar should be authorized or not.
There are a lot of trust management approaches
proposed in the literature. Since our framework is
role-based, any role based trust management work
could be used here. For example, RT (Li, 2002) (a
role-based trust management language) can be used
in our framework to specify the relevant policies on
whether an sar should be authorized. In particular, if
users of HealthCareWorker in Hospital A can
prove Doctor in Hospital B according to the relevant
RT policies, sar = <Hospital A,
HealthCareWorker, Hospital B, {Doctor}> should
be authorized.
4.3 Policy Integration
Policy Integration component is responsible for
preventing access cycles and preserving principle of
security when facilitating an authorized sar. As
discussed before, the existing access cycle removal
approaches employed in global policy based
approaches cannot applied here. We propose a novel
policy integration approach that uses the special
semantics of hybrid hierarchy to prevent the access
cycles. For each authorized sar, we create an access
role for the requesting domain to access the
resources of the involved domain through hybrid
hierarchy, as defined below:
Definition 4 (Access Role). Given an authorized sar
= <d
1
, r
1
, d
2
, R
2
>, the access role of this sar, denoted
as ar (d
1
, r
1
)
,
is a newly created role in d
2
such that
∀r∈R
2
, we make r
1
≥
a
ar (d
1
, r
1
) ≥
i
r.
Figure 5a shows an example of the access role. We
can easily verify that the users of r
1
can acquire the
permissions of R
2
by activating ar (d
1
, r
1
), so the
interoperation has been facilitated. Consider the two
sars shown in Figure 5b. Although there is a cycle
(r
1
, r
2
, ar(d
1
, r
2
), r
3
, r
4
, ar(d
2
, r
4
), r
1
), there is no
violation of principle of security. This is beacuse in
d
1
the users of r
2
cannot acquire the permissions of
r
1
since there is an I-relation preceding an A-relation
in the path. This shows that as long as we use the
proposed policy integration approach by linking the
access role through hybrid hierarchy, the principle of
security will be implicitly preserved regardless of
the specific interoperation needs. We finally define
the interoperation policy and its checking rule:
Definition 5 (Interoperation Policy). Assume R and
AR represent the set of all roles and all access roles
in a domain d, the interoperation policy IP of d, is a
relation between AR and R: IP=AR×R
Definition 6 (Checking Rule of the Interoperation
Policy). A sar = (d
1
, r
1
, d
2
, R
2
) is said to be matched
in the interoperation policy if and only if: ∀r∈R
2
,
(ar(d
1
, r
1
), r)∈d
2
.IP
The interoperation policy is updated by the Policy
Integration component after the Trust Management
component has authorized an sar. Every time an sar
is received, we first check the interoperation policy
to see whether the sar has been authorized by the
trust management component. If not matched, we
run the Trust Management component to make the
authorization decision.
Figure 5: the use of access roles.
r
1
r
2
r
3
r
4
Domain d
1
Domain d
2
r
1
Domain d
1
r
3
r
4
r
5
ar(d
1
, r
1
)
Domain d
2
(a): sar=(d
1
, r
1
, d
2
, R
2
={r
3
, r
4
, r
5
}) (b): sar
1
=(d
1
, r
2
, d
2
, r
3
), sar
2
=(d
2
, r
4
, d
1
, r
1
)
ar(d
2
, r
4
) ar(d
1
, r
2
)
ICEIS 2010 - 12th International Conference on Enterprise Information Systems
360

5 CONCLUSIONS
In this paper, we analyze the specific access control
challenges in loosely-coupled environments, and
propose a secure interoperation framework to
address these challenges. The proposed framework
consists of three components: Domain Discovery,
Trust Management, and Policy Integration.
ACKNOWLEDGEMENTS
This research has been supported by the US National
Science Foundation award IIS-0545912. We thank
the anonymous reviewers for their helpful comments.
REFERENCES
Blaze, M., Feigenbaum, J., and Lacy, J. 1996.
Decentralized Trust Management. In Proceedings of
the 1996 IEEE Symposium on Security and Privacy
(May 06 - 08, 1996). SP. IEEE Computer Society,
Washington, DC, 164.
Ferraiolo, D. F., Sandhu, R., Gavrila, S., Kuhn, D. R., and
Chandramouli, R. 2001. Proposed NIST standard for
role-based access control. ACM Trans. Inf. Syst. Secur.
4, 3 (Aug. 2001), 224-274.
Gong, L. and Qian, X. 1996. Computational Issues in
Secure Interoperation. IEEE Trans. Softw. Eng. 22, 1
(Jan. 1996), 43-52.
Joshi, J. B., Bertino, E., and Ghafoor, A. 2002. Temporal
hierarchies and inheritance semantics for GTRBAC. In
Proceedings of the Seventh ACM Symposium on
Access Control Models and Technologies (Monterey,
California, USA, June 03 - 04, 2002). SACMAT '02.
ACM, New York, NY, 74-83.
Li, N., Mitchell, J. C., and Winsborough, W. H. 2002.
Design of a Role-Based Trust-Management
Framework. In Proceedings of the 2002 IEEE
Symposium on Security and Privacy (May 12 - 15,
2002). SP. IEEE Computer Society, Washington, DC,
114.
Shafiq, B., Joshi, J. B., Bertino, E., and Ghafoor, A. 2005.
Secure Interoperation in a Multidomain Environment
Employing RBAC Policies. IEEE Trans. on Knowl.
and Data Eng. 17, 11 (Nov. 2005), 1557-1577.
Zhang. Y., and Joshi. J. B. 2010. Role Based Domain
Discovery in Decentralized Secure Interoperations. To
Appear In Proceedings of the 2010 Collaborative
Technologies and Systems (May 17 – 21, 2010).
Chicago, IL.
UNDERSTANDING ACCESS CONTROL CHALLENGES IN LOOSELY-COUPLED MULTIDOMAIN
ENVIRONMENTS
361
