
EXPERIENCES IN REMOTE MONITORING OF PATIENTS
WITH CHRONIC DISEASES USING MOBILE TECHNOLOGIES
Jaime Galán-Jiménez, Alfonso Gazo-Cervero and José-Luis González-Sánchez
Polytechnic School of Cáceres, University of Extremadura, Avda. Universidad S/N, Cáceres, Spain
Keywords: Chronic Diseases, Biomedical Devices, Bluetooth, UMTS, J2ME, SOAP, MOBILE Tele-monitoring,
eHealth.
Abstract: During recent years the number of patients who suffer from chronic diseases has noticeably increased in
developed countries. This implies an increase both in costs and resource allocation of the health system and
in the commuting frequency to health centers by patients as well. These costs can be reduced by using
mobile communication technologies. In addition, these technologies can also be used to improve the
patients´ quality of life who suffer from chronic diseases, their relatives and caregivers. However, wireless
communications can be affected by interferences generated in the patient’s domestic environment. The work
presented in this paper describes an architecture which aims to improve assistance quality using health
monitoring services and remote monitoring of patients that suffer from chronic diseases.
1 INTRODUCTION
Medical care for chronic patients is becoming a
priority problem in developed countries, although
there is also a notable increase in developing
countries. It is estimated that chronic pathologies
will represent more than 60% of worldwide illness
in 2023. Heart failure is a chronic disease under
constant growing, mainly due to the ageing of
population and survival of patients with a heart
condition. This illness has a great impact over
cardiovascular problems, like diabetes and high
blood pressure.
Another emerging point is the cost for the health
system caused by the increase of hospital
admissions due to chronic heart failure.
Consequently, it is crucial to find steps that would
improve their quality of life. In this way, it is
possible to improve both the diagnosis of cardiac
events and to avoid or delay an admission to the
hospital and treatment compliance.
Current developments of mobile communications
technologies allow the creation of solutions for
health services and online monitoring not available
in the past. These solutions aim at reaching final
users who do not possess specific technological
knowledge.
The diagnosis of a chronic disease means to a
greater or lesser extent a decrease in both patient and
caregivers’ quality of life. The nature of the chronic
pathology usually implies regular monitoring with
continuous trips to health centers. Minimizing
commuting by patients to centers could increase
reaction time in potential complications. In some
cases, patients can be trained for making monitoring
tests in their own houses. However, this approach
can only be applied to a set of simple tests and
therefore raise uncertainty on obtained results.
Alternative solutions have been considered to make
homemonitoring more effective and efficient.
In the last few years, there has been considerable
research activity in wireless body area networks
(WBAN) (van Dam et al., 2001). MobiHealth project
(Van Halteren et al., 2004) has developed and trialed
a highly customizable vital signs monitoring system
based on a body area network and a mobile-health
service platform utilizing next generation public
wireless networks. For example, (Jovanov et al.,
2005) focus on computer assisted physical
rehabilitation by designing a WBAN based on
intelligent motion sensors. Other approaches like
(Latré, 2004) aim at developing energy efficient
network protocols for this kind of networks.
However, the use of different mobile and
wireless technologies can entail some problems
related to the effects produced if all of them operate
at once in the same environment: the interferences
they cause to each other. The simultaneous use of
93
Gal
´
an-Jim
´
enez J., Gazo-Cervero A. and Gonz
´
alez-S
´
anchez J. (2010).
EXPERIENCES IN REMOTE MONITORING OF PATIENTS WITH CHRONIC DISEASES USING MOBILE TECHNOLOGIES.
In Proceedings of the Multi-Conference on Innovative Developments in ICT, pages 93-98
Copyright
c
SciTePress

technologies and the way they transmit to the
medium in a reduced environment can generate
interferences that affect the performance of the
networks they make up. This results from the free
use of the industrial, scientific and medical bands,
which are internationally reserved, not intended for
commercial use and open to everyone who wants to
use them.
This work proposes the application of mobile
communications to track chronic disease patients
who need frequent trips to medical centers. The
technological infrastructure developed in this work
allows a selected group of patients to not modify
significant aspects of their daily life. This
infrastructure is composed by a network of
biomedical sensors and mobile devices. Biomedical
devices collect individual biomedical data, which is
sent through mobile devices to centralized
information systems from the infrastructure. Data is
directly obtained by patients who take their
measurements from their own houses by using
mobile communications. Thus, mobile
communication technologies minimize the number
of visits to health centers from patients and enhance
their quality of life as well as their relatives and
caregivers. The system provides information to
medical staff for managing different services
associated to medical monitoring, treatment
compliance control and alert receipt.
Thus, this document focuses on technical aspects
of the proposed architecture for a set of specific
pathologies and parameters in remote tracking as
well as on the deployment problems caused by the
existing interferences in patients’ home.
Following on from this Introduction, Section
Two focuses on pathologies, biomedical parameters
and monitoring devices. Section Three shows the
full system architecture whereas Section Four
includes information related to the deployment and
evaluation methodologies. Section Five shows a
study of the influence over mobile devices caused by
radio interferences. Finally, Section Six offers some
conclusions and future pathways for research.
2 PATHOLOGIES, PARAMETERS
AND BIOMEDICAL DEVICES
This work focuses on cardiology health service. Our
aim is controlling heart failures from hypertensive
patients older than 50 years and prone to weight
increase. In collaboration with (GRIMEX, 2010),
some meetings took place to identify pathologies
and biomedical parameters to track:
Weight Control. Liquid Retention. Patients' daily
weight is controlled due to potential anomalies
related to liquid retention. Weight thresholds have
already been considered regarding the actual health
state of chronic patients. A daily weight tracking
should be done to obtain a trend about these
variations. In case of rapid weight increasing,
alarms for medical staff are sent. We used a
Bluetooth weight control device model (A&D
Medical Precision Health Scale, 2010).
Heart Rate Control. Tracking of heart rate in
patients is conducted using individual
electrocardiography monitors. Measurements are
done on a daily basis and in case the patient is
feeling unwell. Similarly to weight control, alarms
that detect anomalies notify medical staff, who are
the ultimate responsible of patient care. The device
used for heart rate control is (Card Guard PMP
4
SelfCheck ECG, 2010), with Bluetooth capabilities.
Blood Pressure Control. Blood pressure is
another factor that would anticipate heart failure.
The patient conducts blood pressure measurements
on a daily basis using a blood pressure monitor. If
measurements are beyond a predetermined
threshold, an alarm to the medical staff is generated.
Similarly to weight control, there is a trend analysis
that shows variations of systole, diastole, and
arterial pulse in time. The Bluetooth blood pressure
monitor model used is (A&D Medical Digital Blood
Pressure Monitor, 2010).
3 GENERAL SYSTEM
ARCHITECTURE
This section presents the architecture developed for
this work, which is depicted in Figure 1. It is
composed of a communications infrastructure that
incorporates a set of biomedical sensors for chronic
patients distance monitoring.
The architecture components are:
Biomedical Devices (three each patient): they
obtain patients’ biomedical data (weight,
heart rate and blood pressure).
Mobile Devices (one each patient): Data from
biomedical devices is received and sent to a
central server.
Central Server: Stores and processes all data
that comes from measurements of the
monitoring processes.
INNOV 2010 - International Multi-Conference on Innovative Developments in ICT
94

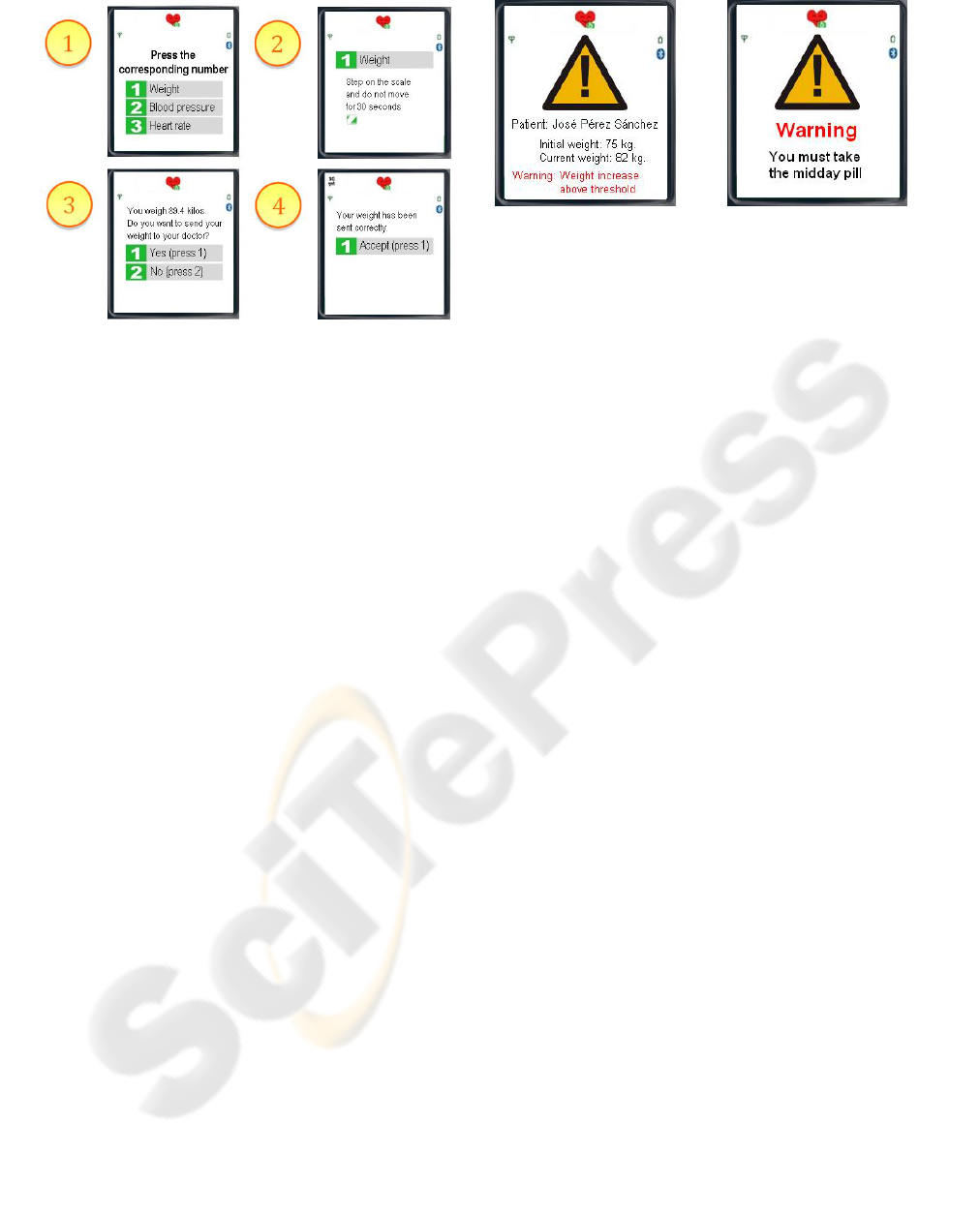
Figure 2: Example of weight monitoring and data sending.
4 DEPLOYMENT
AND EVALUATION
The deployment of the experiment has been carried
out with patients selected following a random
process. All of them are members of groups of
patients currently monitored in the Cardiology Unit
in the Don Benito-Villanueva de la Serena Hospital
of the province of Badajoz in Extremadura, Spain
(Pérez et al., 2009).
Inclusion criteria are described below:
Patients with diagnosis of chronic heart
failure (HF).
Recently hospitalized for this reason.
Currently in situation of medical stability.
Patients’ home inside an UMTS coverage
area (metropolitan areas of the region).
Exclusion criteria include:
Psychophysical handicap to do the
experiment or lack of assistance.
Fail a test about how to use the devices.
Refuse signing an informed consent.
Lack of UMTS coverage in the place
where patient lives.
A sample of 9 patients and duration of 6 weeks
were estimated for the period of the experiment.
With the aforementioned criteria, the study was
carried out on men and women between 49 and 69
years of age, both experienced in the use of mobile
communication technologies and without any
previous experience.
(a) (b)
Figure 3: Monitoring and treatment compliance alerts.
Results allowed doing a division into two clearly
distinct groups according to the age:
Group A (Aged 59-69): The five patients over 59
years old did not have any experience using mobile
devices. Three of them used biomedical and mobile
devices and carried out the tests with the help of any
other people. The other two patients lived alone with
their spouses and did not rely on the help of third
parties to use the devices and carry out the
measurements. The result of the experiment with the
patients that received some support was
optimum/satisfactory. However, in the case of
patients with no help, the result was deficient/not
satisfactory.
Group B (Aged 49-58): The four patients with
diagnosis of heart failure over 50 years old had
experience in the use of mobile devices and carried
out the tests autonomously, without help of third
parties. Result: optimum/satisfactory.
For those patients without experience in the use
of these technologies, the help provided by third
parties was fundamental. Problems arising from
patients that could not carry out the measurements
can be avoided with training both for the patient and
his family environment. Ergonomics and usability
both biomedical and mobile devices have been
essential in this pilot experiment. The main problem
detected when using biomedical devices was the
electrocardiography monitor.
Several interviews have been held with some
patients at the beginning, at mid-term and at the end
of the pilot experiment. Moreover, there was a final
survey for every participant, both doctors and
patients. Patients seemed to be keen on participating
within the experiments and admitted the validity of
the approach. Participating doctors also admitted the
validity of the system and the need of its integration
in health services.
INNOV 2010 - International Multi-Conference on Innovative Developments in ICT
96
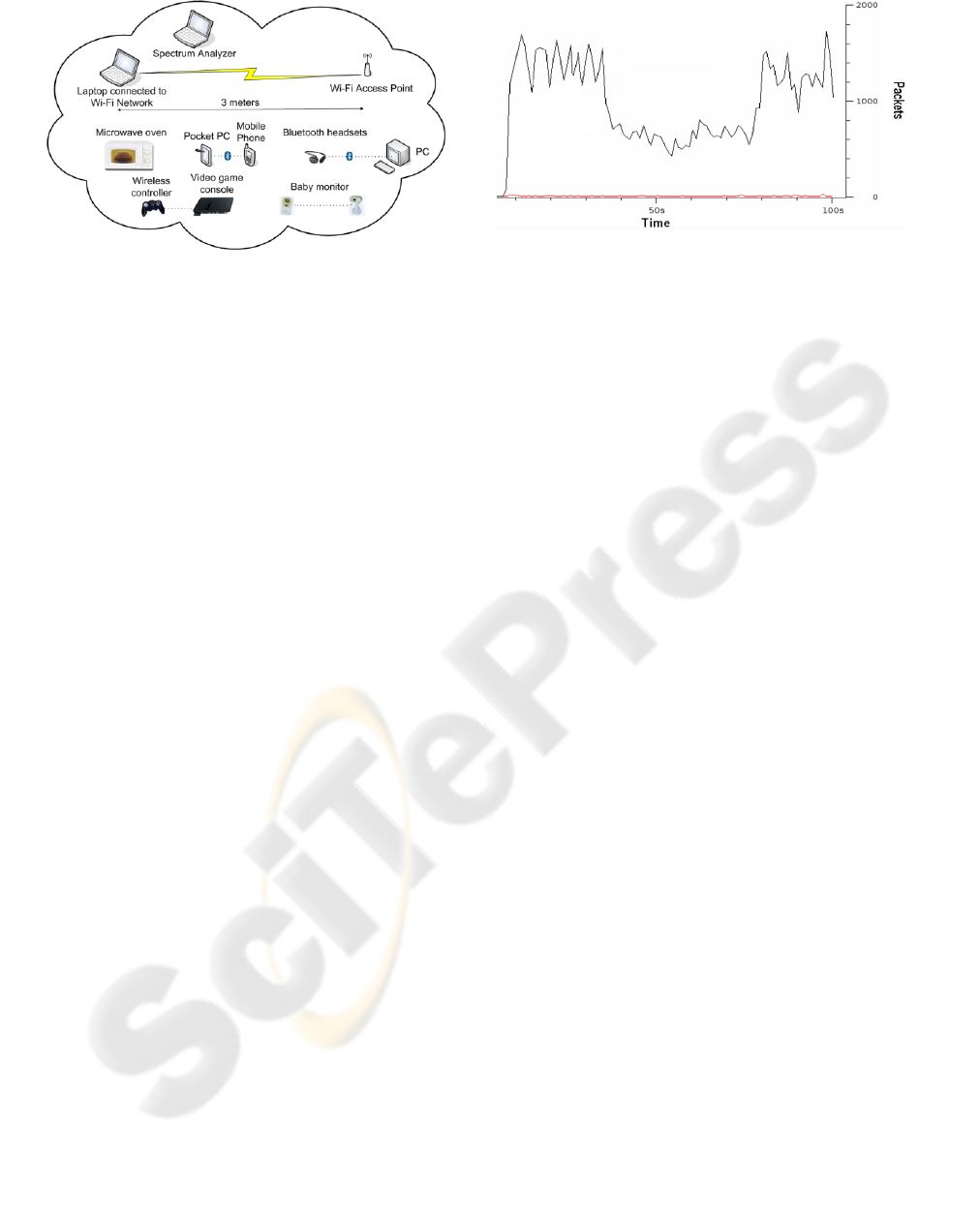
Figure 4: Test environment.
5 STUDY OF INTERFERENCES
IN MOBILE MONITORING
Another topic investigated is the effect produced
when mobile and wireless technologies are exposed
to certain situations in some interference
environments (Angrisani et al., 2008); (Mathew et
al., 2009); (Theuang et al., 2009). The simultaneous
use of these technologies and the way they transmit
to the medium in a reduced environment can
generate interferences which have negative effects
to the performance of the networks they make up.
This can cause a performance decrease during tests
when transferring data through the communication
established between biomedical devices and the
mobile device. This performance decrease could
also be evident when data is sent from mobile
device to the central server if there are devices
prone to generate interferences operating all at once
in the same environment. As an example, there is
some equipment inside hospitals that can cause
deficient performance of WLANs (Jiang et al.,
2009); (Subramanian et al., 2008).
In order to analyze interference among wireless
technologies, the WildPackets OmniSpectrum
Analyzer was used. We have also developed an
application to obtain real data about the
performance variation in these situations (Galán-
Jiménez et al., 2008).
Three types of tests have been done in this
study: 1) File download using FTP protocol. 2)
Download of the same file using HTTP protocol. 3)
A video file transmission using RTP protocol. The
three aforementioned tests have been carried out for
each of the following situations: file transfer via
Bluetooth, microwave oven, Bluetooth headsets
connected to PC, baby monitor and wireless video
game controller. In other words, we have introduced
a new source of interference to measure the
Figure 5: Performance graph of a HTTP download when
the source of interferences is a Bluetooth transfer.
variation of the wireless network performance
caused by these specific devices. All of these
devices can be found in any of the monitored
patients’ home. Figure 4 shows a scheme of the test
environment.
To obtain reliable and consistent results, tests
have been made following the same methodology:
1) With the spectrum analyzer we obtain the
interference values that a specific device
produces.
2) Next, we start a 100 seconds traffic capture and
the transmission to test.
3) After a 30 seconds interval, we switch on the
interference source to get the effect that it
causes to the wireless network performance.
4) This interference source is active for 30
seconds. Then, we switch the device off.
5) Finally, the capture and transmission finish 100
seconds after start.
Figure 5 shows the chart provided by the
developed software extension. It corresponds to the
HTTP download when the situation which generates
interferences is the file transfer via Bluetooth.
In Table 1, we can observe that the biggest
performance decrease is produced when the baby
monitor is switched on (100%), followed by the
microwave oven in which case is around 80%.
Otherwise, the test done with the Bluetooth headsets
does not affect to the performance of the wireless
communication. Test carried out with the wireless
video game controller and the file transfer using
Bluetooth technology affect to the test that involves
TCP traffic (around 45% of performance decrease),
but they do not affect to the multimedia
transmission with RTP.
By means of the last table, we can assure that
wireless technologies interact each other and their
simultaneous use limits their performance
depending on the type of traffic and on the devices
which are active in the same environment.
EXPERIENCES IN REMOTE MONITORING OF PATIENTS WITH CHRONIC DISEASES USING MOBILE
TECHNOLOGIES
97

Table 1: Percentage of performance decrease by test.
Transfer Device
FTP
Download
HTTP
Download
RTP
Transmission
Microwave oven
79 %
88 %
75 %
Bluetooth
transfer
40 %
50 %
0 %
Bluetooth
headsets
0 %
0 %
0 %
Baby monitor
100 %
100 %
100 %
Game controller
41 %
50 %
0 %
6 CONCLUSIONS
One of the immediate consequences derived from
the successful result of the work is the experience
about remote monitoring of patients with chronic
diseases. Among all of the technological
innovations contributed to this work, we emphasize
the use of biomedical sensor networks and their
communication with mobile devices in
environments where patients live. Besides obtaining
biomedical information, we have studied different
ways to send this information to central health care
systems from both clinical and operative point of
view. Third generation telephony has been taken in
advance to remotely monitoring patients through the
new developed medical Web site. We have
analyzed the effect of interferences among mobile
and wireless technologies over data transmissions in
similar situations like the existing ones in this type
of remote monitoring services.
Future research lines will allow identifying most
suitable patients’ profiles and pathologies to be
monitored using this kind of technologies. Benefits
and disadvantages of using them in communities’
creation could also be studied. These communities
are referred to both patients and people in their
environments. An early identification of the
problems in patients’ health would be possible by
using the information obtained by means of mobile
communication technologies. It would be feasible to
identify anomalies in treatment compliance as well.
ACKNOWLEDGEMENTS
We would like to express our sincere gratitude to all
doctors and patients who have participated in the
experiment. This work is sponsored in part by the
Ministry of Industry, Tourism and Commerce
through the MESEAS project (Ref. FIT-350301-
2007-14 PROFIT-S.I.).
REFERENCES
van Dam, K., Pitchers, S., Barnard, M., 2001. Body Area
Networks: Towards a Wearable Future. In
Proceedings of the WWRF Kick-off Meeting.
van Halteren, A., Bults, R., Wac, K., Konstantas, D.,
Widya, I., Dokovsky, N., Koprinkov, G., Jones, V.,
Herzog, R., 2004. Mobile Patient Monitoring: The
MobiHealth System. In The Journal on Information
Technology in Healthcare.
Jovanov, E., Milenkovic, A., Otto, C., de Groen, P. C.,
2005. A wireless body area network of intelligent
motion sensors for computer assisted physical
rehabilitation. In Journal of NeuroEngineering and
Rehabilitation.
Latré, B., 2004. Networking in Wireless Body Area
Networks. In Fifth FTW PhD Symposium, Faculty of
Engineering, Ghent University.
Grupo Investigador Multidisciplinar Extremeño. GRIMEX
Web Page. Retrieved on May 2010, from
http://www.grimex.org/index2.html.
A&D Medical Precision Health Scale UC-321PBT/UC-
321PBT-G. Instruction Manual.
Card Guard Personal Wireless 1 and 12-Lead ECG
Monitor. PMP
4
SelfCheck ECG.
A&D Medical Digital Blood Pressure Monitor Model UA-
767PlusBT. Instruction Manual.
Council Directive 93/42/EEC of 14 June 1993 concerning
medical devices. In Official Journal L 169, 12/07/1993
P. 0001 – 0043.
Pérez, R., Altuna, A., Fernández-Bergés, M., Galán, L.,
Lozano, L., Nijensohn, S., 2009. MESEAS: Mejora
del Servicio Asistencial. In II Conferencia
Internacional sobre Brecha Digital e Inclusión Social.
Angrisani, L., Napolitano, A., Sona, A., 2008. VoIP over
IEEE 802.11 wireless networks: Experimental analysis
of interference effects. In 2008 International
Symposium on Electromagnetic Compatibility – EMC.
Mathew, A., Chandrababu, N., Elleithy, K., Rizvi, S.,
2009. IEEE 802.11 & Bluetooth Interference:
Simulation and Coexistence. In Communication
Networks and Services Research Conference.
Tehuang, L., Wanjiun, L., 2009. Interference-aware QoS
routing for multi-rate multi-radio multi-channel IEEE
802.11 wireless mesh networks. In IEEE Transactions
on Wireless Communications.
Jiang, X., Howitt, I., 2009. Multi-domain WLAN load
balancing in WLAN/WPAN interference
environments. In IEEE Transactions on Wireless
Communications.
Subramanian, A. P., Gupta, H., Das, S. R., Jing, C., 2008.
Minimum Interference Channel Assignment in
Multiradio Wireless Mesh Networks. In IEEE
Transactions on Mobile Computing.
Galán-Jiménez, J., González-Sánchez, J. L., Carmona-
Murillo, J. D., Cortés-Polo, D., 2008. Performance
Evaluation and Analytical Study of the Effects among
Wireless Technologies. In Proceedings of the ACM-
DL Euro American Conference on Telematics and
Information Systems.
INNOV 2010 - International Multi-Conference on Innovative Developments in ICT
98
