
Service Tailoring: Towards Personalized Homecare
Services
Mohammad Zarifi Eslami, Alireza Zarghami, Brahmananda Sapkota
and Marten van Sinderen
Information Systems Group, University of Twente, Enschede, The Netherlands
Abstract. Health monitoring and healthcare provisioning for the elderly at
home have received increasingly attention. Since each elderly person is unique,
with a unique lifestyle, living environment and health condition, personalization
is an essential feature of homecare software services. Service tailoring, which is
creating a new service to meet individual requirements may be achieved in a
cost-effective and time-efficient manner if new services can be configured and
composed from already existing services. In this paper, we propose an effective
service tailoring process and architecture to personalize homecare services
according to the individual care-receiver’s needs. In addition, we present a
scenario to highlight the need for service tailoring and to demonstrate the
feasibility of the proposed approach.
1 Introduction
As computer networks are becoming widespread, the number of distributed services
available over networks grows rapidly [1]. However, these services are usually
designed for a general purpose, user or situation. In reality, different people have
different requirements, therefore they prefer personalized services. The requirements
for personalization reflect what the user wants, needs, and likes, all of which may
depend on the context at hand (for example, location, physical characteristics of the
environment, available resources, people nearby). Personalization also has an
evolutional aspect as requirements –demands, needs and preferences– of users change
over time. Services have to operate in a constantly evolving environment of people,
content, electronic devices, and legacy systems [2].
Thus, application functionality provided to users as services should (1) be aligned
with the uniqueness of each user's requirements, (2) evolve with changes in these
requirements, and (3) take the dynamic context of the user into account. Ideally this
would call for tailor-made services; however developing such services from scratch
would be economically and technically infeasible. A better approach would be to
reuse existing services, configure and compose them to satisfy the unique
requirements of each individual user. Service tailoring is a way of creating a new
service to satisfy the specific requirements of an individual user. Although service
tailoring is an essential feature in any application domain, we focus on homecare
application services. Tailorability has been studied extensively in the context of
Zarifi Eslami M., Zarghami A., Sapkota B. and van Sinderen M. (2010).
Service Tailoring: Towards Personalized Homecare Services.
In Proceedings of the 4th International Workshop on Architectures, Concepts and Technologies for Service Oriented Computing, pages 79-91
DOI: 10.5220/0003050900790091
Copyright
c
SciTePress

specific technologies and applications [3-7], but those approaches are not suitable for
homecare domain as homecare services have their own specifications such as high
dynamicity of user’s requirements and low level of user's technical skills [8].
To support well-being, health monitoring and independent living, there is an
increasing tendency to provide homecare services for the elderly, especially in
developed countries [9-11]. Several technological challenges concerning homecare
applications have been previously studied, but our focus is to address the uniqueness
of each elderly person by applying the service tailoring approach. Current homecare
systems are generally stand-alone for treating specific diseases, assuming a ‘standard’
patient and in a static situation [8]. However, in reality each user is unique in the way
he or she experiences or is affected by a disease or disability. This is not only because
of each individual’s mental and physical condition, but also because of the social and
physical environment. Current automated homecare systems are often technology-
driven. They can be difficult to use by non-technical users and difficult to change or
adapt when new requirements arise. The key question therefore is: how can services
be tailored to the requirements of the users in this domain, namely, care-receivers and
caregivers?
In this paper, we propose a service tailoring approach for the homecare domain.
The proposed service tailoring approach allows creating a new homecare service
through composing and configuring existing services, based on the user’s specific
requirements. Also, earlier tailoring results can be incrementally changed through
subsequent applications of tailoring to match evolving user’s requirements.
In Section 2, we define a scenario to motivate service tailoring for homecare. We
then define a generic service tailoring process in Section 3. This process is 'generic' in
the sense that it is independent of the knowledge and skills of the person who does the
tailoring. A tailoring architecture for implementing the tailoring process is proposed
in Section 4. This architecture identifies the components of a possible service tailoring
platform. In Section 5, by using a tailoring example applicable to our scenario, we
show how the proposed service tailoring process and architecture aid in creating a
personalized homecare service. Finally, we conclude our paper and discuss possible
future work in Section 6.
2 Example Scenario
To highlight the need for tailored homecare services, we use the following scenario:
“Jan and Linda are 74 and 67 years old respectively. Despite their age and having
various medical conditions, they prefer to remain living in their own home. They need
to take certain medicines at certain times. However, they suffer from Alzheimer’s
disease and may not remember when to take which medicines and how much. In this
situation, a reminder service may help them remember the prescribed time and a
dispenser service may help to take the correct dosage of the right medicines. There
may be situations in which the reminder and dispenser services may not be sufficient
to ensure that Jan and Linda actually take their medicines. Jan, for example,
sometimes ignores the reminder and does not take his medicine because he is too
disoriented. In such situations, assistance or help from other (voluntary or
professional) people is necessary. An alarm service may help detect such situations
110

and trigger a request for external help. Moreover, Jan has a hearing problem and
uses a hearing aid, and Linda cannot see well and so she must use glasses.
During the morning, they have their breakfast and Jan reads the newspaper on the
screen while Linda listens to the radio through the multimedia system. (There are two
multimedia interactive systems, one in the kitchen and one in the living room. These
systems include TV, radio, reminder texts and news, which users select via a
touchscreen). Then, they visit a park close to their home and meet their friends. They
usually have their lunch in a nearby restaurant. They spend most of their evenings at
home; Jan watching TV and Linda reading books. During the weekend, their children
usually come to visit them and Jan and Linda have other things to do and so they have
a different schedule than weekdays one. ”
As this example scenario shows, Jan and Linda have individual requirements and
preferences, and even the same person has different requirements and preferences
depending on the current situation and time. For example, for the medicine reminder
service, during the morning they prefer to have the reminder on the screen in the
kitchen or from the radio. After breakfast, if they go out as usual, they prefer to
receive the reminder on their mobile phone, and in the evening, Jan prefers to receive
his reminder on TV while Linda wants to receive it through her wheelchair vibrator.
Therefore, the desired services have to deliver their functionalities in various ways in
response to changing requirements, preferences and circumstances.
3 Tailoring Process
For doing tailoring, we assume three distinct types of users depending on the
individual knowledge and skill sets they possess: care-receiver (elderly people),
caregiver (family doctor, nurse or relative), and service developer (someone proficient
with the service-tailoring facility and the underlying technologies). A care-receiver
has contextual knowledge about his or her own needs and physical environment, but
probably possesses little domain or technical knowledge. A caregiver has domain
knowledge about healthcare practices and procedures, but probably possesses little
contextual and technical knowledge. Finally, a service developer has technical
knowledge about service modeling and technology, but probably possesses little
contextual and domain knowledge. Therefore, although the proposed tailoring process
is common among the different types of users, they may need different interfaces (for
tailoring) and may have various authoritative roles (levels of tailoring). However,
actors may have distinct roles when they are interacting with the system: Jan, for
example, is a care-receiver, but because of his knowledge in IT may also take on the
role of service developer.
The tailoring process consists of six different steps. These steps are illustrated using
BPMN notation in Figure 1, with each step having a corresponding activity. We do
not show a data flow in the figure because we present the process focusing on
tailoring platform view, regardless of its interaction with the user.
Of these steps, Steps 2, 3 and 4 are further refined into multiple activities. These six
steps and their constituent sub-activities are explained below. To show the feasibility
of the process and to make it easier to follow, each step is exemplified in Section 5.
111

Fig. 1. Service tailoring process in BPMN notation.
Step 1: Selecting the Target User
Our service tailoring process starts with specifying for who the service is being
created. The user data, such as age, their specific functional requirements and health
status, is stored in a user profile. When a target user is selected in this step, the data
stored in the corresponding user profile is used for tailoring the service in the other
steps to suggest the candidate services, with proper configuration, to the user. For
example, if Jan is chosen as a target user (care-receiver), the system knows that he has
a hearing problem and will not offer him any services that use sound.
Step 2: Selecting the Services
Originally, the web was designed for human-human communication, but later it also
become a machine understandable information space [12]. This is also true for web
services. The goal of designing web services was not only to interact with humans,
but also with other applications [13]. This means that data exchanged among services
carry semantics. So the semantics has been used to provide machine-understandable
information and enable services or frameworks to exploit machine-understandable
information to facilitate interoperability. The semantics help systems to automate
various aspects such as discovery, invocation and composition. Moreover, utilizing
semantic similarities among components and services improves adaptability in
selection. For adding semantics to our tailoring process, we exploit ontology. The
ontology aids the tailoring framework to understand user requirements and thereby
discover and suggest services which suit the best to these requirements.
Creating a new integrated service by a nontechnical user is a difficult task: the user
needs to know which existing individual services do what. To make the job easier for
the user, a goal-based method [14, 15] can be used. Goal-based methods have been
used in different areas of computer science to identify stakeholder’s objectives,
discover requirements for software systems and guide the system’s behavior. In
service-oriented computing goals can be used to express users’ requirements.
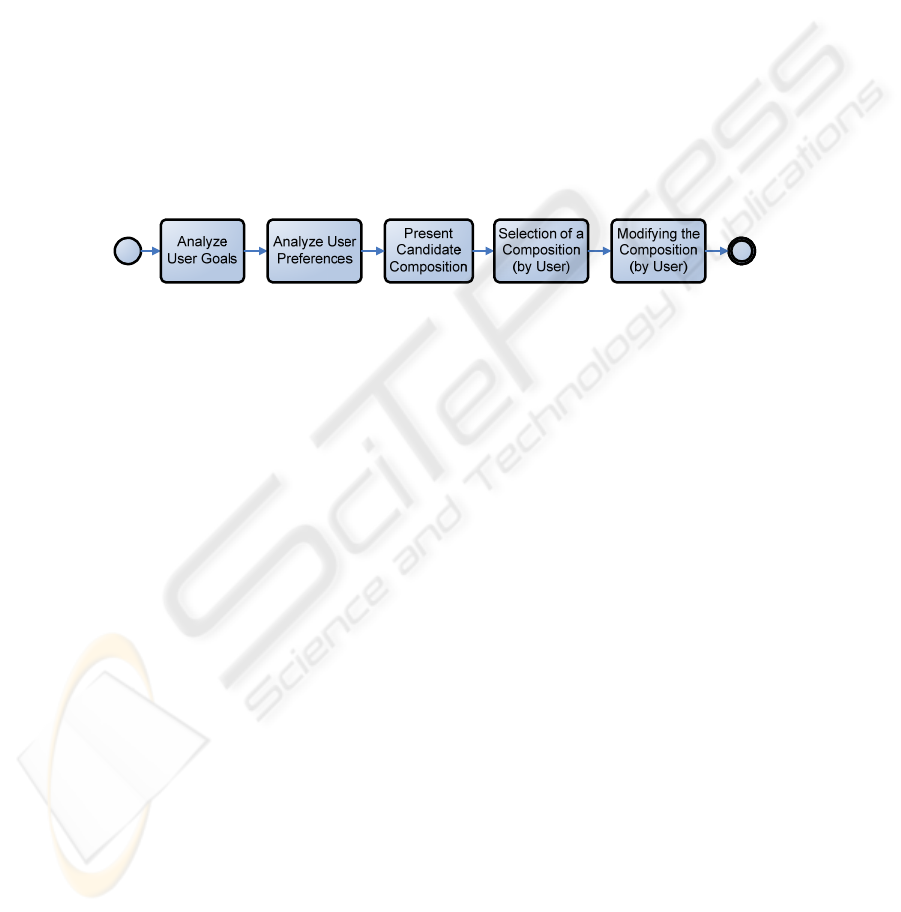
The second step includes five activities as shown in Figure 2:
Fig. 2. Step 2: Selection of services.
112
In this step, first user specifies care-receiver’s goals (requirements and preferences).
The tailoring platform utilizes the goal ontology for homecare domain to analyze user
goals and preferences. The aim of using a goal ontology is to minimize possible
terminological heterogeneities due to autonomously created goals (user requirements)
and tasks (existing services). Besides a goal ontology, a task ontology is needed to
associate existing services with their support functions (tasks). Once a user asks for a
service (determine his or her requirements), the tailoring platform matches the user
goal (requirement) with the proper task existed in the task ontology. Then it tries to
find and select the services associated with that task and suggests it to the user.
Therefore, a goal based method can be used to help users in service requests. In this
manner the users have a way of expressing what they want at a higher abstraction
level.
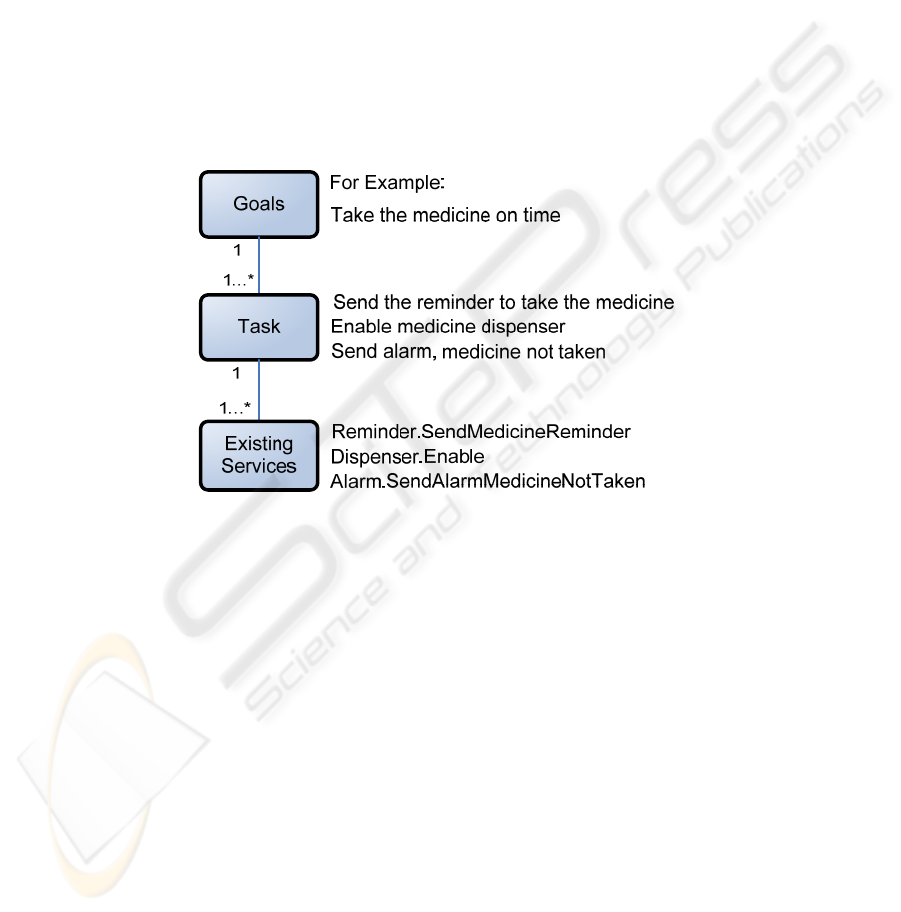
As shown in Figure 3, the user goals are more objective and nonfunctional, which is
easier to be understood by a non-technical user. Whereas tasks are functional but not
concrete, and existing services are more concrete.
Fig. 3. How user goals wind up to the system services.
After identifying the user goals and preferences, for presenting the candidate
services, the service tailoring platform finds and suggests several suitable services. To
do so, the service tailoring platform utilizes a repository of services and a task
ontology which depicts functionalities provided by these services. Each goal in the
goal ontology is associated with a set of tasks in the task ontology. Therefore, after
identifying the goal, the tailoring platform finds the most suitable tasks and then
suggests relevant services to the user.
The tailoring platform also uses the recommendations besides the goal based method
to suggest certain services to the user. The recommendations, using other care-
receivers’ information to suggest certain existing services which are used by them, in
a similar context [16]. As an example, assume that Ben is another elderly person who
lives at his own home with similar requirements as Jan. They both use medicine
dispenser service. If Ben uses an alarm service with the medicine dispenser, the
tailoring platform of Ben recommends the use of alarm service to Jan’s tailoring
113
platform through the network of homecare applications. Then the alarm service will
be recommended in the service selection step. However, services in homecare must be
selected carefully; any recommendation must be confirmed by an authorized user as
will be explained in Step 5.
Later, for selecting services, the caregiver selects his desired services from the set of
services suggested in the previous step by the tailoring platform. In this way, the user
selects explicitly desired services. However, the tailoring platform may also select
additional services because of service dependencies. Some services may need or
recommend other services’ functionalities to work, as a precondition. This means that
–based on user-selected services– the system adds or removes certain other relevant
services. For the second part, we use the service bundling techniques [17, 18]. In a
service bundle, dependencies between services are utilized to help a user to select and
discover services automatically and without the user intervention.
Step 3: Composing the Services
The third step includes five activities as shown in Figure 4:
Fig. 4. Step 3: Composing of services.
In this step, the tailoring platform composes the chosen services to satisfy the user
requested requirements. This composition is done based on the given user goals and
stored preferences in the user profile. Then this composite service(s) will be presented
to the user through our tailoring platform. Predefined service compositions, stored in
the Composition repository by the service developer. To suggest the proper
composition, we can exploit the Event-Condition-Action (ECA) rules. An ECA rule
has the general syntax on event, if condition, do actions. The event part specifies
when the rule should be triggered, which, in our case, can be the user goals. The
condition part specifies the conditions of this event, which, in our case, can be again
the user goals or preferences (configuration of services). The action part states the
actions to be performed automatically if the condition holds. In our case, this action
can be the suggested composition to the user. Therefore, ECA rules can be expressed
as conditions for decision making and can be used for configuration of services or
composition [1, 19].
After presenting the suggested compositions, the user should select one of them. The
user can also edit the desired composition, for example, changing the candidate
services in the composition or their order in the suggested composition. To allow user
to edit the composition, we use a mashup-like technique [20, 21]. Unlike developer-
centric composition techniques, mashup provides a user-friendly graphical approach
to compose services and applications.
Step 4: Configuring the Services
In general, to configure the services two different methods can be used: rule based
114
and learning user behavior. The rule based method is necessary because it may not be
possible to derive rules for new users or applications from user behavior. On the other
hand, learning user behavior by learning user preferences (in different contexts) from
history information is also necessary. It might be difficult to define a generic rule that
is applicable to every user. Therefore, learning the user behavior can be used to
update the predefined rules. We use both methods in our process.
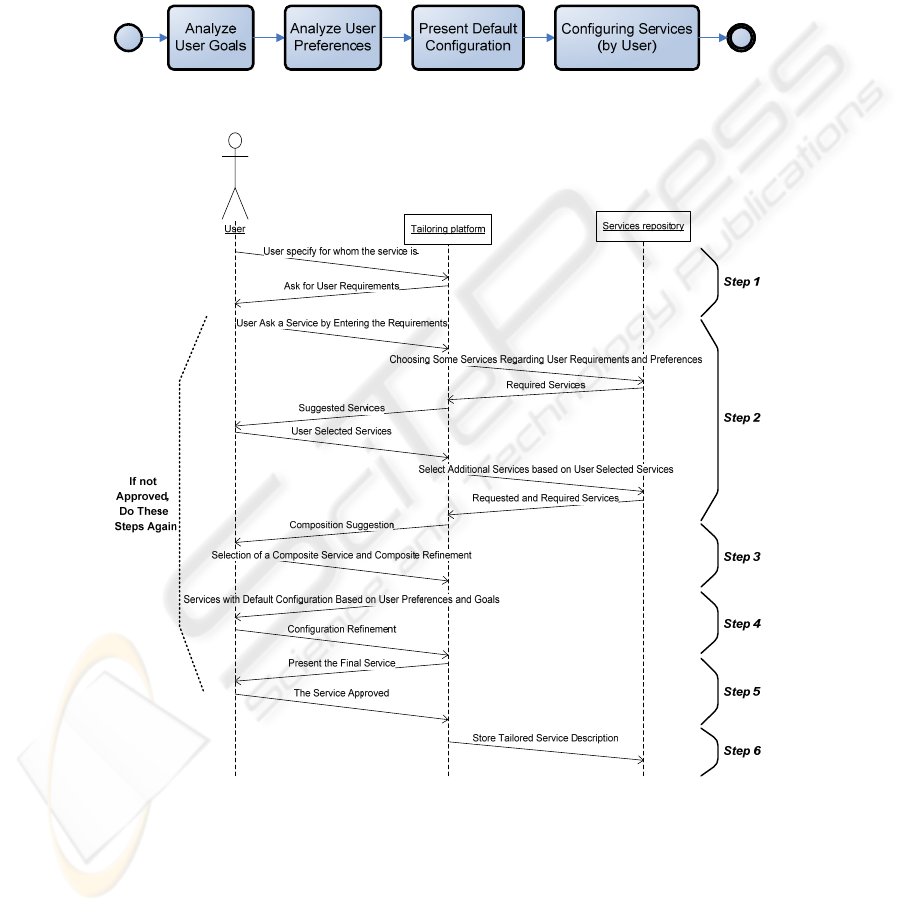
The fourth step includes four activities as shown in Figure 5:
Fig. 5. Step 4: Configuring the services.
Fig. 6. Sequence diagram of the service tailoring process.
The services selected in the previous step are presented to the user based on the
default configuration derived from user preferences as indicated in the service profile
and user goals. However, the user is also allowed to (re)configure the basic services
115
to specify his or her current preferences and needs. To configure the services, user can
use a configuration interface.
Step 5: Presenting the Final Service
In this step, the final newly created service will be presented to the user. After this
step, the user confirms whether the service meets his or her requirements. If the user
does not approve any of the suggested compositions, the process returns to Step 2.
Step 6: Storing the Service
Finally, once the user has approved the suggested service, the description of this
newly created service will be stored for later use. Also, user preferences in the user
profile may change because of configuration of the services by the user.
The sequence diagram shown in Figure 6 summarizes our discussion about the service
tailoring process. It shows the interaction between the ‘user’ and the ‘tailoring
platform’. Although the ‘Service repository’ is a part of tailoring platform, because of
its importance we presented it separately from the tailoring platform in Figure 6.
4 Tailoring Architecture
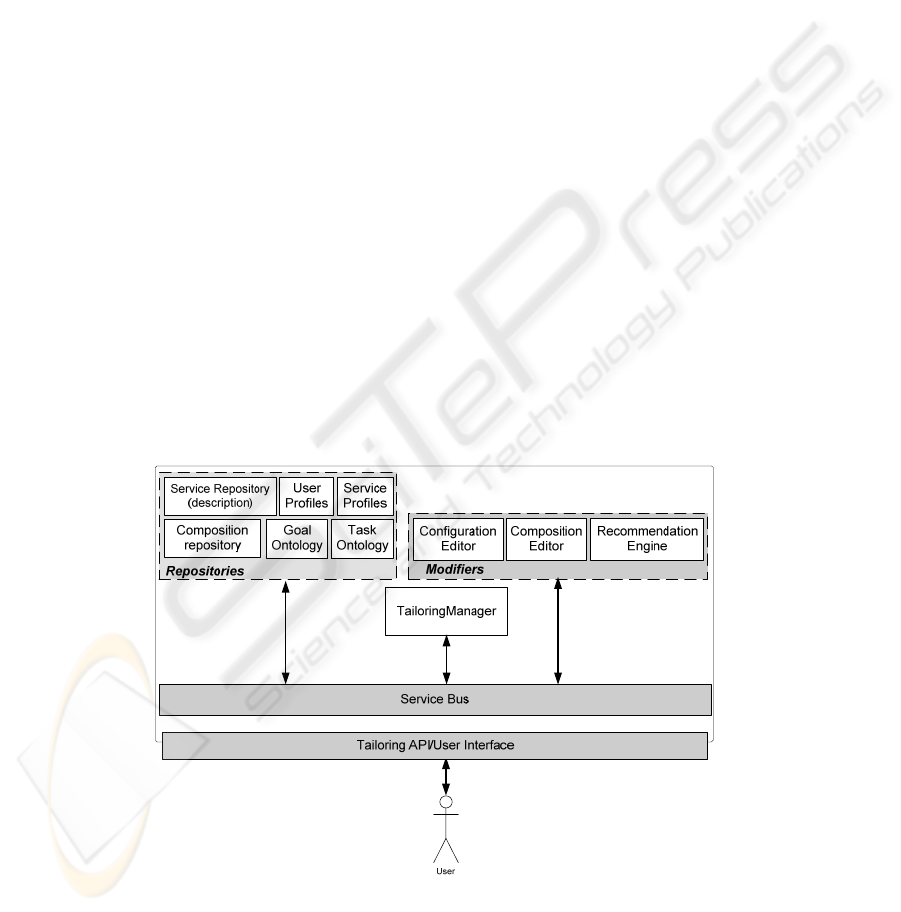
To support the tailoring process described in Section 3, we identify the required
components and propose a tailoring architecture for homecare services. The tailoring
architecture, as presented in Figure 7, has three categories of components:
TailoringManager, Repositories and Modifiers. These components and their
relationships are described separately in the remainder of this section.
Fig. 7. Service tailoring architecture.
116

- TailoringManager. This component is responsible for receiving and resolving
the user requests by utilizing goal and task ontology, suggesting existing services
to the user by utilizing service repository, making initial configuration of services
by utilizing user profile and service profiles, suggesting composition by utilizing
composition repository, and storing the final services in the service repository.
- Repositories:
• Service Repository. The service repository is a repository of existing
services which stores detailed information (for example, in the form of
WSDL) about several patient-neutral homecare services.
• User Profile. This component stores user information. It has two parts: static
part which keeps the static information of user such as name and gender, and
dynamic part which keeps the evolving information of the user such as user
specific requirements.
• Service Profile. This component stores the default configuration of the
services.
• Composition Repository. This is the repository of processes which keeps
different composition of services.
• Goal Ontology. The Goal ontology is used for helping users to specify their
desired goals.
• Task Ontology. The tasks are supported functionalities of existing services
which are defined in the Task ontology. In the Task ontology, each
functionality offered by of a service is associated to one or more tasks (e.g.,
reminding, alarming, etc.). The service developer defines these goals and
tasks ontology.
- Modifiers:
• Configuration Editor. This component supports the user (caregiver or
service developer) in defining and alerting the service configurations. These
configurations can be stored in the service profiles repository.
• Composition Editor. This component support user (caregiver or service
developer) to define processes. These processes are stored in the composition
repository.
• Recommendation Engine. This component recommends services to the
users (caregiver or service developer) in service selection and composition
steps. To do so, we assume all the instances of our homecare systems are
registered in a central server and they can make inquiry about the services
which are used by each of these instances anonymously. Assuming the
central server, enables all of these recommendation engines to maintain a list
of similar anonymous users and their utilized services, by exploiting the
information preserved in the user and service profiles.
5 Run through Example
In this section, we show the support provided by the proposed tailoring process and
architecture for meeting the requirements derived from the example scenario
117
presented in Section 2.
“Assume that Jan is prescribed to take certain medicines at certain times. Nancy, his
caregiver, wants to create a service to assist Jan in taking his medicine at right
times.”
We follow the service tailoring process step by step to see how Nancy creates the
desired service for Jan:
Step 1: Nancy, by choosing Jan’s profile, specifies through the tailoring interface that
a new service to be created is for Jan. By receiving this information, the tailoring
platform looks at Jan’s profile and finds his specific requirements and preferences, for
example, Jan has a hearing problem and will not be able to use any services or devices
which utilize sound as a means to convey messages to him.
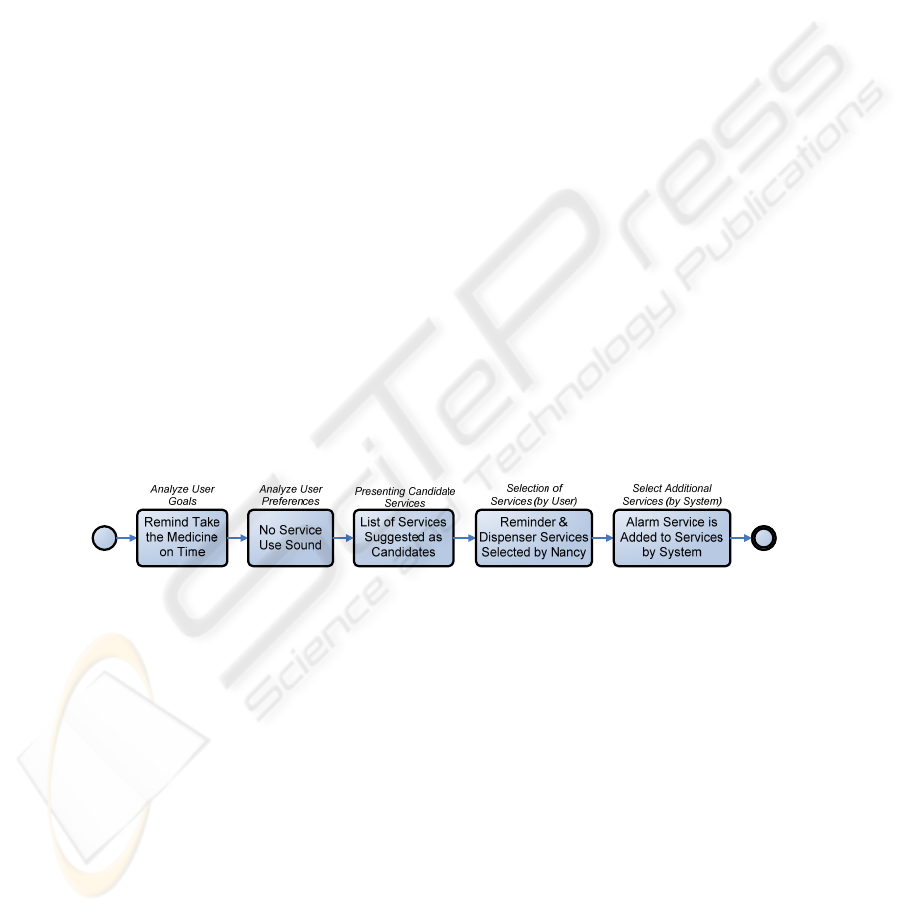
Step 2: As shown in Figure 8, Nancy sends a request to the tailoring platform for a
service which can help Jan to take his medicine at right times. For this purpose, she
chooses a goal among the ones listed by the system and presented in the screen. Next,
she chooses sub-goals to refine or finally define her goal. For example, from the goals
list, she chooses reminder, and then from the new sub-goals’ list she chooses
reminder for medicine. The tailoring platform, after receiving and analyzing this
request and considering the fact that Jan can not use sound related services, suggests a
list of services to Nancy. She chooses a reminder service which will send a reminder
to Jan such that he will not forget the prescribed time to take a medicine. Further, she
selects a dispenser service which will release right medicines such that Jan can take
the right amount of the right medicines. After selecting the reminder and dispenser
services by Nancy, the tailoring platform adds alarm service as an additional service
to the user selected services. As reminder and dispenser services are bundled with the
alarm service, which helps to detect hazard situations (in this case ignoring the
reminder and not taking the medicines) and to trigger a request for help.
Fig. 8. Step2: Selection of services for the example.
Step 3: As shown in Figure 9, the tailoring platform returns a set of possible
compositions, based on user goals and preferences. For example, because Jan prefers
to have reminder three times, the composition will change in such a way that the
reminder service sends the reminder three times. The tailoring platform proposes
different compositions such as P1 and P2, because all these compositions can satisfy
user’s requirements and preferences. This means that the composite service P1 first
sends a reminder message to Jan and then enables the dispenser to let him take the
medicine, whereas the composite service P2 first enables the dispenser and then sends
the reminder message to Jan. Then, Nancy chooses P2 as a one of the possible
compositions. After choosing P2, she may want to modify it, for example, because the
medicine is pain killer and ignoring of taking it by Jan is not a hazard situation, so
118

Nancy removes the alarm service from the P2.
Fig. 9. Step 3: Composing the services for the example.
Step 4: As shown in Figure 10, the tailoring platform returns three selected services
with default configuration to Nancy. These default configurations are done based on
the user goals and preferences. For example, Jan prefers a reminder to him be
repeated three times, allow 5 minutes for him to react, deliver this reminder as text
and deliver it on the TV. So the default configuration for the reminder will be to send
the output to the URI of TV and repeat each 5 minutes if the user does not respond.
Then Nancy adds other configurations, such as reminding Jan to take the medicines
from 10
th
May to 30
th
June 2010, everyday at 10 AM & 8 PM. She can also edit the
default configuration. She changes, for example, the repeating time of the reminder
from 5 to 10 minutes.
Fig. 10. Step 4: Configuration of services for the example.
Step 5 and 6: The tailoring platform presents the final tailored service to Nancy, and
if she approves it the description of the service will be stored. The default
configuration of the reminder service also will be changed, from 5 to 10 minutes
repetition time out. If Nancy does not approve the final service from any of suggested
compositions, the process returns to the Step 2 till Nancy approves the tailored
service.
6 Conclusions and Outlook
Since every care-receiver is unique, personalization is one of the main concerns of
homecare services. To achieve this, a service tailoring approach for homecare, with a
corresponding process and supporting architecture, is proposed. Our service tailoring
approach assumes the availability of basic care-related services which can be used as
building blocks in the tailoring process.
The service tailoring process defines the flow of actions involving the user of the
service tailoring platform to define a personalized homecare service for a
care- receiver. Although we show the feasibility of the proposed service tailoring
process, it is not claimed to be the only or most ideal solution for achieving service
tailoring. In this paper, we describe a process and architecture for achieving
personalized homecare services but further investigation is required to:
119

• Developing a ‘generic’ Service Tailoring Process. The service tailoring
process is 'generic' in the sense that it is independent of the knowledge and
skills of the user of the service tailoring platform. We foresee that the service
tailoring platform should offer different interfaces to optimally support
different types of users. Moreover, the service tailoring process should be
tested to identify whether the service tailoring process has the right
'genericity', and can be extended and specialized for different user types.
• Decreasing Privacy Risks of Recommendations. Our service tailoring
process may use recommendations from care-receivers. However, one of the
main drawbacks of recommendations is privacy risks. To protect the privacy
of care-receivers, distributed recommendation methods such as exploiting
peer-to-peer networks would be interesting as our future work [22].
Acknowledgements
This work is part of the IOP GenCom U-Care project (http://ucare.ewi.utwente.nl)
which is sponsored by the Dutch Ministry of Economic Affairs under contract
IGC0816.
References
1. Fujii, K. and T. Suda, Semantics-based context-aware dynamic service composition. ACM
Trans. Autonom. Adapt. Syst., 2009. 4(2): 1-31.
2. Di Nitto, E., et al., A journey to highly dynamic, self-adaptive service-based applications.
Automated Software Engineering, 2008. 15(3-4): 313-341.
3. Gehlert, A., et al., Towards Goal-Driven Self Optimisation of Service Based Applications,
in 1st European Conf. on Towards a Service-Based Internet. 2008, Springer-Verlag. pp. 13-
24.
4. Hielscher, J., et al., A Framework for Proactive Self-adaptation of Service-Based
Applications Based on Online Testing, in 1st European Conf. on Towards a Service-Based
Internet. 2008, Springer-Verlag. pp. 122-133.
5. Choi, O. and S. Han, Personalization of Rule-based Web Services. Sensors, 2008. 8(4):
2424-2435.
6. Kumanayaka, O. and N. Ranasinghe, Ontology based Web Service Personalization, in Intl.
Conf. on Information and Automation, ICIA. . 2006. pp. 69-74.
7. Kazhamiakin, R., et al., Having Services "YourWay!": Towards User-Centric Composition
of Mobile Services, in First Future Internet Symp., FIS. 2009, Springer-Verlag. pp. 94-106.
8. Zarifi Eslami, M. and M. Van Sinderen. Flexible home care automation: adapting to the
personal and evolving needs and situations of the patient. in 3rd Intl. Conf. on Pervasive
Computing Technologies for Healthcare, PervasiveHealth. . 2009. London, UK. pp. 1-2.
9. Korhonen, I., J. Parkka, and M. Van Gils, Health monitoring in the home of the future.
Engineering in Medicine and Biology Magazine, IEEE, 2003. 22(3): 66-73.
10. White, C.C., et al. Improving Healthcare Quality through Distributed Diagnosis and Home
Healthcare. in 1st Transdisciplinary Conf. on Distributed Diagnosis and Home Healthcare,
D2H2. . 2006. pp. 168-172.
120

11. Kim, Y.-J., et al., Hallym Jikimi 3rd system: web-based monitoring for u-health care
service, in 4th Intl. Conf. on Persuasive Technology. 2009, ACM. pp. 1-5.
12. Berners-Lee, T., Semantic Web Roadmap. 1998. Available at:
http://www.w3.org/DesignIssues/Semantic.html.
13. Papazoglou, M.P. and D. Georgakopoulos, Introduction. Communications of the ACM,
Special section: Service-oriented computing 2003. 46(10): 24-28.
14. Kangkang, Z., L. Qingzhong, and S. Qi. A Goal-driven Approach of Service Composition
for Pervasive Computing. in 1st Intl. Symp. on Pervasive Computing and Applications.
2006. pp. 593-598.
15. da Silva Santos, L.O.B., et al. Towards a Goal-Based Service Framework for Dynamic
Service Discovery and Composition. in Information Technology: Sixth Intl. Conf. on New
Generations ITNG '09. 2009. pp. 302-307.
16. Manikrao, U.S. and T.V. Prabhakar, Dynamic Selection of Web Services with
Recommendation System, in Intl. Conf. on Next Generation Web Services Practices. 2005,
IEEE Computer Society. 5 pp.
17. Gordijn, J., S. de Kinderen, and R. Wieringa. Value-driven Service Matching. in 16th IEEE
Intl.Conf. on Requirements Engineering, RE '08.. 2008. pp. 67-70.
18. Jun, H., et al., Personalized Active Service Spaces for End-User Service Composition, in
IEEE Intl. Conf. on Services Computing, SCC '06. 2006. pp. 198-205.
19. Wang, F. and K.J. Turner, Towards personalised home care systems, in 1st intl. conf. on
Pervasive Technologies Related to Assistive Environments. 2008, ACM. pp. 1-7.
20. Xuanzhe, L., et al., Towards Service Composition Based on Mashup, in IEEE Congress on
Services. 2007. pp. 332-339.
21. Nan, Z. and M.B. Rosson, What's in a mashup? And why? Studying the perceptions of
web-active end users, in IEEE Symp. on Visual Languages and Human-Centric Computing,
VL/HCC 2008. pp. 31-38.
22. Schafer, J.B., et al., Collaborative filtering recommender systems, in The adaptive web:
methods and strategies of web personalization. 2007, Springer-Verlag. pp. 291-324.
121
