
CONTEXT-AWARE SECURITY IN CLOUD
EMERGENCY MEDICAL SERVICES
Vassiliki Koufi, Flora Malamateniou and George Vassilacopoulos
Department of Digital Systems, University of Piraeus, 80 Karaoli & Dimitriou Str., 18534 Piraeus, Greece
Keywords: Emergency care, Personal Health Records, Cloud Computing, Web Services, Context-aware Security.
Abstract: Recently, there has been a remarkable upsurge in activity surrounding the adoption of Personal Health
Records (PHRs). Since PHRs contain global patient information and not certain pieces collected by
individual healthcare providers, they can be used as basic infrastructures for building and operating several
important systems for both healthcare and the tax payers. Emergency medical systems (EMS) are among the
most crucial ones as they involve a variety of activities which are performed from the time of a call to an
ambulance service till the time of patient’s discharge from the emergency department of a hospital and are
closely interrelated so that collaboration and coordination becomes a vital issue for patients and for
emergency healthcare service performance. This paper is concerned with the development of a PHR-based
EMS in a cloud computing environment and focuses on the security aspect of delivering this particular
service. Although cloud-based services can prove important in healthcare delivery, the inherent nature of
medical service delivery underscores the need for ensuring that data security is better maintained. Moreover,
high expectations for emergency care delivery can be achieved only if provider organizations select systems
with the appropriate features, security being among the most prominent ones. Thus, the proposed EMS
system comes with a suitable security mechanism in order to ensure secure access to medical information
when and where needed. To this end, context-aware authorization has been embedded into the emergency
care process, enabling authorization to be based not only on static rules and roles but also to be influenced
by the process execution context to ensure precise and tight access control.
1 INTRODUCTION
Recent years have seen a remarkable upsurge in
activity surrounding the adoption of Personal Health
Records (PHR) to enable access to integrated
medical information that may entail to increased
patient satisfaction and continuity of care (Tang,
Ash, et.al., 2006; Wiljer, Urowitz, et.al., 2008). A
PHR is a consumer-centric approach to making
available comprehensive healthcare information
about a patient at the point of care while fully
protecting patient privacy (Lauer, 2009; Win, Susilo,
et.al., 2006). Unlike traditional electronic healthcare
records (EHRs) that are based on the “fetch and
show” model, PHR architectures are based on the
fundamental assumptions that the complete records
are held on a central repository (e.g. a data center)
and that each patient retains authority over access to
any portion of his/her record (Lauer, 2009; Wiljer,
Urowitz, et.al., 2008).
Although patients are the primary beneficiaries and
users of PHRs, healthcare providers may benefit
from their use as well as they have both economic
and quality impact (U.S. Department of Health and
Human Services, 2006; Shimrat, 2009; Van der Burg
and Dolstra, 2009). In particular, since patients may
receive care by various healthcare providers and
under various circumstances, there is a need for
ubiquitous, context-aware access to relevant and
timely patient information (Tentori, Favela, et.al.,
2006). Moreover, several healthcare applications can
be built around the PHR concept based on the
integration of leading-edge networking technologies,
such as cloud-based services and mobile
communications, to meet healthcare needs by
enabling easy and immediate access to patient data
from anywhere and via almost any device. Thus,
healthcare providers and organizations are
increasingly considering migrating to cloud
computing in an attempt to increase flexibility and
agility of their healthcare systems and services and
121
Koufi V., Malamateniou F. and Vassilacopoulos G..
CONTEXT-AWARE SECURITY IN CLOUD EMERGENCY MEDICAL SERVICES.
DOI: 10.5220/0003106001210130
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2011), pages 121-130
ISBN: 978-989-8425-34-8
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

enhance quality of patient care (Shimrat, 2009; Van
der Burg and Dolstra, 2009).
Cloud computing may be able to provide a
solution to the need for sharing geographically
dispersed healthcare information. Cloud computing
concepts may assist in accomplishing some of the
goals that have been articulated by government
healthcare IT policy committees. Example goals
include the development of software that improves
interoperability and connectivity among health
information systems; infrastructure and tools for
telemedicine; the promotion of interoperability of
clinical data repositories; the development of self-
service technologies that facilitate the use and
exchange of patient information and reduce waiting
times; technologies that facilitate home healthcare
and patient monitoring; technologies that facilitate
the continuity of care among healthcare settings; and
technologies for developing mission critical
applications for healthcare delivery in all levels of
care (Rosenthal, Mork, et.al, 2010; Van der Burg
and Dolstra, 2009). This paper is concerned with the
development of emergency medical service (EMS)
systems and focuses on the security of medical
information stored and exchanged in dealing with
emergency cases.
Emergency medical services are concerned with
the provision of pre-hospital and in-hospital
emergency care and their operations typically
involve a wide range of interdependent and
distributed activities, performed by cooperating
individuals (administrative, paramedical, nursing
and medical) who differ on levels of background,
skill, knowledge and status. Conceptually, these
activities can be interconnected to form emergency
healthcare processes within and between the
participating organizations (i.e. ambulance services
and hospitals), thus comprising a virtual emergency
healthcare enterprise within the area covered by each
ambulance service. Thus, in developing an
information system that supports EMS processes, it
is essential to place particular emphasis on
supporting individual process activities as well as on
the collaboration and coordination needs among
them.
The development of an EMS system as a cloud
computing application which interfaces with a PHR
enables immediate access to critical medical
information concerning an emergency case either by
authorized ambulance center personnel on site of
incident and during patient transfer to a hospital or
by emergency department personnel allowing them
to check patient medical histories, patient
medication history, patient allergies and much more
to ensure that the treatment provided is the safest
and most effective choice for the patient (Buyya,
Yeoa, et.al., 2009).
Service-oriented architectures (SOA) can make
system-to-system interfaces consistent in the
enterprise architecture, thus saving resources on
future integration and hopefully improving the speed
at which integration can occur. The emphasis of
cloud computing is to leverage the network to
outsource IT functions across the entire stack. While
this can include software services as in an SOA, it
goes much further. Cloud computing allows the
marketplace to offer many IT functions as
commodities, thus lowering the cost to consumers
when compared to operating them internally. On
these grounds, cloud computing platform and
storage service offerings can provide a value-added
underpinning for SOA efforts. (Raines, 2009)
Hence, combining cloud computing with SOA
presents a new way for service-oriented integration
(SOI) of existing healthcare systems and for
developing distributed applications within and
between healthcare organizations. On these grounds,
ambulance services and hospital emergency
departments can integrate and automate their
operations by making information available where
and when needed and by providing an infrastructure
for the integration of pre-hospital and in-hospital
emergency medical care.
One important consideration in developing an
EMS system as a cloud application is security
(Bruening and Treacy, 2009; U.S. Department of
Health and Human Services, 2004). In addition to
the usual challenges of developing secure systems,
cloud computing presents an added level of risk
because essential services are externalized. Thus,
data security and confidentiality needs to be
examined and methods developed to minimize risks
and maintain privacy. For example, patients need
assurances that emergency care data will not be used
to harm them through disclosure to a prospective
employer. Thus, there is need for adhering to
appropriate privacy and security rules to provide the
necessary protections and, to this end, audit trails
and role-based access controls are strongly
recommended (Bruening and Treacy, 2009).
This paper focuses on a role-based, context-
aware authorization mechanism that is incorporated
into a prototype EMS application developed as a
cloud service which interacts with a cloud-based
PHR and is provided to authorized users on demand.
In particular, the EMS application has been
implemented in the framework of NefeliPortal, a
prototype medical portal which provides a web
HEALTHINF 2011 - International Conference on Health Informatics
122

interface to healthcare applications that are
implemented in a SOA architecture over a cloud
computing infrastructure. The proposed access
control mechanism incorporates the advantages of
role-based access control (RBAC) and yet provides
the flexibility for adjusting role permissions on web
service invocations and web service method
executions according to context (OASIS Standards,
n.d.). Thus, at run time contextual information is
collected to adapt user permissions to the minimum
required for completing a job.
2 CLOUD-BASED HEALTHCARE
SERVICES
Cloud computing is an on-demand service model for
IT provision, often based on virtualization and
distributed computing technologies (IBM
Corporation, 2009). It may be divided into software
as a service (SaaS), which allows software offered
by a third party provider to be available on demand,
usually via the Internet, platform as a service (PaaS),
which allows customers to develop new applications
using APIs deployed and configurable remotely, and
infrastructure as service (IaaS), which provides
virtual machines and other abstracted hardware and
operating systems which may be controlled through
a service API (Shimrat, 2009; van der Burg and
Dolstra, 2009). Clouds may also be divided into
public, which are available publicly (i.e. any
organization may subscribe), private, which are
services built according to cloud computing
principles, but accessible only within a private
network, and partner, which are cloud services
offered by a provider to a limited and well-defined
number of parties.
Cloud computing provides a new information
delivery and consumption model in which
applications and information are accessed from a
web browser while software and data are stored on
servers (IBM Corporation, 2009). Cloud components
communicate with one another over application
programming interfaces, which are usually web
services. Service computing focuses on the linkage
between business processes and IT services so that
business processes can be seamlessly automated
using IT services. Examples of services computing
technologies include SOA and web services. SOA
facilitates interoperable services between distributed
systems in order to communicate and exchange data
with one another while web services provide the
capability for self-contained business functions to
operate over the Internet (Communications of the
ACM, 2003).
In addition, cloud computing may be assumed a
disruptive technology that has the potential to affect
not only Internet services but also IT as a whole
since it enables organizations to increase hardware
utilization rates dramatically and scale up to massive
capacities in an instant — without having to invest
in new infrastructure, train new personnel or license
new software. It also creates opportunities to build a
better breed of network services in less time and for
less money (Buyya, Yeoa, et.al., 2009; IBM
Corporation, 2009). Cloud computing may be seen
as an extension of the paradigm wherein the
capabilities of business applications are exposed as
sophisticated services that can be accessed over a
network. Cloud service providers are incentivized by
the profits to be made by charging consumers for
accessing these services. Consumers, such as
healthcare enterprises, are attracted by the
opportunity for reducing or eliminating costs
associated with “in-house” provision of these
services. However, since cloud applications may be
crucial to the core business operations of the
consumers, it is essential that the consumers have
guarantees from providers on service delivery,
including the appropriate levels of security
(Bruening and Treacy, 2009; Muttig and Burton,
2009).
There is considerable excitement over the
potential benefits of operating in a cloud computing
environment. In fact, several reports highlight the
potential benefits of cloud computing for health –
and leading the way by using it to develop new
healthcare services – but they also identify at least
one major stumbling block. For example, the report
by the European Network and Information Security
Agency says that although health agencies can see
the benefits of cloud computing in terms of
increased flexibility and lower cost, they are
concerned about security (Bruening and Treacy,
2009; Muttig and Burton, 2009). It also uses the
analysis of an actual ehealth application that uses the
cloud to identify real issues about who is responsible
for infrastructure faults and information governance.
The agency suggests that there is a need to clarify
the obligations of cloud providers to report faults
and security breaches to customers and in setting
minimum data protection standards.
Healthcare delivery, consumption, cost and
quality as well as healthcare IT in general can
benefit from this new approach to computing.
Interoperability, open standards and open-source
software are critical to the growth of cloud
CONTEXT-AWARE SECURITY IN CLOUD EMERGENCY MEDICAL SERVICES
123

computing (Buyya, Yeoa, et.al., 2009). Sharing
patient data across the multiple institutions from
which patients receive healthcare services is a
problem for which no good solution currently exists.
Multisite institutions with business relationships
may invest in network connections and virtual
private networks to perform electronic data transfers.
However, such an approach is problematic and
costly and adversely affects the quality of care. In a
cloud computing environment, medical data could
be stored in a virtual generic archive and accessed
by healthcare providers as needed through the cloud.
This could facilitate the sharing of medical data and
significantly reduce local storage requirements. In
this context data security and confidentiality will
need to be examined and methods developed to
minimize risks and maintain privacy (Bruening and
Treacy, 2009).
Potential developments in the healthcare field
include health IT architectures supporting electronic
exchange or perhaps facilitate regional health
information organizations or even just multiple
healthcare systems wanting to share data (Lauer,
2009). The current implementations of regional
healthcare information organizations are not
practical for adoption as a standard approach, but
cloud computing may be able to provide a solution
to healthcare information sharing without
geographical boundaries (Lauer, 2009). A cloud
could be built to provide a way to input, store and
access medical information without the need to build
complex infrastructures to support outside medical
record numbers or patient identifiers, dictionaries
and user accounts, different databases and archive
protocols, and so on.
A scenario in which patients and healthcare
providers plug into front-end web services to input
all of patient’s information, including medications,
allergies, laboratory results, medical images and so
on, from wherever that patient has received medical
care might be envisioned for healthcare
environments of the future by evolving toward the
cloud (Shimrat, 2009; Van der Burg and Dolstra,
2009). Moreover, a cloud infrastructure provides the
ability of any authorized user to access web services
on demand in order to retrieve patient information at
the point of care as if all the information was stored
in one system. One realization of this scenario
constitutes the implementation of an EMS system
(Anantharaman and Han, 2001).
Emergency healthcare delivery involves a variety
of activities (administrative, paramedical and
medical) that are performed from the time of a call
for an ambulance to the time of patient’s disposal
from the emergency department of a hospital
(Reddy, Paul, et.al. 2009). As these activities are
performed in at least two organizations (i.e.
ambulance service and hospital) and they are
interrelated to form inter-organizational healthcare
processes, collaboration and coordination become a
vital issue for patients and for EMS performance.
Such activities may involve basic life support (BLS)
and advanced life support (ALS). For example, in
the case of a cardiac patient BLS emphasizes prompt
recognition of the case, treatment with oxygen and
rotating tourniquets for patients in pulmonary
edema. On the other hand, ALS adds skills in
electrocardiogram (ECG) arrhythmia pattern
recognition, antiarhythmic drug and/or defibrillation
treatments, intravenous therapy and airway
management with entrotracheal and/or esophageal
treatment. ALS activities impose increased support
requirements on an EMS: triage at the point of
dispatch (i.e. assessing patient’s condition), on-line
medical control, ECG transmission to a hospital base
for medical control and broadband wireless
communications.
Conceptually, EMS activities can be
interconnected to form EMS processes within and
between the participating organizations (i.e.
ambulance services and hospitals), thus comprising a
virtual healthcare enterprise. Hence, it is important
to define and automate EMS processes that span
organizational boundaries so that to create and
empower collaboration and coordination among the
participating organizations. Standard workflow
technology such as Business Process Execution
Language (BPEL) and SOA provide an appropriate
technological infrastructure for this purpose. They
enable easy integration of possibly heterogeneous
existing applications of the participating
organizations by orchestrating web services through
the use of BPEL (OASIS, 2007). Hence, cloud
applications that are based on a number of BPEL-
orchestrated web services present a new way for
service-oriented integration (SOI) of existing
systems and for developing distributed applications
within and between healthcare organizations. Thus,
through process automation and the use of web
services in the context of a cloud application,
ambulance service and hospital emergency
departments can automate their operations by
making information available where and when
needed and by providing an infrastructure for the
integration of pre-hospital and in-hospital
emergency healthcare. A prototype implementation
of this approach is considered in this paper.
HEALTHINF 2011 - International Conference on Health Informatics
124

The benefits accrued from the implementation of
an EMS system are manifold: For example, the
system puts eligibility, insurances and medical
information at the physician’s and other healthcare
professional’s fingertips when and where needed.
This enables healthcare professionals to exert best
practice approaches in emergency care delivery
provided by the insurance scheme (Reddy, Paul,
et.al. 2009). It also informs physicians of lower cost
alternatives. In addition, physicians can access a
timely and clinically sound view of a patient’s
medical history at the point of care, decreasing the
risk of preventable medical errors (Anantharaman
and Han, 1998; Reddy, Paul, et.al. 2009). Also, in
some circumstances medical instruction routing
from ambulance service physicians to ambulance
paramedics electronically during patient transfer
reduces the risk of medical errors associated with
uninformed ordering.
One aspect of the EMS service that needs
particular attention concerns home care, where
physicians may need to provide medical care during
home visits and cases where physicians may need to
provide pharmaceutical treatment during patient
transfer to a hospital by an ambulance (en-route
treatment). In such cases, there is a need to ensure
that medical information regarding the case (e.g.
health problems, allergies, medication history) is
automatically made available to the physician before
prescribing and/or administering the medications
needed. Thus, care inefficiencies are eliminated
resulting in enhanced quality of care and cost
containment (Bates, Leape, et.al. 1998).
3 MOTIVATING SCENARIO
The basic motivation for this research stems from
our involvement in a recent project concerned with
developing a prototype EMS system for the needs of
the Greek National Health Service with the objective
to improve quality of care while containing cost. To
illustrate the main principles of the security
architecture incorporated into the NefeliEMS,
consider an EMS process scenario that shows an
example of how an EMS may work. Figure 1 shows
a broad view of the EMS process.
In the EMS process of Figure 1, where the
ambulance service and a hospital emergency
department are involved, five user roles are
identified: ambulance communication operators,
ambulance service physician, ambulance
paramedics, emergency department physician and
emergency department nurse.
Ambulance communication operators -
Ambulance communication operators are located in
the ambulance center premises and use an EMS
application to write into a PHR system emergency
case data which is provided by either the patient or
another person and to pass this data to ambulance
personnel.
Ambulance service physician - Ambulance
service physicians are usually located in the
ambulance center premises and use an EMS
application to read from and write into a PHR
system relevant medical data of their current patients
(e.g. medical history, patient allergies and other
critical health factors) so that to give appropriate
medical instructions to ambulance paramedics,
regarding en route treatment, that are also recorded.
Ambulance paramedics - Ambulance paramedics
use an EMS application, via a smart handheld
device, to read authorized portions of medical data
from a PHR system and write data regarding the
paramedic activities performed on the patient at the
site of incident and en route.
Emergency department physician - Emergency
department physicians use an EMS application to
read from and write into a PHR system relevant
medical data of their current patients (e.g. medical
history, patient allergies and other critical health
factors).
Emergency department nurse - Emergency
department nurses use an EMS application to read
authorized portions of patient data from a PHR
system, to write a nursing assessment of patient’s
condition (triage) and to write data of the nursing
activities performed on the patient.
From a role-based authorization perspective in a
process-oriented environment, the business process
of Figure 1 surfaces several requirements with
regard to task execution and associated data
accesses. These requirements include the following:
Task Execution - Task execution specified by
a role-to-task permission assignment may be
further restricted dynamically during EMS
process execution and be a subset of the
authorized role holders. For example, medical
instructions to ambulance personnel may only
be provided by physicians who are currently at
the ambulance service premises and are
assigned to deal with the particular case (having
access to the “Provide & Write Medical
Instruction” task).
Data Access - Some role holders are allowed to
exercise a set of permissions on certain data
objects only and/or for a limited duration. For
CONTEXT-AWARE SECURITY IN CLOUD EMERGENCY MEDICAL SERVICES
125
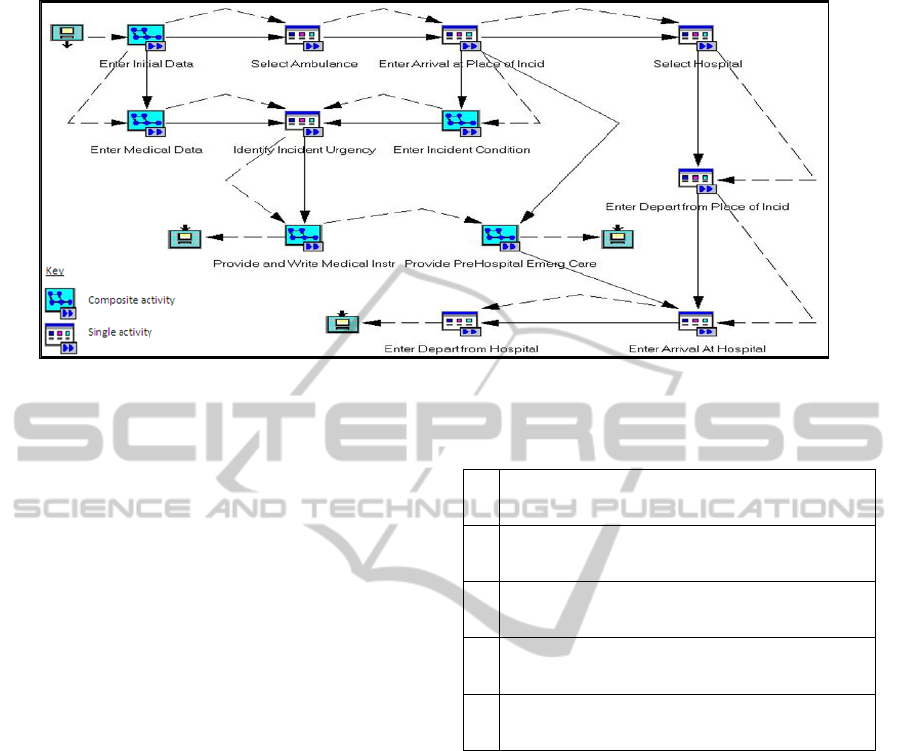
Figure 1: A high level model of an emergency care process.
example, during the execution of the “Provide
& Write Medical Instruction” task, a physician
may be allowed to read patient records only
for his/her patients and the permission to read
patient records may be revoked upon
successful task execution.
Table 1 shows an extract of authorization
requirements regarding task execution and related
data access privileges assigned to the roles of
“ambulance communication operators”, “ambulance
service physicians” and “ambulance service
paramedics”, “emergency department physicians”
and “emergency department nurses”, respectively.
These requirements suggest that certain task
execution and associated data access permissions of
the EMS process participants depend on the EMS
process execution context. In particular, contextual
information available during process execution, like
user/patient relationship, location or time, can
influence the authorization decision that allows a
user to perform a task and access associated data
objects. This enables a more flexible and precise
authorization policy specification that incorporates
the advantages of having broad, role-based
permissions across process tasks and object classes,
like RBAC, yet enhanced with the ability to
simultaneously support the above requirements.
Given a cloud PHR architecture, where relevant
medical data are accessed via web services, the
above authorization requirements of the EMS
process can be translated into authorization
requirements with regard to web service invocations
and associated method executions as follows:
Web Service Invocation: Web service
invocations for EMS and PHR access may be
Table 1: Extract of authorization requirements for the
emergency process.
1
Ambulance communication operators may write current
patient data into relevant portions of PHRs from within
ambulance center premises only.
2
Ambulance service physicians may read and write
relevant portions of PHRs of their current patients and
from within ambulance center premises only.
3
Ambulance service paramedics may read and write
relevant portions of PHRs of their current patients and
from within ambulances only.
4
Emergency department physicians may read and write
relevant portions of PHRs of their current patients and
from within hospital premises only.
5
Emergency department nurses may read and write
relevant portions of PHRs of their current patients and
from within hospital premises only.
specified by a role-to-web service permission
assignment.
Method Execution: Given an authorization for
invoking a web service, role holders can
execute a dynamically determined set of web
service methods subject to contextual
constraints (e.g. user/patient proximity, time
and location of method execution).
Thus, permission is defined as the authority to
invoke a specific web service and/or to execute a
web service method on a class of objects. A role is
then defined as a collection of such permissions. A
user may be granted membership of a role, but the
role membership is only valid within a certain
context that limits the applicability of the role's
permissions to a subset of the process instances. The
advantage of this approach is that the role context
can be specified by the system administrator at the
time of role creation and remains valid unless the
role definition itself changes.
HEALTHINF 2011 - International Conference on Health Informatics
126

4 SYSTEM ARCHITECTURE
The EMS system comprises a number of
BPEL-orchestrated web services that are called
either by the ambulance service personnel or by the
physicians and nurses of a hospital emergency
department. The whole process starts when the
telephone operator of the ambulance service receives
an emergency call and records the case’s
demographic and medical data. If a physician of
either the ambulance service or the emergency
department of a hospital requests past medical data
of the current patient, the appropriate web service is
invoked. This takes as input the doctor’s role and the
patient’s code or name and searches the patient’s
PHR to retrieve authorized portions of medical data.
Case data collected by the ambulance service
personnel and by the personnel of the emergency
department of a hospital form two separate XML
documents that are recorded into the cloud storage.
These XML documents are formed automatically
upon recording ambulance arrival at the emergency
department of a hospital and when the patient is
discharged from the emergency department,
respectively.
Figure 2: System Architecture.
Figure 2 shows a high-level architectural view of
the prototype NefeliPortal cloud computing
environment. In essence, this architecture refers to
both the PHR system and the EMS application
delivered as services over the Internet and the
hardware and systems software in the data centres
that provide those services. Thus, central to the
cloud architecture is the PHR component which is
accompanied by a number of peripheral applications
such as the EMS system component. These
applications are licensed for use as services and are
provided to authorized users on demand. The
application software of both the PHR and the EMS
component consists of a number of web services
which are deployed and orchestrated using BPEL.
Authorized users interact with NefeliPortal through
either a desktop workstation or a mobile device such
as a Personal Digital Assistant (PDA) that run an
HTTP(S)-based client.
In our implementation, process models were
used for the definition of web services and web
services were used for process activity
implementations. Specifically, there exists a web
service of the mechanism for retrieving past medical
data of a patient by authorized users. This web
service is used by the ambulance service and the
emergency department of a hospital on demand as a
BPEL activity implementation. The system
architecture is illustrated on Figure 3.
In broad terms, the architecture of the prototype
NefeliPortal cloud computing environment consists
of the following main components:
PHR Application: PHR architectures are based
on the fundamental assumptions that the
complete patient records are centrally stored
and that each patient retains authority over
access to any portion of his/her record. Hence,
the PHR platform consists of a data repository
which stores patient data and a user interface
which allows patients to access their own
information and authorized healthcare
professionals to access appropriate parts of
patient information.
EMS Application: The EMS application
consists of a data repository which stores
emergency medical data and the application
software comprised by a number of BPEL-
orchestrated web services that are accessed by
authorized personnel of the ambulance service
and the emergency department. Users which are
authorized to use the EMS system for some
patients are also authorized to access certain
portions of the PHR of these patients.
Portal: The portal component provides a web-
based front end to PHR and EMS processes.
Authorized users enter the portal to interact
with either the PHR or the EMS system. The
portal is flexibly sized so that to fit in PDA or
mobile phone screen, which is particularly
useful in cases where there is a need for remote
SAAS
NefeliEMS
Security Services
Business Processes
Web Services
Platform as a Service
PAAS
BPEL Engine
PHR Platform
Web/Application Server
Web Portal Container
Infrastructure as a Service
IAAS
Servers
Networking
Data Server Fabric
Storage
Software as a Service
CONTEXT-AWARE SECURITY IN CLOUD EMERGENCY MEDICAL SERVICES
127
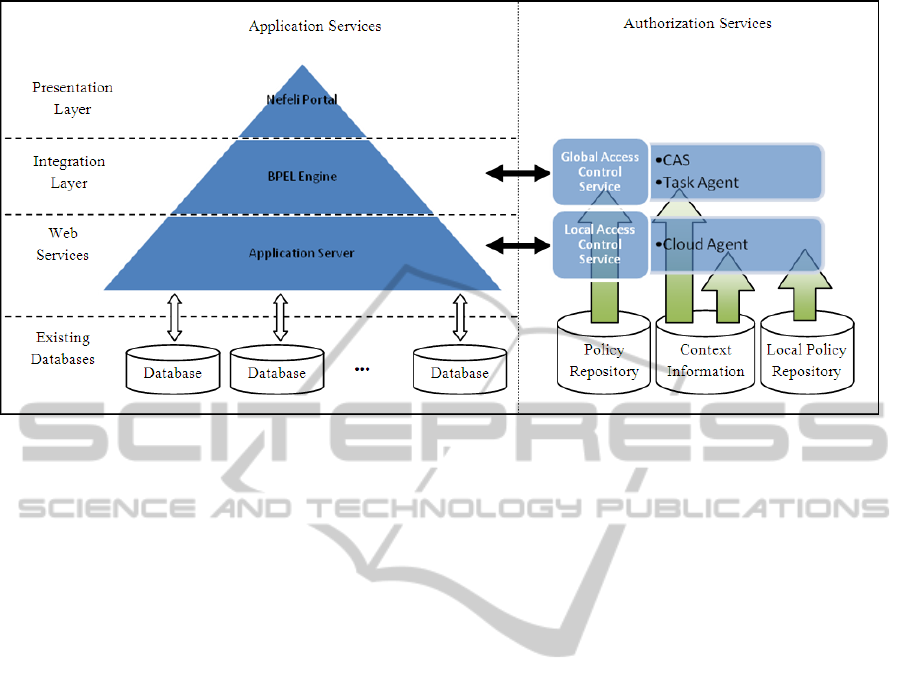
Figure 3: Security Architecture of NefeliEMS Service.
access to these applications (e.g. in emergency
cases where the patient’s PHR is accessed
through a wireless network either from the
place of incident or from the ambulance en
route).
5 AUTHORIZATION
ARCHITECTURE
A significant issue in cloud computing is the lack of
delegated authorization. While some cloud services
provide for delegated strong authentication that
enables access control based on user identity, few, if
any, provide delegated authorization to enable
access control based on contextual information and
user roles. This capability is turning out to be
increasingly important as fine-grained entitlements
for authorization management and control will be
most essential. Hence, more granular authorization
is needed. Authorization can be coarse-grained
within an enterprise or even a private cloud, but in
order to handle sensitive (such as medical) data and
compliance requirements, public clouds will need
granular authorization capabilities (such as role-
based access controls and IRM) that can be
persistent throughout the cloud infrastructure and the
data’s lifecycle (Bruening and Traecy, 2009; IBM
Corporation 2009).
As the number of partners and shared resources
increase, one will face extra labour to manage
permissions. There is also extra risk of inappropriate
data release, due to having more users who may
misunderstand policy or be careless or malicious.
Hence, a security system must be implemented that
reduces the possibility of breaching patient privacy
under any circumstances. To this end, one important
issue is to define and enforce authorization
constraints that are both effective and efficient.
Figure 3 shows a high-level view of the
authorization architecture implemented into
NefeliPortal. The access control mechanism uses
collected contextual information to mediate between
subjects (healthcare professionals) and objects (web
services and associated tasks) to decide whether
execution of an object by a given subject should be
permitted or denied. The access control mechanism
is certificate-based as it relies on Community
Authorization Service (CAS) certificates issued to
healthcare professionals by a CAS server. These
certificates specify user-to-role assignments in the
form of security assertions, expressed in Security
Assertion Markup Language (SAML) (Pearlman,
Welch, et.al., 2002). The role-to-permission (role-to-
web service invocation and role-to-task execution)
mapping is performed by means of access control
policies expressed by using the RBAC profile of
eXtensible Access Control Markup Language
(XACML) (OASIS Standards, n.d).
In the NefeliPortal prototype, the contextual
information is determined by a pre-defined set of
attributes related to the user (e.g. user certificate,
user/patient relationship), to the environment (e.g.
location and time of attempted access) and to the
client or healthcare organization (e.g. local security
policy). Contextual information is collected by a
Context Manager which consists of two kinds of
HEALTHINF 2011 - International Conference on Health Informatics
128

agents developed in JADE (Java Agent
Development Framework, n.d.):
Cloud Agent: Hosted on a cloud server and
manages user permissions on web services.
Task Agent: Hosted on a cloud server and
manages user permissions on web service
methods.
Each agent uses context collection services to
monitor context and interacts with a state machine
that maintains the permission subset of each role.
The state machine consists of variables that encode
state (permissions assigned to each role) and events
that transform its state. Upon an attempted access
(either to a web service or to an associated task), the
relevant agent generates an event to trigger a
transition of the state machine. Changes in user and
environmental context are sensed by both agents,
whereas changes in client context are sensed and
dealt with by the cloud agent of each client node.
6 IMPLEMENTATION ISSUES
The prototype implementation of the EMS system
and its authorization architecture has been developed
on a laboratory cloud computing infrastructure. The
system has been developed as a web application
using the Apache/Tomcat as Web/Application
Server. The platform used for the generation of
sample patient PHRs is Care2X Integrated
Healthcare Environment (Care2X Integrated
Healthcare Environment, n.d.). Although Care2X is
not a PHR platform but an open source Web based
hospital information system, it has been considered
sufficient for the purpose of our research. In order to
enable access to data stored in Care2X repository a
number of web services have been implemented
which make use of the Care2X Application
Programming Interface (API). The BPEL engine
used for the execution of BPEL healthcare processes
is ActiveBPEL, an open source BPEL Engine
(Active Endpoints, n.d.). NefeliPortal that provides
access to this engine is based upon IBM WebSphere
portal framework (IBM, n.d.), a JSR-168 compliant
portal (JSR-168 Portlet Specification, n.d.).
Development of cloud computing applications
that provide readily access to integrated healthcare
information at the point of care introduces security
risks especially with regard to authorization and
access control. To this end, a suitable security
mechanism is embedded into the proposed cloud
portal application, which ensures authorized data
access through the invocation of relevant web
services. Authorization decisions are made subject to
the constraints imposed by the execution context.
With regard to web service invocation, the
security mechanism acts as follows: Upon
submitting a request for invoking a web service, the
roles contained in the CAS certificate accompanying
the request are extracted and their permissions
regarding web service invocations are specified
using a file where XACML policies have been
stored. Then, during web service execution, a
request for executing one of the associated tasks is
issued which is accompanied by the same CAS
certificate. The roles extracted from this certificate
are used in order to specify the permissions
regarding BPEL task executions using XACML
policies which are stored at each client node (i.e.
healthcare organization). Permissions on both web
services and associated BPEL tasks are dynamically
adapted by the constraints imposed by the current
context.
7 CONCLUDING REMARKS
Healthcare organizations are faced with the
challenge to improve quality by preventing medical
errors, to reduce costs by improving administrative
efficiencies, to reduce paperwork and to increase
access to affordable healthcare. One important
healthcare delivery application is EMS system
which has been modeled as an inter-organizational
process involving ambulance services and hospital
emergency departments based on the need for
integrating pre-hospital and in-hospital emergency
care activities into a virtual healthcare enterprise.
Cloud computing and SOA convergence can be
used to meet the increased collaboration and
coordination requirements between emergency
healthcare process participants by facilitating
relevant information access by authorized people
where and when needed. Cloud computing was used
to produce a flexible and scalable system, supporting
interoperability and execution of platform
independent applications while providing secure
access to sensitive data. This paper presents a cloud
EMS system, within the context of a prototype
healthcare portal, namely NefeliPortal. One
important characteristic of the proposed system
specifically calls for the integration of EMS systems
with PHRs and, possibly, other external systems
since systems integration is a prerequisite for
accurate safety alerts, patient monitoring, and other
recommended capabilities.
CONTEXT-AWARE SECURITY IN CLOUD EMERGENCY MEDICAL SERVICES
129

Development of cloud computing applications
that provide readily access to healthcare information
introduces security risks especially with regard to
authorization and access control. Hence, this paper
presented a context-aware security framework which
can be embedded into the EMS cloud application to
ensure authorized invocation of web services and
execution of associated web service tasks subject to
contextual constraints. The security framework
proposed should aid EMS developers in comparing
alternative systems and in prioritizing their
development efforts. However, there is an obvious
need for its real world validation before it is widely
adopted. This requires setting up a cloud computing
infrastructure for eHealth services, an endeavour that
needs much more than proven technological
feasibility.
REFERENCES
Communications of the ACM, 2003. Service-Oriented
Computing, 46 (10).
Active Endpoints, ActiveBPEL Open Source Engine
Project, http://www.activebpel.org/
Anantharaman, V., Han, L., 2001. Hospital and emergency
ambulance link: IT to enhance emergency pre-hospital
care, International Journal of Medical Informatics, 61:
147–161.
Ash, J. S., Berg, M., Coiera, E., 2004. Some Unintended
Consequences of Information Technology in Health
Care: The Nature of Patient Care Information System
Related Errors. Journal of American Medical
Informatics Association, 11(2): 104-112.
Bates, D. W., Leape, L. L., Cullen, D. J., Laird, N.,
Petersen, L. A., Teich, J. M., et.al., 1998. Effect of
Computerized Physician Order Entry and a Team
Intervention on Prevention of Serious Medication
Errors. Journal of the American Medical Association,
280(15): 1311–1316.
Bruening, P., Treacy, B, 2009. Cloud Computing: Privacy,
Security Challenges. In The Bureau of National
Affairs.
Buyya, R., Yeoa, C. S., Venugopala, S., Broberga, J., and
Ivona Brandicc, I., 2009. Cloud computing and
emerging IT platforms: Vision, hype, and reality for
delivering computing as the 5th utility. Future
Generation Computer Systems, 25: 599-616.
Care2X Integrated Healthcare Environment,
http://www.care2x.org/
IBM, IBM Websphere, www.ibm.com/websphere
IBM, 2009. IBM Point of View: Security and Cloud
Computing, Cloud Computing White paper, ftp://
public.dhe.ibm.com/common/ssi/sa/wh/n/tiw14045use
n/TIW14045USEN_HR.PDF
Java Agent Development Framework, http://jade.
tilab.com/.
JSR-168 Portlet Specification, http://www.jcp.org/
aboutJava/communityprocess/final/ jsr168/
Lauer, G., 2009. Health Record Banks Gaining Traction in
Regional Projects, http://www.ihealthbeat.org/
features/2009/health-record-banks-gaining-traction-in-
regional-projects.aspx
Muttig I., Burton C., 2009. Cloud Security Technologies.
Information Security Technical Report, 14: 1-6.
OASIS Standards, http://www.oasis-open.org/
OASIS, 2007. OASIS Web Services Business Process
Execution Language (WSBPEL) v.2, http://docs.oasis-
open.org/wsbpel/2.0/wsbpel-v2.0.pdf
Pearlman, L., Welch, V., Foster, I., Kesselman, C.,
Tuecke, S., 2002. A Community Authorization
Service for Group Collaboration. In the 3rd IEEE
International Workshop on Policies for Distributed
Systems and Networks.
Raines, G., 2009. Cloud Computing and SOA. Service-
Oriented Architecture (SOA) Series, Systems
Engineering at MITRE.
Reddy, M. C., Paul, S. A., Abraham, J., McNeese,M.,
DeFlitch, C., Yen, J., 2009. Challenges to effective
crisis management: Using information and
communication technologies to coordinate emergency
medical services and emergency department teams.
International Journal of Medical Informatics, 78 (4):
259-269.
Rosenthal A., Mork, P., Lia, M. H., Stanforda, J.,
Koestera, D., Reynolds, P., 2010. Cloud computing: A
new business paradigm for biomedical information
sharing. Journal of Biomedical Informatics, 43: 342-
253.
Shimrat, O., 2009. Cloud Computing and Healthcare, San
Diego Physician.org.
Tang, P. C., Ash, J. S., Bates, D. W., Overhage, J. M.,
Sands, D. Z., 2006. Personal health records:
definitions, benefits, and strategies for overcoming
barriers to adoption. Journal of American Medical
Informatics Association, 13 (2): 121-126.
Tentori, M., Favela, J., Rodriguez, M. D., 2006. Privacy-
Aware Autonomous Agents for Pervasive Healthcare,
IEEE Intelligent Systems Magazine, 21 (6): 55-62.
U.S. Department of Health and Human Services: Personal
Health Records and Personal Health Record Systems,
A Report and Recommendations from the National
Committee on Vital and Health Statistics, 2006.
Van der Burg, S., Dolstra, E., 2009. Software
Development in a Dynamic Cloud: From Device to
Service Orientation in a Hospital. Environment, In
2009 ICSE Workshop on Software Engineering
Challenges of Cloud Computing.
Wiljer, D., Urowitz, S., Apatu, E., DeLenardo, C.,
Eysenbach, G., Harth, T., Pai, H., Leonard, K. J.,
2008. Patient accessible electronic health records:
exploring recommendations for successful
implementation strategies. Journal of Medical Internet
Research,. 10 (4).
Win, K. T., Susilo, W., Mu, Y., 2006. Personal Health
Record Systems and Their Security Protection.
Journal of Medical Systems, 30: 309-315.
HEALTHINF 2011 - International Conference on Health Informatics
130
