
REMOTE REHABILITATION OF STROKE PATIENTS
Rafal Wcislo, Jacek Kitowski, Michal Wrzeszcz
Department of Computer Science, AGH University of Science and Technology, Cracow, Poland
Janusz Otfinowski, Karolina Probosz
Collegium Medicum, Rehabilitation Clinic, Jagiellonian University, Cracow, Poland
Artur Sobczyk, Malgorzata Pisula
University Hospital, Rehabilitation Institution, Cracow, Poland
Keywords:
Stroke, Remote rehabilitation, Computer-aided rehabilitation, Multimedia rehabilitation, Telemedicine.
Abstract:
In the paper we present a concept of remote rehabilitation of stroke patients. Rehabilitation plays a vital role
in helping stroke survivors partly or fully recover their functions lost after brain injury. The duration of the
rehabilitation plays a crucial role. We believe that many of common disabilities that result from a stroke can
be treated at patients’ homes with the use of a specially designed computer system. The architecture of the
system is presented as well as its main goals and assumptions.
1 INTRODUCTION
Stroke may have a clear-cut negative impact on pa-
tients’ psychosocial functioning. There are common
disabilities that result from a stroke: decline in at-
tention, selective attention deficits, decline in logi-
cal thinking, planning and reasoning tasks, compre-
hension, synthesis and analysis, weakening of short-
term as well as long-term, verbal and visual memory,
speech disorders (aphasia, dysarthria).
Rehabilitation plays a vital role as it helps the
stroke survivors partly or fully recover their functions
lost after brain injury.
Not only does the choice of proper exercises play
a vital role as well as their correct and systematic per-
formance but the duration of rehabilitation is gener-
ally of utmost importance. It should be as long as
possible. On the other hand, prolonging rehabilita-
tion in the rehabilitation centre is expensive and it
takes another patient’s seat. That is the reason for our
claim that after the rehabilitation in the clinic the pa-
tient should undergo further rehabilitation at home.
The research presented in (Jack et al., 2001;
Broeren et al., 2002; Merians et al., 2002; Sveistrup
et al., 2003; Otfinowski et al., 2006) proved that the
implementation of computer systems specially de-
signed for rehabilitation purposes speeds up stroke
patients’ recovery. Using multimedia in post-stroke
rehabilitation makes the therapy process more inter-
esting. It also motivates patients and makes them
deeply involved in the rehabilitative therapy as it pro-
vides an additional stimuli for their hard and long
work. The reported results reflect enhancement of
our previous development in this field (Kitowski et al.,
2009; Wcislo et al., 2009; Probosz et al., 2009; Szom-
bierski, 2009; Wcislo et al., 2010).
The aim of the project presented in this article is to
adjust the computer rehabilitation program in such a
way as to make it possible for patients to use at home.
Some patients are able to continue their rehabilitation
under the supervision after leaving the clinic. The
doctors are provided with full insight into patients’
performance of exercises having the possibility to re-
motely control and modify the parameters of the re-
habilitative program.
2 COMPUTER-AIDED
REHABILITATION
2.1 Rehabilitation Stages
Post-stroke rehabilitation consists of four stages:
500
Wcislo R., Kitowski J., Wrzeszcz M., Otfinowski J., Probosz K., Sobczyk A. and Pisula M..
REMOTE REHABILITATION OF STROKE PATIENTS.
DOI: 10.5220/0003131605000503
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2011), pages 500-503
ISBN: 978-989-8425-34-8
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)
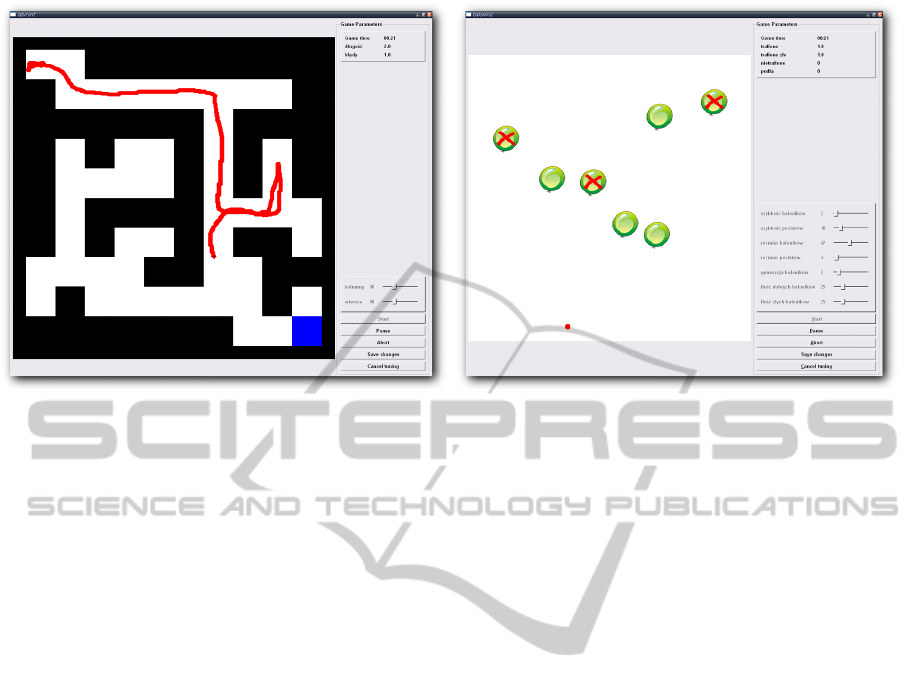
Figure 1: Sample exercises.
• Stage 1: Diagnostics. Types and levels of dis-
ability are estimated on the ground of neurologic
examination and psychological tests.
• Stage 2: The Main Rehabilitation Stage. The
patients perform adequately chosen exercises
within approximately three months’ time.
• Stage 3: Goal Attainment Scaling. A patient un-
dergoes diagnostic evaluation that assesses their
progress.
• Stage 4: Remote Rehabilitation. Chosen pa-
tients might continue rehabilitation at home – an
individualized computer application is prepared
for them that lets the doctors monitor the patients’
exercises via the Internet. The doctors might also
make some changes in the performed tasks.
2.2 Exercises and Trainings
More than 25 rehabilitation exercises have been pre-
pared and verified by psychologists and therapists to
target at different disabilities:
• logopedic exercises for patients affected by vari-
ous forms of aphasia,
• exercises that help retrain stroke-impaired limbs,
• exercises improving cognitive functions (com-
prehension, association, concentration, memory,
etc.).
Some of the exercises take into account more than
one disability at a time. Figure 1 shows screenshots of
sample exercises. Patients perform the exercises with
the use of a joystick, Virtual Reality, a parapodium
gloves or a keyboard.
The therapy consists of clearly designed exercises
– the exercise quantity and the order of exercises are
strictly designated by the training programme. The
difficulty level is controlled by exercise parameters.
The parameters are selected in such a way that the
exercises are neither too difficult (in order not to dis-
courage the patients), nor too easy. During the ther-
apy the computer system stores all the parameters and
the patient’s results (e.g. the duration of exercise, the
number of mistakes). It lets a doctor supervise a pa-
tient’s progress and, if necessary, modify the exercises
and training.
3 REMOTE REHABILITATION
Not all of the patients are able to take part in the re-
mote rehabilitation process. Choosing the proper pa-
tients depends on various factors such as medical rea-
sons (e.g. not all of the rehabilitative exercises may
be performed without a professional supervision) or
the necessity of being the owner of a personal com-
puter and having assistance of somebody who is able
to operate the rehabilitation application.
The access to the Internet is not necessary in order
to perform the exercises. However, the lack of the
Internet access significantly limits the possibilities of
the system. A graphical user interface of the software
installed on a patient’s computer is to be identical with
the one that the patient worked on while staying in the
clinic. It will facilitate the start of a rehabilitation at
home. The system is characterized by the following
activities or features:
• The program installed at patient’s home sends the
achievement scores to the clinic immediately after
REMOTE REHABILITATION OF STROKE PATIENTS
501
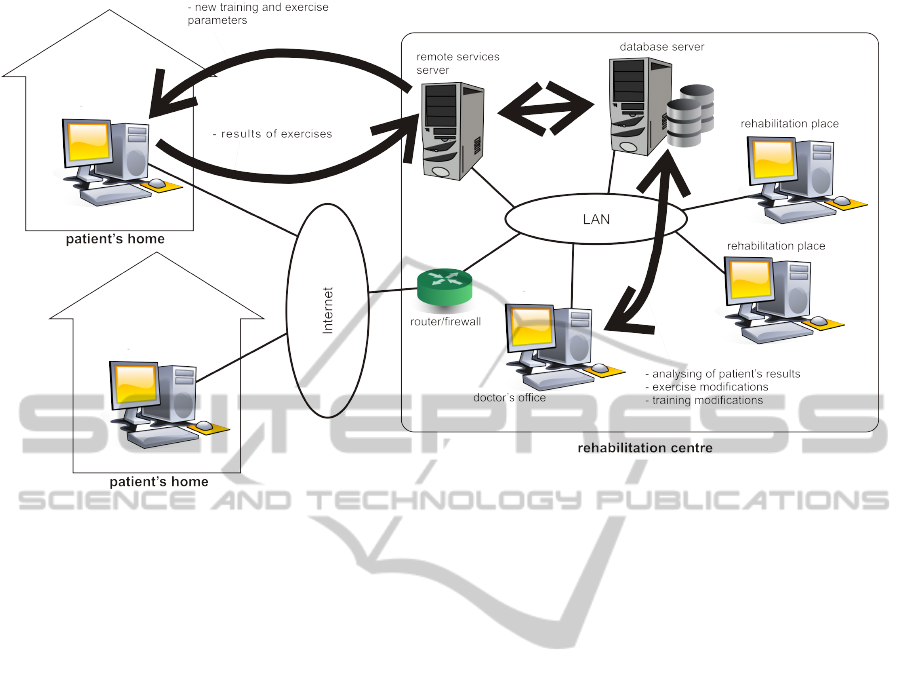
Figure 2: System architecture.
the completion of each exercise, or – if there is
no access to the Internet– as soon as the Internet
connection is established.
• On the grounds of patient’s scores a doctor is able
to change the parameters of the exercises and the
trainings so that they can meet the requirements of
the rehabilitation better. These modifications are
automatically sent to the patient’s application via
the Internet.
• Considering the necessity to keep the personal
data confidential and secure the transmission be-
tween the rehabilitation program and the clinic is
encrypted and authenticated bilaterally on the ba-
sis of the previously generated (in the clinic) cer-
tificates. The login and the password are remem-
bered due to automatic authentication of the pa-
tient.
• Due to the same reasons the client’s application
are devoid of personal details or the information
about the disease since such data is stored only in
the rehabilitation centre.
Additionally, a simultaneous audio-video connec-
tion between a doctor and a patient during the exercise
performance is anticipated. The doctor will watch the
patient doing the exercise on one’s computer screen
and will be able to provide additional explanation or
give another piece of advice.
As the number of patients shall grow due to the
necessity of dealing with the remote patients, the ad-
visory system that aids rehabilitation doctors shall be
developed as well. The doctors will be able to get
immediate information on each patient including the
data about their exercise progress. The system shall
automatically highlight the fact that a patient omits
certain exercise or does it too rarely; it will also in-
dicate if any exercise is performed too easily or is of
great difficulty to a patient.
What seems to be a more difficult challenge is the
implementation of the procedures that could propose
the modification of exercises on their own (e.g. by
making the exercises more difficult) if there is a long
break in the Internet connection between a clinic and
a patient. It would surely stimulate the patient more
and make it possible to avoid the monotony.
4 SYSTEM ARCHITECTURE
Figure 2 presents the architecture of a computer sys-
tem used in post-stroke rehabilitation. Its most impor-
tant components are as follows:
• A database server that stores patients’ details, pa-
tients’ trainings, parameters of exercises and all
of their achieved scores (performance duration,
number of mistakes, screenshots, a set of parame-
ters for which the exercise is performed).
• A remote services server for communication with
patients’ programs activated outside the clinic.
• Client applications intended for the doctors to fol-
low the patients’ progress and modify the exer-
HEALTHINF 2011 - International Conference on Health Informatics
502

cises and trainings. Already existing trainings
might also be used as templates for creating train-
ings for new patients – what really facilitates the
preparation of a rehabilitation program.
• Rehabilitation applications that are located in the
clinic and in the patients’ house. They are used
for performing the rehabilitation.
All applications are written in C++ using Nokia
Qt environment and libraries. As the database server
MySQL RDBM system is used.
5 EXPLOITATION NOTICE
The rehabilitation system is in the routine local op-
eration in the Rehabilitation Clinic, CM UJ. Accord-
ing to the tests (Wcislo et al., 2010) for both apha-
sia disease and concentration and memory dysfunc-
tion important improvement of patients’ ability was
observed. The pilot version of the system for the re-
mote rehabilitation (section 3) has already been vali-
dated functionally, proving its reliable operation.
6 CONCLUSIONS
The research has proved the usability of a computer-
aided rehabilitation. However, the duration of the re-
habilitation plays a crucial role and it is not advisable
to finish it after three months. We hope that the remote
rehabilitation shall make it possible for many patients
to continue their treatment at home and it shall influ-
ence their full recovery.
Our future work will be focused on paradigms of
exploration of the existing data kept in the relational
database system in order to extract knowledge con-
cerning a rehabilitation process of each patient sepa-
rately. The knowledge will be further used for defin-
ing patients’ profiles to be used by a kind of advice
system for both medical doctors and patients. Its role
will be to generate hints autonomously on the basis
of extracted knowledge for the doctors and patients
concerning continuation of the rehabilitation process.
ACKNOWLEDGEMENTS
This research is financed partially by Polish Min-
istry of Education and Science, Project No. N N519
315435 and by the AGH grant No. 11.11.120.865.
REFERENCES
Broeren, J., Bjorkdahl, A., Pascher, R., and Rydmark, M.
(2002). Virtual reality and haptics as an assessment
device in the postacute phase after stroke. In Cy-
berpsychol. Behav., pages 207–211.
Jack, D., Boian, R., Merians, A., Tremaine, M., Burdea, G.,
Adamovich, S., Recce, M., and Poizner, H. (2001).
Virtual reality-enhanced stroke rehabilitation. In IEEE
Trans. Neural Syst. Rehabil. Engng., volume 9 (3),
pages 308–318.
Kitowski, J., Wcislo, R., Slota, R., Otfinowski, J., Skubis,
M., Probosz, K., Pisula, M., Sobczyk, A., and Regula,
K. (2009). Distributed computer system for remote
support of holistic rehabilitation of patients affected
by stroke. In Proc. of CGW’08, Cracow, Poland,
pages 388–392. ACC Cyfronet AGH.
Merians, A., Jack, D., Boian, R., Tremaine, M., Burdea, G.,
Adamovich, S., Recce, M., and Poizner, H. (2002).
Virtual reality-augmented rehabilitation for patients
following stroke. In Phys. Ther., volume 82 (9), pages
898–915.
Otfinowski, J., Jasiak-Tyrkalska, B., Starowicz, A., and
Regua, K. (2006). Computer-based rehabilitation of
cognitive impairments and motor arm function of pa-
tients with hemiparesis after stroke. In Neurologia
i Neurochirurgia Polska, volume 40 (2), pages 112–
118.
Probosz, K., Wcislo, R., Otfinowski, J., Slota, R., Kitowski,
J., Pisula, M., and Sobczyk, A. (2009). A multi-
media holistic rehabilitation method for patiens after
stroke. In Wiederhold, B. and Riva, G., editors, An-
nual Review of Cybertherapy and Telemedicine 2009,
Advanced Technologies in the Behavioral, Social and
Neurosciences, Studies in Health Technology and In-
formatics, volume 144, pages 261–263. IOS Press.
Sveistrup, H., McComas, J., Thornton, M., Marshall, S.,
Finestone, H., McCormick, A., Babulic, K., and May-
hew, A. (2003). Experimental studies of virtual
reality-delivered compared to conventional exercise
programs for rehabilitation. In Cyberpsychol Behav.,
volume 6 (3), pages 245–249.
Szombierski, A. (2009). Development of NLP algorithms
for rehabilitation of patients affected by aphasia,
M.Sc. Thesis (In Polish). AGH-UST, Cracow, Poland.
Wcislo, R., Kitowski, J., Slota, R., Otfinowski, J., Regula,
K., and Probosz, K. (2009). Concept of virtual or-
ganization paradigm for holistic rehabilitation of pa-
tiens after stroke. In Tadeusiewicz, R., Ligeza, A.,
Mitkowski, W., and Szymkat, M., editors, Proc. of 7th
Conference ’Computer Methods and Systems’, Opro-
gramowanie Naukowo Naukowo-Techniczne, pages
345–350.
Wcislo, R., Probosz, K., Kitowski, J., Slota, R., Otfinowski,
J., Sobczyk, A., and Pisuala, M. (2010). Multimedia
holistic rehabilitation method for patiens after stroke
- efficiency analysis. In Wiederhold, B., Riva, G.,
and Kim, S., editors, Annual Review of Cybertherapy
and Telemedicine 2010. Advanced Technologies in Be-
havioal, Social and Neurosciences, Technologies and
Informatics, volume 154, pages 67–72. IOP Press.
REMOTE REHABILITATION OF STROKE PATIENTS
503
