
DETERMINANTS OF IT ADOPTION IN HOSPITALS
IT Maturity Surveyed in an European Context
Patrick Mikalef and Ronald Batenburg
Institute of Information and Computing Science, Utrecht University, Padualaan 14, Utrecht, The Netherlands
Keywords: Hospitals, IT Adoption, IT Maturity, European Study, Survey research.
Abstract: Following the increase of investments in Information Technology (IT) in organizations and companies
during the past decade, hospitals are expected to increase their IT maturity as well. But what drives hospitals
to invest in IT, in particular integrative and enterprise-wide IT? In the present study we make an attempt to
identify key elements of IT adoption for the hospital enterprise, and formulate a model in order to assess
their level of IT adoption and maturity. Driven by this model and based on survey data from an European
research conducted on 18 countries, statistical analysis is performed. It indicates that IT adoption in
hospitals is strongly related to size, i.e. the number of employees and the number of beds of a hospital.
Additionally, it is revealed that there are significant differences in adoption levels between general and
specialized health care hospitals. Finally, a cross-country analysis shows striking differences between the 18
EU countries in the IT maturity of hospitals as well, from which pioneering as well as the straggling clusters
of countries can be classified.
1 INTRODUCTION
Investments in Information Technology (IT) have
increased dramatically over the past decade in
organizations and companies. At the same time,
organizations and their managers struggle on gaining
a financial as well as a competitive advantage from
their IT investments (Venkatesh et al, 2003).
According to some estimations, since the 1980`s
approximately 50 percent of capital investment has
been spent on IT systems (Westland and Clark,
2000). Several empirical studies have indicated that
investments in IT, after some time, positively affect
the overall performance of organizations (Raymond
et. Al., 1995; Chan et al., 1997). Others claim that IT
can likewise take firms down, with greater
expenditures rarely translating into superior financial
results (Carr, 2003). Many agree that the same
controversy also applies for organizations of the
healthcare sector. Most organizations within the
health care sector represent the area of primary care
(e.g. general practitioners, dentists, pharmacists). To
specifically explore the resemblance between private
and public organizations in their IT investments and
IT maturity however, this study will focus on what is
called ‘the Hospital Enterprise’ (Lorenzi & Riley,
1995; Hatcher, 1998; Paré & Sicotte 2001).
Even though hospitals seems to be delayed in
deploying IT systems because of their ‘legacy
burden’, one of the most important drivers for them
to invest in (Health) Information Technology is the
need to minimize operating costs. It is estimated that
up to $81-162 billion can be saved annually for both
inpatient and outpatient care and approximately
200.000 potentially fatal adverse drug events can be
eliminated each year (Taylor et al., 2005; RAND
2005) cutting costs by an additional $1 billion. The
largest percentage of savings occurs from the
reduced hospital stays, the need for fewer nursing
staff and more efficient drug utilization. Furthermore
by adopting Health Information Technology (HIT)
age-adjusted mortality could be lowered by 18
percent and days taken off work due to sickness
could be reduced by 40 million annually (Taylor et
al., 2005). In addition, there is a need for a safer
system with less human errors which is emphasized
in a 2000 report which estimates that as many as
98,000 patients die each year from preventable
medical errors (Kohn et al., 2000). Furthermore, in
the last years there is a tendency to shift from a
institution (supply) centered healthcare system to a
more patient (demand) oriented one. This has forced
hospitals to apply IS/IT that is patient and process
oriented rather than administrative oriented. This
164
Mikalef P. and Batenburg R..
DETERMINANTS OF IT ADOPTION IN HOSPITALS - IT Maturity Surveyed in an European Context.
DOI: 10.5220/0003132001640173
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2011), pages 164-173
ISBN: 978-989-8425-34-8
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

shift occurs from the need to standardize operations
and to create a more safe and flexible health care
system (Bates & Gawande, 2003). Because of the
specific complexity of the hospital sector, the shift
towards a patient-oriented model proves to be very
difficult. Unlike other industries, IS/IT in health
cannot enable “mass customization”. While mass
customization refers to the efficient, reliable
production of services and goods based on the
personalized requirements of the customer (Bates &
Gawande, 2003), ‘health’ is highly sensitive and
intangible good that does not comply with the
standard economic model of production and
consumption. It might be for this reason, that most
of the expenditure in IT within hospitals is aimed at
administrative tasks such as accounting and
logistics, (Haux et al., 2002; Brynjolfsson & Hitt,
2000). At a slow pace, investments shift from IT that
support the execution of daily tasks to more
hospital-wide and integrative IS/IT.
The adoption and maturity of IS/IT in hospitals
has been hardly analyzed in an empirical way, i.e.
measured, let alone monitored and evaluated for its
potential value to improve quality and cut costs.
Based on existing measurement methods, and driven
by an unique data sample of European hospitals, we
explore a measurement for IS/IT adoption and
maturity by hospitals. We also construct a
conceptual model in order to determine and evaluate
the level at which hospitals make effective use of
these systems. Besides this theoretical contribution,
we claim that such an conceptual model makes it
easier to create an adoption plateau for hospitals in
order to plan deployment phases for IT systems. In
another practical sense, it can also provide useful
information about the outcomes of each level of
adoption. It is for this reason that this paper aims to
theoretically develop an IT maturity model for
hospitals, and empirically apply and validate this on
a large-scale dataset.
1.1 Structure
This paper is structured as follows. In the next
section, a literature overview is presented on the
most relevant and recent work on IS/IT adoption in
hospitals. Section 3 introduces a conceptual model
developed to measure IT maturity and IT adoption in
hospitals. Section 4 presents the sample that is used
for empirical validation of the model, as well as the
basic statistical analysis and methods applied. In
section 5, the determinants are tested that are
expected to have an influence on the IT adoption
level of hospitals, i.e. their size, type and home
country. Finally section 6 includes the conclusions
which are drawn about the results and a discussion
about how this research can be extended or
continued.
2 RELATED WORK
In order to study the adoption level of IS/IT in the
hospital sector, many researchers have started by
classifying the different systems that are used and to
create a scale that represents the maturity of these
systems. In their study Heinzl & Guttler propose a
five stage model of hospital IT reconfiguration based
on Venkatramans model of maturity (Heinzl &
Guttler, 2000). Venkatraman’s model became
particularly known since it describes stages of how a
business can be reconfigured in order to make use of
available IT systems and gain a competitive
advantage (Venkatraman, 1991). In their study,
Heinzl & Guttler focus on the strategies, IT
characteristics and organizational variables and their
association with the five levels of maturity of the
Venkatraman model. The study of Pare & Sicote
also focuses on measuring the level of IT maturity in
the hospital sector, influenced by the EDP growth
model of Nolan. The authors distinguish between
technological sophistication – which include the
different hardware devices – and functional
sophistication – which represent the diversity of
activities or processes (Pare & Sicote, 2001). Based
on this two-dimensional distinction the authors
present a framework in which hospital activities are
divided into three parts, the administrative activities,
patient management and patient care activities and
finally clinical support activities. For each of these
the technological and functional sophistication is
measured. Also, the framework takes into account
the external partners of hospitals such as clinics,
laboratories etc.
Source: Pare´ G., & Sicotte C. (2001) Information
technology sophistication in health care: an
instrument validation study among Canadian
hospitals. International Journal of Medical
Informatics, 63, 205-223.
A recent study by the Healthcare Information and
Management Systems Society (HIMSS) specifies the
adoption rate of Electronic Medical Records (EMR)
by presenting an eight stage model. It starts from
stage ‘0’ where no major ancillary department
systems for laboratory, pharmacy and radiology are
implemented, to stage 7 where medical records are
fully electronic. The HIMSS model represents the
necessary steps that are required so all patient
DETERMINANTS OF IT ADOPTION IN HOSPITALS - IT Maturity Surveyed in an European Context
165
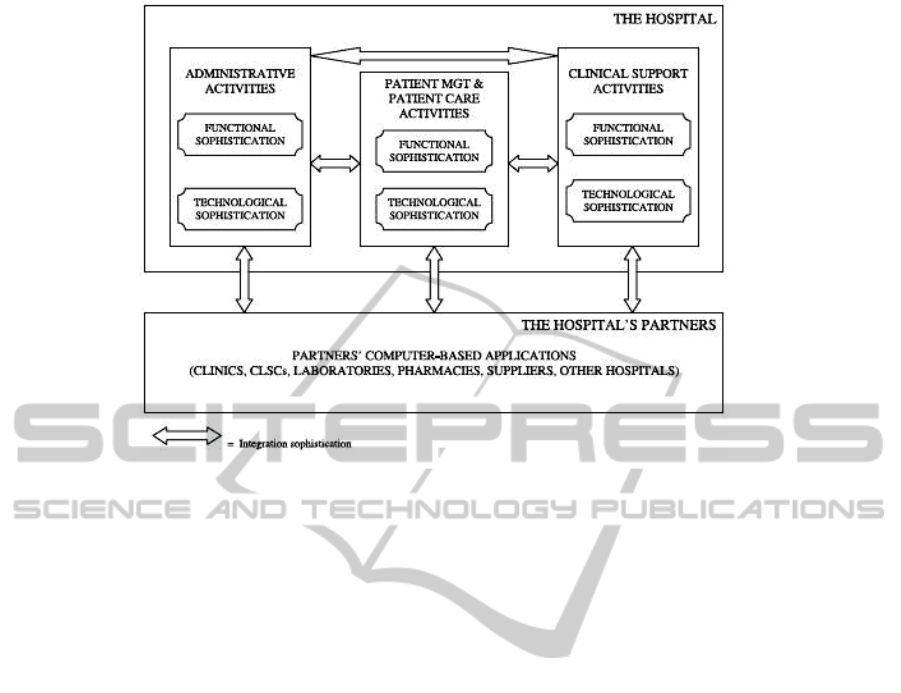
Figure 1: IT Sophistication framework in hospitals.
related functions are completed electronically.
Although this model provides a planning tool for
adopting EMR systems, it does not apply for other
IS/IT used by hospitals.
3 A CONCEPTUAL MODEL FOR
IT ADOPTION BY HOSPITALS
Following the work of the scholar’s referred to in the
above section, we develop our conceptual model for
IT maturity in hospitals by first identifying the
elements of IS/IT adoption in the hospital enterprise.
The common attributes of the frameworks presented
in the previous section are used to define the ‘pillars’
of measuring hospital IT adoption. Commencing
from the work of Tornatzky & Fleischer (1990), who
in their framework study the adoption of E-Business
in a wide range of enterprises, we identify six
different pillars or key elements of IT adoption.
• As in all industries including the hospital
sector, IT infrastructure must be present in
order to support all necessary activities either
within the hospital or between business
partners. This need for IT infrastructure is also
pinpointed in the study of Pare and Sicote who
name it technological sophistication and place it
in all four variables of their framework.
• Next to infrastructure, Tornatzky & Fleischer
allocate a central position in their framework to
IT expertise, referring to the knowledge and
skills of the people involved in the use of IT
systems. This IT expertise or e-skills is a
variable used in many frameworks of IT
adoption which underlines its importance
(Tornatzky & Fleischer, 1990; Zhu et al, 2002).
• Another important part of the Tornatzky &
Fleischer Technology – Organization –
Environment framework is the Industry Specific
Know-how with regard to IS/IT. This variable
addresses both the IT knowledge of the (top)
management, as well as the organizational
knowledge of the IT managers and consultants
(cf. Luftman, 2000, 2007). Basically, this is
about business/IT alignment (Chan & Reich,
2007), in this context expressed as the expertise
to understand healthcare specific IT.
• To model IT maturity from an integrative, i.e.
cross-functional and external perspective, we
propose that IT maturity should also address the
concept of online sales & marketing. The rise
of client or customer orientation mentioned
earlier, has radically redesigned processes
within numerous organizations, including
hospitals. The introduction of the Electronic
patient Record illustrates this, but also the
cooperation between hospitals and health
insurance organizations that are the main
financial customers of hospitals in many
countries.
• In line with the previous element, online
HEALTHINF 2011 - International Conference on Health Informatics
166

Figure 2: Classification of six hospital IT adoption elements.
sourcing & procurement can be considered a
business function that has been significantly
digitized, which is described by many authors
(Beukers et al., 2006; Kiang et al., 1999).
Another aspect that has an influence on the
adoption of IT systems is the readiness of
trading partners which is also included in the
framework of Tornatzky & Fleischer. In their
study they regard the lack of trading partners as
an inhibitor for the adoption of E-Business
systems, and with the same rationale we make
the assumption that the more ready trading
partners there are, the more likely a hospital
will be to adopt IT systems. This fact is also
denoted in the work of Pare & Sicotte, where
the hospitals external partners are included in
their framework and are considered an
important factor in IT sophistication for the
hospital sector.
• Finally one last factor that is becoming
increasingly important due to the large number
of interacting IT systems is that of e-Standards.
A number of authors refer to the increasing
concern in the use of e-Standards, including
Chen, who underlines the importance of
integrating different IT systems with other
external partners as well as internally (Chen,
2002).
The six elements described above comprise the
first part of our conceptual model. The second part
of the model consists of a scale that measures each
of the 6 elements in terms of actual adoption and
maturity level of IT in hospitals. This maturity
classification can be considered as the second
dimension of our conceptual model that is combined
with the first dimension, being the six elements of IT
adoption as described above. We measure the
maturity of each element on a scale from a situation
where no IT or related processes exist within a
hospital, to the highest level of IT adoption in which
the full potential of IT is leveraged to shape and
transform business operations both internally and
externally. The graph below shows the two
dimensions of our conceptual model and how this
stretches the IT maturity field. The dots and line
depict an example of a hospitals score using this
model. The shape and position of the line indicate
both the level and balance of IT maturity.
3.1 Hypotheses
Having constructed the model of IT adoption in
hospitals in the previous section, it is possible to
make a number of assumptions based on prior
research before analyzing the datasets. IT adoption
levels within hospitals will be benchmarked over
three aspects; the size of the hospital (number of
employees and/or beds), the type and ownership of
the hospital, and the country in which it operates.
According to earlier studies on adoption by cf.
Rogers, it can be expected that large organizations
have an inclination to being more innovative when
considering IT solutions (Rogers, 1983). For e-
business adoption, this is empirically confirmed by
e.g. Batenburg & Constantiou (2008) and Teo, Lin
and Lai (2009). Consequently, we expect the same
for the hospital enterprise.
• H1. Larger hospitals can be expected to be
more innovative, thus having a higher level of
IT adoption.
From past research it can be expected that the
various strategies of hospitals types differ (cf.
Liedtka, 1992), resulting in different IT adoption
levels as is found to apply in organizations of
various sectors.
• H2. Significant differences in IT adoption can
be expected between the individual types of
hospitals.
Many country differences within Europe in IT
adoption can be found on studies conducted on a
range of systems and business domains,
consequently we can expect the same to apply for
DETERMINANTS OF IT ADOPTION IN HOSPITALS - IT Maturity Surveyed in an European Context
167
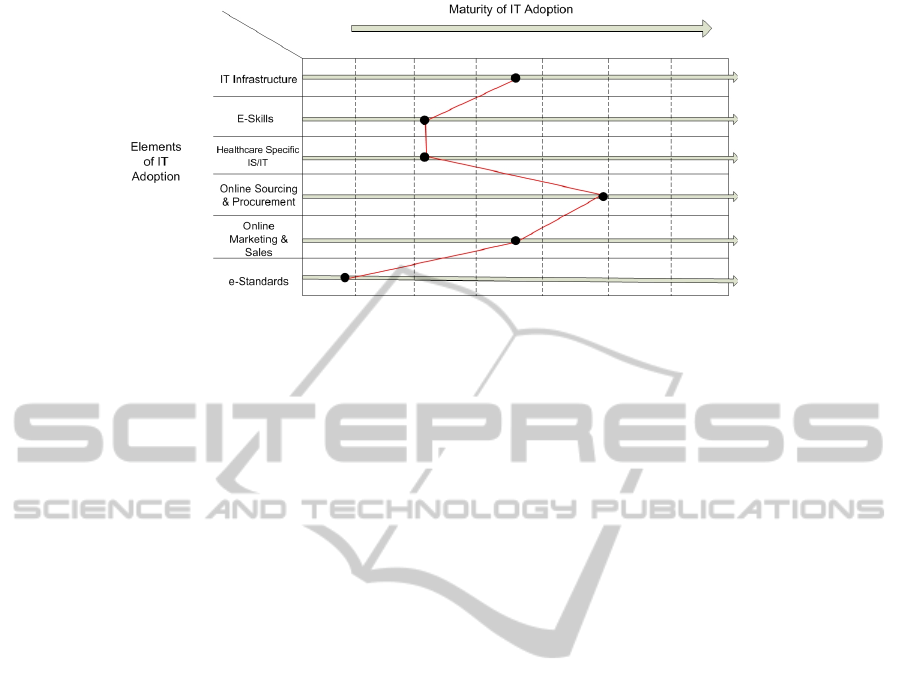
Figure 3: A conceptual model for IT hospital maturity.
hospitals (cf. Selhofer et al., 2008),
• H3. Significant variations can be expected
between countries mean levels of IT adoption.
4 DATA AND MEASUREMENTS
4.1 Dataset
The survey data used for this paper to empirically
validate the conceptual model were collected
through the e-Business W@tch project in 2006. This
EU-funded project has the aim of studying the
impact that e-Business and IT have on a range of
business sectors. The data collection was performed
through a Computer-assisted telephone interview
(CATI) based on a questionnaire which was
completed by 834 hospital respondents in 18
European countries. For each hospital one
respondent responsible for decisions in the IT field
(Head of IT department, Senior in IT department or
Manager for smaller hospitals) was asked to answer
the survey questions consisting of ten modules as
well as some questions about the background of the
hospital. The hospitals that are present in the dataset
include general health care hospitals as well as
specialized health care hospitals.
4.2 Measurements
We measure the six elements of IT adoption in
hospitals as described in the conceptual model. In
order to measure the maturity level of these
elements, a number of questions were selected from
the e-Business W@tch questionnaire. Below all
elements of the IT adoption model are described by
the original survey questions. All questions were
coded in the same binary manner for consistency,
where one point is assigned to each question
answered as Yes and no points are assigned in the
case where the answer is either No or Don`t Know.
4.3 Variable Construction
For each element, the maturity score ranges from a
minimum of zero points (all answers “No” or “Don`t
Know”) to a maximum that depends on the numbers
of questions (all answers “Yes”).The cumulative
score of each element is divided by the total number
of questions so that the scale is standardized
between 0 (none of the questions is positively
answered) and 1 (all of the questions are positively
answered). In order to estimate the overall IT
adoption level for each hospital, the un-weighted
average of all six dimensions is accounted. In all
variable constructions we assume that all questions
per element, and likewise all elements in
accumulation, are of equal importance.
5 ANALYSIS AND RESULTS
The e-Business W@tch dataset contains a vast
amount of information to explore the determinants
of IT adoption in the hospital enterprise. In this
section, the IT adoption and maturity of hospitals is
first described based on our conceptual model. Then
the variation in IT maturity is analyzed by
correlating it with three ‘independent’ variables, (1)
the size of hospitals (i.e. the number of employees
and number of beds), (2) their home country and (3)
the type of hospital (general health care or
specialized health care, and public, non-profit or
private). Not only will the overall IT maturity level
serve as the dependent variable, also each element of
the IT adoption concept will be examined separately,
HEALTHINF 2011 - International Conference on Health Informatics
168

IT Infrastructure
Q: In what way does your hospital enable remote access? Does it enable remote access via:
(1) Fixed line connections, (2) Wireless-Local-Area-Networks or W-LANs, (3) Mobile
communication networks, for example by using mobile devices, (4) Virtual private Network
(VPN)
Q: I am going to read you a list of network applications. For each, please tell me if your hospital
uses this application or not. Does your hospital use:(1) Local Area Network (LAN), (2) Wireless
LAN, (3) Voice-over-IP
e-Skills
Q: Does your hospital use e-learning application that is for instance learning material for
employees available on an Intranet or on the Internet?
Q: Does your hospital regularly send employees to ICT training programmes?
Healthcare Specific IS/IT
Q: Does your hospital use the following departmental systems: (1) Patient Administration
System , (2) Radiology Information System (RIS), (3) Picture Archiving Systems (PACS) and
medical image transmission, (4) Pharmacy Management System, (5) Electronic Transmission of
Prescriptions, (6) Computerised Physician Order Entry (CPOE)
Online Sourcing & Procurement
Q: Does your hospital use the internet or other computer-mediated networks to place order for
goods or services online?
Q: Does your hospital currently support the selection of suppliers or procurement processes
by using specific IT solutions?
Q: Which of the following sourcing or procurement related processes does your hospital
support by specific IT solutions? Do you use IT solutions for: (1) Finding suppliers in the
market, (2) Inviting suppliers to quote prices or submit proposals, (3) Ordering goods or
services, (4) Running online auctions
Online Marketing & Sales
Q: Does your hospital have its own website on the internet?
Q: Does your hospital use a CRM system that is specific software for customer relationship
management?
Q: Does your hospital allow customers to order goods or book services online from the
website or through other computer-mediated networks?
Q: Does your hospital support marketing or sales processes by using specific IT solutions
Q: Which of the following marketing or sales related processes does your hospital support by
specific IT solutions? Do you use IT solutions for: (1) Receiving orders from customers, 92)
Enabling customers to pay online for ordered products or services
e-Standards
Q: Does your hospital take into account industry specific standards when making decisions on
what technology and data standards to use?
Figure 4: The e-business w@tch questions used for measuring for IT hospital maturity.
in relation to the three independent variables. Hence
a larger number of correlation analyses can be
applied to check stability of results.
By performing a descriptive analysis on the six
elements used in the IT adoption model we present
Table 1 below. The first observation is that hospitals
have a higher level of IT adoption of Healthcare
Specific IS/IT in comparison with the other five
elements. On average, hospitals tend to have 44% of
these applications adopted. In contrast, hospitals
have lower adoption rates with regard to Online
Marketing & Sales and Online Sourcing &
Procurement. On average only 18% of the questions
of this element are positively answered. This shows
that most hospitals did not set the step towards
external IS/IT application, i.e. the e-business type of
investments
5.1 Size and IT Adoption
When exploring hospital size into account as a
potential determinant of IT maturity, we examine
two elements, (1) the number of employees, as well
as (2) the total number of beds that the hospital
accommodates. Entries where the respondent did not
provide information on the number of employees or
beds were excluded. Because of this, the total
number of hospitals dropped to 773 with regard to
DETERMINANTS OF IT ADOPTION IN HOSPITALS - IT Maturity Surveyed in an European Context
169
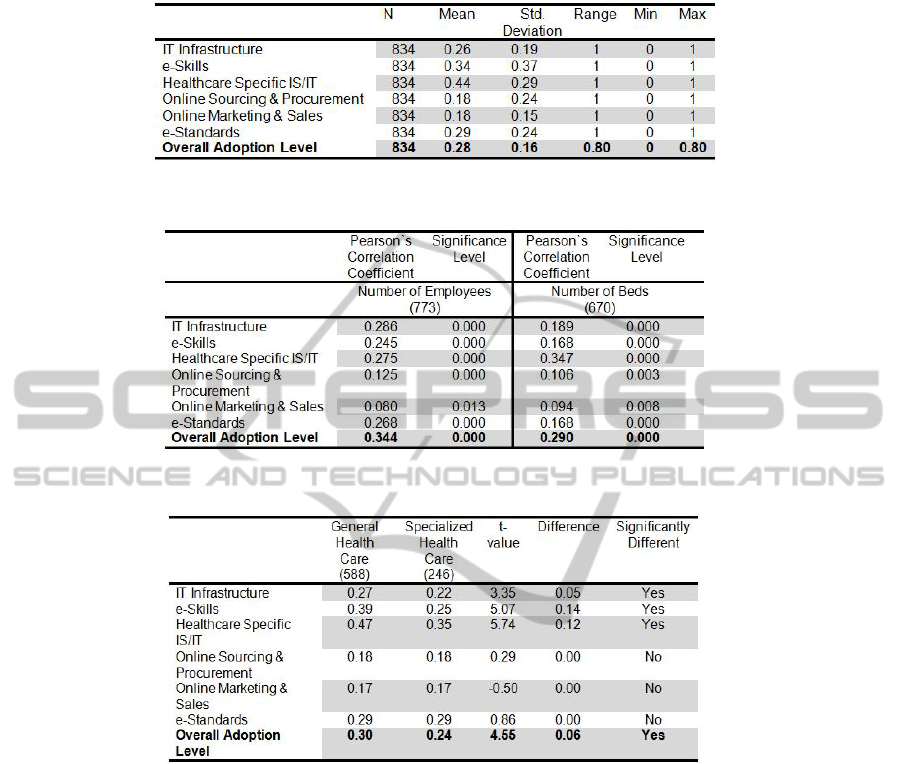
Table 1: IT Adoption Descriptive Statistics.
Table 2: Correlation Analysis: IT Adoption/Absolute number of employees & number of beds.
Table 3: Level of IT adoption by type of hospital.
the absolute number of employees, and to 670 with
regard to the absolute number of beds.
The results of (Pearson) bivariate correlations
analyses confirm our expectation, both for the
number of employees as well as for the number of
beds as indicators of hospital size. The correlation
analyses were pretested checked by computing the
log of both size measurements to control for
skewness of distribution. The results remain the
same. We can therefore conclude that size
significantly matters for the hospital IT adoption and
its maturity elements.
5.2 Type of Hospital and IT Adoption
Another relevant characteristic to be studied is the
type of hospitals, basically distinguishing general
health care and specialized health hospitals, and
public, non-profit and private hospitals. Our sample
consists of 834 hospitals of which 588 are general
health care hospitals and 246 are specialized health
care hospitals. In addition, the ownership of the
hospitals can be broken down with a total of 821
hospitals of which 361 are public, 101 non-profit
and 359 are private. Table 3 and 4 show the results
of split sample analysis and significant test of the
between group differences.
Results from the paired sample T-Test in Table 3
indicate that general health care hospitals have
significant higher IT adoption rates with regard to
the elements of IT infrastructure, e-Skills, and
Internal & External e-Collaboration as well as for
the Overall adoption Level. It appears that these
significant differences are spread over the six
different elements, confirming the general hospital
broadly and generally invest in IT.
HEALTHINF 2011 - International Conference on Health Informatics
170
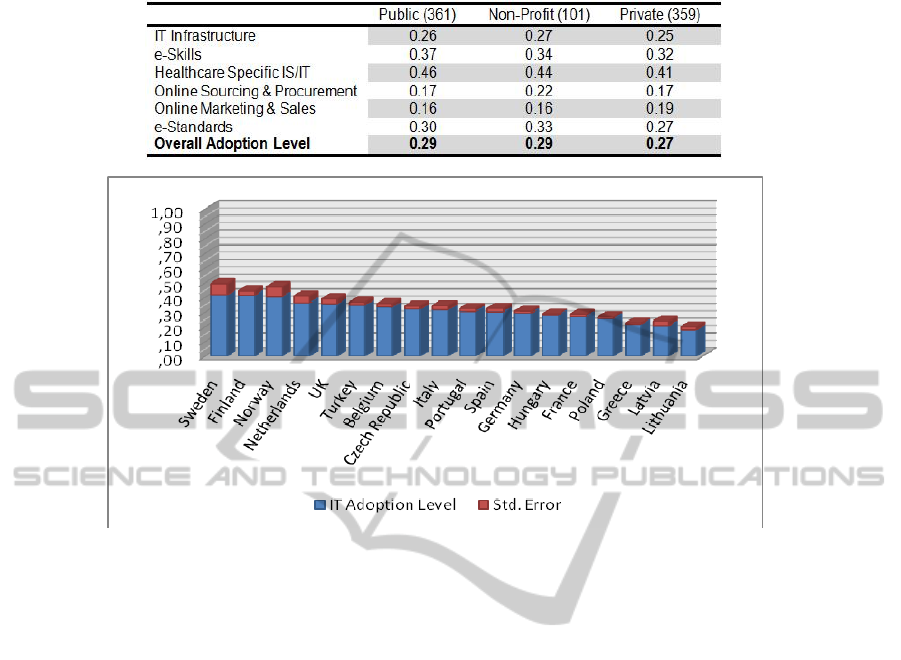
Table 4: Level of IT adoption by type of hospital.
Figure 5: Adoption level of IT in hospitals by country.
Table 4 shows the group averages of the public,
non-profit and private hospitals. Results of t-tests on
all pairs showed no significant differences in IT
adoption level for any group difference. Apparently,
the group differences are too small to be significant,
indicating that this hospital characteristic is not as
important as the distinction between general versus
specialized. One interesting observation from Table
4 though, is that private hospitals have lower
adoption rates in all elements as well as in overall
adoption except for the Online Marketing & Sales
element. This might be explained by the need for
private hospitals act in a ‘competitive’ market.
5.3 IT Adoption by Country
Our final analysis concerns the comparison between
the IT adoption rates by hospitals for each country.
The aim is to identify which countries are front
runners of IT adoption in their hospital enterprises,
and explore what elements might influence in
comparison with other countries. Figure 3 shows the
results for the average and overall IT adoption scale,
included its standard error by country.
Performing an Analysis of Variance on the
dataset, the differences between countries appear to
be significant. The highest IT adoption rates are by
hospitals from Sweden (0.42), Finland (0.41) and
Norway (0.40). The three countries with hospitals
that have the lowest IT adoption levels are Lithuania
(0.17), Latvia (0.18) and Greece (0.20). The fact that
the Scandinavian hospitals are the (relative)
frontrunners in IT maturity, complies with a number
of studies that indicate their leader position within
Europe in terms of ‘Networked Readiness Index’
(OECD, 2004) as well as in per capita spending in
IT (OECD, 2008). However, fully explaining these
differences in IT adoption and their underlying
reasons is a challenge which a number of scholars
have tried to investigate (Batenburg, 2007; Miller et
al;. 2006; Van Everdingen & Waarts, 2003).
6 CONCLUSIONS & FURTHER
RESEARCH
In this paper we studied the IT adoption of 834
hospitals across 18 European countries and
investigated a number of determinants of a hospitals’
IT maturity. The study was based on a model we
developed for IT adoption in hospitals, consisting of
six elements and five maturity levels. The
construction of this model was based on both
DETERMINANTS OF IT ADOPTION IN HOSPITALS - IT Maturity Surveyed in an European Context
171

hospital specific as well as general IT and
organizational studies.
Summarizing we conclude that the number of
employees of a hospital has a significant positive
correlation with the IT adoption level as well as with
its elements. Also, hospitals with larger amounts of
beds have a significantly higher IT adoption rate,
indicating that size strongly matters for IT maturity
in the hospital sector.
In addition, the IT adoption levels for different
types of hospitals were compared. We found that
there is a significant difference between general and
specialized health care hospitals with the former
having higher overall IT adoption rates. Contrary to
our expectation, when comparing between public,
non-profit and private hospitals no significant
differences were found.
Finally, the cross-country adoption level is
analyzed for all 18 countries the responding
hospitals are located in. Results indicate that there
are large differences between countries, with
Scandinavian hospitals having high levels of IT
adoption (Sweden, Finland, Norway) compared to
hospitals from eastern and south European countries
(Lithuania, Latvia, Greece).
Many issues remain to be explored and issued. In
particular, the country differences in IT adoption by
hospitals are subject for further research. How to
identify the reasons that lead this variation of
results? How do country differences relate to other
factors, both on the country as on the hospital level?
REFERENCES
Batenburg, R. (2007). Cumulating Conditions. An
empirical analysis of the EIS adoption by European
firms. In: M. Lynne Markus, J. Felix Hampe, J. Gricar,
A. Pucihar & G. Lenart (Eds.), Conference
proceedings of the 20th Bled eConference, June 3-6,
Bled, Slovenia. Bled: University of Maribor, Faculty
of Organizational Sciences.
Batenburg, R., Constantiou, I. D. (2009). A European
Study of E-Business Maturity and ICT-benefits: Is
there a Conditional Relationship?. In: S. Newell, E.
Whitley, N. Pouloudi, J. Wareham, L. Mathiassen
(Eds.) Proceedings of the 17th European Conference
on Information Systems, Verona, Italy, June 8-10.
Bates D. W. & Gawande A. A. (2003) Improving Safety
with Information Technology. The new england
journal of medicine, 348, 2526-34.
Beukers M., Versendaal J., Batenburg R., and
Brinkkemper S. (2006) The Procurement Alignment
Framework Construction and Application.
WIRTSCHAFTSINFORMATIK 48(5), 323-330.
Brynjolfsson E., & Hitt L. M. (2000) Beyond
Computation: Information Technology, Organizational
Transformation and Business Performance. Journal of
Economic Perspectives, 14(4), 23-48.
Carr G. N. (2003) IT Doesn’t Matter. Harvard Business
Review 81(5), 41-49.
Chan, Y. E., Huff S.L., Copeland D. G. , & Barclay D. W.
(1997) Business strategy, information systems strategy
and strategic alignment. Information Systems
Research, 8, 125–150.
Chen M. (2002) Factors affecting the adoption and
diffusion of XML and Web services standards for E-
business systems. Int. J. Human-Computer Studies 58
(2003) 259–279.
Chan, Y. E. and B. H. Reich, (2008) IT alignment: an
annotated bibliography. Journal of Information
Technology 2008. 316–396
Hatcher M. (1998) Impact of information systems on acute
care hospitals: results from a survey in the United
States. Journal of Medical Systems, 22(6), 379–387.
Haux R., Ammenwerth E., Herzog W., & Knaup P. (2002)
Health care in the information society. A prognosis for
the year 2013. International Journal of Medical
Informatics 66, 3-21.
Heinzl A. & Guttler W. (2000) IT Induced Health Care
Reconfiguration: German Hospitals in Transition.
ECIS 2000 Proceedings.
Hillestad, R., Bigelow, J., Bower, A., Girosi, F., Meili, R.,
Scoville, R. and Taylor, R. (2005). Can Electronic
Medical Record Systems Transform Health Care?
Potential Health Benefits, Savings, and Costs. Health
Affairs, 24(5), 1103-1117.
Kiang Y. M., Raghu T. S., and Shang H .K. (1999)
Marketing on the Internet — who can benefit from an
online marketing approach? Decision Support Systems,
27(2000), 383–393.
Liedtka, J. M., Formulating hospital strategy: Moving
beyond a market mentality. Health Care Management
Review, 1992(17): p. 21-26.
Lorenzi N. M., & Riley R. T. (1995) Transforming
HealthCare through Information Case Studies.
Berlin: Springer.
Luftman J. (2000) Assessing Business-IT Alignment
Maturity. Communications of the Association for
Information Systems 4(14), 1-49.
Luftman, J. N. (2007), ‘An Update on Business-IT
Alignment: “A Line” Has Been Drawn.’, MIS
Quarterly, 6 (3), 165.
Miller, S., Batenburg, R. Van den Wijngaert, L. (2006),
National Culture Influences on European ERP
Adoption. In: Jan Ljungberg & Magnus Andersson
(Eds.), Proceedings of the 14th European Conference
on Information Systems. Goteborg: Goteborg
University
OECD, (2004) The global information technology report:
Towards an equitable information society, New
York/Oxford: Oxford University Press
OECD, (2008) Information Technology Outlook 2008,
Paris: OECD
HEALTHINF 2011 - International Conference on Health Informatics
172

Pare´ G., & Sicotte C. (2001) Information technology
sophistication in health care: an instrument validation
study among Canadian hospitals. International
Journal of Medical Informatics, 63, 205-223.
RAND Corporation. (2005). Health Information
Technology: Can HIT Lower Costs and Improve
Quality? Santa Monica, California: Author.
Raymond L., Pare´ G., & Bergeron F. (1995) Matching
information technology and organizational structure:
an empirical study with implications for performance.
European Journal of Information Systems, 4, 3–16.
Rogers, E. M. (1983). Diffusion of Innovations. New
York: Free Press.
Selhofer, S, Lilischkis, S., Woerndl, M. and O’Donnell, P.
(2008). The European e-Business Report 2008 6th
Synthesis Report of the Sectoral e-Business Watch.
EU/Empirica, Brussels/Bonn.
Taylor R., Bower A., Girosi F., Bigelow J., Fonkych K., &
Hillestad R. (2005) Promoting Health Information
Technology: Is There A Case For More-Aggressive
Government Action? Health Affairs, 24(5), 1234-
1245.
Teo, T. S. H., Lin, S., & Lai, K. H. (2009). Adopters and
non-adopters of e-procurement in Singapore: An
empirical study. Omega, 37(5), 972-987.
Tornatzky L. G., and Fleischer M. (1990) The Process of
Technology Innovation. Lexington, MA: Lexington
Books
Van Everdingen, Y. M., Waarts, E. (2003): The Effect of
National Culture on the Adoption of Innovations,
Marketing Letters, Vol. 14, No. 3, pp. 217–232.
Venkatesh V., Morris M. G., Davis G. B., & Davis F. D.
(2003) User Acceptance of Information Technology:
Toward a Unified View. MIS Quarterly, 27(3), 425-
478.
Westland, J. C., & Clark, T. H. K. (2000) Global
Electronic Commerce: Theory and Case Studies.
Cambridge: MIT Press.
Zhu K., Kraemer K. L., and Xu S. (2002) A Cross-
Country Study of Electronic Business Adoption Using
the Technology-Organization-Environment
Framework International Conference on Information
Systems, 337-348.
DETERMINANTS OF IT ADOPTION IN HOSPITALS - IT Maturity Surveyed in an European Context
173
