
USER CENTERED DESIGN PROCESS OF OSAMI-D
Developing User Interfaces for a Remote Ergometer Training Application
Florian Klompmaker, Bj
¨
orn Senft, Karsten Nebe
C-Lab, University of Paderborn, F
¨
urstenallee 11, 33102 Paderborn, Germany
Clemens Busch, Detlev Willemsen
Sch
¨
uchtermann Schiller’sche Kliniken GmbH & Co KG, Ulmenallee 5-11, 49214 Bad Rothenfelde, Germany
Keywords:
Tele-medicine, Tele-monitoring, User centered design, Usability, User interfaces.
Abstract:
In this paper we present the user centered design process of the research project OSAMI-D. The project
addresses cardiac disease patients during the rehabilitation at home by offering an IT-based solution for a su-
pervised ergometer training. The user centered design process consisted of multiple user studies. We analyzed
the needs and preferences of a specific user group and developed user interfaces that are easy to operate by
them.
1 INTRODUCTION
Rehabilitation after a cardiac event is well established
and highly effective to restore health and to positively
influence possible risk factors. But some studies have
shown that these factors may deteriorate one year af-
ter an event (EUROASPIRE I and II Group, 2001),
(EUROASPIRE II Study Group, 2001). In Germany
there are so called coronary sport groups for phase III
rehabilitation following the common inhospital phase
II rehabilitation. This system is supported for one
year by the insurance companies. However only very
few patients participate on such programs. Reasons
are often a lack of availability close to home, a lack
of desire for training in a special group for cardiac
patients or scheduling conflicts (Bjarnason-Wehrens
et al., 2006). Secondary prevention can enhance risk
profiles if it is regularly conducted. An additional in-
dividual IT-based program can therefore help to close
a gap for patients willing to do exercises for their
health.
1.1 OSAMI
Many telemedical applications and devices available
these days are aimed to healthy sportsmen (e.g. the
POLAR systems
1
or athlosoft by T2BEAM
2
) or el-
1
http://www.polarusa.com
2
http://www.athlosoft.com
Figure 1: Scheme of the OSAMI-D system.
derly people during their everyday life (e.g. (Gay and
Leijdekkers, 2007), (Oppermann and Lorenz, 2008)).
There is no system available until now that addresses
cardiac patients for secondary prevention. The Ger-
man project OSAMI-D addresses remote ergometer
rehabilitation as an example of use.
OSAMI-D is a subproject of the European ITEA2
research project OSAMI (Open Source AMbient In-
telligence). It targets open source common founda-
tions for a dynamic service-oriented platform which
is able to personalize itself in large diversity of coop-
erating software intensive systems.
OSAMI-D offers rehabilitation patients an er-
gometer bicycle (see figure 2) that is controllable via
a touch screen monitor. Further on it consists of wire-
less vital data sensors (ECG, Oxygen Saturation and
Blood Pressure) that are connected via bluetooth to a
base station. This base station is connected via the
internet with a supervision centre (e.g. a heart clinic)
where the data is observed either live or by post pro-
268
Klompmaker F., Senft B., Nebe K., Busch C. and Willemsen D..
USER CENTERED DESIGN PROCESS OF OSAMI-D - Developing User Interfaces for a Remote Ergometer Training Application.
DOI: 10.5220/0003160602680273
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2011), pages 268-273
ISBN: 978-989-8425-34-8
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

Figure 2: Ergometer bicycle equipped with tablet PC (left),
ECG bluetooth sensor developed by the company Cor-
science (right top) and body sensors (right bottom).
cessing (see (Klompmaker et al., 2010) for further de-
tails). Through an intelligent event system based on
current vital parameters the patient can also exercise
offline on her own. A training report is in any case
sent to the hospital. Figure 1 shows a scheme of the
OSAMI-D system.
1.2 User Centered Design
User centered design (UCD) is an established
methodology in the software-industry that focuses on
the users of a future system and aims to create so-
lutions that fits the users needs, their requirements
and supports their tasks and goals. The usability of
products gains in importance not only for the users
of a system but also for manufacturing organizations.
According to Jokela (Jokela, 2001), the advantages
for users are far-reaching and include increased pro-
ductivity, improved quality of work, and increased
user satisfaction. Manufacturers also profit signif-
icantly through a reduction of support and training
costs (Jokela, 2001). The quality of products ranks
among the most important aspects for manufacturers
in competitive markets and the software industry is
no exception to this. One of the central quality at-
tributes for interactive systems is their usability (Be-
van, 1999) and the main standardization organizations
(IEEE 98, ISO 91) have addressed this parameter for
a long time (Granollers et al., 2002). In recent years
more and more software manufacturer consider the
usability of their products as a strategic goal due to
market pressures. Consequently, an increasing num-
ber of software manufacturer are pursuing the goal of
integrating usability practices into their software engi-
neering processes (Juristo et al., 2001), (Nebe, 2009).
Also several telemedicine applications in research and
practice apply UCD processes in order to create so-
lutions for a specific user group, e.g. (Hoogendoorn
et al., 2010).
In order to create usable solutions it is necessary
to involve users in early stages and during the pro-
cess of development. UCD adds to this by providing
different methods applicable at different stages in the
process of development. Examples include contex-
tual and behavioural analysis (in terms of interviews,
site-visits, user tests etc.) in order to gather the users
requirements, needs and habits and to know their en-
vironment.
1.3 Motivation
For OSAMI-D it is crucial that users of the system
easily understand the information that is presented.
The user interfaces informs them about current vi-
tal data, hints from the system or a remote supervi-
sor and asks them questions about their wellbeing.
A training in OSAMI-D consists of several steps like
sensor setup, trainingplan update, pre-questionnaires,
training (warm up, training phase and cool down)
and post-questionnaires. Therefore the system has to
guide the users carefully through every single step.
This takes great demands up the user interface design.
For example the use of medical and technical terms
has to be avoided and easy understandable icons have
to be designed. Text should be short and clear. The in-
formation should not scare the patients but also warn
them in the right manner. Buttons and further user in-
terface elements should make use of a clear metaphor
and produce a unique actions for the user.
Another issue that OSAMI-D addresses is to keep
up the training motivation of the heart patients. Indoor
ergometer training is often very monotonous and frus-
trating. Therefore entertainment features as well as a
regular system feedback about training success is very
important for these kind of telemedical applications.
This paper is structured as follows: In the next
chapter we will explain the prior work of the OSAMI-
D UCD process. Then we explain the user study we
performed in a clinic to evaluate the current prototype
before we describe the results. Finally we sum up and
list some future work.
2 PRIOR WORK
The project OSAMI-D follows an iterative UCD
process for designing the user interfaces. We al-
ready evaluated the user interfaces of the precur-
sor project SAPHIRE (Busch et al., 2009) which
was more technically driven and therefore had some
USER CENTERED DESIGN PROCESS OF OSAMI-D - Developing User Interfaces for a Remote Ergometer Training
Application
269
lack in user interface consistency. Using this results
we developed paper based mockups of the OSAMI-
D user interfaces and presented these to patients in
the Sch
¨
uchtermann clinic (the clinical representative
partner in the OSAMI-D project) who attended car-
diac rehabilitation at that time and which were fa-
miliar with similar hospital based systems. This user
study is described in (Klompmaker et al., 2010). It
helped us to identify several shortcomings of our ini-
tial design ideas. Taking the results as input for devel-
opment, now the first working software prototype of
the OSAMI-D system is finished. In this paper we de-
scribe a user study that was performed by six test per-
sons using this prototype. The results we present will
be used to create the final version of the prototype.
Due to law restrictions it cannot be used by real pa-
tients before a complicated certification process is ac-
complished but this is not the intention of the research
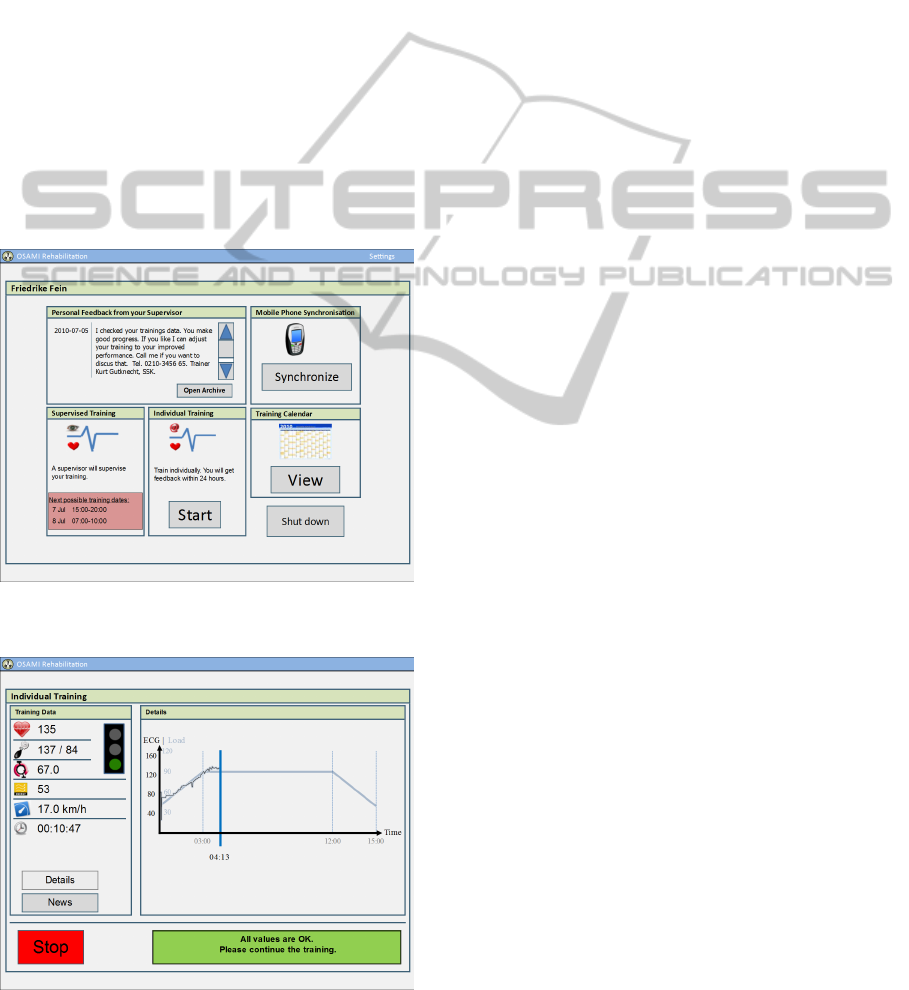
project. Figure 3 and Figure 4 show some screenshots
of the OSAMI-D user interfaces.
Figure 3: OSAMI-D Main Menu.
Figure 4: Screen during the training phase.
3 USER STUDY
As a result of previous user studies (Klompmaker
et al., 2010) it turned out that there is a motivation
barrier for patients using a system like that one devel-
oped in the project OSAMI-D. The new prototype that
has been created addressing major usability problems
resulting from previous studies but basically willing
to motivate the users during their training. Because
the whole OSAMI-D project aimed to be user centred
another final evaluation was planned. The method and
results are described below.
3.1 Method
Usability tests are a standard method in UCD to iden-
tify potential problems of a (future) system. In this
method potential users perform representative tasks
with the system in a controlled environment. Tasks
are part of a more complex user scenario. Thereby
users are observed in terms of
• what the users do
• where they succeed
• where they have difficulties with the user interface
During the course of a test the participants are asked
to vocalize her thoughts, feelings, and opinions while
interacting with the system (called ”think aloud”).
Usually a usability test is performed by at least
three persons. One that moderates the session and
gives the instructions and another one that makes the
recordings and notes while the participant performs
her tasks.
3.2 Setting
The usability test took place in a room of the
Sch
¨
uchtermann Klinik. In the room itself an er-
gometer was placed that had a 17” single-touch-PC
mounted on the handlebar and a webcam on top of
it. The functional patient interface prototype was in-
stalled on this PC. The entertainment system in this
demonstrator was limited to a news feed reader, that
could be used during the training. Even though the
prototype fulfilled not all the entertainment require-
ments resulting from the previous study, the authors
believed that it would be sufficient to testify whether
the motivation barrier could be reached. One major
problem that could not be solved beforehand was the
collection of live-data from the patients training (pa-
tient’s blood pressure, pulse and oxygen saturation ).
In order to solve this the needed vital data for the
patient interface was simulated while the ergometer
data like speed, pedaling frequency and load was real.
HEALTHINF 2011 - International Conference on Health Informatics
270

For the simulated values the so called ”wizard of oz
method” (Kelley, 1984) was used whereas a facili-
tator had access to the patient interface. Hence he
was able to generate specific data like upcoming error
messages or warnings as well as live vital data which
can be shown during the training.
As a consequence of the missing live data acquira-
tion the test team decided not to involve real patients
as participants for the test. It might have been too dan-
gerous not being able to see their live data in the train-
ing. Further on a complicated petition in the clinic
would have been needed to allow for real patients as
test persons. However, as the main reason for this
study was to reach the motivation barrier and to eval-
uate minor usability issues, it seemed to be acceptable
to take non-patients into account.
Six employees of the Sch
¨
uchtermann Klinik in the
age of 51 to 64 years have been chosen. None of them
has had any contact or involvement with the OSAMI-
D project before. Four participants were male and
two female. Therefore they represented the potential
user group quite well. Most of them are employed
as medical staff except one who was in the facility
management. Their affinity for computer is widely
distributed, but at least everyone uses a computer at
work.
As mentioned in the method section, we asked the
participants to think out loud while using the patient
interface. This helps to understand their behaviour
and to get an idea of what they are thinking. In addi-
tion to the audio signal we recorded the patient itself
using a webcam and captured the screen of the pa-
tient interface in parallel. A specific software helped
recording simultaneously i.e. the audio and video
streams. In this setting one person moderated the ses-
sion while two others handled the recordings and took
notes.
The evaluation was structured into four parts. In
the first part, the participants were being introduced.
After that a pre-interview was done in which demo-
graphic and personal data was collected. The partic-
ipants were also asked about their expectations and
knowledge of the ergometer training procedure. The
third part was the main part of the evaluation - the
usability test itself. As the subjects finished the us-
ability test, they were interviewed a last time. In this
post-interview they were asked about their impression
of the patient interface and also how they think about
this training procedure for real patients.
Each evaluation took about 30 to 45 minutes per
participant (6 to 10 minutes introduction and pre-
interview, 18 to 25 minutes for the usability test, and
6 to 10 minutes post-interview and farewell).
3.3 Results
As an overall result it turned out that most of the mi-
nor usability weaknesses have been solved properly
and that the new concept seems to be usable at all.
The implementation of news feeds was very high ac-
cepted by the participants. However, because of the
short duration of the major test it could not be clearly
examined if this entertainment feature really could be
an improvement of the monotonous training in the
long term. There are strong indices based on the user
feedback but further evaluation is needed.
Even if we did not found any serious usability
problems, there has to be done some rework in the
detail. Four major issues need to be improved:
• Trainingstart
• Switch between views in the training
• Vocabulary and icons
• Some interactions and metaphors with the touch
screen
The first issue is the trainingstart. Currently, the
training is started immediately after pressing the OK
button after the sensors have been connected success-
fully. The problem is, that not a single user realized
that the training needed to be actually started. It took
up to two minutes for some users to realize being al-
ready in the training session, which already started
(most participants needed about 30 seconds). It would
be better if a countdown - similar to computer games
- would run and the training starts not until the count-
down ran off. This is an issue that is important for
all automatic applications in the medical field that re-
quires the patient to start at a certain time.
The second issue is the switch between the views
in the training (the standard view shows the vital data
curves while the second alternative is the entertain-
ment system currently showing a news feed) . At the
moment it is realized with a button-like metaphor but
there is now visual connection between the buttons
and the view area. In this case a tab like metaphor
would make a lot more sense, even if users could fa-
miliarize with the button metaphor after a training pe-
riod.
The third issue is about the vocabulary and the
icons. In the patient interface some medical terms
were used, that are even unknown to the users, who
are employed as medical staff. An example for this
is the term ”SpO
2
” (meaning oxygen saturation). Ac-
cording to the statement of the chief of the medical
technical department, especially SpO
2
is a measure-
ment parameter that could be hard to interpret for reg-
ular patients. So it could be better to give the patient
USER CENTERED DESIGN PROCESS OF OSAMI-D - Developing User Interfaces for a Remote Ergometer Training
Application
271

less data, so that he is not overwhelmed with too dif-
ficult terms. For real applications that aims to sup-
port the patient without a supervisor this leads to the
conclusion that medical terms have to be used very
carefully in such systems.
Figure 5: The icons we used during the training: (1) pulse,
(2) blood pressure, (3) rpm, (4) load, (5) speed, (6) remain-
ing time.
Beside the vocabulary there are problems with in-
terpreting the icons, especially the icons that are dis-
played during the training (see figure 5). Only a few
icons were understood correctly by all of the users but
most need some additional information like units for
sensor data values. Especially icons for rpm (revo-
lutions per minute) and load (in watts) could not be
interpreted by most of the subjects. Figure 5 shows
the icons that are visible during the training. Some of
them have to be redesigned even though we thought
we already solved this problem by designing icons
carefully at the very beginning. Another solution to
this problem is to establish a tooltip like information
provider for single touch that provides the user with
additional information. This could be realized for ex-
ample with a long touch on an icon, that results in fad-
ing in additional information next to the icon. In the
authors work on the implications of a user interface
design for such a system (Klompmaker et al., 2010)
it was decided to use easy symbols for the vital data
and ergometer data. But according to this user evalu-
ation it was verified that the symbols are not easy to
understand. According to the problems that the users
had with the icons, they have to be used carefully in
medical applications if they are intend for patient use
only. It could be necessary to provide patients with
additional data for the icons, so they can use the sys-
tem in the most appropriate manner.
One user had also problems to interpret the mean-
ing of the remaining time. The user thought this
would be training duration. This could be due to the
fact that she did not realize that the training had al-
ready started.
The last issue concerns the interactions and
metaphors that also includes the already mentioned
view switching. Because of the use of a touch screen
some standard computer metaphors were not cor-
rectly interpreted or could not be used. For example
displaying links in blue color in the heading of the
newsfeed section was hardly be identified as a link.
It is necessary that links are marked with additional
information. Another problem is the warning at the
bottom of the screen (see figure 2). Most subjects
were close to the screen being able to read the news-
feed etc., that they recognized warnings very lately.
Warnings and hints are most important for the train-
ing so they have to be highlighted in a better way
(e.g. blinking or similar highlighting can attract at-
tention). Recognising warnings lately is a general
problem of medical applications, especially if they
are designed for elderly people. They often have a
poorer vision and need glasses while most people do
not wear glasses during their exercises. This makes it
even harder to recognize smaller items on the screen.
4 CONCLUSIONS AND FUTURE
WORK
In the presented user study the authors verified the im-
plications for a patient user interface design used for
remote training supervision. It was shown, that the
design implications lead to a demonstrator that can
be well used, although there are some minor issues
that have to be reworked. The news reader as part
of the entertainment system earned positive feedback.
Therefore such an entertainment system may help to
make ergometer training at home a better alternative
to outdoor activities. An entertainment system has
the possibility to solve motivation problems caused
by the monotonous nature of the ergometer training
but this has to be verified in the long term use. With
the user evaluation we also determined that there are
some additional implications that have to be consid-
ered in medical applications. This is for example the
emphasis of a task start where the immediately han-
dling is required. Further on icons and vocabulary
have to be chosen carefully, especially if they are criti-
cal. One interesting thing we found out, is that critical
warnings can be recognised very lately because of too
much and too small information. We conclude that
only necessary information should be used in such
patient interface and this information should be large
enough to be read also by people with a bad vision.
The entertainment system and similar additional in-
formation is not realy necessary but very useful in
this context. Therefore it should be easily available
via user interface elements that are placed marginally.
The next step in the iterative UCD process is to use
the results described in this paper as input for the fi-
nal project prototype. We currently design new icons,
rearrange and resize some user interface elements, re-
name several labels and develop additional informa-
tion available via tool tips and similar metaphors. Fur-
HEALTHINF 2011 - International Conference on Health Informatics
272

ther on the entertainment system will be improved.
Since video conferencing is another technical aspect
addressed in OSAMI-D it is possible to playback
movie files or music as well.
Another ongoing topic is the creation of user in-
terfaces for the supervisors in the clinic. They get
much live data visualized that has to be analyze in
real-time in order to identify critical situations. Last,
a mobile solution is planned where patients can exer-
cise outdoors using a mobile device. Smartphones are
able to serve as base station but they come along with
small displays that cannot be kept in view during the
training all the time. Here we have to find different
possibilities for the interaction with and for the user.
ACKNOWLEDGEMENTS
The authors would like to thank Andreas Bleiker
and the Sch
¨
uchtermann Schiller’sche Kliniken in Bad
Rothenfelde for supporting the user study presented
in this paper.
REFERENCES
Bevan, N. (1999). Quality in use: Meeting user needs for
quality. Journal of System and Software, vol. 49(1).
Bjarnason-Wehrens, B., Held, K., and Karoff, M. (2006).
Herzgruppen in deutschland status quo und perspek-
tiven. [heart groups in germany-current situation and
prospects].
Busch, C., Baumbach, C., Willemsen, D., Nee, O., Gorath,
T., Hein, A., and Scheffold, T. (2009). Supervised
training with wireless monitoring of ecg, blood pres-
sure and oxygen-saturation in cardiac patients. Jour-
nal of Telemedicine and Telecare, Vol. 15.
EUROASPIRE I and II Group (2001). Clinical reality of
coronary prevention guidelines: a comparison of eu-
roaspire i and ii in nine countries.
EUROASPIRE II Study Group (2001). Lifestyle and risk
factor management and use of drug therapies in coro-
nary patients from 15 countries. European Heart Jour-
nal.
Gay, V. and Leijdekkers, P. (2007). A health monitoring
system using smart phones and wearable sensors. In-
ternational Journal of ARM.
Granollers, T., Lors, J., and Perdrix, F. (2002). Usability
engineering process model. integration with software
engineering. In Proceedings of HCI International.
Hoogendoorn, M., Klein, M. C. A., and Mogles, N. M.
(2010). An intelligent support system for diabetic pa-
tients. In Third International Conference on Health
Informatics (HEALTHINF 2010). Springer.
Jokela, T. (2001). An assessment approach for user-centred
design processes. In Proceedings of EuroSPI.
Juristo, N., Windl, H., and Constantaine, L. (2001). Spe-
cial issue on usability engineering in software devel-
opment.
Kelley, J. F. (1984). An iterative design methodology for
user-friendly natural language office information ap-
plications. ACM Trans. Inf. Syst., 2(1):26–41.
Klompmaker, F., Nebe, K., Bleiker, A., Busch, C., and
Willemsen, D. (2010). User centered design of pa-
tient user interfaces for remote training supervision. In
Third International Conference on Health Informatics
(HEALTHINF 2010). Springer.
Nebe, K. (2009). Integration von usability engineering und
software engineering: KonformitŁts- und rahmenan-
forderungen zur bewertung und definition von soft-
wareentwicklungsprozessen. Doctoral Thesis, Shaker
Verlag, Aachen.
Oppermann, R. and Lorenz, R. (2008). Seniorengerechte
gestaltung eines dienstes zur mobilen berwachung von
gesundheitsparametern. Bundesministerium fr Bil-
dung und Forschung - BMBF-: Ambient AssistedLiv-
ing. 1. Deutscher Kongress mit Ausstellung.
USER CENTERED DESIGN PROCESS OF OSAMI-D - Developing User Interfaces for a Remote Ergometer Training
Application
273
