
iBALANCE
Hardware and Software Design for a Mobile Diagnostic Device
that Assesses Human Balance
Qian Yang, Bradford Diephuis, Virginia Chu and Katharine E. Forth
iShoe Research Team, Cambridge, U.S.A.
Keywords:
Balance, Stabilometry, Diagnostic, Mobile.
Abstract:
Balance deterioration is a major risk factor for falling, particularly among the elderly. Early detection of
emerging balance problems can allow behavioral and medical interventions to reduce the impact and sever-
ity of balance-related incidents. The iBalance technology presents a small, mobile platform that integrates
hardware and software engineering for balance monitoring at a low cost for use in the home, physical therapy
office, or other point of care setting. The hardware solution has the form factor of a bathroom scale and takes
the standard approach of a force plate with four load cells arranged in the corners beneath the platform. The
load cells output 12-bit data to a computing device running the accompanying software. There is less scien-
tific consensus about the most effective software solution for performing analysis on balance data. A survey
of the literature reveals 16 commonly used metrics of balance derived from force plate data. Using principal
component analysis, we identify three underlying clusters of metrics from which a representative metric for
each cluster may be chosen to construct an exogenous balance score. Finally, we have developed a graphical
user interface for the iBalance that allows researchers to collect raw and/or processed data and view analytic
visualizations of the data, with ease of extensibility for further research and analysis.
1 INTRODUCTION
Deterioration of balance is a common and pressing
problem for senior citizens. Injury from falls is one of
the leading causes of accidental death in adults over
85, and among adults 65 and over a hip fracture is
statistically fatal 25% of the time within 6 months of
injury. According to the Centers for Disease Control
and Prevention, the total direct cost of all fall injuries
for people 65 and older in the year 2000 exceeded $19
billion (CDCP, 2009). The high health and financial
costs associated with poor balance point to a large un-
fulfilled need for diagnostic technology that can help
prevent fall risk and detect deterioration of balance at
an early stage.
Currently, the main method of addressing this
problem has been clinical assessment followed by
physical therapy. Clinical assessments have been
largely limited to qualitative observation over short
time spans by a physician. Some commonly used
techniques include evaluative questionnaires such as
the Berg Balance Scale (Berg et al., 1992), and the
observation of quiescent standing on a foam board
where somatosensory inputs are impaired (Emery
et al., 2005).
Early diagnosis of balance deterioration enables
a host of treatment options including medication, tai
chi, physical therapy, safety equipment such as walk-
ers, and simple adjustments to the home such as rugs
and hand rails. However, a missing link in this pro-
cess is the long-term monitoring and early diagno-
sis of balance deterioration. Because the effects of
balance deterioration are subtle, it is difficult to as-
sess one’s own balance in a timely manner to take
preventative measures before a fall occurs. The in-
convenience of scheduling regular balance monitor-
ing checkups with a physical therapist in the absence
of clear physical symptoms, and the high cost of exist-
ing devices such as NeuroCom units (Chaudhry et al.,
2004) used in state-of-the-art facilities, make long-
term balance monitoring prohibitively inefficient for
most individuals.
107
Yang Q., Diephuis B., Chu V. and E. Forth K..
iBALANCE - Hardware and Software Design for a Mobile Diagnostic Device that Assesses Human Balance.
DOI: 10.5220/0003174001070114
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2011), pages 107-114
ISBN: 978-989-8425-34-8
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

Figure 1: iBalance hardware consisting of a force platform
with an USB extension chord for connection with an exter-
nal computing device. The device has dimensions of 17”
x 14” x .25” and weighs less than 10 lbs; substitution of
lighter materials for the metal casing can significantly re-
duce the weight and increase the portability of the device.
2 HARDWARE DESIGN
The iBalance is a cost-effective, portable, user-
friendly diagnostic device that can be used from the
comfort of the home or at any point of care setting.
The device consists of a durable balance platform
equipped with pressure sensors and a USB serial port
that transfers data collected from the platform onto
any USB-enabled computing device. Alternatively,
wireless bluetooth may also be used. The data from
the balance platform is collected and displayed in real
time by the computing device, which then computes
a balance diagnostic score based on a fixed interval of
data, usually between 20 and 120 seconds. The final
prototype of the device will be able to compute a sim-
ple diagnostic internally so that an external comput-
ing device will not be necessary; this is the adaptation
most suitable for home use, while in clinical applica-
tions the use of a computing device with the ability
to conduct more detailed analysis on the data may be
preferable.
2.1 Mechanical Design
The iBalance hardware consists mainly of a set of
load cells and a stable platform for the subject to
stand on. Since the basis of the iBalance software
relies on changes in the center of pressure (COP) in
the anterior-posterior and medio-lateral directions, at
least three measures of pressure are required to calcu-
late the COP in both directions. To provide the sys-
tem with redundancy and higher resolution, we use
Figure 2: Bottom view of iBalance force platform.
Figure 3: Exploding view of iBalance force platform.
four load cells placed under the corners of the plat-
form. The load cells used in our prototype are similar
to models used in bathroom scale devices.
Three designs were considered for the standing
platform: a single platform (4 load cells per platform),
a separate platform for each foot (2 load cells per plat-
form), and a separate platform for each load cell. The
different designs reflect a trade-off between platform
Figure 4: Design of load cells used in force platform.
HEALTHINF 2011 - International Conference on Health Informatics
108

stability and measurement independence. The single
platform provides the most stability, but all four pres-
sure measures become correlated by virtue of the rigid
platform, and torsion torque would not be measured.
The two-platform design, consisting of one platform
for each foot, would allow for detection of slight dor-
siflexion or plantarflexion of the ankle. However, it
would provide less stability as a platform. The single
load cell platforms provide the least platform stabil-
ity. We chose to use the single-platform design for its
stability and sufficient sensitivity to the stabilometric
properties measured by the software algorithm.
The load cell enclosures were designed to be flex-
ible, since too much rigidity would cause a portion of
the pressure to transfer directly from the platform to
the floor rather than through the load cell. The flex-
ible enclosure was constructed from laser-cut delrin
and acrylic sheets. Aluminum bars were used to pro-
vide structure to the load cell enclosures. The load
cells are rated at 75 kg each with a maximum of 150
2.2 Electronic Design
Load sensing is achieved with four off-the-shelf,
three-wire half-bridge load cells, which is the most
common configuration found in bathroom scales. The
load cells are wired in a standard Wheatstone bridge
configuration. Each load cell through its Wheatstone
bridge sends voltage values to the analog-to-digital
converter (AD7794 from Analog Devices) on differ-
ent ADC input channels. This chip performs both sig-
nal amplification and conversion. The data acquired
by the AD7794 is transmitted to an ATMega324 mi-
crocontroller over a serial peripheral interface (SPI).
The microcontroller then sends this over USB to a
computing device.
The AD7794 is a low-power analog front end for
high precision measurement applications. The out-
puts from the four Wheatstone bridges are wired to
differential input pins on the AD7794 development
board. The AD7794 amplifies the difference between
these pins, and then performs an A/D conversion.
The results of the A/D conversion are made available
to the ATMega324 microcontroller via the AD7794s
communication protocol.
An ATMega324 development board is used to in-
terface to the AD7794 development board. We used
an off-the-shelf AVR development board with an AT-
Mega324 microcontroller. This development board
includes an on-board USB chip which allows the AT-
Mega324 to easily stream data over USB. The AT-
Mega324 development board uses a USB chip from
FTDI to establish communications with a computing
device. Drivers from FTDI were installed on the com-
puting device, which makes the USB connection look
like a COM port.
The firmware for ATMega324 performs the fol-
lowing general functions: using the SPI communi-
cation protocol, the ATMega324 communicates with
the AD7794 to initiate each A/D conversion and read
back the results. It then formats the resulting data into
one channel, and streams the data out over the UART,
which goes through a USB chip and out as a USB
signal. The format of the data streamed is a repeating
cycle through the 16-bit data from each load cell, se-
rialized in clockwise order starting from the front left,
followed by a series of padded zeros.
The AD7794 is programmed to continuously con-
vert data at its maximum speed of 470 Hz. Due to
multiple overheads in transmitting the data to the host
machine, the transmission from one channel clocks in
at 300 Hz, resulting in a frequency of 75 Hz for all 4
channels.
3 SOFTWARE DESIGN
The challenge in designing the software algorithm for
the iBalance is to determine a suitable metric for reli-
ably measuring change in an individual’s balance pro-
file over time. In order to be of practical use in the
home or at the point of care, the metric used by the
iBalance must also be able to be accurately derived
from a relatively small amount of data.
Due to the complexity of the musculoskeletal and
sensory mechanisms underlying balance, it is difficult
to satisfactorily model the stability of an individual
in terms of a deterministic physical model. A vari-
ety of standard techniques used to study balance in-
stead consider the set of observations given by the
time series of an individual’s center of pressure dur-
ing quiescent stance. The resulting time series gives
rise to a large variety of metrics that may be used
to quantify a balance state (Prieto et al., 1996) (Pe-
terka, 2000). A few of the most widely studied in-
clude the peak-to-peak sway in the anterio-posterior
and medio-lateral directions, the average velocity of
the COP, and the power spectral density of the COP.
Studies have shown that there are many redundan-
cies in the full set of such metrics, from which a few
principle parameters may be extracted (Rocchi et al.,
2004). In this section we demonstrate that there are
three principle groups of metrics, from which repre-
sentative metrics may be extracted to form the basis
of a singular parameter which can be used to track the
balance profile of an individual over time.
iBALANCE - Hardware and Software Design for a Mobile Diagnostic Device that Assesses Human Balance
109
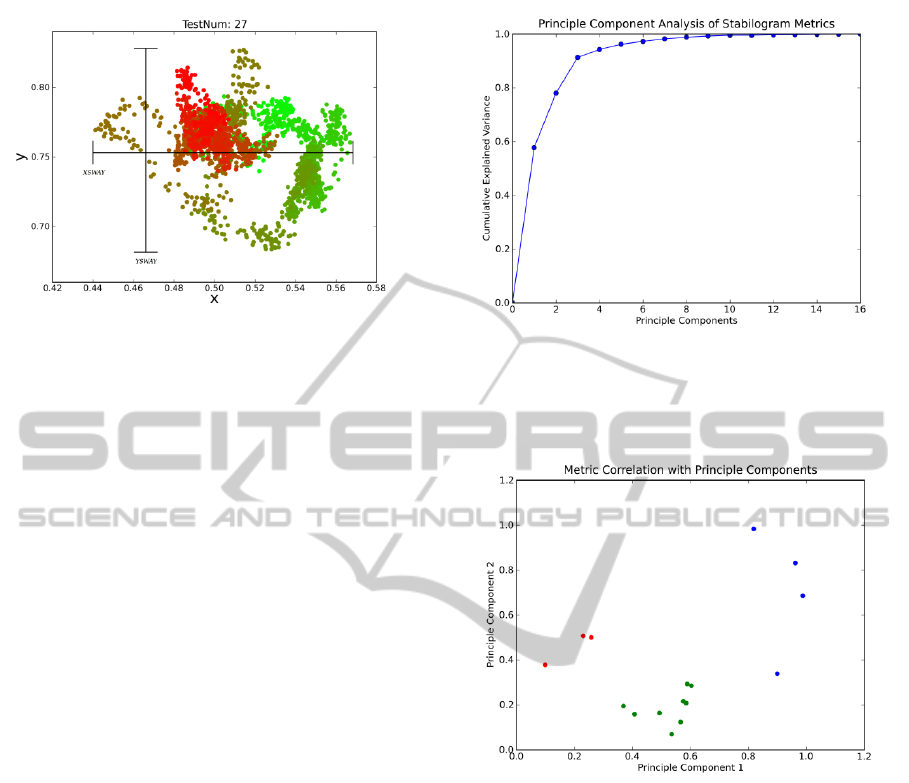
Figure 5: Sample stabilogram plot annotated with the
medio-lateral peaksway (XSWAY) and anterior-posterior
peaksway (YSWAY) metrics. The COP data time series is
plotted relative to the coordinate axis of the force platform,
with (0.5, 0.5) representing the center. The series is colored
in progression from green to red over time.
3.1 Stabilometric Properties of COP
Time Series
A large set of metrics have been reported in the liter-
ature that derive summary statistics from COP data
(Prieto et al., 1996). Researchers have conducted
Principle Component Analysis of different subsets of
these metrics in an attempt to distill a standard combi-
nation with which stabilometric data may be analyzed
(Prieto et al., 1996) (Rocchi et al., 2004).
3.2 Principal Component Analysis of
Astronaut Data
In constructing the iBalance algorithm, we are in-
terested in how to derive a signal from the various
stabilometric properties of the COP that maximally
captures variations in the observed data. We con-
ducted a principal component analysis on data from a
group of individuals in both their normal and balance-
compromised state. The particular dataset we chose
to study was astronaut data generated by NASA. The
effects of long-term exposure to zero-gravity condi-
tions on the vestibular and musculoskeletal systems
of astronauts is a heavily researched problem, and it
is widely known that astronauts experience compro-
mised balance during the first week upon their return
from space, with variations in the recovery period dif-
fering among individuals.
For our analysis, we were able to use data col-
lected from 18 NASA astronauts before launch and
after return from space using NeuroCom Interna-
tional’s dynamic posturography system. Center of
pressure data was collected from each astronaut on
Figure 6: Normalized Cumulative Eigenvectors from Prin-
ciple Component Analysis. The first three principle compo-
nents account for approximately 58%, 78%, and 91% of the
observed variation in the data.
Figure 7: Correlation coefficients of each metric with first
two principle components. The red, green, and blue data-
points correspond to Clusters 1, 2, and 3 listed in Table 1
respectively.
8 different occasions: 60, 30, and 10 days before
launch, twice on return from launch, and 2, 4, and
8 days after launch. On each day of testing, three tri-
als were performed under each of two standard Neu-
roCom protocols: SOT1 (quiescent standing, eyes
open), and SOT2 (quiescent standing, eyes closed).
The time series data collected from these trials were
20 seconds each in length, collected with a sampling
rate of 100 Hz. The COP is represented as the relative
normalized pressure in the medio-lateral and anterior-
posterior directions, with (0.5,0.5) representing per-
fectly balanced pressure in each direction.
We follow the methodology of Rocchi et al in us-
ing the correlation matrix rather than the covariance
matrix in the PCA due to the differences in parame-
ter units and variance (Jolliffe, 1986). This prevents
HEALTHINF 2011 - International Conference on Health Informatics
110

Table 1: PCA shows that stabilometric properties derived from COP time series can be clustered into several distinct groups
that correlate similarly with the observed principle components.
Cluster 1 MD average Euclidean distance of the COP from mean normalized coordinates
RMSD root mean square value of the distance of COP from mean normalized coordinates
YSWAY maximum differential of coordinates along the anterior-posterior axis
XSWAY maximum differential of coordinates along the medio-lateral axis
MAXD maximum Euclidean distance of COP from mean normalized coordinates
MV mean velocity of COP with instantaneous velocity measured at 5 Hz
RMSV root mean square value of the velocity time series
AREA-CC area of circle centered at mean COP containing 95% of the observed COP time
series, assuming Gaussian distr
AREA-CE area of ellipse centered at mean COP containing 95% of the observed COP time
series, assuming Gaussian distr
Cluster 2 MFREQ approximate rotational frequency in Hz of COP trajectory along circular path
centered at the mean with radius equal to average distance from mean
FDCC fractal dimension of COP within 95% confidence circle
FDCE fractal dimension of COP within 95% confidence ellipse
Cluster 3 P50 median frequency, in Hz given by discrete
fourier transform of COP time series
P95 frequency below which 95% of total power is found, in Hz given by discrete fourier
transform of COP time series
FREQD measure of variation in frequency content given by discrete fourier transform
of COP time series
CFREQ measure of frequency at which power spectral density is most concentrated
the resulting principal components from being domi-
nated by inherent differences in the variance of each
parameter caused by differences in units. The results
show that two principal components account for al-
most 80% of the variation in the data and three prin-
cipal components account for more than 90% of the
variation in the data. When we plot the correlation
coefficients of each metric against the first two prin-
cipal components, we see that the metrics naturally
form three distinct clusters.
The first cluster corresponds to the metrics that are
based on the length extent of the phase plot. This
refers to measures of the overall size of the space tra-
versed by the COP time series over a fixed interval of
time. From a physical standpoint, this is analagous to
measures of the maximum tilt from upright position
an individual experiences over the course of the time
series.
The second cluster corresponds to the metrics that
are based on the area of the phase plot. This refers to
measures of the total distance traversed by the COP
time series over a fixed interval of time. Whereas the
length extent of the phase plot only looks at maxi-
mum differentials between COP coordinates, the area
measures look at how the space in between was filled.
From a physical standpoint, this is analagous to un-
derstanding whether the subject was moving quickly
or slowly within the fixed interval of the observed
time series. In combination with the first cluster of
metrics, we can gain an understanding of whether
the subject was moving quickly over a small area, or
moving slowly over a large area, or some other com-
bination thereof.
The final cluster corresponds to metrics based on
the power spectrum of the phase plot. This describes
the frequency of oscillations observed in the COP
time series. From a physical standpoint, analysis of
the frequency domain may reveal underlying patterns
in the feedback-control mechanism of the body as it
attempts to maintain balance during quiescent stand-
ing, as well as any noise fluctuations caused by envi-
ronmental factors that have an effect on balance.
See Table 1 for a list of metrics that belong to each
cluster. These results show that we can use a represen-
tative metric from each of these clusters to determine
a three-dimensional descriptive balance vector. The
distance of this vector from the space of normal bal-
ance may be used as a singular metric describing the
balance profile of an individual.
3.3 Punctuated Equilibrium Model of
Human Balance
In addition to the metrics above, iShoe Research has
developed a new quantitative and descriptive model
for analyzing human balance which provides addi-
iBALANCE - Hardware and Software Design for a Mobile Diagnostic Device that Assesses Human Balance
111
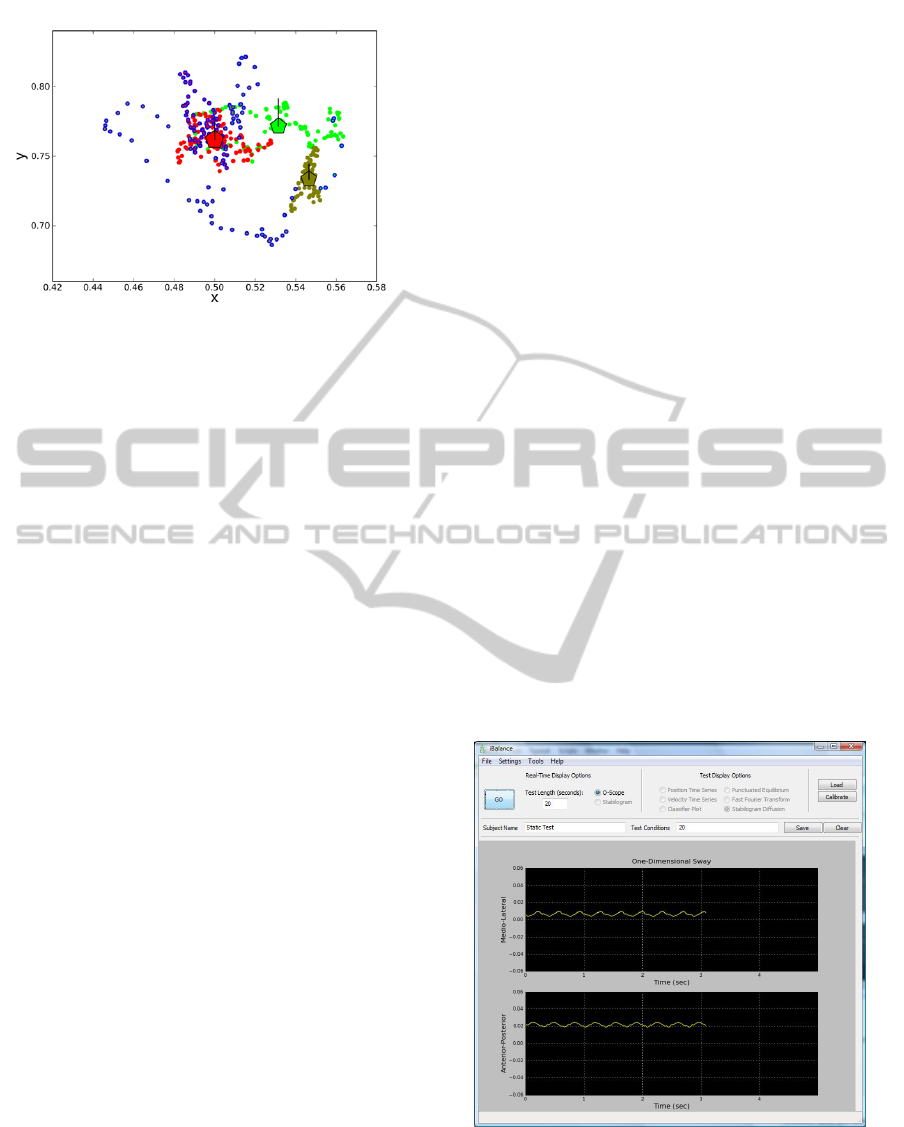
Figure 8: Stabilogram annotated with punctuated equilib-
ria. The colored regions represent different clusters of static
equilibrium, with overlayed pentagons indicating the rela-
tive size of the equilibria. The datapoints outlined in blue
and black represent dynamic trajectories between different
equilibria or returning to the same equilibria, respectively.
tional measures of an individual’s stability. The Punc-
tuated Equilibrium model captures the hypothesis that
human balance can be characterized by two states:
one of static equilibria, during which the center of
mass remains stable within a bounded region, and one
of dynamic trajectories, during which equilibrium is
lost and the center of mass attempts to readjust to a
new equilibrium. It is possible using Hidden Markov
Model analysis to capture from the observed stabilo-
gram data this underlying series of static equilibria
punctuated by dynamic trajectories.
The Punctuated Equilibrium Model provides sev-
eral quantitative measures for balance, including the
number of equilibria, the length of time spent in each
equilibrium, and the size of the bounded region for
each equilibrium. For example, analysis of the NASA
data described above shows a negative correlation be-
tween the number of equilibria and the quality of an
astronaut’s balance as represented by the number of
days since return from space. In addition to these
quantitative measures, the algorithm for Puncutated
Equilibrium is also able to provide a qualitative vi-
sual model of an individual’s balance profile. While
stabilograms are typically difficult to analyze due to
the density of datapoints collected in a bounded re-
gion over time, applying the algorithm for Punctuated
Equilibria transforms the data into regions of stability
and instability. The location and pattern of these equi-
libria and dynamic trajectories can help determine in-
formation such as whether an individual is weaker on
one leg than the other or has a tendency to lean or fall
in a particular direction.
4 GRAPHICAL USER
INTERFACE FOR BALANCE
RESEARCH
In order to facilitate the use of the iBalance as a re-
search device, we developed a basic graphical user
interface. The GUI is designed as a platform for data
collection, as well as for providing analytic visualiza-
tions of the balance data.
4.1 Real Time Data Visualization
The GUI provides two methods for visualizing data
in real-time as it is being collected from the iBalance
platform. In the Stabilogram method, we display the
real-time position of the subjects center of mass on
a two-dimensional coordinate system. The display
shows a trail of the previous second of movement,
so any shift in position from the subject is immedi-
ately visually noticeable. The Oscilloscope method
presents the same data in two simultaneous plots, dis-
playing the time series of the center of mass in the
mediolateral (ML) direction and in the anteroposte-
rior (AP) direction. This second display highlights
one-dimensional movements of the center of mass,
and permits observation of the entire data collection
sequence at any time. These real-time displays are
updated at the same refresh rate as the hardware out-
put.
Figure 9: Oscilloscope view of real-time data collection
from iBalance.
HEALTHINF 2011 - International Conference on Health Informatics
112

Figure 10: Stabilogram view of real-time data collection
from iBalance.
4.2 Static Data Visualization
After data collection is complete, we provide ad-
ditional methods for visualizing the resulting data.
These methods are intended to provide summary
statistics of the data, as well as to display the re-
sults of analysis using a variety of common as well
as novel models for human balance. The two main
models currently implemented for the GUI include
the Stabilogram-Diffusion plot described by Collins
and De Luca (Collins and De Luca, 1993), and the
Punctuated Equilibrium analysis developed by iShoe
Research. The GUI is designed to be easily extensible
to use for visualization of COP data in the context of
new models.
The existing options provide six display modes for
the collected data. The Time Series option is similar
to the real-time Stabilogram display, showing the sub-
jects center of mass on a two-dimensional coordinate
system. However, in the static display, the entire time
series of data is displayed, and color transitions are
used to denote the passage of time. The Velocity Time
Series displays the magnitude and direction of the in-
stantaneous velocity vector over the entire time series,
using the same color transitions to show evolution of
time. The Classifier Plot depicts the steps in the anal-
ysis of punctuated equilibria, which derives regions
of stability and dynamic trajectories from the instan-
taneous velocity time series of the COP data using a
Hidden Markov Model. The Punctuated Equilibrium
plot visually displays the regions of equilibria com-
puted by the HMM and the interspersed dynamic tra-
jectories. The Fast Fourier Transform plot depicts the
results of a Discrete Fourier Transform on the time se-
ries data. Finally, the Stabilogram Diffusion plot de-
picts the Stabilogram-Diffusion plot showing closed-
loop and open-loop control described by Collins and
De Luca (Collins and De Luca, 1993).
Figure 11: Stabilogram-Diffusion analysis (Collins and De
Luca, 1993) of data collected from iBalance.
4.3 Data Collection
While we provide various forms of data visualization
and provide access to our own Punctuated Equilib-
rium analysis, the primary purpose of the GUI is to
be used as a platform for data collection. The GUI
is designed to be easily extensible so that new ap-
proaches to analyzing the data can be incorporated
into the toolkit by users. To this end, we provide func-
tionality to output the raw data collected from the four
load cells into comma-separated values (CSV) files.
These are saved as raw 12-bit values. For the con-
venience of the researcher, we also write to the CSV
file the derived center of mass coordinates in the AP
and ML directions. Finally, the data files are automat-
ically annotated upon creation to allow easy indexing
of collected data.
5 CONCLUSIONS
With the high risk of falling in the senior citizen popu-
lation and the significant health and financial costs of
those falls, the benefits of preventative medicine for
balance deterioration are clear. An effective solution
iBALANCE - Hardware and Software Design for a Mobile Diagnostic Device that Assesses Human Balance
113

for long-term monitoring and early diagnosis of bal-
ance deterioration has the potential to be transforma-
tive for healthcare for senior citizens. The iBalance
technology is a cost-effective platform for which both
simple self-diagnostic algorithms as well as advanced
clinical tools have been developed, with the hope that
balance diagnostics will become as widely adopted as
blood pressure monitoring to help prevent thousands
of injuries each year. In fact, widespread use of the
iBalance device and integrated GUI also has the po-
tential to generate a wealth of data from which re-
searchers may seek to gain a greater understanding of
the variation in balance profiles between individuals
and of the long-term progression of balance profiles
in individuals.
Ongoing research for the iBalance aims to rig-
orously evaluate the accuracy and precision of the
data collected by the hardware device in various en-
vironments, as well as validate the iBalance metrics
against standard physical therapy balance measures
through a prospective study with a blinded clinical
trial. Areas for future work include refining the ana-
lytical algorithm to achieve the most valid and reliable
results with the shortest data sample to increase its
ease-of-use, as well as adapting analytical algorithms
for use with pressure-sensing insoles worn throughout
the day for continuous balance monitoring and mea-
surement of dynamic gait.
ACKNOWLEDGEMENTS
The authors would like to thank Dr. William H.
Paloski of the Neurosciences Laboratory at John-
son Space Center for generously providing data from
NASA for the study of balance metrics.
REFERENCES
Berg, K., Wood-Dauphinee, S., Williams, J., and Maki, B.
(1992). Measuring balance in the elderly: Validation
of an instrument. Canadian Journal of Public Health,
83 Suppl 2:S7–11.
CDCP (2009). Falls Among Older Adults. Centers for
Disease Control and Prevention. Retrieved April 2009
from: www.cdc.gov/HomeandRecreationalSafety/
Falls/adultfalls.html.
Chaudhry, H., Findley, T., Quigley, K., Bukiet, B., Ji, Z.,
Sims, T., and Maney, M. (2004). Measures of postu-
ral stability. Journal of Rehabilitation Research and
Development, 41(5):713–720.
Collins, J. and De Luca, C. (1993). Open-loop and closed-
loop control of posture: a random-walk analysis of
center-of-pressure trajectories. Experimental Brain
Research, 95:308–318.
Emery, C., Cassidy, J., Klassen, T. P., Rosychuk, R., and
Rowe, B. (2005). Development of a clinical static
and dynamic standing balance measurement tool ap-
propriate for use in adolescents. Physical Therapy,
85(6):502–14.
Jolliffe, I. T. (1986). Principal Component Analysis.
Springer-Verlag, New York.
Peterka, R. J. (2000). Postural control model interpretation
of stabilogram diffusion analysis. Biological Cyber-
netics, 82(4):335–343.
Prieto, T. E., Myklebust, J. B., Hoffmann, R. G., Lovett,
E. G., and Myklebust, B. M. (1996). Measures of pos-
tural steadiness: Differences between healthy young
and elderly adults. IEEE Transactions on Biomedical
Engineering, 43(9):956–966.
Rocchi, L., Chiari, L., and Cappello, A. (2004). Feature se-
lection of stabilometric parameters based on principal
component analysis. Medical and Biological Engi-
neering and Computing, 42(1):71–79.
HEALTHINF 2011 - International Conference on Health Informatics
114
