
LIVER TRANSPLANT WAITING LIST SIMULATION
An Agent based Model
Alexander Fl´avio de Oliveira
Instituto de Inform´atica, Pontif´ıcia Universidade Cat´olica de Minas Gerais, Belo Horizonte, Brazil
Ricardo Poley Martins Ferreira
Departamento de Engenharia Mecˆanica, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
Agnaldo Soares de Lima
Instituto Alfa de Gastroenterologia do Hospital das Cl´ınicas, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
Keywords:
Multi-agent systems, Agent based simulation, Simulation, Liver transplant waiting list, Queue discipline.
Abstract:
Generally, Prioritizing is not a simple task. Given a waiting list for organ transplantation with dozens of
patients, which patient must be prioritized at the time of an organ donation? Which patient has been waiting
for longer time or which patient has the worst health? What policy would be fairer and more efficient? The
search for an answer to this question can become a complex decision-making problem. The process for testing
various policies and verifying whether each one of them can bring benefits or not, can be slow and consume
valuable resources. Computer simulations can help by allowing, at a lower cost and with greater security and
flexibility, reproduction and study of events whose real occurrence would not be desirable or even possible.
These efforts result in the creation of tools for modeling and simulation. In this work, a model based on multi-
agent systems was developed and implemented by using the Repast framework. The model was calibrated by
using information taken from a real situation. Experiments were carried out illustrating situations in which the
simulation model could be used. The results demonstrated the ability of the model to capture details of reality
and to simulate defined situations.
1 INTRODUCTION
Waiting lists exist in many situations and their study
and analysis attract researchers from different areas
of knowledge. As a result of their research, models
are proposed to represent queues and their applica-
tions (Gross and Harris, 1998). However, although
useful, the mathematical models have difficulty to
capture details of the environment and to represent
qualitative aspects such as preferences and behaviors,
which are usually associated with individual charac-
teristics. Given these limits of classical queue math-
ematical models, there have been studies using ap-
proaches based on agents. Their main feature is the
fact that the focus is kept on individuals, being able to
capture details of reality (North and Macal, 2007).
Medical science has made organ transplants pos-
sible, and many lives have been saved. In Brazil,
there were more than 1,000 liver transplants in 2006,
and in 2007 more than 7,000 were waiting for a
liver transplant. Patients waiting for a donated or-
gan are organized in waiting lists. This measure,
however, raises some questions: What queue prior-
ity policy should be used? How should the waiting
list be organized? Which patients are to be priori-
tized? Who has been waiting for more time or who
has the worst clinical condition? Studies on priority
policies (Howard, 2001)(Thompson et al., 2004) seek
answers to these complex decision-making questions.
They seek to improve the system efficiency, respect-
ing medical ethics, human rights and distributive jus-
tice.
In 1997, the liver transplant waiting list was or-
ganized by order of patient registration. The objec-
tive was to inhibit frauds in an attempt to minimally
fair organize the access to the grafts (Freeman et al.,
2002). Although objective and transparent, this first-
come first-served service policy caused side effects.
462
Flávio de Oliveira A., Poley Martins Ferreira R. and Soares de Lima A..
LIVER TRANSPLANT WAITING LIST SIMULATION - An Agent based Model.
DOI: 10.5220/0003188904620468
In Proceedings of the 3rd International Conference on Agents and Artificial Intelligence (ICAART-2011), pages 462-468
ISBN: 978-989-8425-41-6
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

Knowing that in the future, their patients will need a
transplant, doctors began to enroll them early in the
waiting list, in order that, when they would need the
transplant, the patients would be in top positions of
the queue and thus they would have a greater chance
of receiving the transplant(Freeman et al., 2002). This
behavior caused a generalized queue swelling, harm-
ing those patients with urgent transplant needs who
arrived in the waiting list with lower priority than pa-
tients with better health who were already waiting.
To inhibit early enrollment, and especially to reduce
mortality on the waiting list (Oton-Nieto et al., 2005),
the first policy was changed in July 2006 in Brazil
when a health based policy was adopted. The new
policy is based on an index of severity MELD(Model
of End-Stage Liver Disease) of the patient. The pa-
tient’s MELD is calculated using a formula that takes
into consideration results obtained from three blood
tests, which measure how effectively the liver pro-
duces bile; how effectively the liver produces blood
clotting agents, and how effectively the kidneys are
functioning. The MELD score is used to estimate the
patient chances of dying within the next three months.
We proposeand implementan agent based simula-
tion model for the liver transplant waiting list (Weiss,
2000) (Sandholm, 1999). The proposed model is used
to explore, empirically, different situations and to an-
swer ”what-if” questions. The objective is to develop
a model which can help medical decision makers to
understand and to answer questions like: given an or-
gan transplant list with dozens of patients enrolled,
how to prioritize who has been waiting for a longer
time or who has the worst clinical condition? What
policy would be more fair and efficient? To choose a
priority policy is not a simple task and can become a
complex decision-making problem.
In literature simulation models to study liver
transplant waiting lists were developed (Howard,
2001)(Teng and Kong, 2008)(Thompsonet al., 2004).
Most of these models use discrete event simulation.
Teng and Kong (Teng and Kong, 2008) proposed
an agent based simulation, describing their ideas and
presenting some design decisions. Their article is
aimed to study the allocation policy of donated liv-
ers from a geographical distribution point of view tak-
ing into consideration aspects related to organ deliver
logistics and organ quality at the of transplant time.
However, the article does not presentresults and states
that the simulator had not yet been calibrated and val-
idated.
Shechter et al (Shechter et al., 2005) proposed a
biologically based discrete-event simulation that rep-
resents the biology of end-stage liver disease and
the health care organization of transplantation in the
United States. They studied changes in the allocation
policies.
Thompson et al (Thompson et al., 2004) pre-
sented a tool called LSAM (Liver Simulated Alloca-
tion Model capable of simulating different aspects of
a liver transplant waiting list as the allocation poli-
cies. They argue that the simulation-based analysis
can inform the policy process by predicting the likely
effects of alternative policies.
In (Howard, 2001), they study how the ratio be-
tween liver demand and supply affects the waiting
time. The main conclusion was that the rule of
”worst-first” is fair, but its efficiency, measured by
the loss of patient’s health decreases as the ratio of
demand-supply increases.
The outline of this paper is as follows. We first
present the liver transplant waiting list model. Then
follows a section that presents computational exper-
iments made to calibrate and test the simulator, and
to show how it can be used to deal with a transplant
waiting list. Concluding remarks appear in section 4.
2 LIVER TRANSPLANT
WAITING LIST SIMULATION
MODEL
The proposed agent-based simulation model repre-
sents each recipient patient and his or her liver dis-
ease, the donated liver and its characteristics, the
waiting list, and the interactions among them. Each
agent interacts with other agents and entities accord-
ing to specific needs and objectives (North and Macal,
2007).
To overview the model some considerations are
presented: The model reproduces the liver transplan-
tation process from the moment an organ is available
until the end of post-transplant care which can last
up to one year; The model considers as available re-
sources: medical staff, material, equipment and op-
erating room necessary for the transplant; The model
considers that a donated liver can be used for only one
patient and it considers only adult patients.
The modeled process begins when a patient is
placed on the waiting list following the MELD based
assortment policy. While the patients wait for a com-
patible liver donation, their health changes because
of their diseases. During the waiting time, a patient
can die, but still has chance of recovering his or her
liver function, showingan improvementand no longer
needing a transplant. Waiting in the transplant list,
the patient might prefer to be transferred to another
waiting list, to give up the transplant, or simply loose
LIVER TRANSPLANT WAITING LIST SIMULATION - An Agent based Model
463

contact with the transplant control center for whatever
reason. These events define the abandon list.
When a liver becomes available, there is an effort
to allocate it to a patient who meets compatibility cri-
teria, respecting his/her position in the waiting list.
Compatibility criteria consider ABO blood type, body
size of the donor and recipient, degree of medical ur-
gency and MELD score (Model for End-Stage Liver
Disease). The patient’s position in the waiting list, in
turn, will depend on the assortment discipline, which
may be first-in first-served, a random order, the worst-
first or the best-first. When a compatible patient is
found, the service is started, and the donated liver is
transplanted. After a liver transplant, the patient en-
ters post-transplant care where he or she can stay for
up to one year. During the post-transplant care, the
patient can die or a graft rejection may occur and the
patient must return to the transplant waiting list. The
model dynamic can be seen in the Figure 1.
Figure 1: Simulation model dinamics.
The model entities involved in the simulation:
• Patient: an agent that represents the recipient pa-
tient;
• Liver: an agent that represents the donated organ;
• Assortment discipline: entity that defines the
waiting list assortment policy;
• Source: an agent responsible for generate patients
and donated livers. We defined two sources types:
patient source and liver source;
• Service: an agent that represents the transplant
surgery, where the donated liver is transplanted
into the recipient patient;
• System Waiting List: an agent responsible for
controlling the entry and the exit in the waiting
list by applying an assortment discipline, and to
verify the compatibility criteria, in order to allo-
cate the donated liver to the chosen patient and to
create services;
• Transplant Follow-up: an agent responsible for
maintaining in the simulation transplanted pa-
tients and to accompany them during a period
of one year. It is also responsible for removing
from the simulation those patients who died post-
transplant and to re-apply on the waiting list those
who have problems with the graft;
• Disease: entity responsible for changes in the pa-
tient’s MELD;
• Report: entity responsible for accounting and
recording on file the simulation results and indi-
cators.
The patient agent can assume different states:
”sick”, ”sick again”, ”transplanted”,”retransplanted”,
”cured” and ”deceased”. The state in which the pa-
tient lies defines its behavior. Figure 2 shows the pa-
tient agent states and the events that trigger the tran-
sition between these states.
Figure 2: Patient’s state diagram.
As the patient agent, the liver agent can assume
different states: ”useful”, ”useless” and ”used”. Its
state defines its behavior.
The patient and the donated liver arrivals are con-
trolled by the sources already defined. When the sim-
ulation begins, the patient source populates the wait-
ing list with an initial number of patients reported by
the user. This step aims to leave the waiting list with
an initial size, defined by the situation being simu-
lated. The source creates agents according to a Pois-
son distribution, assuming a central value entered by
the user. For each created agent, the source provides,
probabilistically, valuesfor someof its attributes. Fig-
ure 3 presents the simulator class model.
Considering the basic elements that describe the
waiting list system (Gross and Harris, 1998), some
model details are given below:
• Patient arrival pattern in the waiting list is repre-
sented by a Poisson distribution;
• The server pattern: each service attends a patient,
and the service time is predetermined and equal
ICAART 2011 - 3rd International Conference on Agents and Artificial Intelligence
464

Figure 3: Simulator class diagram.
for all services;
• Discipline: discipline implemented were: worst-
first MELD based, Fist-In First-Served;
• System capacity: there is no restriction on the size
of the waiting list which is capable of receiving a
not-bounded number of patients;
• number of service channels: there is no restriction
on the amount of simultaneous services;
• Number of service stages: service (transplant) is
performed in one stage.
In this model, agents use probabilities as a basis
for controlling their behavior. The probability values
used were taken from historical database analysis and
defined by expert ad hoc decision.
The abstract class Disease represents the common
behavior of all diseases that can affect the patient. A
disease has an attribute bonus which contains a value
passed as a parameter by the user. The bonus is a
correction value that is added to the patient MELD
according to their disease, since some disease types,
such as carcinomas, compromise the patient’s health
rapidly requiring urgent transplant.
The disease types implemented by the model are:
ethanolic cirrhosis, post-viral B and C cirrhosis, cryp-
togenic cirrhosis, Hepatocellular Carcinoma and oth-
ers. These types make up represents diseases that can
lead a patient to the transplant waiting list. Generic
graft rejection is implemented as a disease which
affects transplant patients who have problems after
surgery and require a new transplant.
Each disease type is a concrete implementation of
Disease. Thus, the method getHealthTransition (), re-
sponsible for defining the evolution of the patient’s
MELD is defined in Disease, but behaves as the im-
plementation of each patient disease (polymorphism).
This design allows each disease to cause a distinct im-
pact on the patient’s MELD evolution and allows a
greater model detail.
The possibility to register as the patient’s health
changes over time, according to (Howard, 2001), is
important to better capture the dynamic nature of the
problem. However, due to the lack of information, all
the diseases modeled used the same evolution of the
MELD. During this work, no information was found
on the impact of each disease type on MELD value.
So, all diseases evolve in the same way and the value
of the patient’s MELD is increased by a random num-
ber between 0 and 1 in each time interval, each day.
System Waiting List is the agent responsible for
controling and organizing the list agents (patients and
livers), to find patients compatible with the available
organs respecting the defined discipline, and to create
the service care . The class that represents this agent
is QueueSystem.
3 COMPUTATIONAL
EXPERIMENTS
Computational experiments were made in order to
calibrate and to test the simulator, as well as to il-
lustrate how it can be used to deal with real situations
and to study the transplant waiting list. The experi-
ments described in this section were performed with
a notebook with a AMD Athlon 64 X2 QL-64 pro-
cessor and 4 GB of RAM memory. Running Win-
dows Vista H.E. 64 bits and the Java version used
was 1.6.0 17. The model was implemented using the
Repast http://repast.sourceforge.net/).
3.1 Model Calibration
The chosen calibration situation was the liver trans-
plantation waiting list of the state of S˜ao Paulo,
Brazil. The obtained data was from the 2008 cen-
sus produced by the State Health Department (Censo
2007 and 2008). This information is presented in Ta-
ble 3. The comparison among the simulation results
output data and the real situation reference data was
made.
The model agents use information and probabili-
ties to control their behavior. These parameters were
obtained from data and were calibrated:
• Probability of health improve: in this context, the
improvement consists in the liver function recov-
ery: 1,15%;
• Probability of death after transplant: 31,78%;
• Probability of re-transplant: 10%.;
• Probability of death in a three months waiting pe-
riod: depending on the patient’s MELD;
• Probability of abandon the list: 23,03%;
• Patient gender probability: 65,7% to be male;
• Patient and liver donor blood types probabilities -
Table 1;
LIVER TRANSPLANT WAITING LIST SIMULATION - An Agent based Model
465
• Patient and liver donor body sizes probabilities:
Small 30%, Medium 40%, Large 30%;
• Initial MELD index probability - Table 2;
• Patient disease type probability: Ethanolic cir-
rhosis 25,71% , Post-viral B and C cirrhosis
28,57%, Cryptogenic cirrhosis 14,29%,Hepato-
cellular Carcinoma 1,43%, Others 30%.
Table 1: Patient and liver donor Brazil blood types proba-
bilities.
Type - +
O 5,3% 42%
A 4,1% 32,2%
B 1,4% 11,1%
AB 0,4% 3,5%
The probability of death in the waiting list is not
a predefined parameter, because the death is related
to the patients MELD. To initialize the simulation the
simulated situation must be defined. The situation is
set up from input data. The data are shown in Table
3. Table 6 shows the obtained results. The ”initial
available livers” and ”special situation bonuses” re-
ceived the value 0, because these informations were
not available. Calculation methods for obtaining the
values of reference data are presented in Table 4 and
applying the formulas Reference and Input data were
obtained. Once defined the situation, the values of
the input data, the comparison indicators and the ref-
erence data, five simulations were performed and the
average of the results were compared with the refer-
ence data. To compare the results of simulation with
real data we used the defined error in the calibration
process. The error represents the relative difference
between output and the reference data. Table 6 shows
the obtained results. The error represents the relative
difference between the output data and the reference
data, and is defined by the following formula:
erro
i
= (
OutputData
i
Ref erenceData
i
− 1) × 100 (1)
Table 2: Initial MELD index probability.
MELD Probability
6 - 10 43,22%
11 - 14 32,63%
15 - 20 19,92%
21 - 30 3,81%
30 0,42%
3.2 Testing the Simulation Model
A second test was made to observe the behavior of the
simulation model using another situation. The cho-
Table 3: 2007 and 2008 waiting list census of the state of
S˜ao Paulo, Brazil.
(P)Time 01/01/2007 01/01/2008
31/12/2007 31/12/2008
(Ci) Initial size of the
waiting list 3.904 3.493
(E)Arrival patients 1.021 1.212
(I)Inscriptions 1.021 1.212
(S) Patients who left 1.439 2.132
(Tdv)Living donor transplants 95 79
(Tfe)Transp. outside the State 5 8
(Tps)Transp. inside the State 331 455
(Tsc)Transp. without
confirmation 5 3
(A)Abandon 5 10
(FHr)Liver function recovered 45 54
(NQT)Patient do not want be
transplanted 14 15
(Rid)Rem. (duplicate ) 5 2
(Rmv)Rem. MELD/PELD
( overdue 365 days) not informed 835
(Rs)Rem.(suspended 365days) 119 113
(Rpe)Rem. by the medical 44 32
(Rsc)Rem. without clinical
conditions 50 50
(Toe)Moved to another state 15 17
(O)Pre-transplant death 706 459
(Cf)FINAL RECORD 3.486 2.573
Removed(Rem.), Transplanted(Transp.).
Based on: (Censo 2007 and 2008).
sen situation was the 2007 S˜ao Paulo liver transplant
waiting list. Table 3 does not contain any informa-
tion about removedpatients from the list because their
MELD three blood tests were not made in the last 365
days. In the 2008 census, 835 patients were in this sit-
uation. This represents 17.75% of the total number of
patients. Therefore, the abandon probability used in
the validation process had to be adjusted. The input
values to the model were obtained using Table 4 for-
mula.
The data presented in Table 3 refers to an assorted
waiting list using the MELD index. Applying the
formulas presented in Table 4, we obtain the values
shown in the Table 5.
Once defined the case to be studied, the input data
values, the comparison indicators and the reference
data, five simulations were performed and the aver-
age results were compared with the real data. Re-
sults presented in the Table 6 indicates the difference
between the real situation and the simulation results.
The health improvement rate increased by 31,59% in
relation to the real situation The pre-transplant death
and the abandon rates are larger than the real rates.
But the number of patients who died in the waiting
list and the number of patients who abandoned the list
were smaller than pre-transplant deaths increase.
ICAART 2011 - 3rd International Conference on Agents and Artificial Intelligence
466

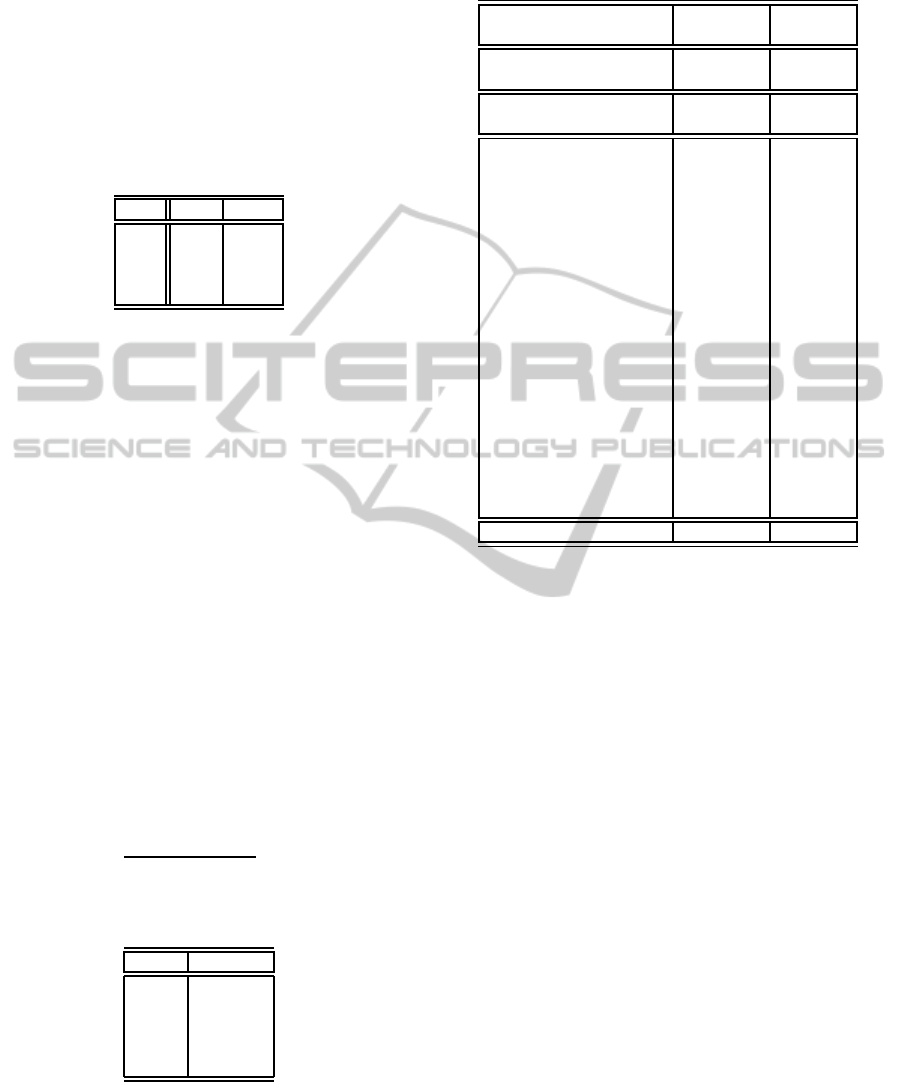
Table 6: Calibration results Simulation results versus Reference data 2008 census and Validation results Simulation results
versus Reference data 2007 census.
Result Indicator Reference Simulation error
Year Data Result
Waiting list size 4.703 4.722 0,41%
Calibration Patients per day arrival rate 3,32 3,37 1,50%
Donated livers per day arrival rate 1,46 1,46 -0,23%
∗
2008 Health improvement rate 1,15% 1,10% -4,20%
Pre-transplant death rate 9,76% 9,64% -1,27%
Abandon rate 23,03% 23,46% 1,88%
Waiting list size 4.920 4.928 0,15%
Validation Patients per day arrival rate 2,78 2,80 0,71%
Average livers arrival rate per day 1,17 1,20 2,77%
2007 Health improvement rate 0,91% 1,20% 31,59%
Pre-transplant death rate 14,35% 11,22% -21,78%
Abandon rate 5,22% 6,39% 22,42%
Table 7: Comparing WF-Meld based versus First-in First-Served disciplines.
Comparison indicator 2008 Values Simulation results
List size 4.703 4717
Number of patients with health improved 54 58
Pre-transplant number of deaths 459 428
Number of patient’s abandon 1083 1067
Discipline WF-MELD Based FIFS
Table 4: Input data equations and Reference data formulas.
Input data Formula
Number of simulated days (P)
Initial number of patients
in the waiting list (Ci)
Initial number of disponible livers -
Average patient arrival rate per day
(I)−(Rid)
(P)
Average liver arrival rate per day
(Tdv)+(T ps)
(P)
Spacial situation bonus -
Discipline Worst-First
Reference data Indicators Formula
List size (I) − (Rid) + (E)
Average patient arrival rate per day
(I)−(Rid)
(P)
Average liver arrival rate per day
(Tdv)+(T ps)
(P)
Health improvement rate
(FHr)
(Ci)+(E)
× 100
Pre-transplant death rate
(O)
(Ci)+(E)
× 100
The simulator allows the inclusion of other details.
As long as more information is available about a sit-
uation, you can represent them in the model. This
versatility allows the model gradually becomes more
complete and capable of reproducing complex situa-
tions.
With the objective of verifying what could be the
results if other waiting list assortment discipline was
used, a simulation was performed taking the 2008
scenario and changing the discipline from worst-first
MELD based to the First-In First-Served discipline
which was adopted before 2006. The simulation re-
sults presented in Table 7 suggests that the old policy
Table 5: Input data extracted from the 2007 Census and
from the 2008 Census.
Input data 2007 2008
Number of simulated days 365 365
Initial number of patients
in the waiting list 3.904 3.493
Initial number of
disponible livers 0 0
Average patient arrival
rate per day 2,78 3,32
Average liver arrival
rate per day 1,17 1,46
Spacial situation bonus 0 0
Discipline WF-MELD WF-MELD
Based Based
FIFS (First-In First-Served) was more efficient than
the new MELD based policy. According to the re-
sults, the FIFS policy provides a greater number of
patients with the improved health, a reduction in the
pre-transplant number of deaths, and in the number of
patients who abandon the list.
4 CONCLUDING REMARKS
This research is interested in the liver transplant pa-
tient waiting list organization,and considers problems
that arise from the decision-making process to define
what assortment policies to adopt.
LIVER TRANSPLANT WAITING LIST SIMULATION - An Agent based Model
467

Seeking to contribute to the study of this prob-
lem, this work developed an agent based simulation
model. The free open source framework Repast was
used. Each component of the process - the patient,
the liver, the waiting list, the transplantation, and the
sources of livers and patients were modeled as agents.
This approachallowed the characterization of the pro-
cess in detail and with a finer granularity.
The simulator was calibrated and some ex-
ploratory experiments were performed. The per-
formed experiments in this study have a demonstra-
tive nature, i.e. they were performed in order to il-
lustrate situations where the simulation model could
be used. For these experiments, comparison indica-
tors were defined and measured to compare the per-
formance of the waiting using a different waiting list
assortment discipline.
The obtained results show the expected behavior.
A more detailed interpretation of the results requires
further study. This effort, while important, goes be-
yond the scope of this paper. Theexperiments demon-
strated the ability of the model to capture details of re-
ality and to reproduce real situations. The model can
be extended, as needed, to represent more complex
situations.
ACKNOWLEDGEMENTS
This work has been supported by FAPEMIG (PPM-
00399-09), CNPQ (371756/2008-1).
REFERENCES
Freeman, R. B., Wiesner, R. H., Harper, A., McDiarmid,
S. V., Lake, J., Edwards, E., Merion, R., Wolfe, R.,
Turcotte, J., Teperman, L., UNOS/OPTN Liver Dis-
ease Severity Score, U. L., Intestine, and Commit-
tees, U. P. T. (2002). The new liver allocation system:
moving toward evidence-based transplantation policy.
Liver transplantation, 8:851–858.
Gross, D. and Harris, C. M. (1998). Fundamentals of
Queueing Theory (Wiley Series in Probability and
Statistics). Wiley-Interscience.
Howard, D. H. (2001). Dynamic analysis of liver allocation
policies. Medical Decision Making, 21(4):257–266.
North, M. J. and Macal, C. M. (2007). Managing Busi-
ness Complexity: Discovering Strategic Solutions
with Agent-Based Modeling and Simulation. Oxford
University Press, USA.
Oton-Nieto, E., Barcena-Marugan, R., Carrera-Alonso, E.,
Blesa-Radigales, C., Garcia-Gonzalez, M., J. Nuo, G.
P.-P., and Garcia-Plaza, A. (2005). Variability of meld
score during the year before liver transplantation. In
Transplantation Proceedings, volume 37, pages 3887
– 3888.
Sandholm, T. (1999). Multi-agent Systems: A Modern In-
troduction to Distributed Artificial Intelligence, chap-
ter Distributed Rational Decision Making, pages 201
– 258. MIT Press.
Shechter, S., Bryce, C., Alagoz, O., Kreke, J., Stahl, J.,
Schaefer, A., Angus, D., and Roberts, M. (2005). A
clinically based discrete-event simulation of end-stage
liver disease and the organ allocation process. Medical
Decision Making, 25(2):199–209.
Teng, Y. and Kong, N. (2008). Applying agent-based mod-
eling and simulation (abms) to the u.s. organ trans-
plantation and allocation network. In 3rd INFORMS
Workshop on Data Mining and Health Informatics
(DM-HI 2008), pages 331–338.
Thompson, D., Waisanen, L., Wolfe, R., Merion, R., Mc-
Cullough, K., and Rodgers, A. (2004). Simulating
the allocation of organs for transplantation. In Health
Care Management Science 7, pages 331–338.
Weiss, G. (2000). Multiagent Systems: A Modern Approach
to Distributed Artificial Intelligence. The MIT Press.
ICAART 2011 - 3rd International Conference on Agents and Artificial Intelligence
468
