
ROBUST FACE DETECTION IN PATIENT TRIAGE IMAGES
N
iyati Chhaya and Tim Oates
University of Maryland, Baltimore County, 1000 Hilltop Circle, Baltimore, Maryland, U.S.A.
Keywords:
Face detection, Feature extraction, Triage images.
Abstract:
Disaster events like the attack on the World Trade Center in New York City in 2001 and the earthquake in Haiti
in 2010 result in a desperate need for family and friends to obtain information about missing people. This
can be facilitated by automatically extracting textual descriptors of patients from images taken at emergency
triage centers. We show that existing face detection algorithms, a necessary precursor to extracting such
descriptors, perform poorly on triage images taken during disaster simulations, and propose and demonstrate
the superiority of an ensemble-based face detection method that is a combination of robust skin detection and
simple pattern matching face detection techniques. The addition of a template-based eye detection method
further improves the accuracy of our face detection method.
1 INTRODUCTION
Disaster events like the attack on the World Trade
Center in New York City in 2001 and the earthquake
in Haiti in 2010 have both local and non-local effects.
Locally, there is significant loss of life and property.
Non-locally, there is a desperate need for informa-
tion about the status of friends and family who might
have been directly impacted. An increasingly com-
mon practice in disaster preparedness drills, which are
required annually of hospitals in the United States,
is the use of digital cameras to take pictures of pa-
tients as they are triaged. Privacy concerns, as well
as the sometimes graphic nature of the images when
injuries are severe, makes it impractical to make the
images publicly accessible. However, descriptive fea-
tures extracted from the images – hair color and style,
clothing color and style, distinctive features like tat-
toos, gender, ethnicity, age, etc. – can be made pub-
licly available and searchable.
To extract descriptive features from triage images,
one must first locate the patient’s face. This proves to
be a difficult task given that triage images are taken
in highly variable lighting conditions from many dif-
ferent viewing angles and distances, and the patients’
faces are often obstructed with bandages, dirt, debris,
and blood. In this paper we propose a novel ensem-
ble based face detection algorithm that combines skin
detection and face detection based on pattern match-
ing that works well (in terms of precision and recall)
for our corpus of images. We also show that state-of-
the-art face detection algorithms perform poorly on
a corpus of patient triage images taken during a dis-
aster preparedness drill. Finally, we apply template
based eye detection along with the proposed face de-
tection algorithm to show how locating eyes in the
image gives better results for the resultant face detec-
tion. Figure 1 shows the overview of the proposed
ensemble based algorithm.
The remainder of the paper is organized as fol-
lows. Section 2 reviews related work for skin, face,
and eye detection. Our proposed approach is de-
scribed in Section 3. Section 4 presents our dataset
and empirical results, and Section 5 concludes and
points to future work.
2 RELATED WORK
Even in the domain of disaster response where faces
can be obstructed in a variety of ways, good skin de-
tection is essential. Probabilistic models such as (El-
gammal et al., 2009) compute the probability that a
pixel corresponds to skin given, for example, it’s RGB
values. Others approaches (Vassili et al., 2003) make
hard decisions. For example, Peer et al. (Peer et al.,
2003) declare all pixels that meet the following con-
ditions to correspond to skin:
R > 95, G > 40, B > 20
max(R, G, B) − min(R, G, B) > 15
|R− G| > 15, R > G, R > B
(1)
326
Chhaya N. and Oates T..
ROBUST FACE DETECTION IN PATIENT TRIAGE IMAGES.
DOI: 10.5220/0003319303260333
In Proceedings of the International Conference on Computer Vision Theory and Applications (VISAPP-2011), pages 326-333
ISBN: 978-989-8425-47-8
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)
!"#$%#&#'()*$
+,-$./0/1#$
3/4#0*$5/&'67*8$
9/'#$%#&#'()*$
:#1.;/&#$5/&'67*8$
<=7*$%#&#'()*$$
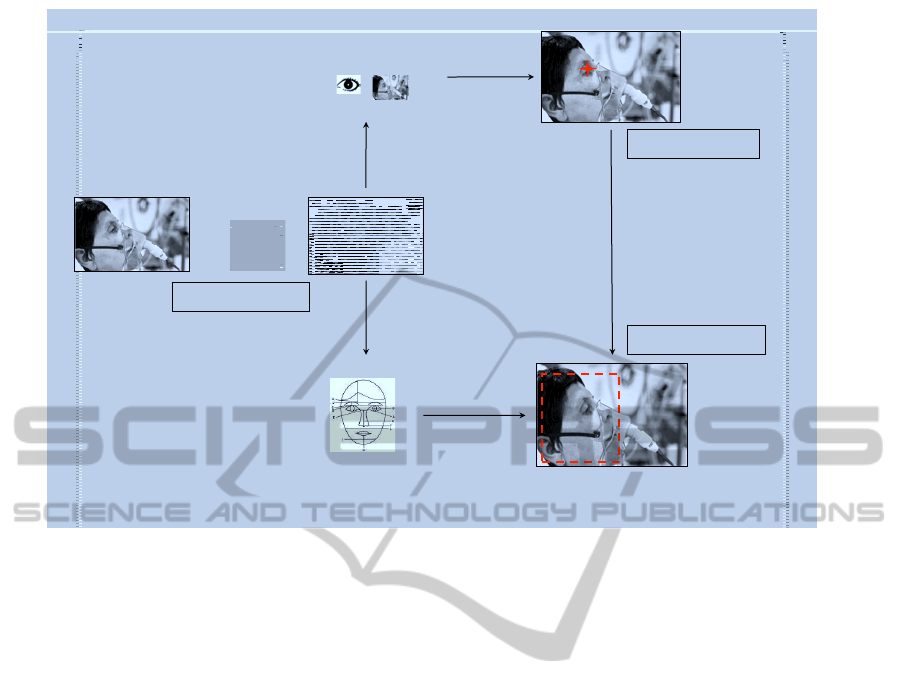
Figure 1: An overview of the processing done on each patient image for face detection.
This algorithm is a component of ours. Once relevant
pixels are found, they can be grouped into distinct re-
gions that may correspond to different body parts or
different people (Aznaveh et al., 2008; Ravichandran
and Ananthi, 2009; Phung et al., 2005).
In this work we are concerned with face region de-
tection (Yang et al., 2002) (finding contiguous regions
in an image that mostly contain faces), which is con-
trasted with face recognition (determining the identity
of a person based on an image of their face) and face
detection (marking the locations of faces, but not their
spatial extent). Some approaches use combinations of
facial features for face region localization. For exam-
ple, (Pai et al., 2006), which we incorporate in our al-
gorithm, uses the height to width ratio of the face and
the presence of eyes and a mouth. Ratios in the range
[0.75, 1.75] are acceptable, and eye and mouth loca-
tions are found using color histograms and shape fea-
tures. The baseline against which we compare our re-
sults is the Viola-Jones face detection algorithm (Vi-
ola and Jones, 2001) which uses a feature representa-
tion based on Haar wavelets and trains a discrimina-
tive model using AdaBoost (Collins et al., 2000). This
algorithm has state-of-the-art performance on com-
monly used datasets.
Many face detection algorithm can take advan-
tage of information on the location of eyes. There
are numerous approaches to eye localization, such as
the use of active IR (Peng et al., 2005) which is not
feasible for disaster events due to the requirement for
specialized equipment. Others use eye templates ex-
tracted from images either to train supervised clas-
sifiers or for matching. We incorporate a template
matching algorithm in our approach. Combination
approaches such as locally selective projection with
SVMs (Zheng and Wang, 2008), rotation invariant
Zernike moments with SVMs (Kim and Kim, 2008),
and face circle fitting with dark pixel filters (Lin and
Yang, 2004) have also been studied.
Interestingly, many of the most commonly used
datasets in face detection were originally developed
for face recognition, and thus are relatively uni-
form. For example, the FERET face dataset (Phillips
et al., 2000) contains images taken from frontal and
left/right profile views, the Yale dataset (Yal, 2006)
contains frontal images with glasses and various fa-
cial expressions, and the MIT dataset (MIT, 2000)
contains images of 10 different people taken under
different lighting conditions and poses. All of these
datasets lack diversity along a number of dimensions:
race, open vs. closed eyes, presence of facial hair, tat-
toos, etc. This is part of the reason that existing al-
gorithms, developed and tested on uniform data, per-
form poorly on images from disaster events that vary
along all of these dimensions and many others.
ROBUST FACE DETECTION IN PATIENT TRIAGE IMAGES
327

3 PROPOSED FACE DETECTION
ALGORITHM
As shown in Figure 1, the input patient image un-
dergoes a sequence of processing events. The face
detection task is treated as a combined result from
a color–based skin detector, pattern matching–based
face detector and a template matching–based eye de-
tector. The system takes an input image and cleans up
the background using skin detection, this processed
image is then fed into the face detection algorithm.
Using this combination the system needs to find the
face only within the detected skin region. To fur-
ther improve face detection accuracy, eye detection
is used. After the skin detection step, eye detection
is performed, this gives us eye coordinates. This out-
put is fed into the face detection algorithm and then
pattern matching is done with the already known eye
coordinates. The system is hence a combination of
interlocked algorithms where the feedback from eye
detection is used to improve the performance of the
face detection algorithm. Each component of this en-
semble system is explained here.
Referring back to Figure 1, first, skin detection
is done. The skin detection algorithm of Peer et
al. (Peer et al., 2003) is used, modified slightly
so that max(R, G, B) − min(R,G,B) > 10 rather than
max(R, G, B) − min(R, G, B) > 15 to allow for more
variation in ethnicity, obstruction by dirt and blood,
etc.
As mentioned, skin detection allows us to elimi-
nate the background and focus on those regions that
are most likely to contain a face, which is done with
the face detection algorithm in (Pai et al., 2006) that
uses the height to width ratio of the skin region and
the presence and location of eyes and a mouth. If any
of these features are present in the image the algo-
rithm computes a bounding rectangle around the face.
We relaxed the maximum allowed height to width ra-
tio from 1.75 to 1.8 to allow for more variation. The
eye localization algorithm uses color histograms in
the Y
′
C
B
C
R
color space. Likewise for mouth local-
ization.
For eye detection, we implemented a template-
based eye detection algorithm given that many of
the patients have their eyes closed, thus confound-
ing color-based approaches. Fifty templates were ex-
tracted from images not used in our evaluation. Some
of them are shown in Figure 2. For matching we
use two different methods and combine the results.
The first is the normalized sum of squared differ-
ences (SSD) between the template and image patches;
the second is the normalized cross correlation (NCC).
NCC is useful when lighting conditions vary, as they
do in our images. Equation 2 and Equation 3 give
expressions for SSD and NCC, respectively.
ssd(u, v) = Σ
x,y
( f (x, y) −t(x− u, y− v))
2
(2)
ncc(u, v) =
1
n− 1
Σ
x,y
( f (x, y) −
¯
f)(t(x, y) −
¯
t)
σ
f
σ
t
(3)
In the above equations, n is the number of pixels,
f is the image, t is the template, and the summation is
over positions x, y under the template at position u, v.
σ is the standard deviation.
(a) (b) (c)
Figure 2: Example eye templates.
Because patients can be, and are, in many differ-
ent orientations in our images, we rotate each eye
template and use the rotated templates as indepen-
dent templates for comparison. The rotation is done
around the center of the eye template in 30 degree in-
crements, producing twelve different templates from
each original. Other transformations, such as scal-
ing, were tested, but had little impact on the results.
Empirically, the template-based method works better
than the built-in method of (Pai et al., 2006), so to im-
prove face localization we first locate the eyes using
templates and then run the face detection algorithm.
This system being an ensemble of algorithms,
treats the face as a combination of different features
on a given skin area, whereas the Viola-Jones ap-
proach, the system is looking for a complete set of
Haar-like features that match the face. Hence, if there
is a partial face or a face with a different orientation,
our system performs considerably better than the stan-
dard face detection algorithms that are trained spe-
cially for full upright straight face images.
4 EXPERIMENTAL RESULTS
Recall that our problem domain is images of pa-
tients taken during disaster events. Much of our data
came from drills conducted by the Bethesda Hospi-
tals’ Emergency Preparedness Partnership (BHEPP),
which is a collaboration between the National Navel
Medical Center, the National Institutes of Health
Clinical Center, and the Suburban Hospital in
Bethesda, Maryland. One of the goals of BHEPP is
to develop a transportable, proven model for defining
VISAPP 2011 - International Conference on Computer Vision Theory and Applications
328

Table 1: Dataset Summary.
Source Count Remark
CMAX 22 BHEPP disaster drill
Web 6
Lost Person Finder 22 Female
Lost Person Finder 26 Male
Lost Peron Finder 21 Child
Total 97
best practices in casualty care management through
ongoing multi-agency collaboration, integration, and
training. Part of the training is an annual Collabora-
tive Multi-Agency Exercises (CMAX) drill in which a
disaster event is simulated, complete with actors play-
ing the role of disaster victims. Patients are taken to
emergency medical care centers for treatment where
they are triaged and a primary record is created, in-
cluding an image of the patient. In addition, some
of our images come from the National Institutes of
Health Lost Person Finder (LPF) project, which is a
web-based system for re-uniting family and friends
with victims during disaster events.
Figure 3 shows sample images from our dataset
and contrasts them with images often used in face de-
tection and recognition work. Note that the faces in
the BHEPP images are in different orientations, fill
different amounts of the field of view, are obstructed
by bandages and other visible signs of injury, have
open and closed eyes, are surrounded by other pa-
tients and medical personnel, etc. In contrast, images
from standard face datasets are remarkably uniform.
As we will see shortly, state-of-the art face detec-
tion algorithms perform exceptionally poorly on the
BHEPP images, necessitating a new approach. Table
1 gives a summary of the 97 images used in our ex-
periments.
We compared four different face detection ap-
proaches as described below:
• OpenCV: The state-of-the-art Viola-Jones face
detection algorithm (Viola and Jones, 2001) im-
plemented in the OpenCV toolkit
• Skin + OpenCV: Skin detection is done before
running the Viola-Jones algorithm
• Skin + FaceDetect: Skin detection is done before
running the face detection algorithm of Pai et al.
(Pai et al., 2006)
• Skin + Eye + FaceDetect: This is the same as Skin
+ FaceDetect except the template-based eye de-
tection method is used
For setting a standard testing platform, we asked
humans to manually annotate our image set for face
detection. They were asked to draw the tightest
bounding rectangle around the face region in each im-
age. Figure 4 shows examples of these annotated im-
ages. These annotations were used as reference im-
ages and results from each of the different methods
are compared against the annotated reference images.
For numerical analysis, we use precision/recall values
and the F-Score, defined as:
Precision(P) =
Annotated ∩ Program
Program
Recall(R) =
Annotated ∩ Program
Annotated
F − Score =
2 × P × R
P + R
(4)
We calculate precision and recall values by count-
ing the amount of pixel overlap between the human
annotations and the bounding boxes produced by the
algorithms. If the result from our algorithm falls com-
pletely inside the human-annotated area then we have
perfect precision and a lower recall value. If the result
from our algorithm completely contains the human-
annotated rectangle then we have perfect recall and
lower precision. And, finally, if there is no overlap
between the regions from human annotation and that
from program then precision and recall are 0. There
is no distinction between no overlap and no detection
(no rectangle marked) in the results.
4.1 OpenCV
On testing face detection using OpenCV on our im-
ages we got extreme results in most cases. Large
numbers of images had no detection of the face (pre-
cision/recall=0) whereas some images had perfect de-
tection of the face (precision/recall=1). Table 2 sum-
marizes the results. Due to OpenCV’s failure to de-
tect faces in almost 50% of the images, the average
F-Score is also low (0.47) for this algorithm.
Table 2: Results: OpenCV.
Property Number of Images
Total Images 97
No Detection 48
Perfect Detection 28
Average Recall 0.49
Average Precision 0.47
Average F-Score 0.47
The images with perfect face detection are all
frontal clean face images, very similar to those from
ROBUST FACE DETECTION IN PATIENT TRIAGE IMAGES
329

(a) Source: BHEPP (b) Source: BHEPP (c) Source: BHEPP
(d) OpenCV test image:
Lena
(e) Images from Yale face database (f) Profile test image from
CMU face database
Figure 3: Images from BHEPP disaster drills (a - c) compared to images often used in face detection and recognition work (d
- f).
(a) (b) (c)
Figure 4: Annotated Images.
Table 3: Results: Skin + OpenCV.
Property Number of Images
Total Images 97
No Detection 37
Perfect Detection 31
Average Recall 0.6
Average Precision 0.58
Average F-Score 0.59
standard face databases. As OpenCV is trained us-
ing Haar wavelets for frontal face features it fails for
anything outside that frame. Cascading of Haar fea-
tures, done as a part of the OpenCV system, also
does not improve performance for non-frontal im-
ages. Another observation is that a cluttered back-
ground greatly affects the performance of OpenCV
face detection. In some images, non-face regions
were detected as faces.
4.2 Skin + OpenCV
The performance of OpenCV showed us that chang-
ing the background distracts the algorithm. Our next
experiment involved first doing skin detection and
then continuing to run OpenCV face detection on the
images with only the skin area visible. This method
helped us eliminate background noise. As seen from
the results, the overall performance of the algorithm
improved. Also the number of no-detections went
down from 48 images in the previous experiment to
37 images in this experiment. Table 3 summarizes
these results.
4.3 FaceDetect
We first performed skin detection on all images and
then applied the pattern–matching–based face detec-
tion algorithm (FaceDetect) on the detected areas.
The results in Table 4 show that there were very
VISAPP 2011 - International Conference on Computer Vision Theory and Applications
330

Table 4: Results: Skin + FaceDetect.
Property Number of Images
Total Images 97
No Detection 7
Perfect Detection 0
Average Recall 0.66
Average Precision 0.72
Average F-Score 0.65
Table 5: Results: Skin + Eye + FaceDetect.
Property Number of Images
Total Images 97
No Detection 1
Perfect Detection 1
Average Recall 0.77
Average Precision 0.83
Average F-Score 0.78
few images with no face detection at all. Though
at the same time, the number of images with perfect
face detection is zero. The more frontal face images
give high recall values but the precision is not per-
fect. Also, we observe that most face detected re-
gions cover only part of the actual face and tend to
be towards one side of the face rather than covering
the complete face area.
4.4 Eye + FaceDetect
The results of face detection from the previous sec-
tion showed that the detected face tends to be shifted
on either side of the actual face. In this experiment,
we first implemented eye detection on detected skin
areas and then did the face detection with the eye lo-
cations known. Table 5 summarizes the results for
all images. The number of no–detections reduces to
just one. Also, the average precision/recall value is
very high as compared to that from prior results. The
increase in average F-Score shows that there is an im-
provement in precision, recall, or both.
4.5 Comparisons
In this section we compare the results of all the above
methods. Figure 5 shows results when only OpenCV
is used and when OpenCV is used after skin detec-
tion. From the graph we observe that the average per-
formance improves and the number of no-detections
also decreases.
Figure 6 shows results from both methods using
the pattern–matching–based face detection. As seen
from the graph, average performance for both of these
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
OpenCV, Skin + OpenCV
Recall
Precision
OpenCV
Average: OpenCV
Skin + OpenCV
Average: Skin + OpenCV
Figure 5: Graph: OpenCV, Skin + OpenCV – Each point
in the graph represents precision/recall value of one image
from the database.
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Skin + Facedetect, Skin + Eye + Facedetect
Recall
Precision
Skin + Facedetect
Average: Skin + Facedetect
Skin + Eye + Facedetect
Average: Skin + Eye + Facedetect
Figure 6: Graph: Skin + FaceDetect, Skin + Eye + FaceDe-
tect – Each point in the graph represents precision/recall
value of one image from the database.
methods is better than OpenCV and also that the av-
erage after Eye + FaceDetect improves as compared
to that of FaceDetect.
Table 6: Results: Average F-Score Value.
Method Avg. F-Score value
OpenCV 0.47
Skin + OpenCV 0.59
Skin + Facedetect 0.65
Skin + Eye + Facedetect 0.78
4.6 Eye Detection
Figure 8 shows the detected face area for a given im-
age using different methods. The complete rectan-
gle is the annotated reference region, the – rectangle
is from FaceDetect result and the -. rectangle shows
ROBUST FACE DETECTION IN PATIENT TRIAGE IMAGES
331
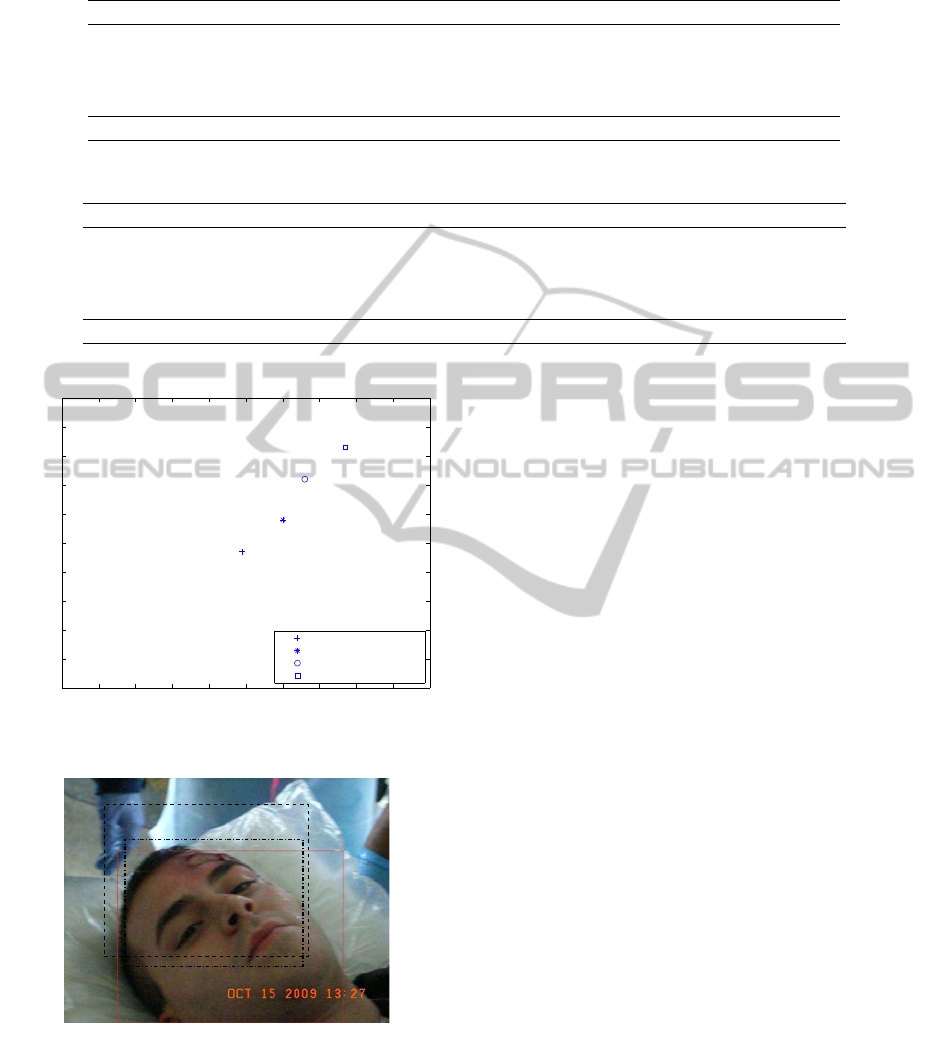
Table 7: Results: Eye Detection–Without template rotation.
Image Count Correct Detected(%) False Positives No detected Templates
Open Eyes 67 51 (76.12) 13 3 8
Closed Eyes 10 4 (40.00) 1 5 3
Half Open 15 7 (46.67) 1 7 4
Not Visible 5 0 (-) 1 0 0
All 97 62 (63.91) 16 15 15
Table 8: Results: Eye Detection–With template rotation.
Image Count Correct Detected (%) False Positives Not detected Templates
Open Eyes 67 58 (86.57) 8 1 6
Closed Eyes 10 8 (80.00) 1 1 3
Half Open 15 14 (93.33) 1 0 3
Not Visible 5 0 (-) 1 0 0
All 97 80 (82.48) 11 2 12
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Average: All methods
Recall
Precision
OpenCV
Skin + OpenCV
Skin + Facedetect
Skin + Eye + Facedetect
Figure 7: Graph: All Methods - Average.
Figure 8: Face Detection Result: — : Human annotated - -
- : Skin + FaceDetect .-: Skin + Eye + FaceDetect.
result of the Eye + FaceDetect algorithm. As seen
from the image, FaceDetect detects partial face and
FaceDetect done after eye detection detects a more
accurate face region. These results are reflected in
Figure 7 where average precision and recall from all
methods are shown. The graph shows an almost lin-
ear improvement in performance. Table 6 compares
average F-Scores from all methods. These numbers
also show improvement as the methods change. The
best performance is shown using the Skin + Eye +
FaceDetect method.
We performed an accuracy test to test the eye de-
tection algorithm by itself. The images under the
non–visible eyes section are those images where the
person is either wearing sunglasses or has a bandage
around the eye region.
Tables 7 and 8 show results of eye detection using
template matching with normal templates and using
rotated templates respectively. As observed from the
results, eye detection with template rotation performs
better than that without any rotation. The principal
reason behind this result is the presence of large num-
ber non–upright face images in the dataset.
5 CONCLUSIONS
We began with comparing standard face databases
against the dataset from real life mass disaster situ-
ation. The results from the previous section show that
an ensemble–based face detection algorithm performs
better than using off–the–shelf standard face detec-
tion algorithms. Relaxing parameters for skin detec-
tion helps in accommodating a wider range of skin
color and noise in the skin area, hence resulting in
improved performance. Performance of face detec-
tion algorithms improves drastically with elimination
of unwanted background regions. Also, the face de-
tection algorithm that we use gives better accuracy if
eye detection is done first. Template–matching–based
eye detection using a normalized sum of squared dif-
VISAPP 2011 - International Conference on Computer Vision Theory and Applications
332

ference and normalized cross correlation is effective
for this database. The key aspect of the algorithm is
rotation of templates for comparison. The rotation al-
lows accurate detection of eyes in images where the
person is lying down or not in an upright position.
Hence, we have both face to eye detection and eye
to face detection. This allows us to check the perfor-
mance of each algorithm and use the other one as a
feedback mechanism to improve performance.
We developed a mesh–like structure with the al-
gorithms, where each algorithm acts as a feedback for
the other, hence validating the performance and aid-
ing to improve performance of individual algorithms.
Our work also illustrates how algorithms meant for
standard face databases can be modified for real–life
noisy databases. We use individual unrelated methods
at each stage of detection such as color model analy-
sis for skin detection, pattern–matching for face de-
tection and template–matching for eye detection, all
of these finally coming together for an improved face
detection algorithm.
REFERENCES
2000, MIT Face Recognition Database. Online.
2006, Yale Face Database. Online.
Aznaveh, M. M., Mirzaei, H., Roshan, E., and Saraee, M.
(2008). A new color based method for skin detection
using rgb vector space.
Collins, M., Schapire, R. E., and Singer, Y. (2000). Lo-
gistic regression, adaboost and bregman distances. In
Conference on Learning Theory, pages 158–169.
Elgammal, A. M., Muang, C., and Hu, D. (2009). Skin de-
tection. In Encyclopedia of Biometrics, pages 1218–
1224. Springer US.
Kim, H.-J. and Kim, W.-Y. (April 2008). Eye detection
in facial images using zernike moments with svm.
Electronics and Telecommunications Research Insti-
tute, 30:335–338.
Lin, D.-T. and Yang, C.-M. (2004). Real-time eye detec-
tion using face-circle fitting and dark-pixel filtering.
In International Conference on Multimedia and Expo,
pages 1167–1170.
Pai, Y.-T., Ruan, S.-J., Shie, M.-C., and Liu, Y.-C. (2006). A
simple and accurate color face detection algorithm in
complex background. IEEE International Conference
on Multimedia and Expo, 0:1545–1548.
Peer, P., Kovac, J., and Solina, F. (2003). Human skin color
clustering for face detection.
Peng, K., Chen, L., Ruan, S., and Kukharev, G. (2005).
A robust and efficient algorithm for eye detection on
gray intensity face. In International Conference on
Advances in Pattern Recognition (2), pages 302–308.
Phillips, P. J., Moon, H., Rizvi, S. A., and Rauss, P. J.
(2000). The feret evaluation methodology for face-
recognition algorithms. IEEE Transactions on Pat-
tern Analysis and Machine Intelligence, 22(10):1090–
1104.
Phung, S. L., Bouzerdoum, A., and Chai, D. (2005). Skin
segmentation using color pixel classification: Anal-
ysis and comparison. IEEE Transactions on Pattern
Analysis and Machine Intelligence, 27(1):148–154.
Ravichandran, K. and Ananthi, B. (2009). Color skin
segmentation using k-means cluster. International
Journal of Computational and Applied Mathematics,
4:153–157.
Vassili, V. V., Sazonov, V., and Andreeva, A. (2003). A
survey on pixel-based skin color detection techniques.
In in Proc. Graphicon-2003, pages 85–92.
Viola, P. and Jones, M. (2001). Robust real-time object de-
tection. In International Journal of Computer Vision.
Yang, M.-H., Kriegman, D. J., and Ahuja, N. (2002). De-
tecting faces in images: A survey. IEEE Transac-
tions on Pattern Analysis and Machine Intelligence,
24(1):34–58.
Zheng, Y. and Wang, Z. (2008). Robust and precise eye
detection based on locally selective projection. In In-
ternational Conference on Pattern Recognition, pages
1–4.
ROBUST FACE DETECTION IN PATIENT TRIAGE IMAGES
333
