
aal@home: A New Home Care Wireless Biosignal
Monitoring Tool for Ambient Assisted Living
Joana Sousa
1
, Susana Palma
1
, Hugo Silva
1,2
and Hugo Gamboa
1,3
1
PLUX - Wireless Biosignals, Lisbon, Portugal
2
IT/IST - Instituto de Telecomunicac¸˜oes, Lisbon, Portugal
3
CEFITEC - FCT - Universidade Nova de Lisboa, Lisbon, Portugal
Abstract. In this article we describe a new wireless biosignal system which
monitors in a long-term basis, the users at their homes. The system consists of
wearable sensors that measure heart rate, blood oxygen saturation and physical
activity levels, sending data to a mobile phone and from this to a remote monitor-
ing station located in a clinical facility. Whenever an abnormal situation occurs,
an alarm is triggered and caregivers can provide assistance. The system has been
deployed at a major Portuguese public hospital and 30 patients under long-term
oxygen therapy have been continuously monitored remotely. The results report
that the patients feel comfortable and safe when they are continuously remote
monitored and for caregivers the system allows them to optimize their time and
give better and faster assistance.
1 Introduction
Life expectancy has been increasing in the last years. In Europe, in 1960, it was of
45.6 years old for men and 49.7 for women while in 2050, projections show that it will
increase to 79.7 and 85.1 years old for men and women, respectively. Also, a clear shift
is being witnessed from 1960 up to now regarding the proportion of elderly people (65
years and over) in the overall population [1]. According to Eurostat base scenario, in
2008 the proportion of old people in Europe (EU 27) was 17.08% (84 million), in 2020
it will be 20.06% (103 million) and in 2050 it will be 28.81% (148 million) [2,3]. As
a consequence, the old age dependency ratio in the EU 27 is rising from 25.39% in
2008 up to 50.42% in 2050 [2,3]. This situation will have an enormous economic and
social impact in a number of areas, namely in healthcare systems. The increase of the
number of elderly people will lead to an increase in the proportion of population with
physical or mental impairments, disabilities and chronic illnesses which can difficult the
accomplishment of daily life activities and consequently increase the potential need for
assistance. Faced with this problem, Europe is coming across a challenge: to develop
health and social means that allow to provide safety, comfort and good quality of life to
the older population.
At the same time, technology has also been evolving and it has now spread across
several areas such as telecommunication services, education, research and healthcare,
among others. The results obtained in Research and Development studies in the fields of
electronics, signal processing and wireless communications, have shown that we have
now technology with potential to respond to the challenge of providing tools to enhance
Sousa J., Palma S., Silva H. and Gamboa H..
aal@home: A New Home Care Wireless Biosignal Monitoring Tool for Ambient Assisted Living.
DOI: 10.5220/0003339900980107
In Proceedings of the 1st International Living Usability Lab Workshop on AAL Latest Solutions, Trends and Applications (AAL-2011), pages 98-107
ISBN: 978-989-8425-39-3
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

healthcare, safety and quality of life of the elderly and other disabled population groups.
Taking advantage of these base technologies, the Ambient Assisted Living (AAL) so-
lutions are now emerging and this is currently one of the most important research and
development areas, where accessibility, usability and learning play an important role
[4]. AAL solutions aim to apply intelligent technology in order to help people with
specific demands, such as disabled or elderly population to live independently at their
homes longer [4]. Thus, AAL has potential to improve the quality of life of elderly
people and to decrease the costs associated with this population.
Several studies have been reported in the last years, presenting solutions and tech-
nologies for AAL field. For example, Hristova et al. [5] presented a prototype system
with a number of context-aware services such as heart rate monitoring, medication
prompting, generation of agenda reminders, weather alerts and emergency notifica-
tions for ambient assisted living applications. Flynn et al. [6] have developed a wireless
biomonitor for AAL which integrated a wearable blood pressure and ECG sensors. On
the other hand, Stelios et al. [7] have developed a system capable of providing localiza-
tion data for ambient assisted living, integrating an event detection platform.
Despite the advantages of the AAL solutions, the acceptance of technology by el-
derly people still is a threat. There are some examples of the high acceptance of tech-
nology in this sector of the population, such as the usage of mobile phones, ATM ma-
chines. However, people do not accept everything that is technological possible and
available. The use and acceptance of technologies depend on adequate design, advan-
tage and practical use of the device, biographical experience of the potential user as well
as physical, mental and cognitive skills. Therefore, the main requirements of an AAL
product involve not only health, safety and independence aspects but also mobility and
social contact [1].
In this article we will describe a new system designed for home care and inde-
pendent living proposes, aiming to provide an infrastructure for continuous long term
biosignal monitoring in near real-time. The target group for using this system is com-
posed by the senior users who still have full mental capabilities and are able to have
their independence but need to have some of their physiological parameters monitored
on a long-term basis. An example of potential users are people with chronic respiratory
or cardiac problems. For example, cardiovascular disease is the most frequent cause
of death among the European population aged 65-84, both for men and women. This
includes not only ischaemic heart diseases and other heart pathologies but also cere-
brovascular diseases [8].
The rest of the paper is organized as follows: Section 2 describes the AAL system;
Section 3 presents the system validation; Section 4 details the main results and Section
5 highlights the main results.
2 aal@home
Our AAL system, aal@home, was developed aiming the continuous long term mon-
itoring of patients in their homes. The system is based on five features: (a) wearable
system; b) integration and modular system; c) wireless communication; (b) continuous
monitoring; (c) portability.
99

The aal@home system uses wireless communication in order to provide portability
and give comfort and mobility to the users. These characteristics are further enhanced
because the system is based on miniaturized and light-weight sensors that can be easily
worn by the users all day long. The real-time continuous monitoring allows the doc-
tors, nurses and orderlies to monitor in real-time the physiological parameters of each
end-user throughout day.
Monitoring different physiological parameters generally implies the use of different
devices from different brands. However, the use of several devices at the same time
is not comfortable for the user, contributing for the loss of portability and usability of
the solution. Regarding this issue, we have developed a modular system which enables
the integration of multiple parameters into a single brand system. With this design, we
improve the usability of the system and provide the caregivers with a tool that allows to
choose monitoring cardiovascular and activity parameters simultaneously or just one of
these parameters.
2.1 Overview
aal@home consists in a wearable system used for biosignal acquisition that integrates
one or two independent wireless sensor nodes, depending on the needs of the patient.
Data acquired is sent wirelessly to a mobile phone that operates as a mobile gateway,
promoting the interaction between the wireless sensor nodes and a remote monitoring
station. This monitoring station is located in a clinical facility and allows the medical
staff to monitor the status of a number of patients, at the same time. Each mobile gate-
way is associated with a number that allows the system to identify each end-user. The
mobile gateway also provides local on-screen visualization of the monitored physiolog-
ical parameters: physical activity, heart rate and oxygen saturation level. This feature
provides the user with ”self-monitor” capabilities, giving him a sense of conscience and
responsibility for the status of its health. In situations for which the mobile phone is out
of network coverage, the software on the mobile gateway is enabled with data buffering
and re-transmission capabilities.
The remote monitoring station is provided with a database containing information
about each end-user and is the point where the collected signals are stored. Through a
web interface also installed in this computer, the caregivers can monitor the physiolog-
ical parameters that are being sent by the mobile gateways. A schematic representation
of the web interface is represented by Figure 1. Furthermore, the aal@home system de-
tects anomalous situations and sends notifications and alarms to the central monitoring
station whenever the end-user has his/her physiological parameters out of the estab-
lished boundaries. This feature ensure that a fast and effective assistance is provided to
the patient whenever he needs it.
2.2 Sensors
Currently, aal@home monitors three physiological parameters: activity level, heart rate
and blood oxygen saturation. In order to accomplish these measurements, the system
integrates two kinds of sensors: a tri-axial accelerometer and a pulse oximeter.
100
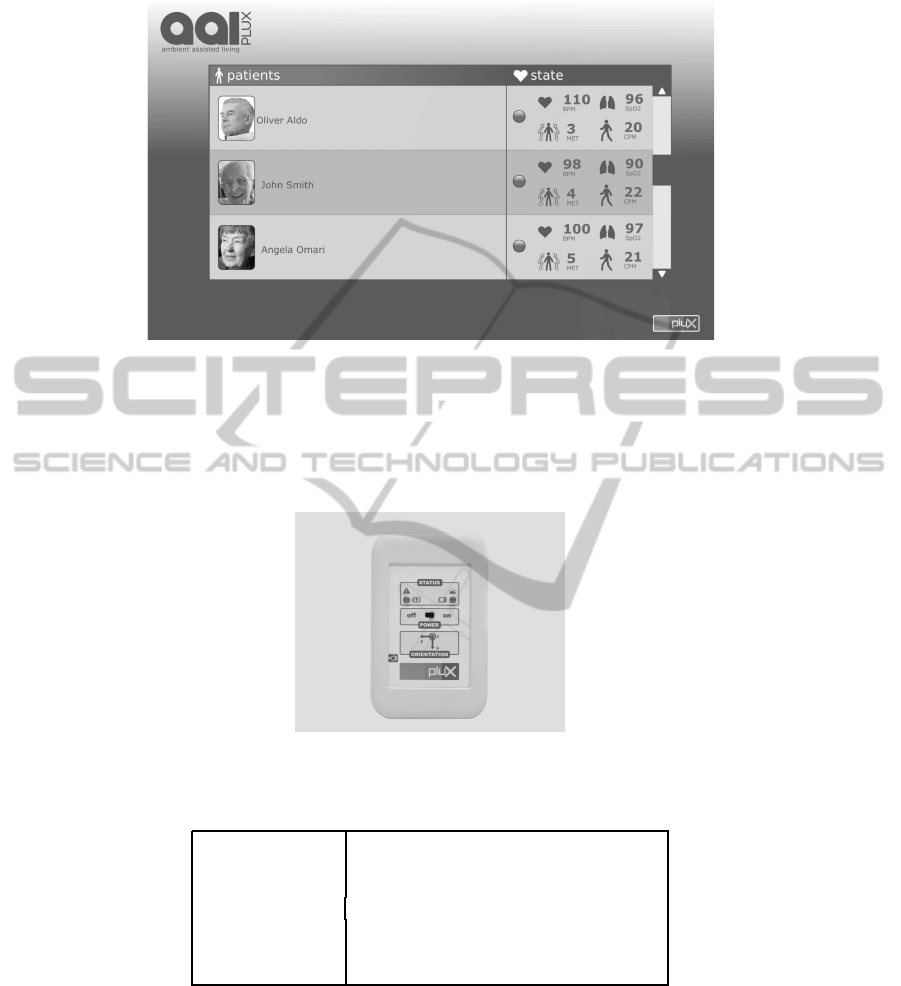
Fig.1. Schematic representation of the web interface of aal@home.
Tri-axial Accelerometer. Physical activity level is monitored throughout day by a
portable and miniaturized wireless tri-axial accelerometer placed at level the waist level,
represented by Figure 2. The technical specifications of the accelerometer are listed in
Table 1.
Fig.2. Wireless tri-axial accelerometer.
Table 1. Specifications of the accelerometer.
Connectivity Class II Bluetooth Connectivity; 10 m range
Resolution 12 bit
Sampling Rate 1000Hz
Measurement Range ± 3G
Weight 74g
Dimension 84x53x18 mm
Battery Li-On; 7.4V; 800mAh
Physical activity level is determined by correlating acceleration magnitude with the
physical activity intensity level, expressed in ”Counts” and ”MET” units. From the
acceleration magnitude, the system calculates the Counts that are the base physical ac-
tivity measurement unit. Counts are then converted into METs (”Metabolic Equivalent
101
of Task”), which is a standard unit to characterize energy expenditure in physical activ-
ities [9,10]. The conversion of Counts to MET is performed through a non-linear signal
processing algorithm. This processing algorithm correlates Counts values with MET
values using two regression equations based on the method described by Crouter et al.
[11]. This way, the physical activity level is classified according to the respective MET
value [10], as shown in Table 2.
Table 2. Activity levels classification according to MET values.
MET Value Intensity of the activity
≤ 3 Light
3 >MET ≥ 6 Moderate
MET >6 Vigorous
Pulse Oximeter. We have integrated in the aal@home system a pulse oximeter for
measuring heart rate (HR) and blood oxygen saturation (SpO2) [12], allowing to moni-
tor heart failures or vascular problems. The device, represented by Figure3 has a finger
clip pulse oximeter sensor [12] and is enabled with Bluetooth connectivity, to trans-
mit the data in real-time to the mobile phone. Currently, we have a Bluetooth finger
clip sensor under development that will be used for this purpose in the future. Table 3
presents the technical specifications of this sensor.
Fig.3. Wireless Pulse Oximeter.
Table 3. Technical specifications of the pulse oximeter.
IR Wavelength 870 nm
RED Wavelength 635
Bandwidth (-3dB) 0.5 Hz to 6 Hz
2.3 Data-Flow
In aal@home, data-flow is made in two phases: first from the sensor nodes to the mobile
gateway, and then from the mobile gateway to the remote monitoring station. Each user
has its own mobile gateway and is monitored by wireless sensor nodes, for which the
alarm thresholds are remotely configured by the practitioners at the monitoring station.
The interaction between aal@home components is shown in Figure 4.
102

Fig.4. Data-flow between aal@home components.
The raw signals are measured at 1000Hz by the accelerometer and at 200Hz by the
pulse oximeter. The data is sent in real-time and via Bluetooth RF connection to the
mobile gateway, which buffers and processes this data, showing the Counts, MET, HR
and SpO2 values continuously on-screen. From the mobile gateway, data is streamed to
the remote monitoring station by TCP/IP socket connection over cellular 3G or 802.11
WiFi network. The remote monitoring station consists of an Internet-enabled computer,
installed at the healthcare institution. A MySQL relational database management sys-
tem runs on the computer and allows the system to receive and store all incoming data
from each mobile gateway, associating that data to the corresponding patient record.
In the remote monitoring station, caregivers can access to the data through a web
interface and monitor the evolutionthroughout time of physiological parameters of each
end-user. This interface also enables the caregivers to define the regular bounds of each
physiological parameters and communicate with the end-users.
It may occur that the mobile devices are out of network coverage, causing loss
of data in the central monitoring station. In order to prevent this situation, a protocol
was developed for transactional management of the transmitted data, that together with
the buffering capabilities of the mobile gateway, avoids data loss due to lack of network
coverage or communication problems. From the remote monitoring station it is possible
to check the status of the mobile communication.
2.4 Safety
For monitoring the physiological parameters and consequently to ensure the safety of
the patients, aal@home uses a real-time communication protocol that contributes for
the enhancement of the speed and effectiveness of the assistance that is provided to
patients at their homes.
From the web interface of the remote monitoring station, caregivers can define the
physiological regular bounds for each end-user’s signals. Whenever some abnormal
situation occurs, alarms and notifications are generated in the mobile gateway and sent
to the remote monitoring station in order to inform caregivers of the users’ need of
assistance. The alarms and notifications can also be generated by the user itself by
pressing a pre-defined key on the mobile gateway. Furthermore, when caregivers detect
103

some deviations in the physiologicalparameters, they can also send a short text message
to the end-user, advising them on how to proceed, through the same communication
channel but in the inverse order: remote monitoring station → mobile gateway → end-
user.
The system is also prepared to send notifications to the central monitoring station
whenever the connection is lost, or low battery or incorrect sensor placement are de-
tected on any of the devices worn by the end-users.
Thus, the aal@home system provides a bilateral communication tool not only for
monitoring the end-users but also to provide the means to quickly and effectively detect
problems and take the necessary actions.
3 Validation
3.1 Pilot Installation
aal@home has been deployedat a major Portuguese public hospital and 30 patients have
been continuously monitored remotely by doctors. The selected evaluation group was
composed by patients with an average age of 55 years old, and suffering from Chronic
Obstructive Pulmonary Disease (COPD) under long-term oxygen therapy. These pa-
tients need periodic visits to the hospital unit on a weekly basis. The selection ofpatients
with respiratory insufficiency was based on the fact that frequent travels to the hospital
are difficult and demanding on their health, therefore, a home based long term monitor-
ing could be more beneficial. Consequently, the number of hospital visits would tend
to decrease as well as the associated costs. Also, the quality of the assessments would
improve since the patients would be monitored in a continuous basis instead of just
visiting the doctor on a weekly basis. The pilot study started on December 2009 and is
currently still ongoing.
3.2 Training
Before starting this study, all the people involved in the process, from caregivers to pa-
tients and including other agents that provide individual assistance to end-users at home
have received basic usage training with aal@home. For this purpose, a quick guide was
prepared, summarizing the most elementary information regarding the regular usage of
the devices, such as: connecting, disconnecting and charging the wireless sensor nodes
and mobile gateway, interpreting the on-screen data and SMS visualization.
Furthermore, caregivers received an initial training, focused on essential aspects
related to the system such as: features available on each device, alarm management,
device assignment and replacement procedures and charging.
4 Results and Discussion
The results obtained from the Pilot Installation are centered on the usability of the sys-
tem and the practitioners’ acceptance regarding its application in a real life scenario.
104

The results was acquired based on the observation and feedback of the patients and
caregivers.
The tests also report that the patients feel comfortable and safe when they are con-
tinuously monitored by the wearable equipments. Their independence and autonomy
are not compromised by the use of the sensors nor by the fact that they are being con-
tinuously monitored by a remote system. Also, as a result of the training program,
there were no major issues with the use of the system both by the end-users at their
homes or by the caregivers. Our support technical staff was involved in the training on
a more continuous way: they were available to help the users or caregivers whenever
they needed in order to enhance the learning process. From the caregivers’ perspective,
results show that the system is a useful tool which enables the caregivers to optimize
their time and provide better and faster assistance to the patients. Moreover, aal@home
allows caregivers and clinical practitioners to have a closer contact with the patients,
and follow them up on a much more regular basis, contributes to improve the diagnosis
process, customize, and enhance the assistance given to the patients. Moreover, since
the system can provide a greater long term communication between the clinicians and
the patients, the number of visits to the hospital decreases, improving the quality of life
of the users.
The tests show that usability is a key issue regarding the applicability of our system:
the users (both the monitored people and the practitioners at the clinics) need to be
capable of understanding all features of the equipments and be able to comfortably use
them. Only having this knowledge, the full potentialities of this remote monitoring tool
may be used. Regarding this issue, our present goal is to improve the usability of the
system so that the training step becomes more straightforward and thus takes less time
to be performed. Therefore, we are now engaged in the creation of intuitive and more
user-friendly software applications for the project, so that interpretation of the presented
data on the central monitoring station is straightforward, this way further enhancing the
caregivers’ performance. All modifications and new developments, that are being done
with this purpose, take in consideration the feedback of the patients as well as the health
specialists that are participating in the Pilot Installation.
Comparing this system with others, aal@home system presents a functional proto-
type with a portable and miniaturized sensors. The sensors are provided for being inte-
grated as wearable sensors, and so to increase the comfort of the patients. Moreover,the
system monitors at least three physiological variables, while other systems only monitor
one or two variables [6,7]. This way, aal@system takes advantage not only in terms of
usability, but also in terms of design, since it was projected as a multifunctional system.
5 Conclusions
We are facing an increase in the proportion of elderly people with respect to the overall
population. As a consequence, the demands of this fraction of the population are also
increasing and becoming more delicate towards the society. This problem is having
a strong impact on the national healthcare systems. However, technology is growing
faster and we believe that it has now the potential to create innovative tools and infras-
tructures that allow the governments and private institutions to respond to the society
105

needs. AAL is one of the most viable and promising solutions to bridge the lack of tools
for assisting and enhancing the quality of life of the elderly population.
In this article we presented a wireless and portable system for long-term monitoring
in long term physiological parameters, adapted to people who have special needs.The
system allows to monitor HR, SpO2 and activity level through wearable sensor nodes.
This feature together with wireless communication and miniaturization makes the sys-
tem comfortable for the patient and easy to carry with him/her during the normal day-
life. aal@home’s main feature is the safety tool which provides caregivers with an
easy-to-use resource to closely follow up the users at distance, this way creating the
conditions for a faster and more effective assistance to the patient in case of emergency.
Despite the fact that the system is still in pilot phase, the results so far are very
positive and demonstrate that according to the requirements, it has a good usability
and portability and is able to enhance the caregivers’ quality of work. Moreover, pa-
tients have been feeling comfortable and safe since they are continuously monitored.
For caregivers, aal@home is being a good tool for a closer monitoring process and for
customizing the assistance to each patient. Additionally, the pilot tests are showing that
the number of visits of the patients to the hospital can be decreased with aal@home.
This fact will certainly have a strong impact not only at social levels but also at eco-
nomic level because aal@home can provide a mean for decreasing the costs of the visits
as well as the number of people in the hospitals.
Acknowledgements
This work was partially supported by the National Strategic Reference Framework
(NSRF-QREN) program under contracts n 4329 and 7900 (respectively: Internation-
alization and Living Usability Lab for Next Generation Networks), and by Fundac¸˜ao
para a Ciˆencia e Tecnologia (FCT) under grant SFRG/BD/65248/2009, whose support
the authors gratefully acknowledge.
References
1. Steg, H., Strese, H., Loroff, C., Hull, J., Schmidt, S.: Europe is facing a demographic chal-
lenge Ambient Assisted Living offers solutions. IST Project Report on Ambient Assisted
Living (2006)
2. Giannakouris, K.: Ageing characterises the demographic perspectives of the european soci-
eties. Eurostat: Statistics in Focus. Retrieved 9 (2009) 08072
3. Eurostat - tables, graphs and maps interface (2010)
4. Stephanidis, C., ed.: Universal Access in Human-Computer Interaction. Ambient Interaction.
Volume 4555. Springer Berlin Heidelberg, Berlin, Heidelberg (2007)
5. Hristova, A., Bernardos, A., Casar, J.: Context-aware services for ambient assisted living: A
case-study. In: Applied Sciences on Biomedical and Communication Technologies, 2008.
ISABEL08. First International Symposium., IEEE (2008) 1–5
6. Flynn, B., Angove, P., Barton, J., Gonzalez, A., Donoghue, J., Herbert, J.: Wireless Biomon-
itor for Ambient Assisted Living. In: Oral Presentation at Conference on Signals and Elec-
tronic Systems (ICSES), Citeseer (2006)
106

7. Stelios, M., Nick, A., Effie, M., Dimitris, K., Thomopoulos, S.: An indoor localization
platform for ambient assisted living using UWB. In: Proceedings of the 6th International
Conference on Advances in Mobile Computing and Multimedia, ACM (2008) 178–182
8. Niederlaender, E.: Causes of death in the EU (2006)
9. Ainsworth, B., Haskell, W., Leon, A., Jacobs, D., Montoye, H., Sallis, J., Paffenbarger, R.:
Compendium of physical activities: classification of energy costs of human physical activi-
ties. Medicine and Science in Sports and Exercise 25 (1993) 71
10. Ainsworth, B., Haskell, W., Whitt, M., Irwin, M., Swartz, A., Strath, S., O’Brien, W., Bas-
sett Jr, D., Schmitz, K., Emplaincourt, P., et al.: Compendium of physical activities: an
update of activity codes and MET intensities. Medicine and science in sports and exercise
32 (2000) S498
11. Crouter, S., Clowers, K., Bassett Jr, D.: A novel method for using accelerometer data to
predict energy expenditure. Journal of applied physiology 100 (2006) 1324
12. Medeiros, J., Martins, R., Palma, S., Gamboa, H.: Blood Volume Pulse Peak Detector with
a Double Adaptive Threshold. In: 6 International Conference on Technology and Medical
Sciences, TMSi (2010)
107
