
HEAD TRACKING BASED AVATAR CONTROL FOR VIRTUAL
ENVIRONMENT TEAMWORK TRAINING
Stefan Marks
Department of Computer Science, The University of Auckland, Auckland, New Zealand
John A. Windsor
Department of Surgery, Faculty of Medicine and Health Sciences, The University of Auckland, Auckland, New Zealand
Burkhard W
¨
unsche
Department of Computer Science, The University of Auckland, Auckland, New Zealand
Keywords:
Virtual Environments, Head Tracking, Nonverbal Communication, Teamwork Training, Surgery.
Abstract:
Virtual environments (VE) are gaining in popularity and are increasingly used for teamwork training purposes,
e.g., for medical teams. One shortcoming of modern VEs is that nonverbal communication channels, essential
for teamwork, are not supported well. We address this issue by using an inexpensive webcam to track the user’s
head. This tracking information is used to control the head movement of the user’s avatar, thereby conveying
head gestures and adding a nonverbal communication channel. We conducted a user study investigating the
influence of head tracking based avatar control on the perceived realism of the VE and on the performance of
a surgical teamwork training scenario. Our results show that head tracking positively influences the perceived
realism of the VE and the communication, but has no major influence on the training outcome.
1 INTRODUCTION
In recent years, virtual environments (VEs) have be-
come increasingly popular due to technological ad-
vances in graphics and user interfaces (Messinger
et al., 2009). One of the many valuable uses of VEs
is teamwork training. The members of a team can
be located wherever it is most convenient for them
(e.g., at home) and solve a simulated task in the VE
collaboratively, without physically having to travel to
a common simulation facility. Medical schools have
realised this advantage and, for example, created nu-
merous medical simulations within Second Life or
similar VEs (Danforth et al., 2009).
When looking at teamwork, communication is a
vital aspect. An ideal VE would therefore facilitate all
communication channels that exist in reality – verbal
as well as non-verbal. Due to technical limitations,
this is not possible, and therefore, existing commu-
nication in VEs is currently mostly limited to voice.
Other channels like text chat, avatar body gestures,
facial expressions have to be controlled manually and
thus do not reflect the real-time communicative be-
haviour of the user.
Analysis of communication in medical teamwork
has shown that nonverbal communication cues like
gesture, touch, body position, and gaze are equally
important to verbal communication in the analysis of
the team interactions (Cartmill et al., 2007). VEs that
do not consider those nonverbal channels are likely to
render the communication among the team members
less efficient than it would be in reality.
We propose an inexpensive extension of a VE by
camera-based head tracking to increase the “commu-
nication bandwidth”.
Head tracking measures the position and the ori-
entation of the user’s head relative to the camera and
the screen. The rotational tracking information can be
used to control the head rotation of the user’s avatar.
That way, other users in the VE can see rotational
head movement identical to the movement actually
performed physically by the user, like nodding, shak-
ing, or rolling of the head.
The translational tracking information can be
used to control the view “into” the VE. This so called
(HCP) enables intuitive control, like peeking around
corners by moving sideways, or zooming in by simply
moving closer to the monitor. The use of head track-
257
Marks S., A. Windsor J. and Wünsche B..
HEAD TRACKING BASED AVATAR CONTROL FOR VIRTUAL ENVIRONMENT TEAMWORK TRAINING.
DOI: 10.5220/0003364702570269
In Proceedings of the International Conference on Computer Graphics Theory and Applications (GRAPP-2011), pages 257-269
ISBN: 978-989-8425-45-4
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

ing information has therefore the potential to simplify
the usage of a VE by replacing non-intuitive manual
view control by intuitive motion-based view control.
Especially in medical applications, this has the poten-
tial to free the hands of the user, enabling the use of
other simulated instruments or tools, e.g., an endo-
scope.
This paper presents the results of an experimental
study designed to measure any influence that the in-
troduction of head tracking has on teamwork commu-
nication, teamwork efficiency, and perceived realism
of the VE.
2 RELATED WORK
The reproduction of nonverbal communication in vir-
tual environments is an ongoing research topic that
benefits from technological advancement. In the early
stages, data was captured by using magnetic track-
ing sensors, facial markers, data gloves, etc. (see,
e.g.,(Ohya et al., 1993)). With the development of
better hardware and advanced tracking algorithms, it
became possible to use only one camera instead of
multiple systems.
(Cordea et al., 2002) track the head of the user
with a camera to extract the rotational information.
This can easily and efficiently be transmitted during a
video call to simulate the head movement of the user’s
avatar on the receiver’s side. However, the focus of
this paper is more on information reduction than on
virtual environments.
(Wang et al., 2006) use only the 2-dimensional po-
sition of the face within the camera image to control
the 2D-movement of a game character.
This idea is extended into the 3
rd
dimension by
(Yim et al., 2008), where a head-mounted LED line
is used to track the position and rotation of the user’s
head. This information is used again to control a game
instead of an avatar.
Using only a single camera, (Sko and Gardner,
2009) present a range of interaction techniques based
on 3-dimensional translation and rotation tracking
data. A predefined set of head gestures is recognized
and associated with certain actions in a game. Slightly
tilting the head sideways is used for peering around a
corner. Leaning forwards is interpreted as zooming.
Head rotation is used for a slight change in the view
direction, whereas head translation is used for HCP.
These techniques focus on a single user, but the au-
thors have not extended their research on the possibil-
ities for multi-user scenarios.
In a recent study, (Marks et al., 2010) found that
users can clearly perceive head motions, facial ex-
pressions, and mouth movement of avatars, and that
camera-based HCP is more natural and intuitive to use
than manual view control.
3 QUESTIONS
AND HYPOTHESES
In this paper, we are going to validate the following
hypotheses:
H1 When head tracking is enabled, the participants
demonstrate more overall head movement than
when head tracking is disabled.
H2 When head tracking is enabled, the amount of
head movement is greater when participants talk
to each other compared to when head tracking is
disabled.
H3 When head tracking is enabled, the participants
perceive the other avatars as more natural than
when head tracking is disabled.
H4 When head tracking is enabled, the participants
perceive the communication with the other partic-
ipants as more natural than when head tracking is
disabled.
H5 When head tracking is enabled, the participants
look more at each other’s avatars than when head
tracking is disabled.
H6 When head tracking is enabled, the participants
solve the teamwork task better than when head
tracking is disabled.
4 DESIGN
The following factors were involved in the design of
the study:
• The number of participants was limited to three
due to the amount of available game engine li-
censes.
• It should be impossible or at least infeasible for
only one or two participants to solve the scenario
efficiently and instead require the effective team-
work of all three users involved.
• To facilitate comparison of the results, the sce-
nario should be of equal length when repeated.
• To avoid too much of a learning curve effect, the
scenario should vary at least in parts.
GRAPP 2011 - International Conference on Computer Graphics Theory and Applications
258
4.1 Overview
We chose a simplified surgical procedure for the sim-
ulation scenario. It involves three participants: a sur-
geon, an anaesthesiologist, and a nurse. Each of these
three roles has very clear and defined tasks:
• The surgeon performs the necessary steps of the
surgical operation on the patient.
• The anaesthesiologist monitors the patient’s vi-
tal signs and stabilises the patient when critical
events occur.
• The nurse is responsible for supplying the surgeon
and the anaesthesiologist with the correct instru-
ment respectively medication.
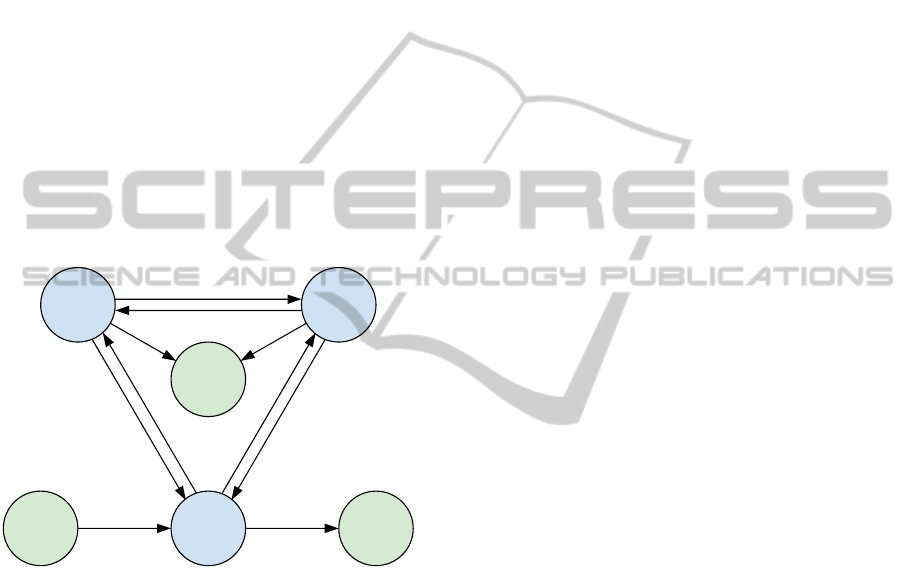
This clear definition of the roles and tasks together
with the necessary interactions is depicted in Figure 1.
Every role has to communicate with every other role
throughout the scenario. Ineffective communication
would inevitably lead to an ineffective teamwork.
request status update
inform/interrupt
o
p
e
r
a
t
e
o
p
e
r
a
t
e
m
o
n
i
t
o
r
/
s
t
a
b
i
l
i
s
e
o
p
e
r
a
t
e
r
e
q
u
e
s
t
/
r
e
t
u
r
n
i
n
s
t
r
u
m
e
n
t
g
i
v
e
/
r
e
c
e
i
v
e
i
n
s
t
r
u
m
e
n
t
r
e
q
u
e
s
t
d
r
u
g
g
i
v
e
d
r
u
g
Drug/
Instrument
Trays
Disposal
Bin
take drug/
instrument
dispose of
instrument
Anaesthesi-
ologist
Patient
Nurse
Surgeon
Figure 1: Diagram of the relations and interactions between
the three roles and the patient.
For measuring the effectiveness of the teamwork
of a group of participants, we used the following two
metrics:
• The total time from the beginning of the first step
of the surgical procedure until the completion of
the last step.
• The relative amount of time that the patient’s vi-
tal signs are critical (e.g., blood pressure too low,
heart rate too high).
For each group of three participants, we con-
ducted six experiments, rotating the roles and dis-
abling/enabling the head tracking so that no partic-
ipant would have the same role in two successive
experiments, and every participant would experience
each role with head tracking disabled and enabled.
4.2 Surgical Procedure
The selection of the nature of the simulated surgical
procedure was mainly based on the abilities of the
game engine we used for creating the VE, a modi-
fied version of the Source Engine (Valve Corporation,
2004).
In general, larger objects can be handled more eas-
ily in this VE than small objects. Therefore, we chose
the relatively large torso of the patient as the operat-
ing field, as opposed to the leg or other extremities.
This allowed us to design relatively large instruments
that would cause less problems for the participants to
move and position.
For the same reason, we chose to design a rather
large incision along the middle of the upper body, re-
vealing organs of the digestive system like stomach,
liver, pancreas, small intestines, and colon.
Located in the centre of this incision are the stom-
ach and the pancreas. After consultation with staff of
the surgical department, we decided on the removal of
dead and infected tissue from the pancreas of the pa-
tient as the surgical procedure to simulate. In medical
terms, this procedure is called pancreatic necrosec-
tomy.
4.3 Role Description
The positions of the three roles involved in the surgi-
cal procedure and the layout of the room can be seen
in Figure 2.
4.3.1 Surgeon
The surgeon operates on the right side of the patient.
The task of the surgeon is to apply the right instru-
ments in the right order to the patient to complete the
procedure step by step.
The steps of the simulated surgical procedure are
visualised in Figure 3. To get from one step to the
next, the indicated instrument has to be used. The
surgeon uses the instrument on the patient by touching
the operating field with it.
When the instrument is the correct one for the
task, it starts to blink blue and a progress bar gets vis-
ible in the lower right corner of the screen. Each step
takes a certain amount of time, also listed in Figure 3.
When the instrument has been applied for that amount
of time, the progress bar disappears, the instrument
blinks green once and can now be disposed of by the
nurse.
When the surgeon applies a wrong instrument, it
blinks red and has no effect.
HEAD TRACKING BASED AVATAR CONTROL FOR VIRTUAL ENVIRONMENT TEAMWORK TRAINING
259

Nurse
Anaesthesiologist
Surgeon
Light
Patient
Patient Monitor
Instruments
Disposal Bin
Nurse
P
a
t
i
e
n
t
Surgeon
Blood/Drugs
Instruments
Anaesthetic Machine
Stereo
Disposal Bin
Figure 2: Two views of the operating theatre implemented in our simulation.
4.3.2 Anaesthesiologist
The anaesthesiologist is located at the head of the pa-
tient, close to the airways. The role of the anaesthe-
siologist is to observe the patient’s vital signs on the
patient monitor and to counteract four different types
of events that will occur at random times during the
operation:
1. The oxygen level of the patient’s blood falls lower
than 80%. This will cause a hypoxaemia alarm.
In this case, the anaesthesiologist has to press the
“O
2
” button of the anaesthetic machine to sup-
ply additional oxygen and cause the blood oxygen
level to rise back to normal again.
2. The blood pressure drops due to bleeding during
the procedure, resulting in hypotension. In this
case the anaesthesiologist has to start a blood in-
fusion to stabilise the blood pressure again. The
blood pressure will continue to drop as long as the
bleeding is not stopped by the surgeon who has to
apply pressure by using pads.
3. An increasing heartbeat rate is an indicator of
tachycardia and has to be treated by administer-
ing β-Blockers. The procedure does not have to
be stopped during this condition, but as it is the
nurse who has to hand the drug to the anaesthe-
siologist, the surgeon might have to wait for the
next instrument.
4. A decreasing heartbeat rate is a sign of brady-
cardia and has to be treated by administering At-
ropine to the patient. Similar to tachycardia, the
procedure does not have to be stopped, but might
be delayed by the nurse having to pass the drug to
the anaesthesiologist.
4.3.3 Nurse
The nurse is located opposite, on the other side of the
patient. The role of the nurse is to
• switch on the lighting of the operating field,
• hand the requested instrument to the surgeon,
• take back the used instrument from the surgeon
and dispose of it, and
• hand the requested drugs to the anaesthesiologist.
4.3.4 Role Enforcement
Physical and logical barriers prevent any of the users
from taking over the role of any other user.
• The anaesthesiologist cannot reach the table with
the drug and blood bottles, because the stereo (see
Section 4.7 for details), a small tray, an IV stand,
and the disposal bin are in the way.
• The surgeon and the anaesthesiologist cannot eas-
ily reach the position of the other, because they
are blocked by the gas lines to the anaesthetic ma-
chine.
• The surgeon can see the instruments and guide the
nurse by looking at them, but it is impossible to
reach them from the other side of the patient.
• When roles other than the surgeon try to apply an
instrument on the patient, it will not have any ef-
fect.
• Running and jumping is disabled to prevent par-
ticipants with a higher experience in first person
perspective games to jump over the patient or ob-
jects to reach other users’ locations.
GRAPP 2011 - International Conference on Computer Graphics Theory and Applications
260

Start
Skin antiseptic
Skin layer cut
Skin layer retracted
Muscle layer
stitched
Use sponge to “paint patient”
with antisepsis solution (10s).
Clamp applied
Tissue removed
Cut skin layer
with scalpel (10s).
Muscle layer cut Finish
Retract skin layer
with retractor (7s).
Cut muscle layer
with scalpel (10s).
Remove necrotic tissue
in three steps
with different instruments (3x10s).
Stitch muscle layer
with needle and thread (10s).
Stitch skin layer
with needle and thread (10s).
Apply clamp (7s).
Figure 3: Overview of the steps of the simulated surgical procedure and the instruments necessary to reach the next step. The
coloured areas symbolise the sections of the procedure during which the events in Figure 4 can occur.
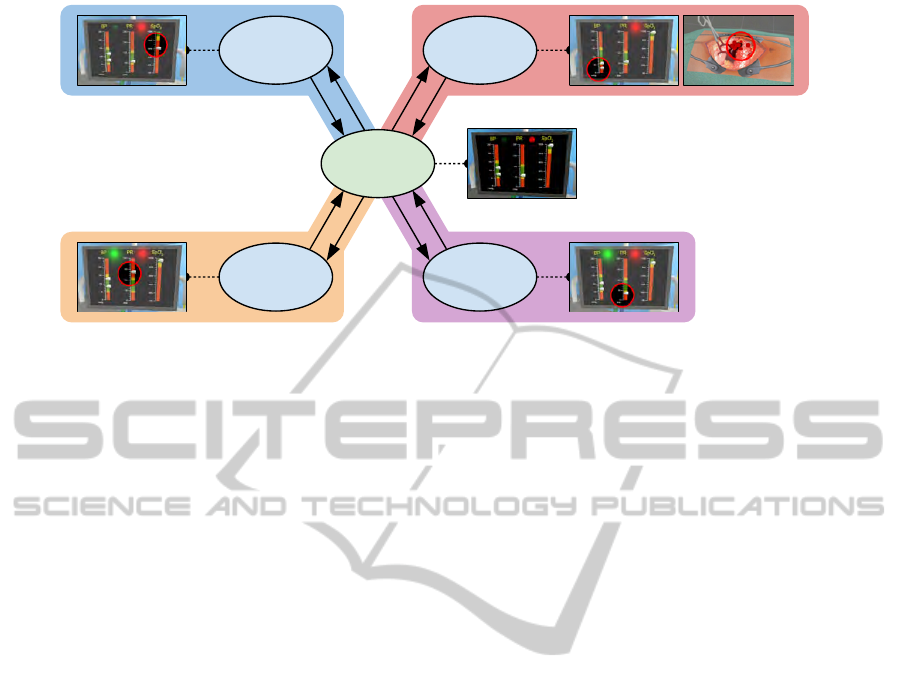
4.4 Events
During certain phases of the procedure, the events de-
scribed in Section 4.3.2 will occur. In Figure 3 and
Figure 4, the times at which the events can happen
are visualised by different colours.
During a certain phase of the operation, especially
while the clamp is applied or the necrotic tissue is be-
ing cut, unexpected and severe bleeding might occur.
This has to be stopped by applying pressure with a
pad. The operation can only be continued when the
bleeding has stopped. Bleeding is visualized by a red
particle system simulating a medium intense blood
flow inside the operating field. At the same time, the
anaesthesiologist will notice a loss of blood pressure.
Therefore, bleeding is an event that is easy to recog-
nise by all three roles.
At random times before and after this part, tachy-
cardia and bradycardia will occur. Those events are
most apparent to the anaesthesiologist who will see
the pointers on the patient monitor rise or fall. The
surgeon and the nurse will only have the audio cue
of the beeping heartbeat monitor becoming faster or
slower.
Finally, at another random point in time, the oxy-
gen saturation will drop significantly. The anaesthe-
siologist has to keep an eye on this value to prevent
hypoxaemia. This event is apparent only to the anaes-
thesiologist.
All four events are spaced temporally so that they
do not occur at the same time. Only when the partic-
ipants do not react to an event and instead continue
with the operation, the effects of multiple events will
eventually build up.
4.5 Face Validity
The simulated procedure is a very simplified version
of a real surgery. We had to find a compromise be-
tween face validity, the medical term for realism, and
simplicity for several reasons:
• The game engine has limitations in terms of phys-
ical simulation and animation.
• The interaction of the user with the VE has to be
kept simple.
• Some of the participants were non-medical stu-
dents who did not have a solid background in
medicine.
For both participant groups, medical and non-
medical, an explanation was given beforehand that
this scenario is a very simplified simulation and does
not always realistically reflect procedures, devices,
and effects.
HEAD TRACKING BASED AVATAR CONTROL FOR VIRTUAL ENVIRONMENT TEAMWORK TRAINING
261
Normal
Tachycardia Bradycardia
Blood loss/
Hypotension
Hypoxaemia
Administer β-Blocker
Administer Atropine
Start Blood Infusion / Surgeon: Stop BleedingIncrease Oxygen Flow
Figure 4: Overview of the four events that the team has to react to during the simulated surgical procedure. The events with
a coloured background occur at a random point of time during the steps of the procedure in Figure 3 with the same coloured
background.To return to the “Normal” state, the action next to the arrow has to be taken.
In summary, the following aspects of the simula-
tion are not realistic:
• The avatars don’t wear face masks which, in real-
ity, are mandatory for infection control (Lipp and
Edwards, 2002).
• A medical team is usually comprised of more than
only tree members. In our case, the roles of, e.g.,
the running nurse (responsible for fetching instru-
ments and gear from outside of the operating the-
atre) and anaesthesiology nurse (mainly responsi-
ble for assistive tasks required by the anaesthesi-
ologist) are not covered.
• The anaesthetic machine and the patient monitor
have a very simplified functionality and a different
look compared to real machines.
• In case of blood loss between 15% and 30% of
the total blood volume, defined as Class II hem-
orrhage by the American College of Surgeons,
saline fluid is usually sufficient to stabilise the
blood pressure (O’Leary et al., 2008, p. 564). A
blood transfusion is only necessary when the pa-
tient has lost larger amounts of blood. In addi-
tion, due to its viscosity, blood would not flow fast
enough into the circulatory system of the patient.
• In case of blood loss, the blood pressure does not
immediately decrease. Instead, the heart starts
to beat faster to maintain the blood pressure de-
spite the loss of blood volume (O’Leary et al.,
2008, p. 564). During this phase, only the dias-
tolic blood pressure starts to drop, caused by the
tachycardia and contracting blood vessels, while
the systolic pressure stays more or less the same.
• The incision is in general too large for an abdom-
inal procedure. In addition, removal of necrotic
pancreas is usually not done by an open opera-
tion. A multi-centre study (van Santvoort et al.,
2010) has shown that endoscopic procedures re-
sult in less complications and a lower mortality
rate among patients compared to open procedures.
• In the simulation, the pancreas is immediately vis-
ible. In reality, a larger part of the pancreas is hid-
den behind the stomach.
• The treatment for the critical events in the simula-
tion is extremely simplified.
• Instruments that have been dropped on the floor
can be used again on the patient without the risk
of infection (see further commentary to this issue
in 7.3).
• A team coming together for a real world medical
simulation already has a reasonable background
of medical knowledge and experience. During the
simulation, this knowledge and understanding of
their roles enables them to completely focus on
the teamwork and the task. In contrast, several of
the participants in our VE scenario had no medi-
cal knowledge and had to learn their roles as well
as having to work together as a team. For some
of them, having to learn the use of the VE was
another additional task.
4.6 Room Design
The overall design of the room was based on photos
of real operating theatres. 3D modelling of the in-
struments and other objects in the operating theatre
was done in the 3D open-source software Blender
(Blender Foundation, 2007). As for the room, we
used photos and schematic diagrams for textures and
GRAPP 2011 - International Conference on Computer Graphics Theory and Applications
262

measurements, but enlarged the majority of the instru-
ments by 20% to 50% to enable easier handling in the
VE.
4.7 Sound
To disrupt voice communication, we added two sound
sources to the simulation. Random announcements
can be heard in intervals of 20s to 40s through a
speaker mounted in the ceiling. Those announce-
ments are meant to disrupt the communication be-
tween the participants on a regular, but short basis.
A second sound source is a CD player with speak-
ers in the operating theatre, which is common practice
in operating theatres (Ullmann et al., 2008). It ran-
domly plays one of six music tracks that are all about
6min to 8min long and differ in style: Rock, Funk,
Folk, Jazz, Trip Hop, and Ambient. The anaesthesiol-
ogist can change the track, but cannot switch it off or
alter the volume.
The music is intended to be a continuous source
of noise, making it slightly harder for the participants
to fully rely on pure voice communication. There-
fore, we purposely violate a general recommendation
that, during a surgical procedure, the music should be
turned to a low volume in general and completely off
in cases of emergency (Hodge and Thompson, 1990).
5 SETUP
For the VE, we use the Source Engine, running a
heavily modified version of a multi-player death-
match game. The head tracking is done by an exter-
nal program that uses the commercial tracking engine
faceAPI (Seeing Machines, 2009). This program runs
in the background and communicates with the VE,
continuously transmitting updates of the user’s head
position and rotation.
We used three DELL Optiplex 745 desktop com-
puters
1
as clients and the development machine
2
as
the server.
The simulation was run with a 60Hz framerate on
the server as well as on the clients.
The client desktops were equipped with a Log-
itech QuickCam Pro 9000 webcam. This camera pro-
vided a stable framerate of 30fps with only the avail-
1
Intel Core
TM
2 Duo CPU, 2.13GHz, 3GB memory, Windows
Vista Enterprise 32bit, Radeon X1300 graphics card with 256MB
graphics memory, DELL 2007FP 20.1inch flat panel monitor with
1600x1200pixel resolution.
2
Intel Core
TM
2 Quad CPU, 2.4GHz, 4GB memory, Windows
XP Professional, NVIDIA Quadro FX 570 graphics card with
256MB graphics memory.
able room lighting. Autofocus ensured that even with
movement away and towards to the monitor, the heads
of the participants always stayed in focus.
It was not possible to organise three separate
rooms for the participants, so we had to use other
methods to ensure that they could not hear or see each
other directly. One solution was the use of Logitech
G35 headsets which covered the ears of the partici-
pants completely and provided enough isolation from
outside sounds. That way, the participants had to rely
solely on communication channels provided by the
game engine.
To prevent the participants from seeing each other
or each other’s screens, we set up office walls that
occluded direct line of sight between the three client
workstations and in addition provided further acous-
tic separation of the participants. A photo of the com-
plete setup is shown in Figure 5.
6 METHODOLOGY
We recruited participants by printed advertisements in
the buildings of the departments of Computer Science
and the Medical School, and by emails sent to classes
and postgraduate students of the department of Com-
puter Science.
On average, one user study took around 90min to
complete. Due to this extended duration, we reim-
bursed the participants by handing out grocery vouch-
ers valued 10 NZD. We assumed that this amount
would encourage participants sufficiently without in-
troducing the risk that they would “just do it for the
money”.
We explained the overall goal of the study to the
participants, mentioning the head tracking and the
possibility to control the view and the head movement
of the avatar. Afterwards, we gave a brief overview of
the procedure and the roles and their responsibilities.
The participants were encouraged to interrupt and ask
questions at any stage.
Before the actual study took place, We introduced
the participants to the VE by running an introduction
simulation without recording any data. The partici-
pants were able to get accustomed to the environment
and to experiment with objects, instruments, and de-
vices. Each participant had a set of three information
sheets in front of them that described their role, the
necessary instruments or devices, and the mouse and
keyboard controls.
After the introduction and any further questions
from the participants, we enabled data logging of the
simulation and started the actual series of six exper-
iments. The participants were not informed whether
HEAD TRACKING BASED AVATAR CONTROL FOR VIRTUAL ENVIRONMENT TEAMWORK TRAINING
263

Figure 5: Photo of the experimental setup with three participants. The participants are isolated visually by office walls and
acoustically by headsets that completely cover the ears.
head tracking was disabled or enabled.
After each experiment, the participants filled in a
short questionnaire about their opinion on teamwork
and communication aspects of the simulation. During
that time, we changed the information sheets accord-
ing to the rotating roles of the participants.
At the end of the six experiments, the participants
filled out an additional questionnaire page with gen-
eral questions about the VE.
7 RESULTS
7.1 Participants
More than 30 people answered to the invitation emails
and advertisements. However, due to financial and
time constraints, we had to limit the amount of par-
ticipants to 27. The age of the participants, 6 of them
being female, covered a range from 20 to around 44
years (see Figure 6 for more details).
All participants have used a computer often or
more. 5 of them have not played computer games at
all within the three months before the study. 22 of the
participants have had experience in using a webcam,
e.g., by using it for video conferencing. 11 of them
have not used a VE before.
7.2 Hypotheses
Hypothesis H1: When head tracking is enabled, the
participants demonstrate more overall head move-
ment than when head tracking is disabled.
For the verification of this hypothesis, we calcu-
lated the total amount of translational and rotational
head movement in 1s steps and compared the values
from experiments with head tracking disabled to the
values from experiments with head tracking being en-
abled.
The resulting data is not normally distributed, but
instead strongly skewed towards lower values and
tailing off towards higher values. For that reason, it is
not possible to apply the t-test to this data. Instead, we
chose the Wilcoxon rank sum test (McCrum-Gardner,
2008).
The results show a statistically significant but only
minute difference in translational movement (me-
dian values 28.2mm / 26.7mm, Wilcoxon rank sum
test with continuity correction, p < 0.001, 95% CI
0.71mm to 1.51mm) and a minute and statistically in-
significant difference in rotational movement (median
values 11.2
◦
/ 11.1
◦
, Wilcoxon rank sum test with
continuity correction, p = 0.500, 95% CI -0.07
◦
to
0.16
◦
). Based on this outcome, Hypothesis H1 has to
be falsified. When head tracking is active, the partici-
pants do not increase the amount of their overall head
movement. On the contrary, the data suggests that the
amount of movement is the same irrespective of head
tracking being disabled or enabled.
Hypothesis H2: When head tracking is enabled, the
amount of head movement is greater while partici-
pants talk to each other compared to when head track-
ing is disabled.
For the analysis of this hypothesis, we prepared
the data in the same way as described for the hypoth-
esis before, but selected only the subset of the mea-
surements when the participants were talking. Again,
we had to apply the Wilcoxon ranked sum test due to
the skewed distribution of the data.
Like for the previous hypothesis, the results of
the test for head movement of the participants when
they were talking do either indicate statistically sig-
GRAPP 2011 - International Conference on Computer Graphics Theory and Applications
264

Percent of Total
0%
50%
100%
Female Male
6 21
(a) Gender
Percent of Total
0%
50%
100%
<20 20−24 25−29 30−34 35−39 40−44 45−49 50−54 55−59 >=60
8 6 8 3 1 1
(b) Age Group
Figure 6: Demographic data of the participants of the multi user study.
nificant but minor differences, or statistically in-
significant differences. Translational head movement
differs only by -1.0mm (median values 35.9mm /
34.9mm, Wilcoxon rank sum test with continuity cor-
rection, p = 0.054, 95% CI -0.00 to 1.53), and rota-
tional movement by -0.2(median values 14.0 / 13.8,
Wilcoxon rank sum test with continuity correction,
p = 0.183, 95% CI -0.06 to 0.42).
Similar to the previous one, Hypothesis H2 has
to be falsified. While talking, the participants do not
increase their head movement significantly when head
tracking is enabled. Instead, the results suggest that
the amount of movement is the same for head tracking
disabled respectively enabled.
Hypothesis H3: When head tracking is enabled, the
participants perceive the other avatars as more natu-
ral than when head tracking is disabled.
For the verification of this hypothesis, we evalu-
ated the questionnaires that the participants had to an-
swer after each of the six experiments (see Figure 7).
We converted the answers to the 7-point Likert
scales on the questionnaires to a numerical value us-
ing a translation scale of −3 for “Strongly Disagree”
to +3 for “Strongly agree”. We then compared the
answers of experiments 1, 3, and 5 (head tracking dis-
abled) to the answers of experiments 2, 4, and 6 (head
tracking enabled) using a t-test.
The comparison reveals a statistically non-
significant difference of 0.2 (mean values 1.4 / 1.6,
Welch Two Sample t-test, p = 0.282, 95% CI −0.45
to 0.13), thereby weakly supporting the validity of
the hypothesis. The participants perceive the other
avatars slightly more natural when head tracking is
enabled compared to when head tracking is disabled.
Hypothesis H4: When head tracking is enabled,
the participants perceive the communication with the
other participants as more natural than when head
tracking is disabled.
We evaluated the answers to the question about
how natural the communication is perceived (see Fig-
ure 8) in a similar way to the one described for the
previous hypothesis. Again, we compared the results
of experiments 1, 3, and 5 (head tracking disabled) to
the answers of experiments 2, 4, and 6 (head tracking
enabled) using a t-Test.
The comparison suggests that the participants per-
ceive the communication slightly more natural when
head tracking is enabled than when it is disabled
(mean values 1.7 / 1.9, Welch Two Sample t-test,
p = 0.059, 95% CI −0.55 to 0.01), thereby support-
ing the hypothesis.
Hypothesis H5: When head tracking is enabled, the
participants look more at each other’s avatars than
when head tracking is disabled.
The logged data from the simulation also recorded
which user has been looking at which object or avatar
for how long. We used this information to calculate
the relative amount of time each participant had been
looking at one of the team members. The results,
grouped by role, are visualized in Figure 9.
Though there are differences in the comparisons,
those are again only minor and statistically insignif-
icant. When head tracking is enabled, the surgeon
spends 0.4% more time looking at the colleagues
(mean values 25.0% / 25.4%, Welch Two Sample t-
test, p = 0.849, 95% CI -5.15% to 4.25%), the anaes-
thesiologist 1.6% (mean values 11.7% / 13.3%, Welch
Two Sample t-test, p = 0.430, 95% CI -5.71% to
2.47%), and the nurse 1.4% (mean values 23.9% /
25.3%, Welch Two Sample t-test, p = 0.576, 95% CI
-6.05% to 3.40%) compared to when head tracking is
disabled.
Overall, these results add only very weak support
for the hypothesis. Nevertheless, it is interesting to
see how the values reflect the different observation
patterns of the three roles. It is apparent that the
anaesthesiologist has a different pattern than surgeon
and nurse. This difference is most probably caused by
the primary task of the role of the anaesthesiologist:
to watch the patient monitor for changes in the vital
signs.
HEAD TRACKING BASED AVATAR CONTROL FOR VIRTUAL ENVIRONMENT TEAMWORK TRAINING
265

Percent of Total
0%
50%
100%
Strongly
Disagree
Disagree Slightly
Disagree
Neutral Slightly
Agree
Agree Strongly
Agree
2 6 34 31 8
(a) Head Tracking disabled
Percent of Total
0%
50%
100%
Strongly
Disagree
Disagree Slightly
Disagree
Neutral Slightly
Agree
Agree Strongly
Agree
3 4 29 32 13
(b) Head Tracking enabled
Figure 7: Results of the questionnaires about how natural the participants perceive the teammember’s avatars.
Percent of Total
0%
50%
100%
Strongly
Disagree
Disagree Slightly
Disagree
Neutral Slightly
Agree
Agree Strongly
Agree
4 5 14 49 9
(a) Head Tracking disabled
Percent of Total
0%
50%
100%
Strongly
Disagree
Disagree Slightly
Disagree
Neutral Slightly
Agree
Agree Strongly
Agree
2 4 10 46 19
(b) Head Tracking enabled
Figure 8: Results of the questionnaires about how natural the participants perceive the communication with their team mem-
bers.
Hypothesis H6: When head tracking is enabled, the
participants solve the teamwork task better than when
head tracking is disabled.
As described in Section 3, we calculated the effi-
ciency of the teamwork based on two values that are
extracted from the data:
• The total time for completion of each experiment.
• The relative amount of time that the patient is in a
critical state.
For all two values, we expected the influence of
the head tracking to reflect on the results like shown in
Figure 10. The participants were repeating a similar
task six times, so we anticipated a learning curve that
would demonstrate a tendency towards faster comple-
tion with each repetition, with a gradient that would
ease out towards the end. The positive influence of
head tracking would be visible by average values that
are below the fitting curve for experiments 2, 4, and 6,
whereas experiments 1, 3, and 5 without head track-
ing would produce results above the fitting line.
However, the measured results look very differ-
ent. The learning curve is visible in experiments 2 to
6, but experiment 1 has a significantly lower comple-
tion time than experiments 2 to 3. The reason for this
outlier is most probably the practice run that the par-
ticipants had to complete before the first experiment
was conducted.
For the practice run, they performed the teamwork
task without their results being recorded and with help
and minor intervention from the simulation admin-
istrator. After the practice run, the first experiment
started with the participants having the same roles
than in the practice run. They had gotten used to their
roles and were able to finish the teamwork task rela-
tively fast.
For experiment 2 and 3, the roles were rotated so
that every participants had to learn the requirements
and tasks of the new roles. The influence of this new
learning process reflects in the similar results for ex-
periments 2 and 3.
Finally, for experiments 4 to 6, the participants
were repeating former role combinations. Because by
now, they had experienced every role, they were bet-
ter able to focus on the task.
Due to the unusual values of the boxplots re-
sults, it is not possible to model an average curve for
the comparison of the results with and without head
tracking. Instead, we grouped the values by head
tracking “off” (experiments 1, 3, and 5) and “on” (ex-
periments 2, 4, and 6) and compared the mean values
using a t-test. The values do not differ significantly
(mean values 285.2s /285.9s, Welch Two Sample t-
test, p = 0.974, 95% CI -45.21s to 43.74s). Instead,
the high p-value suggests that head tracking makes no
difference at all on the completion times of the team-
work task.
Likewise, the comparison of the relative amount
of time that the master alarm was on results in a sta-
tistically insignificant difference (mean values 16.7%
/ 17.3%, Welch Two Sample t-test, p = 0.821, 95%
CI -6.68% to 5.33%), suggesting additional support
for the hypothesis that head tracking makes no differ-
ence at all.
GRAPP 2011 - International Conference on Computer Graphics Theory and Applications
266

Relative Time Looking at Avatars / %
Head Tracking
On
Off
10 20 30 40
●
Surgeon
10 20 30 40
●
Anaesthesiologist
10 20 30 40
●
Nurse
Figure 9: Plots of the relative amount of time the participants have been looking at the avatars of their team members.
Experiment Number
Completion Time / sec
100
200
300
400
500
1 2 3 4 5 6
(a) Expected results
Experiment Number
Completion Time / sec
100
200
300
400
500
1 2 3 4 5 6
●
●
●
●
●
●
●
●
(b) Measured results
Head Tracking
Completion Time / sec
100
200
300
400
500
Off On
●
●
(c) Grouped by head
tracking off/on
Figure 10: Box plots of the times the participants needed to complete the task.
7.3 Overall Impression
Overall, the participants enjoyed to work in teams
within the simulation and had no major problems with
the head tracking. In fact, the tracking was so unob-
trusive, that several participants later commented that
they were not at all aware of the tracking and the head
movements.
When being asked about the stressfulness of the
roles, the majority of the participants agreed that the
nurse was the most stressful role, in contrast to the
anaesthesiologist, who was considered the most re-
laxed role.
7.3.1 Head Tracking
There were slight problems resulting from a combi-
nation of head tracking jitter and handling of small
objects like the scalpel. In these cases, some partic-
ipants had problems passing on the scalpel from one
to another. The tracking jitter of one simulation client
would move the object in a slightly random pattern,
making it more difficult for the opposite user to grab
it. In their comments, several participants agreed on
the fact that small objects were most difficult to han-
dle, especially the scalpel.
On the other hand, head tracking was mentioned
as being very useful in precise placement of instru-
ments or for zooming in on the patient monitor.
In general, the rotation of the avatar’s heads by
head tracking was perceived, although most partici-
pants stated that they were too preoccupied by the task
to pay attention to the head movements. Occasions
where the tracking would stand out were when the
participants would physically look sideways to their
role description sheets and their avatar would also per-
form that sideways look. Other occasions were, for
example, head bobbing to the rhythm of the music.
7.3.2 Involvement
The participants demonstrated a high level on involve-
ment, characterized by utterances like “Oh No!”,
when the master alarm would go off, or “Don’t die,
please!” when the bleeding could not be stopped im-
mediately. Sometimes, participants would even en-
gage in role play and joke around or tease their team
colleagues.
On some occasions, when teamwork was not op-
timal, and the group was especially competitive, the
HEAD TRACKING BASED AVATAR CONTROL FOR VIRTUAL ENVIRONMENT TEAMWORK TRAINING
267

tone turned slightly aggressive. In one group, for ex-
ample, the nurse ignored the request of the surgeon for
the pad and instead decided to give a bottle of blood to
the anaesthesiologist first. In terms of efficiency, this
step was not optimal, because as long as the bleeding
was not stopped, the patient continued to lose blood.
So the first priority of the team should have been to
stop the bleeding first (i.e., give the surgeon a pad)
and then to stabilise the blood pressure. The surgeon,
being aware of this ineffectiveness, commented in a
slightly annoyed tone: “We need another nurse!”, In
return, the nurse defiantly countered: “I think we need
another surgeon!”.
7.3.3 Unexpected Behaviours
A disadvantage of the rotation of roles was that on
several occasions, participants would take over re-
sponsibilities of other roles. A nurse who was the
anaesthesiologist in the previous run would keep an
eye on the patient monitor and grab the necessary
drug before the current anaesthesiologist would no-
tice and require it. However, in a training environ-
ment where roles are predetermined and not rotated
after every simulation, this problem would occur only
to a lesser extent or not at all.
Another unexpected behaviour, observed espe-
cially with participants who indicated a high amount
of computer game playing time, was the exploration
of similarities and differences between the simula-
tion and reality. When participants had, for exam-
ple, dropped the scalpel on the floor, there was an
initial hesitancy to use that scalpel again on the pa-
tient, caused by basic knowledge of the risk of in-
fection in reality. However, when the participants
found out that, in the simulation, this re-use did not
have any negative consequences, they continued to
use dropped instruments on the patient in favour to de-
manding a new and “clean” instrument from the nurse
and thereby losing time.
8 CONCLUSIONS
Table 1 summarizes the hypotheses and the results of
our findings. In summary, the evaluation of experi-
mentally obtained data is showing
• that avatars with tracking-based head movement
are perceived as more natural than avatars without
tracking-based head movement, and
• that avatars with tracking-based head movement
facilitate a communication that is perceived as
more natural than with avatars without tracking-
based head movement,
However, these results are either only weakly sup-
ported by the data or the difference in the participants’
perception is only marginal.
Table 1: This table summarises the results of the multi user
study. “+” indicates that the results support the hypothesis.
“-” indicates that the results falsify the hypothesis.
Hypothesis Experimental Result
H1 -
H2 -
H3 +
H4 +
H5 +
H6 -
Unfortunately, there is only very weak support for
the hypothesis that participants look at each other’s
avatars more regularly when head tracking is enabled.
Finally, contrary to the original hypotheses, the
analysis of the data also shows
• that the participants do not change the amount of
head movement when head tracking is enabled
compared to when head tracking is disabled,
• that, while talking, the participants do not change
the amount of head movement when head track-
ing is enabled compared to when head tracking is
disabled, and
• that the teamwork performance does not improve
when head tracking is enabled compared to when
head tracking is disabled.
While especially those last three statements have
the potential to discouragement, they nevertheless in-
dicate an important fact: Although a new technol-
ogy has been introduced with several possibilities for
failure and measurement errors, the participants were
largely unaware of that new technology. They per-
ceived an improvement in the naturalness of the VE
and an improvement of the quality of communication,
but did not experience any major negative limitations
imposed upon them by this new technology.
We assume that the main reason for the lack of
influence of head tracking was the fact that the simu-
lated scenario required more focus on the task and on
handling the instruments than on the communication.
In addition, not all possibilities of this new tech-
nology have been explored yet. For our experiment,
the head rotation was simply mapped onto the avatars
without any further semantic analysis. One future ex-
tension will be to calculate the actual target of the
user’s head direction on the screen and to use that in-
formation to transform the tracking data so that the
user’s avatar looks at the same target in the VE. An
GRAPP 2011 - International Conference on Computer Graphics Theory and Applications
268

additional level of realism would be introduced by eye
tracking and a similar transformation of the avatar’s
gaze.
Automatic recognition of facial expressions is an-
other future extension. This feature would not in-
crease the complexity of the physical setup and would
also not require any major changes in our simulation
engine. However, we would expected that the inclu-
sion of this communication channel can further in-
crease at least the perceived naturalness and ease of
use – if not more.
REFERENCES
Blender Foundation (2007). Blender. http://
www.blender.org.
Cartmill, J., Moore, A., Butt, D., and Squire, L. (2007).
Surgical Teamwork: Systemic Functional Linguistics
and the Analysis of Verbal and Nonverbal Meaning in
Surgery. ANZ Journal of Surgery, 77(Suppl 1):A79–
A79.
Cordea, M. D., Petriu, D. C., Petriu, E. M., Georganas,
N. D., and Whalen, T. E. (2002). 3-D Head Pose Re-
covery for Interactive Virtual Reality Avatars. IEEE
Transactions on Instrumentation and Measurement,
51(4):640–644.
Danforth, D., Procter, M., Heller, R., Chen, R., and John-
son, M. (2009). Development of Virtual Patient Sim-
ulations for Medical Education. Journal of Virtual
Worlds Research, 2(2):3–11.
Hodge, B. and Thompson, J. F. (1990). Noise pollution
in the operating theatre. The Lancet, 335(8694):891–
894.
Lipp, A. and Edwards, P. (2002). Disposable surgical
face masks for preventing surgical wound infection in
clean surgery. Cochrane Database of Systematic Re-
views 2002, 1(CD002929).
Marks, S., Windsor, J., and Wnsche, B. (2010). Evalua-
tion of the Effectiveness of Head Tracking for View
and Avatar Control in Virtual Environments. 25th In-
ternational Conference Image and Vision Computing
New Zealand (IVCNZ) 2010.
McCrum-Gardner, E. (2008). Which is the correct statistical
test to use? British Journal of Oral and Maxillofacial
Surgery, 46(1):38–41.
Messinger, P. R., Stroulia, E., Lyons, K., Bone, M., Niu,
R. H., Smirnov, K., and Perelgut, S. (2009). Vir-
tual Worlds – Past, Present, and Future: New Direc-
tions in Social Computing. Decision Support Systems,
47(3):204–228.
Ohya, J., Kitamura, Y., Takemura, H., Kishino, F., and
Terashima, N. (1993). Real-time reproduction of
3D human images in virtual space teleconferencing.
In Virtual Reality Annual International Symposium,
1993, pages 408–414.
O’Leary, J. P., Tabuenca, A., and Capote, L. R., editors
(2008). The physiologic basis of surgery. Wolters
Kluwer Health/Lippincott Williams & Wilkins, 4 edi-
tion.
Seeing Machines (2009). faceAPI. http://
www.seeingmachines.com/product/faceapi.
Sko, T. and Gardner, H. J. (2009). Human-Computer Inter-
action - INTERACT 2009. In Gross, T., Gulliksen, J.,
Kotz, P., Oestreicher, L., Palanque, P., Prates, R. O.,
and Winckler, M., editors, Lecture Notes in Computer
Science, volume 5726/2009 of Lecture Notes in Com-
puter Science, chapter Head Tracking in First-Person
Games: Interaction Using a Web-Camera, pages 342–
355. Springer Berlin / Heidelberg.
Ullmann, Y., Fodor, L., Schwarzberg, I., Carmi, N., Ull-
mann, A., and Ramon, Y. (2008). The sounds of music
in the operating room. Injury, 39(5):592–597.
Valve Corporation (2004). Valve Source Engine Features.
http://www.valvesoftware.com/sourcelicense/ engine-
features.htm.
van Santvoort, H., Besselink, M., Bakker, O., Hofker, H.,
Boermeester, M., Dejong, C., van Goor, H., Schaa-
pherder, A., van Eijck, C., Bollen, T., van Ramshorst,
B., Nieuwenhuijs, V., Timmer, R., Lamris, J., Kruyt,
P., Manusama, E., van der Harst, E., van der Schelling,
G., Karsten, T., Hesselink, E., van Laarhoven, C.,
Rosman, C., Bosscha, K., de Wit, R., Houdijk, A.,
van Leeuwen, M., Buskens, E., Gooszen, H., and
Dutch Pancreatitis Study Group (2010). A Step-
up Approach or Open Necrosectomy for Necrotizing
Pancreatitis. The New England Journal of Medicine,
362(16):1491–1502.
Wang, S., Xiong, X., Xu, Y., Wang, C., Zhang, W., Dai,
X., and Zhang, D. (2006). Face-tracking as an aug-
mented input in video games: enhancing presence,
role-playing and control. In CHI ’06: Proceedings of
the SIGCHI conference on Human Factors in comput-
ing systems, pages 1097–1106, New York, NY, USA.
ACM.
Yim, J., Qiu, E., and Graham, T. C. N. (2008). Experience in
the design and development of a game based on head-
tracking input. In Future Play ’08: Proceedings of
the 2008 Conference on Future Play, pages 236–239,
New York, NY, USA. ACM.
HEAD TRACKING BASED AVATAR CONTROL FOR VIRTUAL ENVIRONMENT TEAMWORK TRAINING
269
