
STUDY AND DEVELOPMENT OF THE RESCUE ROBOT
PREVENTING CRUSH SYNDROME
OF EARTHQUAKE VICTIMS
Taku Sahashi
1,2
, Akira Sahashi
2
, Hisashi Uchiyama
1
and Ichiro Fukumoto
1
1
Nagaoka University of Technology, 1603-1, Kamitomiokamachi, Nagaoka, Niigata, Japan
2
Project-I Co. Ltd., 154-403, Utasato-cho, Nishi-ku, Nagoya, Aichi, Japan
Keywords: Disaster, Earthquake, Rescue robot, Crush syndrome.
Abstract: In the Hanshin and Chu-etsu earthquake, many victims were crushed by rubble and died by “crush
syndrome”. Even the simple rescue method that remove the rubble, it could be a cause of death. As the only
countermeasure, DMAT (=Disaster Medical Assistance Team) creeps into fallen houses, and treat dialysis
or drip “crush injury cocktail”. But these methods are very dangerous for victims and DMAT to treat amid
the aftershocks. We think that Rescue Robot technique is just suitable solution for the dilemma under
various and dangerous situations. The Rescue Robot has the dual tiered crawler. The Rescue Robot goes
through under rubble open, and the victims are held in the container inside of the Robot body. We already
built a prototype model, so we present an outline of our rescue robot. And we will show the research of the
Blade mechanism to open rubble, and the mechanism of prevent Crush Syndrome that will be mounted on
1/1 size prototype model in the future.
1 INTRODUCTION
Japan has 0.25 percent of global land in the world.
Compared to it, the frequency of earthquakes above
magnitude 6 is 20.8 percent (see Figure 1), and the
number of active volcanoes is 7.0 percent compared
with the world total.
Japan is a small country, but there has the most
frequent earthquake.
Figure 1: Number of earthquakes above magnitude 6.
(Copied from Homepage of Japanese Cabinet Office
http://www.bousai.go.jp/1info/pdf/saigaipanf.pdf).
1.1 Problem with Current Disaster
Medical Engineering (ME) in
Japan
Professor Fukumoto of Nagaoka University of
Technology, who was performed disaster medical
treatment at 2004 Chu-etsu earthquake and 2007
Chu-etsu offshore earthquake in Japan. He got a
shock because disaster ME was not progressed since
Great Hanshin earthquake 1995. In shelter,
medicines, water and electricity were not enough
supplied for several days cause of lifeline damage.
Almost medical equipments were broken by falling
on the floor or/and power failure, and the run out of
manpower caused by many patients rushing to an
Alternative Medical Treatment Site at the same time.
The doctor was not able to take even a short break
for 4 days.
If this situation was ignored, the likelihood of
medical negligence of doctors increases, and
decrease doctors who voluntarily treat in a disaster
time
43
Sahashi T., Sahashi A., Uchiyama H. and Fukumoto I..
STUDY AND DEVELOPMENT OF THE RESCUE ROBOT PREVENTING CRUSH SYNDROME OF EARTHQUAKE VICTIMS.
DOI: 10.5220/0003536200430049
In Proceedings of the 8th International Conference on Informatics in Control, Automation and Robotics (ICINCO-2011), pages 43-49
ISBN: 978-989-8425-75-1
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

Figure 2: Outline of the Disaster Medical Assistance System.
1.2 The Disaster Medical Assistance
System
To solve these problems, we, “The Disaster ME
laboratory” are aiming to construct “the Disaster
Medical Assistance System” (see Figure 2) which
has been designed to support disaster medical care
through medical engineering that based on bitter
experiences of these earthquakes.
Devices of “the Disaster Medical Assistance
System” have correlations with each other
in terms
of
by functioning systematically and dealing with
various disaster situations.
The Rescue Robot is one of the devices of the
Disaster Medical Assistance System. It is belonging
to the center of this system that was defined as
“Rescue phase”.
In other words, this rescue robot is not intended
to operate alone. This Robot will be able to work
only after embedding this system.
2 THE RESCUE ROBOT
We will introduce “The dual crawler-type Rescue
Robot” to prevent crush syndrome.
Figure 3 is the picture in which prototype model
of the robot was demonstrated in “the safe and
secure festival in Yokohama 2009”.
Figure 3: Appearance of the Rescue Robot.
2.1 Necessity of the Rescue Robot
In the Hanshin and Chu-etsu earthquake, many
victims crushed by rubble. But many victims died by
symptom of “crush syndrome”, too. Even the simple
rescue method that remove the rubble, it could be a
cause of death.
As the only countermeasure, Disaster medical
assistance team (DMAT) creeps into fallen houses,
and perform confined space medicine (CMS) that
treat dialysis or administration of intravenous fluids
at present.
These methods are too dangerous to treat amid
the aftershocks for both victims and DMAT.
ICINCO 2011 - 8th International Conference on Informatics in Control, Automation and Robotics
44
Nonetheless, it is problem that cannot begin the
rescue operation until safety is secured.
We think that the rescue robot technique is just
suitable solution for the dilemma under various and
dangerous situations.
2.2 Crush Syndrome
Crush syndrome is a form of traumatic
rhabdomyolysis (= a condition in which damaged
skeletal muscle tissue breaks down rapidly) that
occurs after prolonged continuous pressure and
characterized by systemic involvement.
Extensive muscle crush injury culminating in the
crush syndrome is often lethal unless promptly and
vigorously treated.
The damages are seen after a prolonged period
of pressure on a muscle group. The pressure causes
necrosis of the muscle, and during revascularisation,
diffusion of calcium, sodium, and water into the
damaged muscle cells is seen, together with loss of
potassium, phosphate, lactic acid, myoglobin, and
creatinine kinase. These changes can lead to
hyperkalemia (= medical emergency due to the risk
of potentially fatal abnormal heart rhythms), acidosis
(=an increased acidity in the blood), acute renal
failure, and hypovolemic shock (= cause of lack of
blood).
Crush syndrome is commonly encountered after
earthquakes, and in various other disasters.
Sudden release of a crushed extremity may result
in “reperfusion syndrome” (= acute hypovolemia
and metabolic abnormalities). This condition may
cause lethal cardiac arrhythmias. Further, the
sudden release of toxins from necrotic muscle into
the circulatory system leads to myoglobinuria (= the
presence of myoglobin in the urine), which causes
renal failure if untreated.
Difficulties with communication and
transportation in the disaster often prevent early
rescue and treatment. Early rescue and
administration of intravenous fluids are important in
preventing renal failure.
2.3 Advantage of the Rescue Robot
2.3.1 Strong Point of our Crawler System
We wanted to make the Rescue robot that can work
under rubble. But, we could not adopt existing
crawler mechanism.
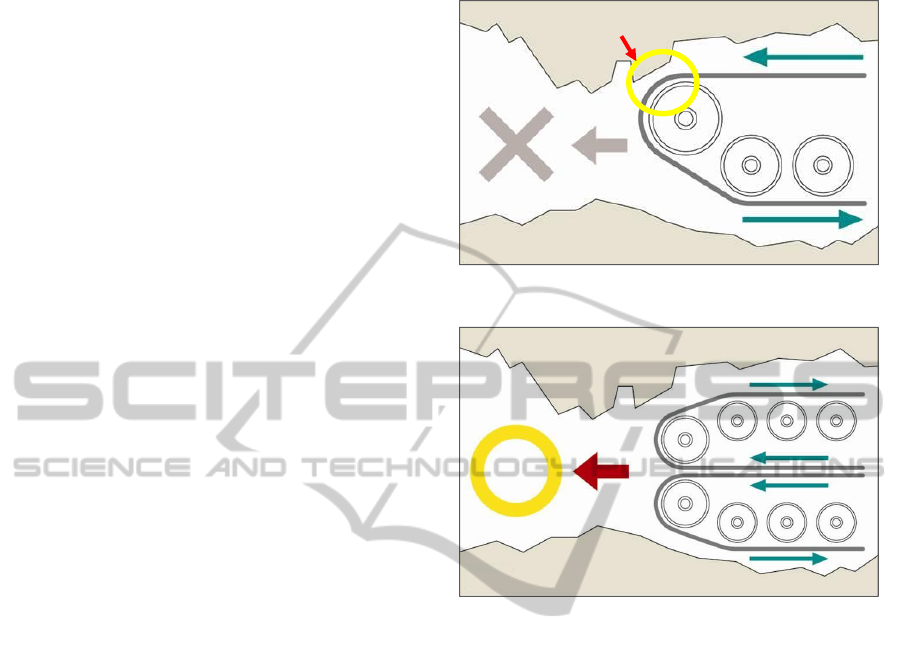
Existing crawler robots are too hard to proceed
under rubble. Because the crawler has problem with
rotational direction. The problem is that they are
lodged in narrow space vertically (see Figure 4).
Figure 4: Problem of existing crawlers.
Figure 5: Advantage of our crawler system.
Therefore, we thought out the dual tiered crawler
that coupled with crawler runs adverse directions.
This crawler system could grip obstructions above,
and it was also possible to even use as foothold (see
Figure 5).
2.3.2 Mechanism of the Crush Syndrome
Prevention
As “2.1 Necessary of Rescue Robot”, if the Rescue
Robot could reach at the victim under rubble, the
victim would occur Crush syndrome cause of just
only way to remove rubble.
Therefore, we designed “the mechanism of the
Crush syndrome prevention”.
The Rescue Robot is equipped with the cuff into
that body. The cuff is inflatable band used in
sphygmomanometer (= blood pressure meter).
The cuff is inflated rapidly by using carbon
dioxide gas from small-sized cylinder. It is able to
stop blood flow around affected part (mostly leg) by
inflate cuff pressure. In other words, this cuff works
to prevent re-circulating of blood that cause
contamination, which prevents the Crash syndrome.
Stuck b
y
here!
STUDY AND DEVELOPMENT OF THE RESCUE ROBOT PREVENTING CRUSH SYNDROME OF EARTHQUAKE
VICTIMS
45

This method is only a first–aid treatment, it is
necessary to treatment minutely by doctor after the
rescue.
In addition, there is no practical example of this
approach, it will require further research and
experimentation.
2.3.3 Vital Sign Sensor Probe
Procedure of Crush syndrome prevention is a
medical practice. Therefore, measurement of vital
signs is essential.
The Vital Sign Sensor Probe is composed of
Near Infrared Camera, Infrared LED Light and
Microphone/Speaker. These Sensors are equipped
with tip of the flexible arm.
The Near Infrared Camera and the Light checks
the victim status and blood flow measurement
visually. The Microphone is used to determine
responsiveness of victims and check their heartbeat.
The Speaker is used to call the victim and give their
encouragement. (see Figure 6)
The doctor and operator utilize them for
determining the severity of the victims.
Because hemoglobin absorbs near infrared light
(wavelengths about 780nm), we can confirm
superficial veins and the flow.
Figure 6: Outline of the Vital Sign Sensor Probe.
2.4 Expected Procedures of the Rescue
Operation
First, the Rescue Robot is operated by three peoples
and more. As the detail of the member’s professions
and rolls, Emergency Medical Technician (EMT) as
operator, Firefighters (or any can operate) as cable
management assistant, and doctor who performed
the operation instructions (see Figure 7). This
selection was designed based on the laws of Japan.
This Robot can be controlled remotely by wired
control panel. It goes through under rubble with
squeezing rubble and reached to victim (see Figure
8). After removal of rubble, affected parts of victims
are tighten smoothly by cuff to prevent crush
syndrome. And the victim is picked up in the
container inside of the Robot body. (see Figure 9).
Figure 7: Expected operators of the Rescue Robot.
Figure 8: Assumed figure of the Rescue Robot Operation.
Figure 9: Assumed figure of putted on the cuff.
After picking up the victim in the container, the
Rescue Robot goes back from under rubble to
ICINCO 2011 - 8th International Conference on Informatics in Control, Automation and Robotics
46

ground. In the safe place to both victims and
rescuers, after that the victims are took enough
treatment by doctors.
2.5 Specification of the Rescue Robot
The following are the specs of 1/1-sized prototype
model of the Rescue Robot that currently under
development. Incidentally, all of figures do not
include the figure of “the Blade mechanism to open
rubble” and “the mechanism of the Crush syndrome
prevention” that cannot be installed to the Rescue
Robot currently.
Length: 1.92m
Width: 1.33m
Height: 0.76m
Weight: 329kg (Only the vehicle weight. Not
include control panel’s and cable’s)
Engines: 2 motors of CVVF (Constant-Voltage
Variable-Frequency) control drive
Batteries: DC12V × 6 = 72V (see Figure 10)
Controls: Using the remote control panel
connected by 10 meters cable wire (Batteries are
mounted on control panel carrier)
Sensors: Front and Rear Cameras (and
considering mount a roof top camera), the Vital Sign
Sensor (made by Near Infrared Camera, Microphone
/ Speaker and LED Light)
Figure 10: Motors and Batteries.
3 ISSUES OF THE RESCUE
ROBOT
3.1 Current Issues
Various problems arise in disaster time, but this
prototype may be able to withstand these situations.
Introduce of the following improvements to the
Robot enable the handling of various situations from
now on.
1) Improvement of the anti-crush durability of
whole parts including container and crawler.
2) Waterproof and fireproof.
3) Study and development of the Blade
mechanism to open rubble.
4) Improvement of the victim accommodation
mechanism.
5) Improvement of the mechanism of prevents
Crush Syndrome.
6) Improve maneuverability.
7) Improve Safety.
Importantly, 3), 4), 5), and these quick and
smooth cooperation are very important to rescue
victims.
3.2 Present Status of the Blade
Mechanism to Open Rubble
The first prototype of the Rescue Robot is not
mounted on this blade mechanism. Because we
intended that the Robot will action to collapsed
Japanese-style one-story houses. These are the most
collapsed building in past Japanese earthquakes. But
collapsed Japanese houses still have roofs in many
cases (see Figure 11). So we have supposed that can
lift and go through under the roof, it is enough for
the crawler only.
Figure 11: Collapsed Japanese-style house by Chu-etsu
earthquake.
STUDY AND DEVELOPMENT OF THE RESCUE ROBOT PREVENTING CRUSH SYNDROME OF EARTHQUAKE
VICTIMS
47

However, we found that it is need to lift objects
smaller than roofs, now we designing to the Blade
mechanism make use of 1/5 sized model. Figure 12
is one of the proposed designs
Figure 12: Proposed design of the Blade mechanism.
3.3 Present Status of the Mechanism to
Prevent Crush Syndrome
This mechanism is necessary to directly touch the
living human body, it is requires a very delicate
design. For example, the disaster scene severity,
victim’s body position, place of the affected area,
and so on.
Figure 13 is the latest proposed design of the
mechanism to prevent Crush syndrome.
Figure 13: Proposed design and its procedures of “Two-
step inflates method”.
The advantage of this method will not have to
touch the victim directly by the mechanical arm.
And it can make the mechanism simply, and thus it
can be expected to improve reliability.
However, we will have to conduct a detailed
examination, including the shape of Cuff that can
prevent Crush syndrome effectively or not.
In the future, we will produce the new design
mechanism experimentally, after mechanical tests,
give medical tests.
4 CONCLUSIONS
In this study, we produce the first 1/1 sized
prototype model.
In the future, we are planning to make
mechanical improvements using 1/5 and 1/1 sized
models. At the same time, we will start to make
medical tests (top priority is Crush syndrome) using
1/1 sized prototype.
But many issues still remain to perform medical
tests before.
This robot was born from the needs of
experience in an actual disaster medicine. In order to
prepare for next big earthquake, we will do the
research and development as soon as possible.
ACKNOWLEDGEMENTS
I received generous support from member of
Disaster ME Conference and Fukumoto Lab.
Especially, Ms. Wen-Hsin Lin and Mr. Tomoyuki
Fujiki, They gave me a grateful help to my poor
English language skill.
In addition, a part of this work was supported by
International Risk Management Program 2006 by
The Japanese Ministry of Health Labour and
Welfare.
REFERENCES
Tadokoro, S., 2010. 28(2), 134-137. Journal of the
Robotic Society of Japan. The Robotic Society of
Japan.
Sahashi, T., Sahshi, A., Uchiyama, H., Fukumoto, I., 2010.
212. Program Book of 10
th
APCDM. The 10
th
Asia
Pacific Conference on Disaster medicine.
Fukumoto, I., 2010. OS-2-2. Program &Abstracts Book
(DVD). Conference of Japanese Society for Medical
and Biological Engineering.
ICINCO 2011 - 8th International Conference on Informatics in Control, Automation and Robotics
48

Sahashi, A., Sahashi, T., Uchiyama, H., Fukumoto, I.,
2010. 3-4. Proceedings of the 29th JSMBE Kou-Shin-
Etsu Branch Conference 2010. Japanese Society for
Medical Biological Engineering.
Sahashi, T., Sahshi, A., Uchiyama, H., Fukumoto, I., 2010.
3G1-7. Proceeding of the Robotic Society of Japan
(DVD). The Robotic Society of Japan.
Tsuchiya, S., Tatano, H., Okada, N., 2008. (10), 355-364.
Proceeding of Institute of Social Safety Science.
Institute of Social Safety Science.
Sahashi, T., Sahshi, A., Uchiyama, H., Fukumoto, I., 2009.
Program Book of 9
th
APCDM. The 9
th
Asia Pacific
Conference on Disaster medicine.
Fukumoto, I., 2008. 13(2). 218-225. Japanese Journal of
Disaster Medicine. Japanese Association for Disaster
Medicine.
Higuchi, N., 2008. 63(3), 382-384. Japanese Journal of
Radiological Technology. Japanese Society of
Radiological Technology.
Mahoney, E, L., Whiteside, F, D., Belue, E., Mortisugu, P,
Kenneth., Esch, H, V., 1987. 16(3), 354-358. Annals
of Emergency Medicine. Journal of the American
College of Emergency Physicians. The American
College of Emergency Physicians.
Ensaria, C., Tüfekçioglub, O., Aylia, D., Gümüsc, T.,
Izdesc, S., Turanlid, S., 2002. 92(4), 941–943.
Nephron journals. Karger AG.
Greaves, I., Porter, K,M., 2004. 12(1), 47-52. Accident
and Emergency Nursing. Elsevier Ltd.
Demirkiran, O., Dikmen, Y., Utku, T., Urkmez, S., 2003.
20, 247-250. Emergency Medicine Journal. BMJ
Publishing Group Ltd.
STUDY AND DEVELOPMENT OF THE RESCUE ROBOT PREVENTING CRUSH SYNDROME OF EARTHQUAKE
VICTIMS
49
