
DEVELOPMENT OF A SIT-TO-STAND ASSISTANCE SYSTEM
FOR PARKINSON'S DISEASE SUFFERERS
(Intellectual Handrail)
Osamu Nitta, Yasunari Fujimoto, John Surya
Tokyo Metropolitan University, 2-10-7 Higasiogu, Arakawa-ku, Tokyo, Japan
Yoshiyuki Takahashi
Toyo University, Faculty of Human Life Design, Oka 48-1, Asaka-shi Saitama 351-8510, Japan
Keywords: Parkinson's Disease, Assistance System, Stand Up, Handrail, Force Plate.
Abstract: A Sit-to-Stand Assistance System that can provide functional assistance in standing was developed. Two
650 mm stroke AC servo motor driven linear actuators were squarely combined. The handrail was installed
at the intersection of these actuators. When the user stands from a chair, the handrail leads the user’s
motion. A personal computer (PC) is used to control the handrail motion, and force plates are placed under
the feet. In this experiment the subjects were Parkinson's disease (PD) sufferers. Subjects were not able to
stand up with a fixed handrail; however, they were able to stand up using this system without help.
1 BACKGROUND
Handrails are effective welfare tools that can provide
assistance, such as walking and lifting motion, to the
elderly and disabled. In addition, handrails are
becoming widely used in many homes, and they
have become the most basic item installed in house
renovation. Previous research studies have also
shown handrails are mostly used in restrooms, stairs,
and bathrooms (Oshima et al., 2000; Takashima et
al., 2005). To be used as a welfare tool in a house, it
is necessary to fix the handrail onto the wall.
Therefore, it is not easy to reposition a handrail
once it is fixed onto a wall. Previous handrail studies
have focused primarily on finding what were the
most suitable shape and placement of a handrail.
However, a handrail that can give assistance in
standing and guiding posture has not been
investigated.
Standing-support welfare devices, such as "rising
toilet seat" "rising chair" "rising wheelchair" have
been already developed (Kamnik et al., 2005; Chugo
et al., 2005; Uplift Technologies Inc.; TOTO LTD.).
However, these devices give too much unnecessary
assistance. Moreover, each individual user’s
symptoms, standing pattern, and degree of physical
decline are varied. Naturally, these conventional
standing-support devices cannot accommodate all
these differences. It also should be pointed out that
these devices which tend to lift the entire body
“unnaturally” may unnecessarily promote physical
strength decline.
2 PURPOSE
The purpose of this research was to develop an
intelligent handrail that can give assistance in
standing to PD patients and the elderly whose
physical function has decreased. The motion of the
handrail is guided by the user’s posture, which is
calculated from the 6 axes power sensors, placed on
the handrail, and the ground reaction force sensors.
In this manner, the motion of the handrail is
synchronized with the user’s posture while standing.
In our previous studies, a handrail that could give
assistance to users in standing was developed. (Nitta
et al.; Daisuke et al., 2007).
It consists of two linear actuators which are
crossed at right angles (Fig1). The handrail was
installed at the intersection of these actuators. In this
study, the development of this handrail was
advanced further by the development of a control
program.
189
Nitta O., Fujimoto Y., Surya J. and Takahashi Y..
DEVELOPMENT OF A SIT-TO-STAND ASSISTANCE SYSTEM FOR PARKINSON’S DISEASE SUFFERERS - (Intellectual Handrail).
DOI: 10.5220/0003709701890192
In Proceedings of the International Conference on Bio-inspired Systems and Signal Processing (BIOSIGNALS-2012), pages 189-192
ISBN: 978-989-8425-89-8
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

6-axis force sensor
Hand Rail
Linear Actuator
(X axis)
Frame
Linear Actuator
(Y axis)
Figure 1: A handrail that could give assistance to users in
standing.
3 METHOD
The effect of this control program, a trajectory
generator device placed on the handrail, on standing
movement of PD patients was investigated. In
measuring the force that will be exerted on the
handrail, the center of gravity trajectory, angle of the
body, knee joint torque, load on the body at the time
of standing, and the stability of the center of gravity
were evaluated. In this manner, what would be an
effective trajectory was investigated. In addition, the
research aimed to compare the standing movement
of two healthy adults with two PD subjects.
The average height of the two PD subjects is
1.60 (sd0.03)[m], and their average weight is 48.5
(sd5.5)[kg].The severity of their Parkinson's disease
was stage 4 on Hoehn Yahr scale. Using a
conventional handrail, it was not possible for the two
PD subjects to stand.
Figure 2: 14 optical markers.
As for the healthy adults, their average height is 1.73
(sd0.01)[m], and average weight is 70.5 (sd1.5)[kg].
The subjects were positioned on a height-adjustable
stool. The initial lower limb posture was as follows:
hip flexed 90 degrees and knee flexed 80 degrees.
The trajectory generator of the handrail was
based on the ground reaction force data. The value
of the vertical reaction force, derived from the right
and left feet force plates, changes the trajectory of
the handrail at a certain threshold. For this
experiment, the following values 50[%], 70[%],
80[%] of the subjects’ weight were assumed to be
the thresholds. All subjects were subjected to the 3
thresholds. Healthy subjects did not use this
intelligent handrail; however, they were told to stand
slowly and statically
Each subject executed the experiment 2 times.
As shown in Figure 2, a total of 14 optical markers
were placed on the subjects (the head of the 5th
metatarsal bone, lateral malleoluses, knee joints, hip
joints, shoulders, top of the head, elbow, and wrist)
and the handrail (the edge). Vicon motion analysis
system (Oxford Metrics Company) was used for the
measurement of the location of these body markers.
6 axes power sensors (Nitta Company) were placed
on the handrail and measured the power exerted on
the X-axis and Y-axis of the handrail.
Each set of vertical reaction force was
established from the left and right feet force plates
and the sampling frequency was set to 30Hz. Then,
the angle of the hip joint, the location of the center
of gravity, and the knee joints torque were
calculated. For the PD subjects, measurement was
conducted from the beginning to the end of the
handrail movement. While the healthy adults were
measured from the start of standing until the
acromion marker stopped. Each segment of standing
time, from start to finish, was divided, and the
standing ratio time was established. When it is
established that the power of the Y-axis of the
ground reaction force, under the chair became 0[N],
this indicates the point when hip is off the seat
4 RESULTS
Figure 3 shows an example of the handrail trajectory
of the PD subjects. The starting point (0) is the
initial position of the handrail. Among the 3
thresholds, the 80[%] threshold has the furthest
trajectory. Figure 4 shows the center of gravity
trajectory at the time of standing. The starting
position (0) is when standing movement starts.
In addition, the distance from the starting point is
normalized by the height of the subjects. In healthy
adults, the center of gravity, initially, advances
obliquely downward. Thereafter, it advances upward
curvilinearly. In the PD subjects, when the threshold
was set at 50[%], standing was not possible because
BIOSIGNALS 2012 - International Conference on Bio-inspired Systems and Signal Processing
190

Figure 3: Examples of the handrail trajectory.
the center of gravity did not advance sufficiently to
the supporting feet. When the PD subjects were
made to move at 70% threshold trajectory, it was
possible for them to stand; however, the trajectory of
the center of gravity became linear. When the PD
subjects’ center of gravity was compared with the
healthy adults’ center of gravity, the former center of
gravity advanced very little. On the average, the
furthest center of gravity of the PD subjects was
37[%] of their body height. When the threshold is
set at 80[%], the PD subjects could stand by
themselves, and the handrail continued moving
forward.
Figure 4: The center of gravity trajectory at the time of
standing.
The furthest center of gravity location of this time
was about the same with the healthy adults’ value at
the time of standing, which was 54[%] on the
average. Figure 5 shows the knee joint torque of the
PD and healthy subjects in standing.
Knee joint torque extension is indicated by
negative value. A knee joint torque was normalized
by the weight of the subject. The maximum knee
joint extension torque of the healthy adults was
greater in comparison with the PD subjects. When
the threshold was set at 50[%], the knee joint torque
of the PD subjects was smaller than knee joint
torque at other thresholds because the center of
gravity did not shift. In addition, at 70[%], and
80[%], there was a little difference in the knee joint
Figure 5: Knee joint torque of the PD and healthy subjects
in standing.
torque of the PD subjects. Figure 6 shows the power
exerted on the X-axis of the handrail by the PD
subjects. In the case of 50[%], 70[%], 80[%]: At
50[%], power exerted on the handrail was the
greatest.
Figure 6: The power exerted on the X-axis of the handrail
by the PD subjects.
However, at 70[%], 80[%], it was barely discernible.
Figure 7 also shows the power exerted on the Y-axis
of the handrail by the PD subjects. Positive value
indicates subjects are pushing down on the handrail.
At 80[%], the maximum power exerted on the
handrail is almost half the power exerted at other
thresholds. As mentioned above, the handrail
trajectory was calculated from the ground reaction
force. The finding shows that the 2 PD subjects, who
could not stand with conventional handrail, were
able to stand without help by using this intelligent
handrail. Finally, we concluded that the center of
gravity trajectory at 80 [%] threshold is the most
effective because it is similar to a healthy adult’s
trajectory.
5 DISCUSSION
In healthy adults, the center of gravity trajectory
plots a curve after hip is off the seat. Moreover, at
this moment, the body inclines forward and moves
vertically after hip off the seat. In addition, the
DEVELOPMENT OF A SIT-TO-STAND ASSISTANCE SYSTEM FOR PARKINSON'S DISEASE SUFFERERS -
(Intellectual Handrail)
191
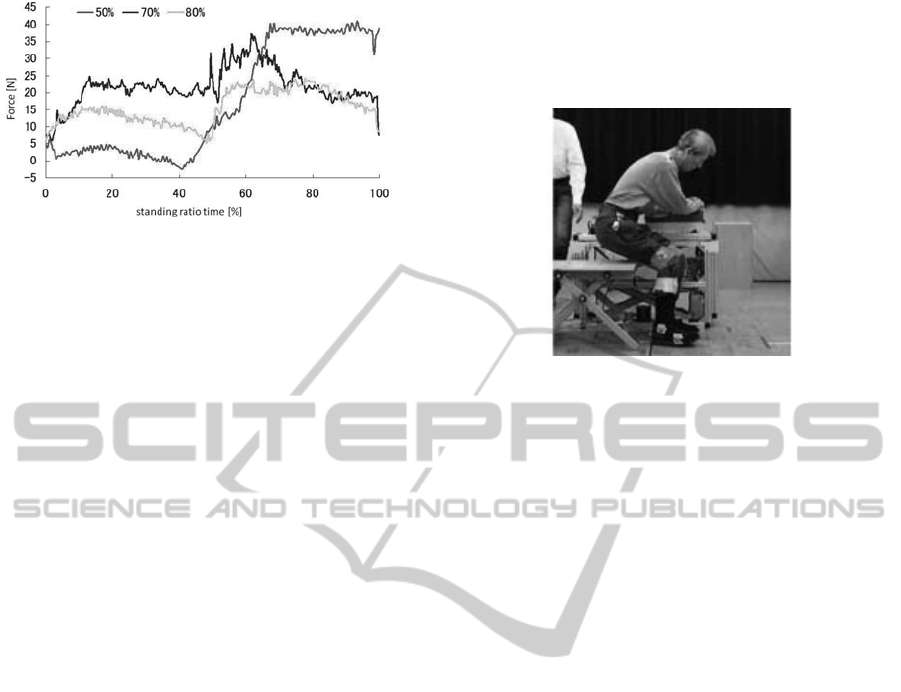
Figure 7: The power exerted on the Y-axis of the handrail
by the PD subjects.
maximum location of the center of gravity was
54[%] on the X-axis, on the average. At this
trajectory, a person is able to stand stably because
posture stability is met. In addition, from this
experiment, it was determined that the maximum
extension torque of the knee joint was
1.19[N*m/kg]. When the PD subjects tried to stand
using the intelligent handrail, standing was not
possible when the vertical reaction force trajectory
was set at 50[%]. This is so because the center of
gravity did not advance sufficiently to the supporting
feet. At 70[%], PD subjects were able to stand.
However, the trajectory of the center of gravity
became linear. It was thought that the timing when
the subject’s body began to move vertically was too
soon. As a result, the handrail began to move
vertically before the subject’s hip was lifted from the
seat. The body’s movement observed here is
different from the standing up movement of a
healthy adult. When the handrail moved vertically,
the center of gravity of the subject is still left behind
the handrail. Therefore, it is thought that the weight
of the subject was exerted on the handrail. Thus, the
power exerted on the handrail was greater than in
other conditions. When the threshold is set at 70
[%], subjects could stand but unstably because too
much load is placed on the upper limbs and the
center of gravity is left behind the supporting feet.
When the threshold was set at 80[%], the PD
subjects’ center of gravity trajectory was similar to
healthy adults’, and thus, standing was possible. The
physical movement resembled a healthy adult’s
movement, in which the body moved vertically after
hip was lifted from the seat. The center of gravity
position of the X-axis trajectory at the time the hip
was lifted from the seat moved to the supporting
feet. In addition, the knee joint torque of the
extension direction became 0.94[N*m/sec] and was
smaller than knee joint extension torque
1.02[N*m/sec], which is typically shown among the
elderly who need assistance, including PD patients.
From this study, it could be suggested that 80[%]
threshold enabled the elderly and disabled
individuals to stand stably. Finally, the application
of this finding is the experimental production of a
small intelligent handrail, shown in Figure 8.
Figure 8: The experimental production of a small
intelligent handrail.
REFERENCES
Oshima T., Ito A., Endo Y., Research of a taste of
“diameter and height” of handrail, Proceedings of
Architectural Institute of Japan, pp.1031-1032.
(2000).
Takashima T., Nakanishi Y., Higaki H., Study of Design
of Handrail, Proceedings of the Japan Society of
Mechanical Engineers, Bioengineering Division,
pp.111-112. (2005).
Kamnik R., Bajd T., Williamson J., Murray-Smith R.
Rehabilitation Robot Cell for Multimodal Standing-Up
Motion Augmentation, Proceedings of the 2005 IEEE
International Conference on Robotics and
Automation, ICRA 2005, pp.2277- 2282. (2005).
Chugo D., Okada E., Kawabata K., Kaetsu H., Aasama H.,
Miyake N., Kosuge K. Force Assistance System for
Standing-Up Motion: 1st Report: Required Assistance
Power for Standing-Up, The JSME Symposium on
Welfare Engineering Vol.2005 (20051207), pp.257-
260. (2005).
http://www.up-lift.com/ (Uplift Technologies Inc.)
http://www.toto.co.jp/ (TOTO LTD.)
Nitta Osamu, Hashimoto Mime, Inoue Kaoru, Takahashi
Yoshiyuki, “Developmental Research of a Power,
Assistance Type Handrail”, The journal of Japan
Academy of Health Sciences, Vol.7, No.3(20041225)
pp. 164-168
Daisuke Karibe, Yasunari Fujimoto, Osamu Nitta, Toru
Yamaguchi, “Developmental Research of Intelligent
Handrail applied movements of standing up”, SICE
SI2007, pp.1192-1193, 2007
BIOSIGNALS 2012 - International Conference on Bio-inspired Systems and Signal Processing
192
