
FRAMEWORK FOR COMPUTER AIDED ANALYSIS OF MEDICAL
PROTOCOLS IN A HOSPITAL
Rene Schult, Pawel Matuszyk and Myra Spiliopoulou
Otto-von-Guericke-University, Universit
¨
atsplatz 2, D-39106 Magdeburg, Germany
Keywords:
Knowledge discovery from medical protocols, Knowledge discovery from anesthesia protocols, Knowledge
discovery, Data mining, Healthcare information systems.
Abstract:
We study the potential of analyzing medical protocols with data mining methods for resource planing.
Background. Medical protocols can be exploited in several resource planing applications, such as optimizing
occupancy of surgery rooms or scheduling teams for surgery operations. Literature has identified many vari-
ables that can be used to predict resource demand; some of them can be extracted from medical protocols.
Contribution. We propose a high-level framework for knowledge discovery from medical protocols, and
present a first instantiation in a German hospital. We report on the findings of this instantiation for the task of
predicting surgical room occupancy time.
1 INTRODUCTION
Hospitals are increasingly facing the demand for ef-
ficient resource planing, not least in response to eco-
nomic recession and demographic evolution. Of par-
ticular interest is the efficient management of re-
sources needed for expensive types of treatment, such
as intensive care, and of resources with high demand,
such as surgical rooms. Eijkemans et al. point out that
more than 60% of hospital patients undergo some sur-
gical treatment (Eijkemans et al., 2010). So, there is
need for methods for predicting and optimizing occu-
pancy of surgical rooms and intensive care units.
Medical protocols encompass information that
can be used to improve room planing. Eijkemans et
al. have identified several predictive variables for ”op-
eration time” (Eijkemans et al., 2010); some of these
variables are routinely recorded in anesthesia proto-
cols. In this study, we consider these protocols for
the prediction of surgery room occupancy time (”SRO
time”), which we define as the elapsed time between
the entry of the patient to the operation room until
the exit moment. This is equivalent to ”operation
time” in (Eijkemans et al., 2010), but we pertain to
the more explicit ”SRO time”, because in some hos-
pitals (including the one we studied) patients occupy
the surgery room until they wake up from anesthesia.
Predictive variables can serve as aid to resource
planers. However, the variables recorded vary among
hospitals. Recording all desirable variables may re-
quire process redesign and thus incur additional costs.
Hence, it is necessary to exploit the predictive power
of available variables to the largest possible extent.
To this purpose, we propose a lightweight frame-
work for knowledge discovery from medical proto-
cols and report on its use for prediction of resource
demand. The overarching idea is that the frame-
work should allow a reporting or prediction task to
be plugged into existing processes, without requiring
process modifications nor additional activities from
the medical staff. We report on a first instantiation
of our framework in a hospital for the analysis of in-
tensive care unit protocols and anesthesia protocols.
We show how knowledge discovery from anesthesia
protocols can lead to better prediction of SRO time;
the full report is in (Schult et al., 2011).
In section 2 we discuss related work. In section
3, we describe our framework at an abstract level; in
section 4 we present its instantiation in a hospital on
two types of medical protocols. Findings on the pre-
diction SRO time from anesthesia protocols are sum-
marized in section 5. Section 6 concludes our study
with lessons learned and planed next steps.
2 RELATED WORK
The importance of information technology in the
health care industry is reflected in increasing invest-
ments in appropriate IT systems (Wilson and Tulu,
225
Schult R., Matuszyk P. and Spiliopoulou M..
FRAMEWORK FOR COMPUTER AIDED ANALYSIS OF MEDICAL PROTOCOLS IN A HOSPITAL.
DOI: 10.5220/0003776702250230
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2012), pages 225-230
ISBN: 978-989-8425-88-1
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)
2010). Avison and Young point out that decision sup-
port systems are one important application in health
care information systems (Avison and Young, 2007),
while Combi et al. stress the importance of times-
tamped data for reasoning, e.g. for clinical diagnosis
and for devising care plans (Combi et al., 2010).
Reasoning, prediction and other forms of decision
support require generic frameworks that allow for the
particularities of each hospital. For example, con-
sider prediction of surgery room occupancy: Dex-
ter et al. report that the average duration of a given
surgery between the second-fastest and the second-
slowest clinic they investigated may differ by up to
50% (Dexter et al., 2006). This implies that predictive
models must be learned for each hospital, on the data
recorded in this hospital. Accordingly, we propose a
framework at a high level of abstraction, and we show
how its instantiation in a German hospital lead to the
exploitation of medical protocols for prediction.
3 FRAMEWORK FOR MEDICAL
PROTOCOLS IN DECISION
SUPPORT
We propose a framework for decision support on the
basis of medical protocols. The main purpose of these
protocols is to store all medical activities that refer to
a patient of a hospital. They are essential for the pa-
tient’s treatment, but also for accounting and billing,
for resource management and planing, and for audit-
ing. They can also be used for scientific research,
studies on new treatments and medication, and for the
analysis and optimization of internal processes.
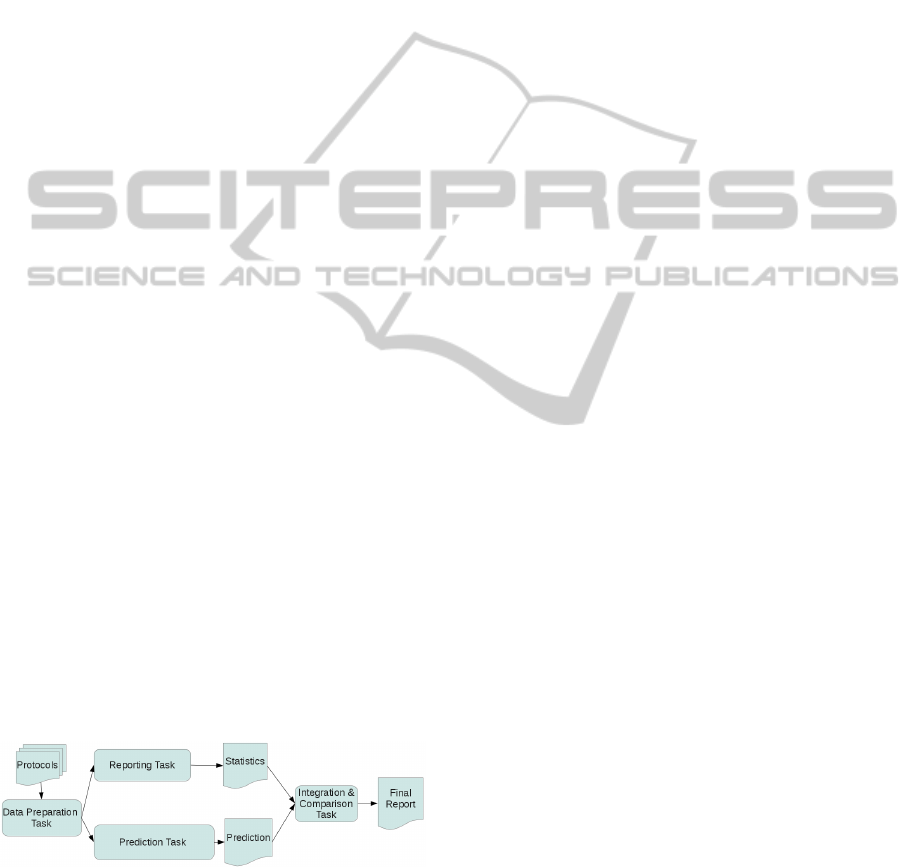
In our framework, we consider medical protocols
for decision support in resource management, and an-
ticipate two core tasks - reporting on resource use, and
predicting resource use. For prediction we focus on
(supervised) data mining methods. All tasks we an-
ticipate are depicted in Figure 1 and described below.
Figure 1: Framework for reporting and analyzing medical
protocols for decision support.
There are different types of medical protocols
that can be used as input to our framework, such
as anesthesia protocols or intensive care unit proto-
cols; they are compiled by different members of the
medical staff, are incorporated in different processes,
and intended for different recipients. This affects the
contents of the protocols, the number of variables
recorded and the format used. Some protocols have
the form of a single record per patient, while oth-
ers adhere to the entity-attribute-value model (Stead
et al., 1983) and consist of several records per patient
– one per variable of interest for this patient. These
differences influence the prediction task, and must be
dealt with during data preparation.
Data Preparation Task. This task involves algo-
rithms that prepare the data for reporting and for data
mining. Conventional data preparation tasks include
finding and handling missing values and errors in the
data, detecting correlations between variables, and
determining the target variable for the subsequent pre-
diction task, depending on the problem at hand. There
are many statistical tools and also mining algorithms
available for such purposes; in our experiment (Sec-
tion 5) we report on those we used for our instantia-
tion to predict SRO time.
Less conventional data preparation is needed to
transfer data from the entity-attribute-value model to
a format that can be used by mining algorithms. We
elaborate more on this issue in Section 4.
Reporting Task. This task involves utilities for data
querying and summarization, as provided convention-
ally with a database management system or data ware-
house. The concrete information to be reported de-
pends on the objective of decision support. For ex-
ample, optimizing surgery room occupancy (SRO) re-
quires an overview of SRO times for different vari-
ables, such as type of surgical treatment, patient age
etc. Relevant variables are listed in (Eijkemans et al.,
2010), but the contents of the output report Statistics
depend obviously on the variables recorded in the pro-
tocols used. In our instantiation (Section 4), we used
anesthesia protocols.
Prediction Task. This task involves data mining al-
gorithms, as provided by commercial suites or open
source tools (free for research purposes). Prediction
can run independently of the reporting task, but often
reporting precedes prediction: some reports can pro-
vide insights on predictive variables.
The algorithms used depend obviously on the con-
crete objective for decision support. In our instanti-
ation, we wanted to predict discrete SRO time slots
(”bins”) rather than exact SRO time, since surgery
rooms are rather occupied in time slots than up to the
minute. is more interessting as the prediction of the
concrete time. For the prediction of values of a con-
tinuous variable, regression methods should be used,
while the prediction of discrete values requires classi-
fication algorithms.
HEALTHINF 2012 - International Conference on Health Informatics
226

The prediction task involves specification of the
target variable and of appropriate evaluation criteria.
Prediction requires training, tuning and comparing
several learners, before a learner (or an ensemble) is
chosen to be used for the prediction over unknown
data. In our experiment (cf. Section 5), we compared
several classifiers, but we also compared data prepara-
tion algorithms, because they turned to influence clas-
sifier performance.
Integration and Comparison. This task involves
placing the report (from the reporting task) and the
results of the prediction task together, including vi-
sualizations. The tools needed here are usually part
of the suites appropriate for the Prediction, resp. the
Reporting task. Integration serves foremostly the jux-
taposition of findings acquired from reports via sim-
ple statistics and querying, and those acquired by ma-
chine learning. The final report serves as basis for a
human decision maker for planing, or as input for a
simulation tool that may consider different resource
planing scenaria. In the long term, comparison also
concerns the juxtaposition of a predictor learned some
time back with newer data; changes in healthcare pro-
cesses or external factors may require re-learning of
predictive models.
In the next two sections, we discuss an instantia-
tion of our framework in a German hospital for inten-
sive care unit protocols and anesthesia protocols, and
summarize our insights from applying our framework
to predict SRO time.
4 INSTANTIATION OF THE
FRAMEWORK IN A GERMAN
HOSPITAL
We present an instantiation of our framework for
knowledge discovery in a German hospital. We study
two types of medical protocols recorded from 2007
till 2009, namely intensive care unit protocols and
anesthesia protocols. As pointed out in section 3, such
medical protocols are typical inputs to our framework.
We first describe briefly the challenges and potentials
of using intensive care unit protocols for knowledge
discovery. Then, we focus on anesthesia protocols,
which we use for the prediction of surgery room oc-
cupancy time (SRO time, cf. Section 1). Our experi-
ment on these protocols is described section 5.
4.1 Intensive Care Unit Protocols
An intensive care unit protocol contains data on the
treatment of a patient in an intensive care unit. Such
data include diagnosis and medication. Special em-
phasis is put on the patient’s vital signs, e.g. body
temperature, pulse and blood pressure, which have to
be monitored constantly.
The data stored in intensive care unit protocols
are very complex: depending on the patient and the
treatment, different variables must be stored. Given
the limitations of database systems with respect to
the maximum number of columns in a table, Stead et
al. proposed to use the entity-attribute-value model
(Stead et al., 1983), where the entity is the patient
identifier, and (attribute, value)-pairs contain the spe-
cific variables and values to be stored for this patient.
This model was used for the intensive care unit proto-
cols in our instantiation, whereby an identifier and a
timestamp was added to each record.
The entity-attribute-value model is not appropri-
ate for data mining. The reason is that a data mining
algorithm requires that all values belonging to one in-
stance (here: one patient of the intensive care unit) be
in one record, so that the algorithm accesses and anal-
yses all attributes of the record together. In contrast,
under the entity-attribute-value model the values be-
longing to one patient are spread over time and stored
separately, as if they belonged to different stays and
treatments of the patient. Hence, the data of each in-
tensive care unit protocol must be collected and inte-
grated into a single record. However, since there is a
large number of possible attributes but only a few are
recorded for each specific patient, the density of infor-
mation for each patient could be too low for learning.
One solution to this problem could be the follow-
ing: group protocols for which the same attributes
have been recorded (preparation task), perform re-
porting and knowledge discovery on resource de-
mand, such as bed occupation or drug utilization,
for each group separately (reporting task / prediction
task), and then integrate the findings of the groups
into a report (integration and comparison task).
4.2 Anesthesia Protocols
An anesthesia protocol contains an exact description
of all anesthetic activities performed during a surgical
treatment. Among the data contained in such a proto-
col are involved personnel, important time points (e.g.
time point of the incision and of the end of a surgery),
and data about medication.
In the hospital of our study, these data were
recorded by an anesthetist during the surgery, us-
ing the Anesthesia Information Management System
(AIMS) NarkoData. NarkoData contains all data as-
sociated to anesthesia during the whole anesthesia
process, including drugs, laboratory results, relevant
FRAMEWORK FOR COMPUTER AIDED ANALYSIS OF MEDICAL PROTOCOLS IN A HOSPITAL
227

vital signs, as well as data on the attributes specified
by the German Society of Anesthesiology and Inten-
sive Care Medicine
1
(DGAI, 1993). NarkoData also
contains data from the hospital information system,
including data on patients and medical staff. Patient’s
attributes are age, weight and body size, disease ac-
cording to the ICD Classification (WHO, 2011), phys-
ical status according to the ASA-Classification, and
type of anesthesia. Information on medical staff is
limited to the identifiers of surgeons and anesthesists.
This allows us to distinguish among staff members
without disclosing personal information.
The time points recorded in the anesthesia proto-
cols are very important: they can be used to predict
the duration of future, similar surgical treatments. In
the next section, we present the findings of the frame-
work’s instantiation in the German hospital for the
prediction of SRO time using anesthesia protocols.
We discuss the concrete activities of
data preparation (Section 5.1) and learning (Sec-
tion 5.2), including results and lessons learned. Sec-
tion 5 is a summary of (Schult et al., 2011), where all
details can be found.
5 KNOWLEDGE DISCOVERY
EXPERIMENT ON
ANESTHESIA PROTOCOLS
The goal of knowledge discovery from anesthesia
protocols in the hospital under study was to learn a
model that predicts the SRO time of future surgery
treatments better than the current baseline. This in-
volved an instantiation of the data preparation task
and of the prediction task (cf. Figure 1). In our
experiment, we consider three discretization meth-
ods for data preparation, and four classification algo-
rithms for prediction, and we compare the quality of
the models learned by the twelve combinations.
Our target variable is a discretized version of SRO
time. As described in section 1, we define ”SRO time”
as the elapsed time between entry and exit of the pa-
tient to/from the surgery room. We thus cover hospi-
tals that do not have a separate room where patients
stay after surgery until they wake up.
We discretize SRO time for learning, because
room occupancy plans deliver time slots (equiv. bins)
rather than exact values. The size of the bin affects
prediction, so we experimented with different binning
methods in the data preparation task described below.
1
DGAI: Deutsche Gesellschaft f
¨
ur An
¨
asthesiologie und
Intensivmedizin
For the evaluation, we compare our models to a
baseline predictor ICDavg: for each class of surgery
according to the ICD classification (WHO, 2011), IC-
Davg finds all protocols refering to treatments of this
class, adds their SRO times and computes the aver-
age. Then, for each anesthesia protocol in the testset,
ICDavg identifies the ICD class of the treatment and
returns the corresponding SRO time average.
To compare our models to ICDavg, we map back
the predicted bin of SRO time to the mid value of the
bin (e.g. a bin of 90 min is mapped to 45 min). Then,
we define a function that computes the Cumulation of
Absolute Differences between true and predicted SRO
time (SROCD) for the whole period of study. The
lower the SROCD, the higher is the model’s quality.
5.1 Data Preparation
The data preparation task in our instantiation for SRO
time prediction involved following activities: (a) in-
corporation of the surgeonID in each record, (b) com-
putation of the SRO time per record and (c) discretiza-
tion of the SRO time into a fixed set of intervals/bins,
so that the SRO time bin becomes the label to be pre-
dicted in the prediction task.
The incorporation of the surgeonID into the anes-
thesia protocols is important because this variable is
predictive (Eijkemans et al., 2010). However, some
surgical treatments involve more than one surgeon,
so that the incorporation of the identifier transformed
one protocol (from the originally 33,862 anesthesia
protocols) into multiple records, whenever multiple
surgeons were participating. This was not a prob-
lem for our experiment, because the duplicates were
considered both by the baseline and by each learner.
However, in a real scenario, a more elaborate ap-
proach is needed for the incorporation of multiple
identifiers of surgeons into a single record.
The computation of the SRO time of each pro-
tocol is performed by using the timestamps and is
fairly straightforward. For discretization, one may
provide the target number of bins as input, or con-
sider methods that both estimate this target number
and do the binning. Since there are cases where the
latter type of methods is not of advantage (see sec-
tion 5.2), we propose following approach, under the
assumption of representative data, to specify the tar-
get number of bins: generate bins for different input
numbers, learn a classifier for each number of bins,
compute the SROCD, and identify the moment of sat-
uration of the SROCD curve.
To test this approach we have experimented in
(Schult et al., 2011) with the discretization methods
(i) Equal Width Interval Binning (EWIB) that parti-
HEALTHINF 2012 - International Conference on Health Informatics
228
tions the SRO times in the anesthesia protocols into
bins of equal size, and (ii) K-Means that groups sim-
ilar SRO times into K clusters, whereby each group
becomes a bin. Unlike EWIB, K-Means builds bins
that are not necessarily of equal width.
Figure 2 depicts the SROCD curve of a J4.8 de-
cision tree classifier upon bins computed with EWIB:
the curve does converge. The saturation is on 50 bins,
the same value was found when using K-Means in-
stead of EWIB. Hence, we can use this experimental
approach to determine the number of bins, provided
that the data set is representative. Anesthesia proto-
cols are recorded anyway for each surgical treatment,
so representative samples can be drawn from them.
●
●
●
●
●
●
●
●
●
●
2 5 10 20 50 100 200
1500000 2000000 2500000
Number of classes
SROCD (in minutes)
Figure 2: SROCD (in minutes) of a decision tree learner
(J4.8) for K = 2, . . . , 200 bins; the contents of a bin for each
value of K was computed with EWIB.
5.2 Prediction
In our instantiation, prediction translates into a clas-
sification task, because the target variable (SRO time)
has been discretized. It is essential to define a baseline
and to study how different learners behave in compar-
ison to this baseline. Then, for the operative task of
prediction on new, unlabeled data, the best model or
an ensemble of learned models should be used.
As baseline we used the ICDavg described at the
beginning of this section: it computed an expected ac-
cumulated SRO time of 1,279,567 minutes. We com-
pared it to Na
¨
ıve Bayes, to the ID3 decision tree clas-
sifier of (Quinlan, 1986), to the J4.8 Java implemen-
tation (Witten and Eibe, 2005) of C4.5 (a successor of
ID3), and to a random forest (Ho, 1995) - an ensemble
of decision trees. For all learners we performed 10-
fold cross validation. For binning, we used K-Means
and EWIB (K = 50 bins), and the Tree-Based Unsu-
pervised Bin Estimator TUBE of (Schmidberger and
Eibe, 2005), which estimates the number of bins. Pa-
rameter settings can be found in (Schult et al., 2011).
The lowest SROCD value (882,513 minutes) was
achieved by ID3 after binning with K-Means. How-
ever, ID3 classifiers abstain from classifying some
records in the test set, hence it is inferior to the learn-
ers build by the other algorithms, which assigns la-
bels to all records. The overall best performance is
achieved by Random Forest with 15 trees (910,383
minutes), and the second best by J4.8 (1,073,231 min-
utes), in both cases after binning with K-Means. The
single tree of J4.8 improves the baseline by 16.2%.
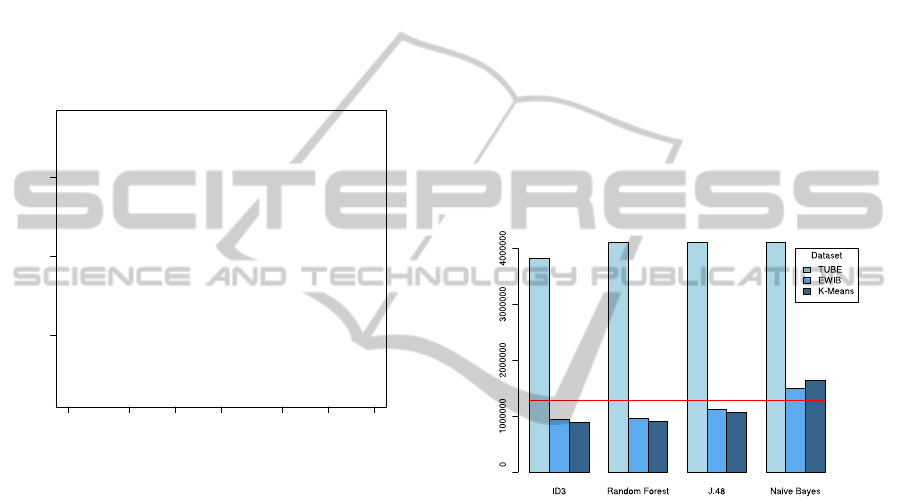
An overview of the results is given in Figure 3.
The horizontal line is the SROCD value achieved by
the baseline ICDavg; of interest are only predictors
that achieve lower SROCD, i.e. improve the baseline.
For each learner, we depict the performance achieved
by each binning method. We see that TUBE leads
to worst performance, K-Means to best performance,
EWIB being only slightly inferior to it.
SROCD (in minutes)
Figure 3: SROCD values for each classification algorithm
(X-axis) combined with each binning method (legend); the
baseline ICDavg is depicted as horizontal line. Lower val-
ues are better, and only values below the baseline corre-
spond to an improvement in predictive power.
In classification tasks, it is usual to evaluate on ac-
curacy. In Table 1, we juxtapose accuracy to SROCD
for Na
¨
ıve Bayes (worst SROCD) and J4.8 (second
best SROCD), considering each binning method. The
juxtaposition shows that accuracy is inappropriate for
the task at hand, as it behaves contrary to SROCD. In
particular, we see that both learners achieve best ac-
curacy under TUBE, but much poorer SROCD values
than under EWIB or K-Means. In contrast, the accu-
racy under EWIB and K-Means is very low.
This is an artifact that may lead the decision
maker to wrong conclusions, so we explain it here:
EWIB and K-Means produced 50 bins, distributing
records evenly among them. TUBE produced 99 bins,
but most of the records were placed in only 3 of
them. Hence, under TUBE, the classifiers essentially
learned to distinguish among three labels/bins. The
FRAMEWORK FOR COMPUTER AIDED ANALYSIS OF MEDICAL PROTOCOLS IN A HOSPITAL
229

Table 1: Impact of binning method on the performance of the classifiers learned by Na
¨
ıve Bayes (NB) and J4.8: performance
is measured as accuracy (higher values are better) and SROCD (lower values are better). Accuracy is an ill choice for the task
at hand, because it shows bias to the number of labels and to the distribution of the data among the labels.
Binning method # bins Accuracy (in%) SROCD (in min)
NB J4.8 NB J4.8
EWIB 50 21.23 41.11 1,488,230 1,120,729
K-Means 50 14.39 35.41 1,639,846 1,073,231
TUBE 3+96 82.12 88.01 4,099,064 4,111,336
prior probability of a miss (wrong label assignment)
is higher if there are 50 labels than if there are only
three. Accuracy is sensitive to the number of labels,
so it is an ill choice if classifiers are learned with dif-
ferent numbers of labels or with a strong bias towards
only a few labels.
Summarizing, the instantiation of the prediction
task for the hospital resulted in predictors that im-
proved the baseline. Among the lessons learned are
the impact of discretization on the learners and the
importance of selecting a proper evaluation measure.
6 CONCLUSIONS
We presented a high-level framework for knowledge
discovery from medical protocols, and its instantia-
tion in a German hospital for the prediction of surgi-
cal room occupancy time (SRO time). Such data are
primarily recorded for medical purposes , but can be
used to support planing decisions, too, provided they
are appropriately prepared and analyzed.
In the instantiation of our framework in a German
hospital we studied intensive care unit protocols and
anesthesia protocols. Instantiation on the former is
still under data preparation, since the intensive care
units’ data were in a format not yet appropriate for
data mining. Anesthesia protocols have been success-
fully analyzed after a preprocessing task that involved
computation and discretization of the target variable
(SRO time). We reported on what steps should take
place during preprocessing and analysis, how differ-
ent algorithms can affect the predicting power of the
learned models, and how they should be compared.
Next steps include the refinement of our frame-
work towards specific activities for decision sup-
port tasks, and instantiations for knowledge discov-
ery from other types of medical protocols, foremostly
from intensive care unit protocols.
REFERENCES
Avison, D. and Young, T. (2007). Time to rethink
health care and ICT? Communications of the ACM,
50(6):69–74.
Combi, C., Keravnou-Papailiou, E., and Shahar, Y. (2010).
Temporal Information Systems in Medicine. Springer.
Dexter, F., Davis, M., Halbeis, C. E., Marjamaa, R., Marty,
J., McIntosh, C., Nakata, Y., Thenuwara, K. N.,
Sawa, T., and Vigoda, M. (2006). Mean operating
room times differ by 50% among hospitals in different
countries for laparoscopic cholecystectomy and lung
lobectomy. Journal of Anesthesia (2006) 20:319–322.
DGAI (1993). Qualit
¨
atssicherung und Datenverarbeitung in
der An
¨
asthesie. Kerndatensatz Qualit
¨
atssicherung in
der An
¨
asthesie. An
¨
asth Intensivmed, 34:331–335.
Eijkemans, M. J. C., van Houdenhoven, M., Nguyen, T.,
Boersma, E., Steyerberg, E. W., and Kazemier, G.
(2010). Predicting the unpredictable: A new predic-
tion model for operating room times using individual
characteristics and the surgeon’s estimate. Anesthesi-
ology 2010; 112:41–9.
Ho, T. K. (1995). Random decision forests. 3rd Int’l Conf.
on Document Analysis and Recognition.
Quinlan, J. (1986). Induction of decision trees. Machine
Learning 1: 81-106, 1986.
Schmidberger, G. and Eibe, F. (2005). Unsupervised dis-
cretization using tree-based density estimation. Lec-
ture Notes in Computer Science, Volume 3721/2005,
240-251.
Schult, R., Matuszyk, P., and Spiliopoulou, M. (2011). Pre-
diction of surgery duration using empirical anesthe-
sia protocols. In The First International Workshop on
Knowledge Discovery in Health Care and Medicine
(KDHCM 2011), pages 66 – 77.
Stead, W., Hammond, W., and Straube, M. (1983). A chart-
less record - is it adequate? Journal of Medicine Sys-
tems, 7:103 – 109.
WHO (2011). World health organization: International
classification of diseases (ICD). http://www.who.int/
classifications/icd/en/.
Wilson, E. V. and Tulu, B. (2010). The Rise of a Health-
IT Academic Focus. Communications of the ACM,
53(5):147–150.
Witten, I. H. and Eibe, F. (2005). Data mining : practical
machine learning tools and techniques. Amsterdam:
Elsevier; San Francisco, CA: Morgan Kaufmann.
HEALTHINF 2012 - International Conference on Health Informatics
230
