
ELECTRICAL STIMULATION OF THE TRANSCUTANEOUS
POSTERIOR TIBIAL NERVE FOR TREATING URINARY
INCONTINENCE DUE TO NEUROGENIC HYPERACTIVE
BLADDER IN MULTIPLE SCLEROSIS
Hellen Orlando Veloso, Karla de Castro Cardoso
State University of Goiás, Goiânia, GO, Brazil
Fabiana S. B. Perez, Luciana R. Tenório Peixoto
School of Medicine, University of Brasília, Brasília, DF, Brazil
Cristiano Jacques Miosso, Adson F. da Rocha
University of Brasília at Gama, Gama, DF, Brazil
Keywords: Electrical Stimulation, Multiple Sclerosis, Overactive Neurogenic Bladder and Posterior Tibial Nerve.
Abstract: This study evaluates the therapeutic effectiveness of Transcutaneous Electrical Nerve Stimulation (TENS)
of the posterior tibial nerve, for treating urinary incontinence (UI) due to detrusor overactivity (DO) in
patients with multiple sclerosis (MS). Five volunteers having positive cutaneous plantar reflexes and intact
innervation of the anterior tibial participated in the study. Individuals with a positive Babinski reflex were
excluded. We applied 10 sessions of TENS currents (20 Hz, 200 milliseconds, tetrapolar), over a period of 5
weeks (2 sessions per week). The treatment was monitored through a Urogynecology Physiotherapeutic
Assessment Questionnaire and by a Voiding Log. We observed a reduction in the average frequency of
miction, as well as decreased nocturia; also, the urge incontinence symptoms in the treated patients were
cleared up.
1 INTRODUCTION
Multiple sclerosis (MS) is a progressive multifocal
neurological demyelinating condition in the central
nervous system. It is characterized by exacerbations
and remissions, and is prevalent in young adults,
females and Caucasians (Coelho, 2009; Poser, 1986;
Lana-Peixoto, 2002; Grzesiuk, 2006; Mendes, 2000;
Diament and Cypel, 1996; Stephen, 1995). Despite
the unknown etiology of MS, the presence of
autoimmune factors triggering attacks on myelin
have been reported (O-Sullivan, 2004).
The symptomology of MS is multiple and
variable, and it can cause lesions from the medulla
to the cerebral cortex (Poser, 1986). Pyramidal signs
such as spasticity, hyperreflexia and the Babinski
reflex are common in those with MS (Hauser and
Goodin, 2008). The presence of this pathological
reflex indicates lesions on the pyramidal tracts,
compromising voluntary motor control modulation
(Souza and Figueiredo, 1995; Dantas, 1992).
Among the symptoms, sensory deficits and
bladder disorders frequently stand out. Loss of
vibratory perception in the lower limbs, paresthesia,
hypoesthesia, disturbance in position awareness,
dysesthesia, and trigeminal neuralgia hyperpathia
are commonly found among the sensations (O-
Sullivan, 2004). And with the evolution of the
pathology, the urgency or urinary incontinence (UI)
will affect most people with MS (Stephen, 1995).
Around 90% of those with MS display detrusor
hyperactivity (DH). Involuntary contraction of the
detrusor muscle causes the bladder to be filled
incompletely with a constant loss of urine (Coelho,
2009), causing further patient discomfort .
230
Orlando Veloso H., de Castro Cardoso K., S. B. Perez F., R. Tenório Peixoto L., Jacques Miosso C. and F. da Rocha A..
ELECTRICAL STIMULATION OF THE TRANSCUTANEOUS POSTERIOR TIBIAL NERVE FOR TREATING URINARY INCONTINENCE DUE TO
NEUROGENIC HYPERACTIVE BLADDER IN MULTIPLE SCLEROSIS.
DOI: 10.5220/0003792902300233
In Proceedings of the International Conference on Biomedical Electronics and Devices (BIODEVICES-2012), pages 230-233
ISBN: 978-989-8425-91-1
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

Assuming the presence of nerve projections from
the posterior tibial nerve to the bladder, treatment
with TENS may decrease the frequency of UI
(Fischer-Sgrott, 2009). Transcutaneous Electrical
Nerve Stimulation (TENS), an electrotherapeutic
resource used in physiotherapy, uses a low
frequency current, with intensity adjustable from 0
to 50 mA; the wave form is asymmetrical biphasic;
and the used frequency is between 1 and 150 Hertz
(Hz) (Frampton, 1998; Agne, 2004).
The electrodes may be placed on the medial
region of the leg, stimulating motor and sensory
innervation. For someone with MS, sensory
innervation may be compromised, and the
physiotherapist will then adjust the intensity of the
current by observing the motor stimulation in the
muscle. The use of this technique may promote a
decrease in the detrusor’s involuntary contractions
(Maciel and Souto, 2009).
Another resource that the physiotherapist can use
is the visualization of the rhythmic flexions/bending
of the hallux, which indicates that the electrodes are
correctly positioned and confirms preserved motor
innervation (Maciel and Souto, 2009; Amarenco,
2003). However, for individuals positive for
Babinski’s reflex, establishing the appropriate
dosage of the therapeutic current is more difficult,
due to the incorrect motor modulation that they
present. In these cases, it may become impossible to
control the intensity of the current produced by the
electrostimulous device and its motor response.
2 MATERIAL AND METHODS
This study was carried out in the School of Clinical
Physiotherapy at the State University of Goiás
(Goiânia, Goiás, Brazil). The research protocol was
submitted to and approved by the Ethics and
Research Committee at the Federal University of
Goiás. We selected twelve volunteers having UI and
who had been diagnosed with MS. Seven were
female, five were male, six were white, three were
mixed-race or medium dark-skinned and three were
black. After signing the Informed Consent Form, the
individuals were submitted to a Physiotherapeutic
Evaluation questionnaire in Urogynecology from the
Federal University of São Paulo and presented a
Voiding Log for three days. Next, we conducted a
physical exam in order to evaluate the cutaneous
plantar reflex.
Volunteers with no pathological reflex had
electrodes attached along the posterior tibial nerve,
as seen in Figure 1, in order to detect if the
innervation was intact with the use of electrical
stimulation (NEURODYN TENS portable, Ibramed
Ltda.).
Figure 1: Positioning of the electrodes.
Eight individuals presented a normal cutaneous
plantar reflex and a positive response to posterior
tibial nerve electrical stimulation, and were then
included as participants in this study. Three patients
abandoned the study. Five people of both sexes and
aged between 33 and 42 years old were submitted to
10 sessions, twice a week, for 20 minutes of
treatment. The TENS parameters used were: 20 Hz
frequency, a pulse width of 200 milliseconds,
stimulation with two channels with four electrodes
positioned on the lower extremity. One electrode
was fixed to the posterior medial malleolus and the
other was fixed 10 centimeters above this (Figure 1).
The intensity parameter in the individuals with hyper
and normal sensitivity was dosed according to how
the patient felt; in the individuals with
hypersensitivity, the rhythmic flexes of the hallux
motor signal were used as the dosing parameter. The
maximum intensity used was 30 milliamperes, as a
safety criterion in the procedure.
3 RESULTS AND DISCUSSION
The results we present below are based on the
descriptive analysis of data collected by both the
evaluation questionnaires and the voiding log of the
volunteers. Through the physical examination, the
presence of detrusor hyperreflexia (DH) was
observed in all the volunteers.
The main complaints reported by the participants
before the treatment and after the electrical
stimulation treatment appear, respectively, in Table I
and Table II. We observe, based on Table II, an
ELECTRICAL STIMULATION OF THE TRANSCUTANEOUS POSTERIOR TIBIAL NERVE FOR TREATING
URINARY INCONTINENCE DUE TO NEUROGENIC HYPERACTIVE BLADDER IN MULTIPLE SCLEROSIS
231
improvement in the urge incontinence and urine
frequency symptomology after the electrical
stimulation treatment.
Table 1: Description of the main patient complaints before
(F
before
: frequency and P
before
: proportion) and after (F
after
:
frequency and P
after
: proportion) the treatment.
Main Complaint F
before
P
before
(%) F
after
P
after
(%)
Urge Incontinence 3 37.5 - -
Urine Frequency 3 37.5 2 50
Urgency 2 25 2 50
Total 8 100 4 100
We also observed that the sensation of the
voiding act changed after the treatment. In Table II,
we present the list of analyzed sensations, and the
frequency at which they occurred. Observe that there
was a decrease in the frequency of most sensations;
in particular, symptoms such as pain, post-void
desire and urge incontinence were no longer
reported after the treatment.
Table 2: Sensation of the voiding act before (F
before
:
frequency and P
before
: proportion) and after (F
after
:
frequency and P
after
: proportion) the treatment.
Sensation of voiding act
F
before
P
before
(%) F
after
P
after
(%)
Burning 2 18 1 20
Residual sensation
2 18 1 20
Post-void desire 4 37 - -
Pain 1 9 - -
Comfort 1 9 3 60
Urge incontinence
1 9 - -
Total 11 100 5 100
In general, urinary incontinence treatment is
considered effective when episodes of urinary loss
are reduced by 50% (Schreiner, 2009). With respect
to this parameter, involuntary loss of urine onto
clothes was reported by only two patients. From
void log entries, the average loss of urine in these
patients before the treatment was 2 times and after
treatment it was 1 time. This reduction may be
explained by possible neuromodulation caused by
the TENS current.
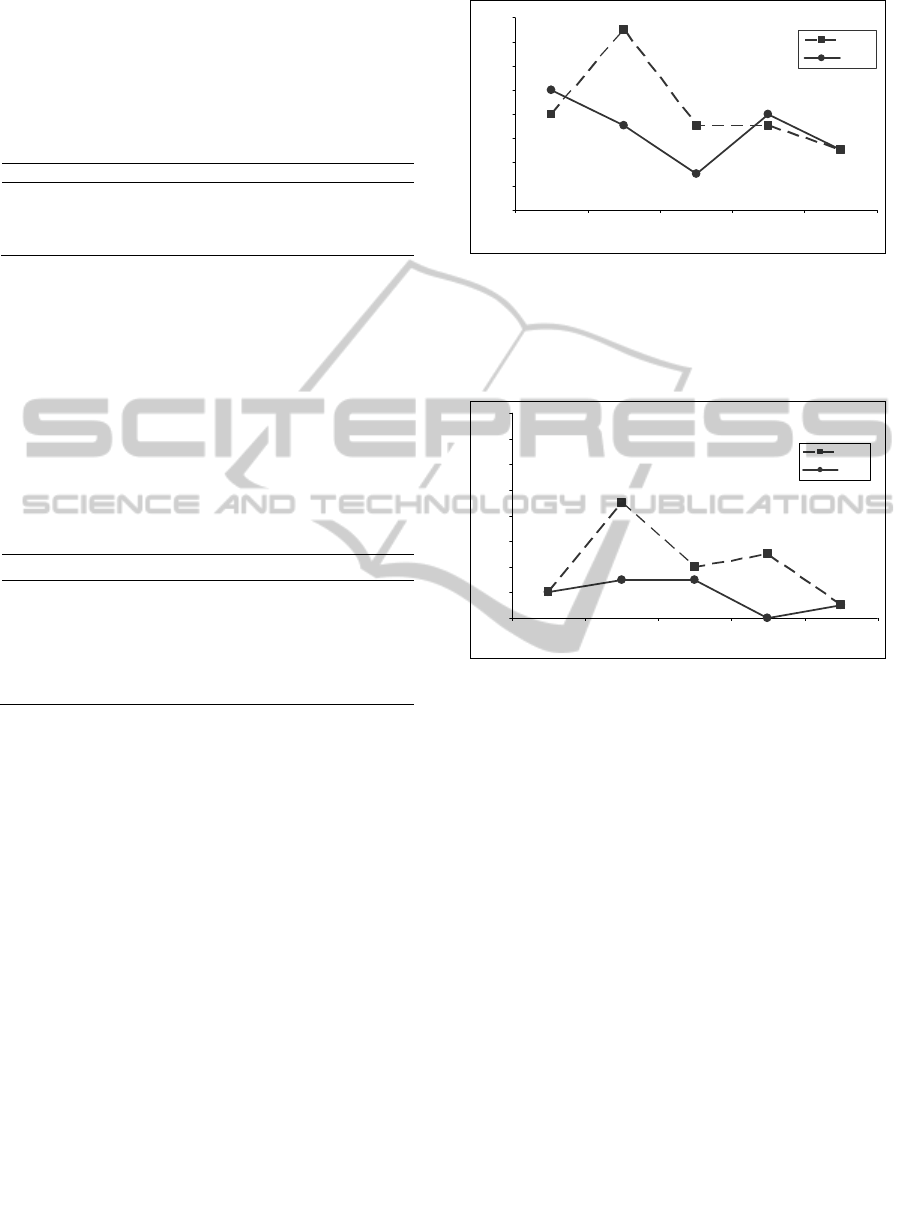
Another analyzed result refers to the reduction in
voiding frequency during the day, as shown in
Figure 2.
The average frequency of visits to the bathroom
at night before the treatment was 4 times, and this
frequency reduced to 2 times after treatment. Studies
about the use of electrical stimulation treatment
suggest a reduction in nocturia, with 38% relief of
this symptom (Marques, 2008), 21% improvement
in nocturnal voiding (Govier, 2001). In a study
involving MS patients, there was an improvement in
nocturia in 75% of patients (Kabay, 2009).
0
2
4
6
8
10
12
14
16
12345
Individuals
Voiding frequency
Before
After
Figure 2: Voiding frequency during the day per
participant.
Finally, we observed an improvement in nocturia
in three patients, as shown in Figure 3.
0
2
4
6
8
10
12
14
16
12345
Individuals
Voiding frequency
Before
After
Figure 3: Voiding frequency during the night per
participant.
4 CONCLUSIONS
Individuals with multiple sclerosis (MS), urinary
incontinence, alteration in the sensitivity and
preserved posterior tibial innervation can safely
receive electrical stimulation treatment. We
evaluated the effect of this treatment on MS patients
with overactive bladders. Our results suggest that
this type of treatment can lead to a decrease in
bladder dysfunction symptoms, and thus improve
this individuals’ quality of life.
REFERENCES
Agne, J. E. Eletrotermoterapia Teoria e Prática. 2ª ed.
Santa Maria: Orium, 2004, 346 p.
Amarenco, G.; Ismael, S. S.; Even-Schneider, A.; Raibaut,
P.; Demaille-Wlodyka, S. Urodynamic Effect of Acute
Transcutaneous Posterior Tibial Nerve Stimulation in
Overactive Bladder. American Urological Association.
BIODEVICES 2012 - International Conference on Biomedical Electronics and Devices
232

v. 109, p. 2215-2215, 2003.
Coelho, M. M. Avaliação Urodinâmica na Esclerose
Múltipla. Acta Urológica, v. 26, n. 3, 2009.
Dantas, H. Do Ato Motor Mental: A Gênese da
Inteligência Segundo Wallon. In: Lataille, Y; Oliveira,
M. K., e Dantas, H. Piaget, Vygotsky, Wallon. São
Paulo. Summer, 1992, p. 37-41.
Diament, A.; Cypel, S. Doenças desmielinizantes na
criança. In: . Neurologia Infantil. São Paulo: Atheneu,
1996. p. 915-938.
Fischer-Sgrott, F. O.; Manffra, E. F.; Junior, W. F. S. B.
Qualidade de vida de mulheres com bexiga hiperativa
refratária tratadas com estimulação elétrica do nervo
tibial posterior. Revista Brasileira de Fisioterapia. São
Carlos, v. 13, n. 6, p. 480-6, nov./dez. 2009.
Frampton, V. Estimulação Nervosa Elétrica Transcutânea
(TENS). In: KITCHEN, S; BAZIN, S. Eletroterapia de
Clayton. São Paulo: Manole, 1998, 350p.
Govier, F. E.; Litwiller, S.; Nitti, V.; Kreder, K. J. Jr,;
Rosenblatt, P. Percutaneous afferent neuromodulation
for the refractory overactive bladder results of a
multicenter study. The Journal of Urology, United
States, v. 165. 2001.
Grzesiuk, A. K. Características Clínicas e
Epidemiológicas de 20 Pacientes Portadores de
Esclerose Múltipla Acompanhados em Cuiabá- Mato
Grosso. Arquivos de Neuro-Psiquiatria, v. 64, n.3,
2006.
Hauser, S. L.; Goodin, D. S. Esclerose Múltipla e Outras
Doenças Desmielinizantes. In: Fauci, M. D. A.;
Brawnwald, M. D. E. Harrison: Medicina Interna. 17ª
ed. Rio de Janeiro: Graw Hill Interamericana Brasil, v.
2, 2008, Cap. 375, p. 2611-2614.
Kabay, S.; Kabay, S.C.; Yucel M.; Ozden, H.; Yilmaz Z.;
Aras O.; Aras B. The clinical and urodynamic results
of a 3–month percutaneous posterior tibial nerve
stimulation treatment in patients with multiple
sclerosis-related neurogenic bladder dysfunction.
Neurourology and Urodynamics, United States, v. 28.
2009.
Lana-Peixoto, L. A. M.; Callegaro, D.; Moreira, M. A.;
Campos, G. B. Consenso expandido do BCTRIMS
para o tratamento da esclerose múltipla. Arquivos de
Neuro-Psiquiatria, São Paulo, v. 60. 2002.
Maciel, L. C.; Souto, S. Estimulação do Nervo Tibial
Posterior (Ptns) no Tratamento da Bexiga Hiperativa.
In: Palma, P. (Ed.). Urofisioterapia: Aplicações
Clínicas das Técnicas Fisioterapêuticas nas Disfunções
Miccionais e do Assoalho Pélvico. 1ª ed. São Paulo:
Unicamp, 2009, Cap. 20, p. 223-227.
Marques, A. A. A eletroestimulação do nervo tibial
posterior no tratamento da bexiga hiperativa.
Unicamp. Campinas, SP: [s.n.], 2008.
Mendes, M. F.; Tilbery, C. P.; Balsimelli, S.; Felipe, E.;
Moreira, M. A.; Barão-Cruz, A. M. Fadiga na forma
remitente recorrente da esclerose múltipla. Arquivos
de Neuro-Psiquiatria, São Paulo, v. 58. 2000.
O’Sullivan, S. B. Esclerose Múltipla. In: O’Sullivan, S. B.
Fisioterapia: Avaliação e Tratamento. 4ª ed. São
Paulo: Manole, 2004, Cap. 22, p. 715-738.
Poser, C. M. Doenças desmielinizantes. In: Rowland, L.
P.; Merritt. Tratado de Neurologia. Rio de Janeiro:
Guanabara Koogan, 1986. p. 603-621.
Schreiner, L. Eletroestimulação do nervo tibial no
tratamento da incontinência urinária de urgência em
idosas. PUCRS. Porto Alegre, 2009. 61 p.
Souza, R. O.; Figueiredo, W. M. O. Reflexo Cutâneo
Plantar em Extensão. Arquivos de Neuro-Psiquiatria.
Rio de Janeiro, p. 318-323, 1995.
Stephen, H. L. Esclerose Múltipla e outras doenças
desmielinizantes. In: Harrison. Medicina Interna. São
Paulo: Nueva Editorial Inter Americana, 1995. p.
2401-2411.
ELECTRICAL STIMULATION OF THE TRANSCUTANEOUS POSTERIOR TIBIAL NERVE FOR TREATING
URINARY INCONTINENCE DUE TO NEUROGENIC HYPERACTIVE BLADDER IN MULTIPLE SCLEROSIS
233
