
DEVELOPMENT OF AN EX VIVO QUANTITATIVE
SPECTROSCOPIC SCANNER
D. S. Ferreira
1
, N. Lue
2
, G. Minas
1
, M. S. Feld
2
, K. Badizadegan
3,4
and C. Yu
5
1
Centro Algoritmi, Universidade do Minho, Campus de Azurém, 4800-058, Guimarães, Portugal
2
GR Harrison Spectroscopy Laboratory, Massachusetts Institute of Technology
77 Massachusetts Avenue, Cambridge, MA 02139, U.S.A.
3
Departments of Pathology and Health Sciences and Technology, Harvard Medical School, Boston, MA 02114, U.S.A.
4
James Homer Wright Pathology Laboratories, Massachusetts General Hospital
WRN219, 55 Fruit St, Boston, MA 02114, U.S.A.
5
Optics Research Laboratory, Research & Development Division, Canon U.S.A., Inc.
9030 South Rita Road, Suite 302, Tucson, AZ 85747, U.S.A.
Keywords: Spectroscopic scanner, Diffuse reflectance, Fluorescence, Spectral imaging.
Abstract: We describe an ex vivo quantitative spectroscopy (QS) scanning platform which enables integration of
different optical modalities for the assessment of ex vivo tissue properties. As a first implementation, the QS
scanner combines diffuse reflectance spectroscopy (DRS) and intrinsic fluorescence spectroscopy (IFS) to
provide a multidimensional image of tissue structural and biochemical properties. The wide area coverage is
achieved by mechanically scanning of the optical probe. The spectroscopic data is taken one grid at a time
with variable grid-to-grid (GTG) distance and field of view (FOV). The ex vivo tissue surface under
examination can have a variable size since both GTG distance and FOV can be controlled. We demonstrate
the clinical utility of this system using an ex vivo tissue model with ultimate goal of imaging excised tissue
margins.
1 INTRODUCTION
Fast and reliable intra-operative diagnosis is critical
for the success of oncological surgery in a variety of
organ systems. After any cancer tissue resection it
has to be ensured that all malignant tissue was
removed and for that a surgical pathologist has to
examine the tissue margins (Haka, 2006). Current
clinical standards include visual inspection of the
tissue, followed by selective assessment of any
suspicious sites by frozen sectioning and rapid
histological evaluation. This procedure is still not
very efficient since according to a study by the
College of American Pathologists (Novis, 1997) a
significant number of hospitals do not routinely
provide intra-operative feedback to the surgeon
within 20 minutes of tissue delivery, adding costs
and an increased risk of morbidity associated with
extra time spent in the operating room. Additionally,
frozen section diagnoses are almost always
performed on a few “representative” portions of
tissue, resulting in potential discrepancies between
the frozen section assessment and the definitive
margin status which becomes only available once
the entire tissue has been processed post-operatively.
Therefore, there is a significant technological and
clinical need for methods capable of rapid and
reliable evaluation of excised tissues in real time.
Ex vivo imaging strategies have already been
proposed as potential tools for surgical margin
assessment. Mahadevan-Jansen and coworkers have
successfully applied contact probe autofluorescence
and diffuse reflectance spectroscopy, and a spectral
imaging to classify positive and negative margins of
excised breast specimens with high sensitivity and
specificity (Keller, 2010). However, a quantitative
analysis using images was not performed. Pogue and
co-workers used confocal reflectance microscopy
and spectrograph to raster-scan ex vivo tumors
margins and obtained mainly quantitative scattering
parameters associated with tissue morphology
(Krishnaswamy, 2009). Similar to previous wide
area spectroscopic imaging, the non-probe method
required some correction to deal with lines shape
spectra if the technique was used to acquire
quantitative absorption parameters (Keller, 2010). A
274
S. Ferreira D., Lue N., Minas G., S. Feld M., Badizadegan K. and Yu C..
DEVELOPMENT OF AN EX VIVO QUANTITATIVE SPECTROSCOPIC SCANNER.
DOI: 10.5220/0003888402740279
In Proceedings of the International Conference on Biomedical Electronics and Devices (BIODEVICES-2012), pages 274-279
ISBN: 978-989-8425-91-1
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

quantitative optical imaging device to assess breast
tumor margins was developed by Ramanujam et al.
(2009) using diffuse reflectance spectroscopy for the
extraction of scattering and absorption information.
In this work the margin surface is obtained by
manually translating an imaging probe that contacts
the specimen in a container through pre-drilled holes
with 5 mm center to center spacing.
Spectral imaging devices for the assessment of
excised tissue have two major advantages over
traditional practices of surgical margin assessment:
(1) real time analysis, with the benefit of reducing
patient anxiety and avoid potential follow-up
surgery; (2) whole area assessment, with the benefit
of reducing the probability of missing a lesion.
These devices can have a huge value in breast-
conserving surgery or in endoscopic mucosal
resection (EMR). Several studies have suggested
that in breast-conserving excision of cancer re-
operation for positive surgical margins discovered
after the surgery may be required in up to 50% of all
cases (Allweis, 2008), and that EMR achieves
complete excision of dysplastic lesions in only 4%
of the cases (Mino-Kenudson, 2005).
In this paper, we present a new and
complementary strategy to enable real-time
comprehensive assessment of surgical margins in
excised tissues. We have developed an ex vivo
spatial high-resolution quantitative spectroscopy
(QS) scanning platform which enables integration of
different optical modalities to provide quantitative
tissue information that correlate to disease state of
the surrounding tissue. Wide area imaging of
excised tissue is achieved by mechanically scanning
an optical probe, with variable spatial resolution.
Tissue samples are placed for analysis in a flat
platform, which enables an equal pressure across
time and an equal distance between probe and tissue
throughout the analysis.
The developed scanning platform currently
integrates diffuse reflectance spectroscopy (DRS)
and intrinsic fluorescence spectroscopy (IFS) for the
extraction of several spectroscopic parameters, but it
is adaptable to assemble many other optical
modalities. DRS and IFS have been first
implemented on the scanning platform since they
have shown great ability for the detection of
neoplastic diseases by assessing different spectral
features associated with normal and cancerous
tissues (Georgakoudi, 2001); (Tunnell, 2003); (Yu,
2008). These modalities provide quantitative
information about biochemical and structural tissue
attributes, from which diagnostic algorithms can be
developed.
Diffuse reflectance spectra from tissues are used
to extract information about hemoglobin
concentration and saturation, and light scattering
parameters using a well-developed model based on
the diffusion approximation of light propagation in
tissue. DRS provides information about the
morphology and biochemistry of the bulk tissue
(Zonios, 1999). Intrinsic fluorescence is the
fluorescence unaffected by tissue scattering and
absorption, and is obtained using the diffusely
reflected light to remove spectral distortions. The
relative contributions of the endogenous tissue
fluorophores (e.g., NADH and collagen) can be
extracted from the intrinsic fluorescence (Müller,
2001). Several studies of reflectance and
fluorescence for tissue diagnosis using optical fiber
contact probes for light delivery and collection have
been performed in different anatomic sites (Bard,
2006); (Chang, 2005); (Georgakoudi, 2001);
(Müller, 2003). Despite their potential, contact probe
techniques commonly suffer from undersampling.
The proposed ex vivo QS scanning platform
overcomes this drawback since it extends spectral
diagnosis to the imaging mode, enabling wide area
surveillance of tissue ex vivo.
This paper describes the design and feasibility
studies of a multi-modal scanning platform for an
intra-operative medical device that is able to perform
a rapid, real-time, detailed, and reliable quantitative
spectroscopic analysis of tissue surfaces. The major
benefit of this “adaptable scanning platform”
concept is that it is not limited to only one optical
modality, enabling the selection of the appropriate
technique for each margin assessment, or to use a
combination of different techniques.
2 METHODS
Given that ex vivo tissue analysis does not have
typical restrictions of in vivo imaging such as
imaging geometry, surface contour, patient motion
and the like, spectroscopic mapping of an arbitrarily
wide area is achieved by mechanically scanning an
optical probe in an inverted geometry. Spectroscopic
data are taken one grid at a time with variable grid-
to-grid (GTG) distance and field of view (FOV). In
our instrument, the ex vivo tissue surface under
examination can have a variable size from 2
square mm to 4 square cm, as well as variable
resolution, which can be as high as a quarter of the
spot size since both GTG distance and FOV are
controllable. Still, if necessary, the area for tissue
analysis can be easily increased in the future by
DEVELOPMENT OF AN EX VIVO QUANTITATIVE SPECTROSCOPIC SCANNER
275
including a larger sample holder to the scanning
platform. Using model-based diagnostic algorithms,
this instrument will be able to correlate
spectroscopic parameters with disease status in real
time.
The instrument’s contact probe, i.e. the FastEEM
probe (Tunnell, 2003), consists of a single light
delivery fiber surrounded by six collection fibers
that collect light from tissue and deliver it back to
the spectrograph (all seven fibers with 200 µm core
and NA = 0.22). All fibers are fused together at the
tip and polished at 17 degree angle to provide the
overlapping of detector and collector optical cones.
For spectroscopic scanning, we use only one of the
collection fibers to collect tissue reflectance and
fluorescence from a spot size of approximately 500
µm. The probe parameters are incorporated in our
reflectance (Zonios, 1999)
and fluorescence (Müller,
2001)
models. Wide area coverage is achieved by
scanning the light spot over the tissue using XY
mechanical scanning.
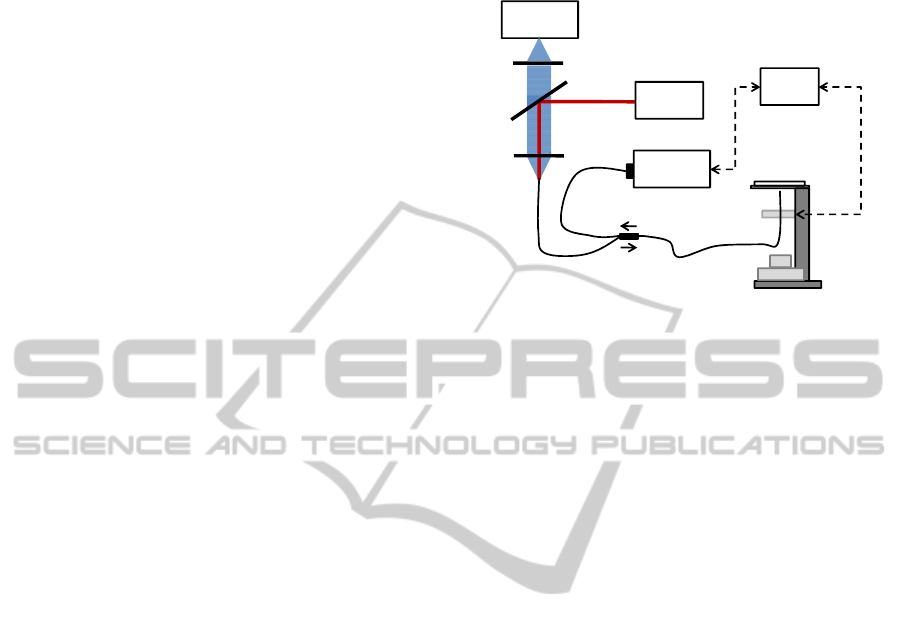
Figure 1 depicts the schematic diagram of the
instrument. To perform DRS measurements, white
light from a 75W CW xenon arc lamp (Oriel
Instruments, USA) is coupled via the delivery fiber,
to illuminate a “diagnostic spot” of ~0.5 mm in
diameter on the tissue sample. DRS signal from the
sample is collected, with adjacent collection fibers,
and coupled to a spectrometer (USB 2000+, Ocean
Optics, USA). A personal computer equipped with
Labview 8.5.0 software and DAQ data acquisition
board NI PCI-6221 (National Instruments, USA) are
used to control and coordinate the various
components, including the GTG distance and FOV
of the 2-D mechanical scanning (M-605.1DD and
M-126.DG1, Physik Instrument, Germany).
Spectroscopic data from the spectrometer and 2D
stage positions are acquired and analyzed. Same
resources, data handling and data acquisition are
utilized for IFS measurements, except the light
source is a pulsed diode pumped solid state laser that
delivers 355 nm light pulses of duration ~0.6 ns and
energy ~0.26 μJ at ~38 kHz (SNV-40F-000, Teem
Photonics, France). Note that different
measurements are accomplished through switching
the excitation sources with an installed flipping
mirror. Without any significant changes to the
scanning engine, the integration of other optical
modalities, such as hyperspectral, infrared or
Raman, would only require add-on and data
acquisition to the platform. This all-in-one device
could be a powerfull tool in clinical tissue
diagnostic. For the measurements, liquid phantoms
and tissue samples were placed in removable
ultraviolet glass Petri dishes, mounted on a custom
sample holder.
Figure 1: Schematic layout of the ex vivo QS scanning
platform.
3 RESULTS
3.1 System Calibration
Calibration was performed using liquid phantoms
with known scattering, absorption and fluorescence
properties. These phantoms were constructed by a
mixture of water based intralipid - scatterer -
(Fresenius Kabi AG), hemoglobin - absorber -
(Sigma Aldrich Co.) and furan - fluorophore -
(Lambda Physik) at various concentrations. This
fluorescent dye was selected because it has an
excitation and emission spectra similar to that of
collagen, which is an endogenous tissue fluorophore
important for diagnosis. All the measurements were
performed using a wavelength range from 350 to
700 nm for DRS and 380 to 700 nm for IFS.
The accuracy and capability of the system for
reflectance measurements was then carried on using
several combinations of various concentrations of
intralipid, furan (0.5 µg/mL) and hemoglobin (0.6, 1,
and 1.5 mg/mL). Reflectance spectra were acquired
from one spot in each sample. All the spectra were
normalized by a reflectance standard (Labsphere
SRS-20) in order to remove spectral distortions and
spatial inhomogeneities related with the instrument’s
spectral and spatial responses.
Figure 2 shows the calibrated DRS spectra, from
the same position on the sample, for different
phantoms. We use DRS for the extraction of
diagnostic information: by fitting the reflectance
spectrum to the diffuse scattering model described
by Zonios et al. (1999) three DRS parameters were
extracted for each pixel: A, the reduced scattering
Delivery fiber
White-Light
Source
Laser Source
Spectrometer
Sample holder
2D
translation
sta ge
White-light
camera
Collection
fiber
PC
Lens 1
Lens 2
Flipa ble
Mirror
BIODEVICES 2012 - International Conference on Biomedical Electronics and Devices
276

coefficient at the reference wavelength; B, related to
the average scatter size; and cHb, the total
concentration of hemoglobin. However, it is
important to notice that in the presented results all
the samples were exposed to air and, thus, their
estimated oxygen saturation is close to 1.0.
Figure 2: Calibrated reflectance spectra (solid lines)
measured on different tissue phantoms. The best fit spectra
are also plotted (dashed lines). The characteristic
absorption bands of hemoglobin at 420nm, 540nm, and
580nm are clearly visible.
Optimal fits were obtained between the measured
and computed spectra from the samples. From the
excellence agreement, the computed spectra give the
correct values of reflectance spectroscopy
parameters, which ensure that the instrument can
accurately measure the scatter and absorber
parameters. The values for parameters A, B, and cHb
are compiled in Table 1.
Table 1: Reflectance parameters (A, in mm
-1
, B, and cHb
in mg/mL) measured from tissue phantoms with different
hemoglobin concentrations.
The accuracy of fluorescence measurements was
assessed using the same set of phantoms. The
fluorescence at each spot is analyzed using IFS:
reflectance measurements are used to correct the
bulk fluorescence spectra (affected by scattering and
absorption) using the model described by Müller et
al. (2001) to extract the IFS spectra. Figure 3 shows
the fluorescence spectrum of pure furan in water
(blue line), and the several bulk and IFS spectra
measured using phantoms with different hemoglobin
concentrations.
Figure 3: Bulk fluorescence spectra (dashed lines)
measured on different tissue phantoms. The corresponding
intrinsic fluorescence spectra (IFS) are also plotted (solid
lines). The blue spectrum is the fluorescence measured
from pure furan in water. Note that the calculated IFS
spectra, which are independent to the absorbers and
scatterers and the raw spectrum of pure furan are well
overlapped.
As expected, the data confirms that bulk
fluorescence spectra vary considerably with
hemoglobin concentration in opposition to the IFS
spectra. The excellent agreement between the IFS
spectra and the spectrum of pure furan in water
indicates that IFS method can be used to remove the
distortions caused by tissue scattering and
absorption. These data provide evidence for accurate
calibration of our QS scanning platform.
3.2 Brain Tissue Imaging
The performance characteristics of the ex vivo QS
system were demonstrated using an inherently high
contrast sample with sharp regional boundaries (a
section of formalin-fixed human brain cortex with
gray and white matter, with an approximate size of 2
cm by 2 cm). A diffuse reflectance map of the brain
is shown in Figure 4(a), obtained using a step size of
125 μm, and an integration time of 3 ms at each
point. In this image, fine detail and high contrast
between the gray and white matter of the brain
cortex is clearly visible. For demonstration, high-
resolution spectral maps of the scattering parameter,
A, and measured hemoglobin concentration are
shown in Figure 4(b) and Figure 4(c), respectively.
As expected, it is revealed a higher hemoglobin
concentration on gray matter (related with higher
blood volume) (Hamberg, 1996). These results
demonstrate the ability of ex vivo QS scanner to
provide spectral contrast based on tissue parameters.
Parameters [Hb] = 0.6 [Hb] = 1.0 [Hb] = 1.5
A 1.074 1.074 1.070
B 0.289 0.278 0.230
cHb 0.619 1.002 1.472
DEVELOPMENT OF AN EX VIVO QUANTITATIVE SPECTROSCOPIC SCANNER
277

Figure 4: Representative QS images of brain cortex taken
with the proposed spatial high-resolution scanner: a) total
reflectance maps (in arbitrary units); b) quantitative map
of the scattering parameter A (mm
-1
); c) quantitative map
of hemoglobin concentration (mg/dl). Each box represents
approximately a 1 x 1 cm scanning area.
The concept has thus been demonstrated with the
developed bench-top platform using DRS and a
small biological sample. However, as previously
mentioned, the system is not limited to DRS and
IFS. Other modalities, such as Raman and infrared
spectroscopy can be readily integrated on our
platform to provide additional tissue information.
4 CONCLUSIONS
A quantitative multi-modal spectroscopy scanning
platform was constructed for assessing ex vivo tissue
biochemical and morphological information. This
newly developed instrument is ideal for
characterization of surgically excised tissue margins
and provides two major benefits over the current
practice: (1) reduce patient anxiety and avoid
follow-up surgery because on-the-fly real time data
analysis can be performed; (2) reduce the probability
of missing a lesion because the whole ex vivo tissue
area can be assessed. The proof of principle has been
demonstrated in this study with bench-top prototype
for quantitative spectroscopic scanning of a
biological sample while the construction of the
compact clinical unit is in progress. For the clinical
system several instrumentation and software
advances are needed: reduction of system size,
increase in collection and analysis speed, and
improved user interface with diagnostic algorithms.
Further investigation is also needed to address
the effect of excision in quantitative hemoglobin and
fluorophores measurements. For instance, excised
specimens contaminated by the presence of surface
blood may absorb the majority of reflected light,
significantly reducing the reflectance signal
(Volynskaya, 2008). In addition, some fluorophores
(e.g. collagen) might be stable in excised tissue,
whereas others (e.g. NADH) might degrade over
time, precluding an accurate extraction of its
concentration.
The extraction of quantitative optical parameters,
such as hemoglobin and collagen, has proven to be
helpful for the differentiation of normal and
malignant tissues. A recent study from Volynskaya
et al. (2008) has successfully demonstrated that
higher hemoglobin concentrations and higher
collagen values were more likely to be found in
ductal carcinoma of breast tissue than in normal
breast tissue, and thus could be used as diagnostic
parameters.
The ex vivo spectroscopic scanning platform
concept is not restricted to only DRS and IFS and
should be extended in the future to other optical
modalities in order to gather additional and
complementary diagnostic information.
ACKNOWLEDGEMENTS
This research was supported by the National
Institute of Health (grants P41-RR02594 and R01-
CA97966) and the Portuguese Foundation for
Science and Technology under the MIT|Portugal
Program (SFRH/BD/38978/2007). The authors
gratefully acknowledge Ramachandra R. Dasari for
all his support during this research.
REFERENCES
Allweis, T. M., Kaufman, Z., Lelcuk, S., Pappo, I., Karni,
T., Schneebaum, S., Spector, R., Schindel, A.,
Hershko, D., Zilberman, M., Sayfan, J., Berlin, Y.,
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
a
b
c
BIODEVICES 2012 - International Conference on Biomedical Electronics and Devices
278

Hadary, A., Olsha, O., Paran, H., Gutman, M.,
Carmon, M., (2008). A prospective, randomized,
controlled, multicenter study of a real-time,
intraoperative probe for positive margin detection in
breast-conserving surgery. Am J Surg 196:483-489
Bard, M. P. L., Amelink, A., Skurichina M., Noordhoek,
Hegt
, V., Duin, R. P., Sterenborg, H. J., Hoogsteden,
H. C., Aerts, J. G., (2006). Optical spectroscopy for
the classification of malignant lesions of the bronchial
tree. Chest 129:995-1001
Chang, S. K., Mirabal, Y. N., Atkinson, E. N., Cox, D.,
Malpica, A., Follen, M., Richards-Kortum, R., (2005).
Combined reflectance and fluorescence spectroscopy
for in vivo detection of cervical pre-cancer. J Biomed
Opt 10:024031
Georgakoudi, I., Jacobson, B. C., Van Dam, J., Backman,
V., Wallace, M. B., Muller, M. G., Zhang, Q.,
Badizadegan, K., Sun, D., Thomas, G. A., Perelman,
L. T., Feld, M. S., (2001). Fluorescence, reflectance,
and light scattering spectroscopy for evaluating
dysplasia in patients with Barrett's esophagus.
Gastroenterology 120:1620-1629
Haka, A. S., Volynskaya, Z., Gardecki, J. A., Nazemi, J.,
Lyons, J., Hicks, D., Fitzmaurice, M., Dasari, R. R.,
Crowe, J. P., Feld, M. S., (2006). In vivo margin
assessment during partial mastectomy breast surgery
using raman spectroscopy. Cancer Res 66:3317-3322
Hamberg, L. M., Hunter, G. J., Kierstead, D., Lo, E. H.,
González, R. G., Wolf, G. L., (1996). Measurement of
Cerebral Blood Volume with Subtraction Three-
dimensional Functional CT. AJNR Am J Neuroradiol
17:1861-1869
Keller, M. D., Majumder, S. K., Kelley, M. C., Meszoely,
I. M., Boulos, F. I., Olivares, G. M., Mahadevan-
Jansen, A., (2010). Autofluorescence and Diffuse
Reflectance Spectroscopy and Spectral Imaging for
Breast Surgical Margin Analysis. Lasers Surg Med
42:15-23
Krishnaswamy, V., Hoopes. P. J., Samkoe, K. S., O’Hara,
J. A., Hasan, T., Pogue, B. W., (2009). Quantitative
imaging of scattering changes associated with
epithelial proliferation, necrosis, and fibrosis in tumors
using microsampling reflectance spectroscopy. J
Biomed Opt 14:014004
Mino-Kenudson, M., Brugge, W. R., Puricelli, W. P.,
Nakatsuka, L. N., Nishioka, N. S., Zukerberg, L. R.,
Misdraji, J., Lauwers, G. Y., (2005). Management of
superficial Barrett's epithelium-related neoplasms by
endoscopic mucosal resection: clinicopathologic
analysis of 27 cases. Am J Surg Pathol 29:680-686
Muller, M. G., Georgakoudi, I., Zhang, Q. G., Wu, J.,
Feld, M. S., (2001). Intrinsic fluorescence
spectroscopy in turbid media: disentangling effects of
scattering and absorption. Appl Opt 40:4633-4646
Muller, M. G., Valdez, T. A., Georgakoudi, I., Backman,
V., Fuentes, C., Kabani, S., Laver, N., Wang, Z.,
Boone, C. W., Dasari, R. R., Shapshay, S. M., Feld,
M. S., (2003). Spectroscopic detection and evaluation
of morphologic and biochemical changes in early
human oral carcinoma. Cancer 97:1681-1692
Novis, D. A., Zarbo, R. J., (1997). Interinstitutional
comparison of frozen section turnaround time. A
College of American Pathologists Q-Probes study of
32868 frozen sections in 700 hospitals. Arch Pathol
Lab Med 121:559-67
Ramanujam, N., Brown, J. Q., Bydlon, T. M., Kennedy, S.
A., Richards, L. M., Junker, M. K., Gallagher, J.,
Barry, W. T., Wilke, L. G., Geradts, J. (2009).
Quantitative Spectral Reflectance Imaging Device for
Intraoperative Breast Tumor Margin Assessment. In:
31st Annual International Conference of the IEEE
Engineering in Medicine and Biology Society.
EMBS’09, Minneapolis, Minnesota, USA, Sept. 2-6,
2009, pp 6554-6556
Tunnell, J. W., Desjardins, A. E., Galindo, L.,
Georgakoudi, I., McGee, S. A., Mirkovic, J., Mueller,
M. G., Nazemi J., Nguyen, F. T., Wax, A., Zhang, Q.
G., Dasari, R. R., Feld, M. S., (2003). Instrumentation
for multimodal spectroscopic diagnosis of epithelial
dysplasia. Technol Cancer Res Treat 2:505-514
Volynskaya, Z., Haka, A. S., Bechtel, K. L., Fitzmaurice,
M., Shenk, R., Wang, R., Nazemi, J., Dasari, R. R.,
Feld, M. S., (2008). Diagnosing breast cancer using
diffuse reflectance spectroscopy and intrinsic
fluorescence spectroscopy. J Biomed Opt 13:024012
Yu, C., Lau, C., O’Donoghue, G., Mirkovic, J., McGee,
S., Galindo, L., Elackattu, A., Stier, E., Grillone, G.,
Badizadegan, K., Dasari, R. R., Feld, M. S., (2008).
Quantitative spectroscopic imaging for noninvasive
early cancer detection. Opt Express 16:16227-16239
Zonios, G., Perelman, L. T., Backman, V. M., Manoharan
R., Fitzmaurice, M., Van Dam, J., Feld, M. S., (1999).
Diffuse reflectance spectroscopy of human
adenomatous colon polyps in vivo. Appl Opt 38:6628-
6637
DEVELOPMENT OF AN EX VIVO QUANTITATIVE SPECTROSCOPIC SCANNER
279
