
Hybrid Simulation Approach for Prospective Assessment
of Mobile Stroke Units
∗
Anatoli Djanatliev
1
, Peter Kolominsky-Rabas
2
, Bernd M. Hofmann
3
, Axel Aisenbrey
4
and Reinhard German
1
1
Computer Networks and Communication Systems, Universit
¨
at Erlangen-N
¨
urnberg, Erlangen-N
¨
urnberg, Germany
2
Interdisciplinary Centre for HTA and Public Health, Universit
¨
at Erlangen-N
¨
urnberg, Erlangen-N
¨
urnberg, Germany
3
Siemens AG, Healthcare Sector, Clinical Competence Center Neuroscience, Erlangen, Germany
4
Siemens AG, Healthcare Sector, Siemens Healthcare Consulting, Erlangen, Germany
Keywords:
Healthcare, Simulation, Hybrid Simulation, System Dynamics, Agent-based Simulation, Prospective Health
Technology Assessment, Ischemic Stroke.
Abstract:
Technology innovations in health care offer high potentials for all stakeholders (e.g., patients, healthcare
providers and health industry), but the development phase of such innovations is often very expensive and
the effects are hardly predictable without a systematic strategy. The new interdisciplinary approach Prospec-
tive Health Technology Assessment (ProHTA) uses simulation techniques to indicate the effects of new health
technologies, early before the cost-intensive development process begins. Furthermore, ProHTA helps to de-
tect gaps and bottlenecks in the health system to catch potentials for new innovations. The scope of ProHTA
includes both a strategic aggregated level of analyses as well as an individual detailed level. This paper de-
scribes the use of hybrid simulation approaches, consisting of System Dynamics and Agent-Based Simulation,
to analyze the effects of an innovative stroke technology. We discuss an example of the prospective assess-
ment of Mobile Stroke Units within a Metropolitan Scenario. The project ProHTA is a part of the Centre of
Excellence for Medical Technology - Medical Valley EMN - and is supported by the German Federal Ministry
of Education and Research (BMBF), project grant No. 01EX1013B.
1 INTRODUCTION
The global market for medical technology products is
growing rapidly due to an increasing demand of in-
novative healthcare technologies. Presumably, some
reasons of this notice are the increasing life ex-
pectancy of the population, new technical opportu-
nities and an increasing complexity of the healthcare
delivery.
A significant consequence of this trend is that the
healthcare industry has to handle even faster trade-
off decisions before developing new innovations in
medicine. To be more profitable a new product must
have a short development phase, low costs and it
is also important that the expected revenue can be
reached. In addition, health technologies are safety-
critical, as the life quality can depend on the product’s
quality. Following this fact, proven evidence is nec-
∗
On behalf of the ProHTA Research Group.
essary and regulatory barriers have to be overcome.
Usually, such activities are time-consuming and their
results are difficult to predict. Often there is also no
proven evidence available, so the development of new
innovations can degenerate into a risky, non-profitable
project.
The main difference between the healthcare do-
main and other safety-critical areas is that many in-
volved stakeholders with different interests have to
be satisfied before a product can be placed on the
market. Some examples of them are patients, health-
care providers such as hospitals and outpatient depart-
ments, manufacturers in healthcare, technology de-
velopers, insurance companies, governments, regula-
tory institutions and academia.
According to the described situation, assessments
of health technologies are very complex and advanced
assessment methods are crucial to prevent disinvest-
ments and to make the product development more ef-
fective. All players must be considered for this pro-
357
Djanatliev A., Kolominsky-Rabas P., M. Hofmann B., Aisenbrey A. and German R..
Hybrid Simulation Approach for Prospective Assessment of Mobile Stroke Units.
DOI: 10.5220/0004029603570366
In Proceedings of the 2nd International Conference on Simulation and Modeling Methodologies, Technologies and Applications (SIMULTECH-2012),
pages 357-366
ISBN: 978-989-8565-20-4
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

cess to reach an overall credibility of the product’s
quality and to detect all kinds of problems as early as
possible.
Three assessment methodologies for healthcare
technologies have been introduced until now. Health
Technology Assessment, Early Health Technology
Assessment and Horizon Scanning.
Health Technology Assessment (HTA) is an ap-
proach used after the market launch of a product when
evidence is available from studies. In accordance with
Goodman (Goodman, 2004), the main field of HTA
is to inform, among others, regulatory agencies and
lawmakers about permission decisions for a commer-
cialization of a regarded innovation.
Early Health Technology Assessment (Early
HTA) tends to be an appropriate tool in cases where
the product is already in the development phase but
only limited evidence is available. Some examples for
such evidence levels are animal testing, early clinical
experience, or data from previous technology genera-
tions (Pietzsch and Pat
´
e-Cornell, 2008).
The impact of Horizon Scanning (HS) is the com-
parative assessment of similar technologies to observe
trends of possible disinvestments and impacts of new
healthcare technologies. Horizon Scanning Systems
focus on health technologies that are ready to enter the
market, i.e. in early post-marketing phases (Geiger-
Gritsch, 2008).
In many cases the technological progress is the
key factor for new products and there is only a little
consideration of possible future consequences. But
new innovations must reach positive assessment re-
sults before their impact can be seen by all stake-
holders as reasonable. Hence, an enormous number
of disinvestments can be expected, as established as-
sessment methods (HTA, Early HTA and HS) are just
used for products that already have passed the expen-
sive design and development process.
For that reason we call for advanced foresight
healthcare assessment methods which are applicable
early before high efforts and investments were made.
This is where our approach ProHTA can take an im-
portant role, because simulation techniques can be ap-
plied to assess new innovations prospectively.
2 RELATED WORK
There are already a couple of publications which are
presenting the use of simulation for the healthcare do-
main. Most of them are considering healthcare pro-
cesses and are modeled by the Discrete Event Sim-
ulation approach. Brailsford (Brailsford, 2008) dis-
cussed System Dynamics (SD) as tool for healthcare
modelers. The author presented several examples and
depicted some reasons for the growth in SD popular-
ity. Following this, some advantages of SD are lower
data requirements, the sight of the big-picture and in
particular very fast simulation runs.
In order to benefit from high-level abstractions as
well as to allow more detailed modeling possibilities,
hybrid simulation techniques are gaining acceptance.
Heath et al. (Heath et al., 2011) discussed several
challenges and successes of cross-paradigm model-
ing. In particular, Discrete Event Simulation, System
Dynamics and Agent-Based Simulation approaches
were considered in detail. Though hybrid simulation
is not precisely defined yet, there are however soft-
ware packages that allow multi-paradigm modeling.
3 PROSPECTIVE HEALTH
TECHNOLOGY ASSESSMENT
Prospective Health Technology Assessment (Pro-
HTA) is a new approach that extends the tool envi-
ronment of healthcare assessment methodologies and
fills the gap, mentioned previously. For this reason
the project is located within the Medical Valley EMN
(European Metropolitan Region Nuremberg) and is a
part of the Centre of Excellence for Medical Technol-
ogy.
The innovative intention of ProHTA is the assess-
ment of health technologies from many perspectives,
early before the development of a medical innovation
begins. It helps to detect potentials for process opti-
mization and allows learning about the influence of
a new technology on the established health system
structures. Innovation’s cost-effectiveness has to be
prospectively calculated as well as the impact on the
patient’s health.
Figure 1 summarizes the main prospective eval-
uation processes. In this respect, two questions are
central to ProHTA:
• What are the changes that result from the launch
of a new technology? - ProHTA will be able to
simulate and assess the effects of changes to pro-
cesses, which are introduced e.g. by a new tech-
nology. ProHTA will project the effects of inno-
vative health technologies on the quality and costs
of health care.
• What does a technology need to be like in order
to have a specific effect? - If certain input re-
quirements of a desired change are specified, the
ProHTA tools will enable outcome related con-
clusions concerning the required changes to the
process (hypothesis development). ProHTA will
SIMULTECH2012-2ndInternationalConferenceonSimulationandModelingMethodologies,Technologiesand
Applications
358
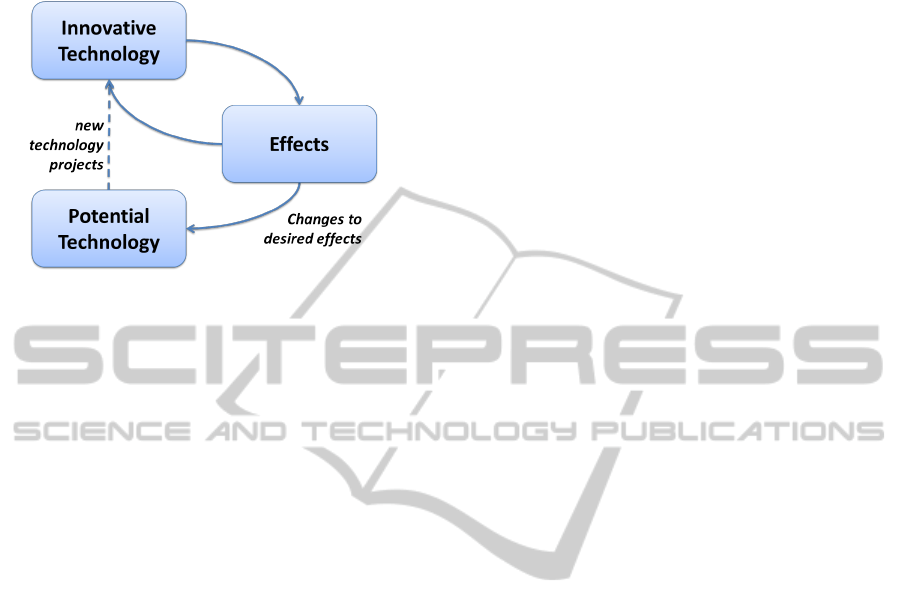
envisage the effects of the potential efficiency en-
hancement on the health care system.
Figure 1: ProHTA overview.
Especially the second question allows ProHTA to
examine the existing health system and to find bottle-
necks and weaknesses of currently applied practices.
This can lead to new ideas for health technologies
that are particularly based on desired effects and not
only on technical opportunities. In the course of the
method creation of ProHTA a new scientific service
platform has to be developed targeting on the scope
of the just described project.
The regarded challenges and questions are han-
dled together by an interdisciplinary team consisting
of experts from the areas of Public Health, Health
Technology Assessment, Clinical Medicine, Health
Economics and Outcomes Research, Medical Infor-
matics, Knowledge Management as well as Modeling
and Simulation. Furthermore, two representatives of
the healthcare industry also participate in the project.
In this paper we discuss the use of hybrid simula-
tion approaches, consisting of System Dynamics (SD)
and Agent-Based Simulation (ABS), for the new fore-
sight assessment method ProHTA. As the complexity
of the considered domain and the interdisciplinary co-
working is enormous, a structured methodology to-
wards a hybrid simulation model will be described
within the next section as well. The current focus
of the approach is the assessment of innovative tech-
nologies in management of acute stroke. We use Mo-
bile Stroke Units (MSU) within a Metropolitan area
as an innovative health technology to show exemplary
how hybrid simulation techniques can be applied to
the impact of ProHTA. Within the discussion section
we look ahead to the future work, including the vali-
dation of our approach and its application to oncology
diseases.
4 CONCEPTUAL MODELING
As already mentioned, many challenges have to be
mastered during the project realization phase. To
achieve an effective and intensive co-working of
all experts with different backgrounds, a structured
methodology is essential.
For that reason a dedicated Conceptual Modeling
Process (CMP) for ProHTA was defined, classifying
the main steps towards a hybrid simulation model, be-
ginning at the domain experts’ knowledge collection.
It is largely based on current work of a research group
from the University of Warwick and Loughborough
University (Robinson, 2011; Kotiadis and Robinson,
2008).
As hybrid simulation builds the focus of this paper
and the CMP will be the topic of another publication,
we introduce in the following only some parts of it, as
it is important for the simulation.
The CMP distinguishes in particular between do-
main experts and technical experts and defines fields
of activity and intermediate interfaces for all of them.
Furthermore, the reality is summarized within the Do-
main World and the abstraction of it is contained in
the, so called, Model World. The significant arti-
fact of the Domain World is the non-formal specifi-
cation of the problem, represented by the Conceptual
Domain Model (CDM). This result is used by an it-
erative formalization process as input for the Model
World, according to create the Formal Conceptual
Model (FCM) which serves as a basis for the simu-
lation model and knowledge base.
Figure 2 depicts by solid lines the main steps of
the Conceptual Modeling Process towards a simula-
tion model. Dashed arrows represent the feedback
steps of iterative improvements.
5 USE-CASE: MOBILE STROKE
UNITS WITHIN A
METROPOLITAN REGION
Stroke is one of the leading causes of death and
disability and absorbs a considerable proportion of
healthcare budgets (Kjellstr
¨
om et al., 2007). In Ger-
many an increase of 1.5 million stroke cases is esti-
mated in the next decade (Kolominsky-Rabas et al.,
2006). Due to an ageing population, increasing inci-
dence values could be expected in the future, as stroke
appears mainly at higher age groups. The costs for
treatment and rehabilitation in Germany are estimated
to be totally about 58 billion of euros in the period
2006-2015 (Kolominsky-Rabas et al., 2006).
HybridSimulationApproachforProspectiveAssessmentofMobileStrokeUnits
359
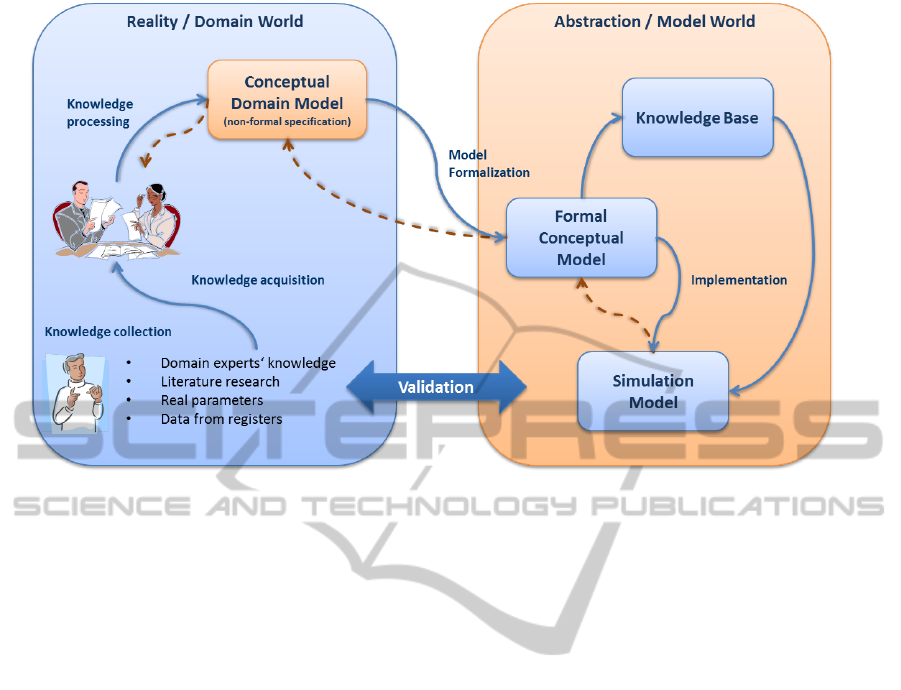
Figure 2: Conceptual modeling process of ProHTA.
One of the most frequent form of stroke is the is-
chemic stroke, caused by an oclusion of cerebral ar-
teries. Currently, an approved method for the treat-
ment is the intravenous thrombolysis by recombinant
tissue plasminogen activator (rtPA) (Fassbender et al.,
2003). However, even in specialized hospitals (Stroke
Units), only 7 to 10 percent of patients are treated by
this effective method (Heuschmann et al., 2010). The
main reason for such a bad rate is the applicability
of the thrombolysis only within 4.5 hours after the
obstruction’s occurrence and the time, elapsed during
the transport to the hospital (Purrucker and Veltkamp,
2011). A significant increase of the rate from 3 per-
cent to 7 percent had been observed after the exten-
sion of the recommended time window from 3 hours
to 4.5 hours in 2008 (Purrucker and Veltkamp, 2011).
In case of an affection, nearly 1.9 million of neu-
rons can die per minute (Kuehn and Grunwald, 2011).
Hence, the “time is brain” concept has to be applied
to the extremely time-critical treatment of stroke. Fol-
lowing this fact, particularly innovations in stroke
treatment are necessary which are able to reduce the
call-to-therapy-decision time.
Two German research groups from Saarland and
Berlin (Walter et al., 2010; Ebinger et al., 2012) are
working with their partners on methods targeting at
the transfer of the thrombolytic inpatient treatment to
the pretreatment phase. In that case the therapy can be
applied before the time-intensive transfer to the hos-
pital and an increase of the number of patients, treated
by thrombolysis can be expected. The main problem
of this idea is the important exclusion of an intracere-
bral haemorrhage, before applying rtPA. This can be
done by laboratory analyses and Computer Tomogra-
phy (CT), usually installed in hospitals. To prevent a
loss of crucial time, both research groups developed
similar prototypes, the Mobile Stroke Unit (MSU) and
the Stroke-Einsatz-Mobil (STEMO). Such a vehicle
extends the standard emergency equipment by a CT
and further tools for a rapid diagnostic decision on-
site at stroke occurrence location.
In an early phase, first trials have shown that
a shortened call-to-therapy-decision-time of approx-
imately 35 minutes is not a vision (Kuehn and Grun-
wald, 2011). To inspect other relevant effects (e.g.
long-term cost-effectiveness, application in other re-
gions) more trials are necessary, so that further time
and cost investments have to be made. This is where
ProHTA can provide an early analysis by hybrid sim-
ulation.
6 HYBRID SIMULATION
For the purpose of the Prospective Health Technol-
ogy Assessment simulation has been identified to be
an appropriate tool. Customized large scale simula-
tion models are crucial to handle complex questions
in situations where an innovative technology possibly
hasn’t been developed yet. Depending on the point
of view, ProHTA must be able to answer specialized
questions (e.g. effectiveness of a new innovation)
SIMULTECH2012-2ndInternationalConferenceonSimulationandModelingMethodologies,Technologiesand
Applications
360
as well as to calculate global and long-term conse-
quences. Hence, large scale models are necessary to
fulfill these requirements. Furthermore, separate data
management and data quality components are crucial
to handle a couple of different input data formats in
an efficient way (Baumg
¨
artel and Lenz, 2012).
We need methods to create models on an abstract,
macroscopic level (e.g. economic flows, population
dynamics) where data about details is not available,
or even is not necessary. In our approach System Dy-
namics (SD) (Forrester, 1999) was qualified as an ap-
propriate tool for this kind of simulation. To model
individual aspects of patient’s workflows and its be-
havior, the Agent-Based Simulation (ABS) approach
has been selected. New technological innovations can
also be modeled by the ABS approach to allow be-
havioral changes, according to inspect their impacts
on output values.
Each assessment scenario is individual. For this
reason we propose to combine the SD and the ABS
approach into a common hybrid simulation using an
adequate ratio according to the desired simulation
level and high simulation performance. This trade-
off decision can be handled by following a top-down
approach. In that case the problem environment can
be modeled as deeply as needed by abstract methods
and a special simulation part will be framed-out and
realized by the ABS approach.
The idea of hybrid simulation is getting more
and more popular in current research (Heath et al.,
2011; Brailsford et al., 2010). There are many soft-
ware packages that allow to create simulations by SD,
Discrete Event Simulation (DES) or ABS models,
but most of them support only one of the presented
approaches. AnyLogic (XJ Technologies Company
Ltd., 2012) offers the power to combine different sim-
ulation paradigms within a common simulation envi-
ronment. This is why this tool is qualified to create
models within the scope of ProHTA.
6.1 Modular Environment
In accordance to the Conceptual Modeling Process
(Section 4), the CDM represents a non-formal de-
scription of the collected experts’ knowledge. The
FCM is central to develop simulation models within
the context of ProHTA.
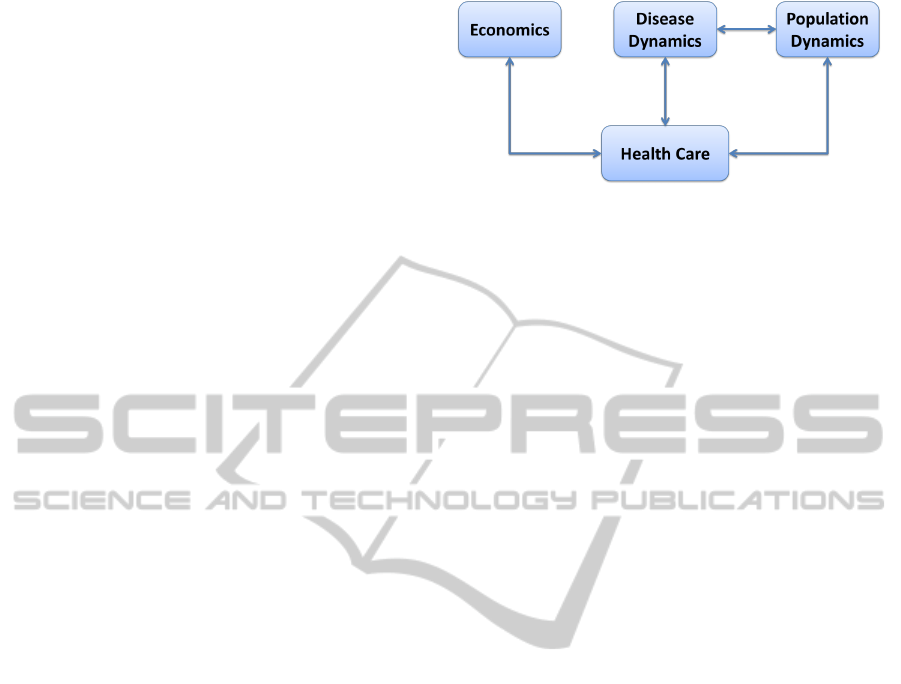
We have to deal with different, interacting simula-
tion parts, such as money flows, healthcare structures,
disease, and population development. To make mod-
els reusable for further assessment scenarios and to
master the complexity, modularization is important.
Figure 3 depicts the identified modules within the
scope of ProHTA.
Figure 3: Overview of the modules.
Population Dynamics summarizes models and pa-
rameters that handle with the development of demo-
graphic structures, e.g. birth rate, mortality, immigra-
tion and emigration.
Disease Dynamics includes generic model parts
that deal with illness parameters, e.g. incidence,
prevalence, case fatality rate and remission.
Economics combines the dynamics of money
flows of the health system. Statutory and private
health insurance can be modeled there as well as the
long-term care system.
Health Care is a module where especially work-
flows of prevention, pre-treatment, treatment and
post-treatment of a regarded disease can be modeled.
Chahal and Eldabi (Chahal and Eldabi, 2008) pro-
posed a process environmental format for hybrid sim-
ulations. In our hybrid simulation approach for Pro-
HTA, SD models can be used to build the environment
of a simulation. An important simulation part can be
modeled by ABS approaches and used as core within
the process environmental format.
6.2 Scenario Description
Before we set the focus on our model, the scenario
with Mobile Stroke Units within a Metropolitan re-
gion will be shortly presented in the following:
• Stroke scenario with usage of a predefined num-
ber of 10 MSUs.
• A German Metropolitan region, represented by
Berlin, with approximately 3.416.000 people is
modeled using data from the statistical calcula-
tions of (Amt f
¨
ur Statistik Berlin-Brandenburg,
2010).
• The regional distribution of people is done by in-
formation about the district density.
• MSUs are randomly distributed within the region
boundaries.
• People can get stroke and call the Rescue Service
(RS).
• RS decides whether an MSU can be sent (e.g.
HybridSimulationApproachforProspectiveAssessmentofMobileStrokeUnits
361

Figure 4: Mobile stroke units within a metropolitan scenario.
there are free MSUs available) to the affected pa-
tient.
• During the affection phase, people pass through
diagnostic and therapy workflows and lose life
quality according to a therapeutic effectiveness.
• In case of using an MSU, thrombolytic therapy
can be started onsite at patient’s location, after
a mobile CT and laboratory diagnose were per-
formed.
• Calculated costs are drawn from financial bud-
gets.
• Demographical information is used to reproduce
the population development.
• Prevalence is used to separate the population in
affected and not-affected parts.
• Incidence is used as a dynamic affection rate.
For assessment purposes the same scenario with-
out MSUs will be used afterwards. It allows to make
the effects of a new intervention (MSUs) visible.
6.3 Simulation Model
6.3.1 Overview
The simulation is started within an initialization phase
and proceeds with a forecasting phase after a couple
of data has been produced.
There are two types of agents modeled within the
hybrid simulation of our MSU scenario, the individ-
ual behavior of persons and Mobile Stroke Units. De-
mographic development is reproduced by a separate
System Dynamics model (Population Dynamics) as
well as money flows of the health system.
Figure 4 depicts a screenshot of a running simu-
lation. Small points represent person agents (number
1). Changing the color from blue to red a patient be-
comes affected. Yellow bullets with black borders are
a representation of MSU agents (number 2). During
simulation runs they are colored in red, if an MSU is
busy to see an overall utilization of the new technol-
ogy. MSUs pick up patients and move them to the
next hospital.
6.3.2 Agents
Age, risk factor (RF), gender and life quality (LQ)
are important attributes of a person and are sampled
initially. A normal risk is represented by RF = 1, high
risk by RF > 1 and low risk is a value RF < 1 ∧ RF >
0. LQ is represented by a value between 0 and 100.
Dependent on the therapy success, the patient loses
more or less LQ points.
Time until the next occurrence of stroke symp-
toms is calculated by an appropriate function. An
annualEvent is used to increase patient’s current age
and to run a death calculation function. The behavior
SIMULTECH2012-2ndInternationalConferenceonSimulationandModelingMethodologies,Technologiesand
Applications
362
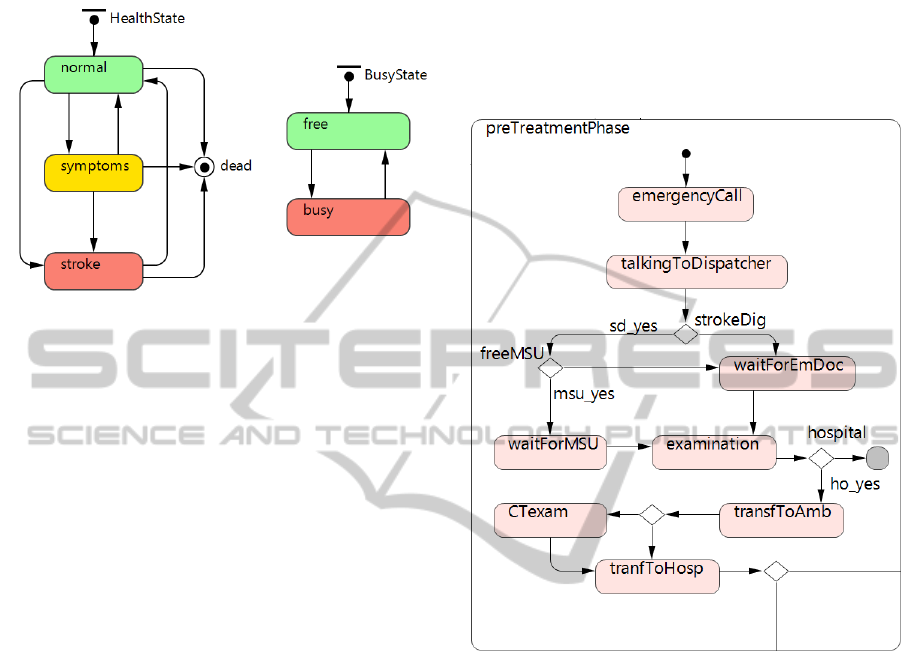
is represented by the left hand state chart of Figure 5
with three states (normal, symptoms, affected).
Figure 5: Behavior state charts of agent person (left) and
MSU (right).
The state chart of the agent type MSU is depicted
on the right hand of the Figure 5 and includes two
states (free, busy). The variable timeApprToScene is
used to simulate the delay of an MSU until arrival at
patient’s location. In a further step it can be used to
reproduce traffic by an additional simulation part.
The health care structure is modeled within a sep-
arate state chart. At the beginning, each person is lo-
cated in the state noHealthCare. After the occurrence
of suitable events, a patient changes to an appropri-
ate composite state, such as prevention, pre-treatment,
treatment and post-treatment that are partially pre-
sented in the following.
Each step that produces costs (e.g. special treat-
ments, materials, staff employment) collects them in
a global variable within the economics System Dy-
namics model. The calculated number is pulled off
from the corresponding budgets once-a-year.
6.3.3 Prevention
As prevention interventions for stroke are not usual, a
simple part of the model takes into account only weak
preventive influences, e.g. healthy lifestyle. Preven-
tive check-ups are simulated in undetermined cycles
with a minimum of five years elapsed since the last
prevention.
The time until next stroke symptoms occurrence is
calculated by a multiplication of the remaining time
and the individual risk factor (RF) of a person. The
higher a RF, the higher the prevention effect and the
earlier a prevention, the higher is the gain of time.
6.3.4 Pre-treatment
After the expiration of the time until next symptoms,
an event is fired and the concerned person enters the
symptoms state and starts the workflow of the pre-
treatment phase within the HealthCare state chart, fig-
ured in 6.
Figure 6: Agent-based model of the pre-treatment phase.
According to the workflow an emergency call is
modeled first. After talking to the dispatcher a first
diagnosis is made and a rescue service is alarmed to
move to the patient. Due to the assessment of MSUs,
the dispatcher searches for free Mobile Stroke Units.
The more of them are initially available, the higher is
the probability to get one free. Otherwise, a normal
emergency doctor will be sent.
In case of MSU usage, a CT exam can be per-
formed at the patient’s location in the pre-treatment
phase, as described in section 5.
Following our assessment scenario, the branches
where MSU are involved are set to 0 during the com-
parative simulation runs.
6.3.5 Treatment
Due to the arrival in the hospital the treatment phase
starts by an invocation of the composite state treat-
ment. Diagnosis and therapy steps which were al-
ready performed during the pre-treatment phase are
HybridSimulationApproachforProspectiveAssessmentofMobileStrokeUnits
363

Figure 7: Mean estimated life quality without/with 10 MSUs.
skipped and a best-case workflow, modeled by our do-
main experts, is traversed by the patient.
6.4 Simulation Results
In our exemplary use-case of Mobile Stroke Units we
noticed some trends due to the implementation of 10
MSUs in a metropolitan area. According to the used
input parameters that were partially estimated by do-
main experts, we monitored some of the expected re-
sults.
Figure 7 shows two plots of the estimated mean
life quality. On the left hand we can see graphs that
were calculated by a simulation run without MSU
usage; on the right hand a scenario with 10 Mobile
Stroke Units was applied. According to the results we
can notice that persons with stroke affection achieve
a higher mean life quality after the launch of the re-
garded innovation. The main reason for this is the
possibility to apply the thrombolytic therapy imme-
diately at the stroke occurrence location and an in-
tervention can be done within the important time-
window of 4.5 hours.
In our model we also aggregated costs caused by
MSU usage to show exemplary economic assessment
calculations. To check if a new technology is reason-
able, a Cost-Effectiveness-Analysis (CEA) was com-
puted by the equation 1 during simulation runs.
CEA =
K
MSU
− K
NoMSU
∆LQ
NoMSU
− ∆LQ
MSU
(1)
We regarded life quality as effectiveness parame-
ter to determine the effect of MSUs. Within the equa-
tion the following variables are defined as follows:
K
MSU
− K
NoMSU
(cost difference between MSU usage
and conventional therapy workflows), ∆LQ
NoMSU
and
∆LQ
MSU
are mean life quality losses of stroke patients
without/with MSU implementation.
Graph 8 shows an example result of a Cost-
Effectiveness-Analysis. The plot suggests that an in-
crease of the mean quality of life of the population of
one point comes with a cost of approximately 12,000.
It also shows the effects of the initialization phase
which have been alleviated in the forecasting phase
starting around the year 2010.
7 DISCUSSION
ProHTA is a new approach that uses simulation tech-
niques to assess health technologies early before the
cost-intensive development process starts. It allows to
evaluate healthcare innovations within the context of
the health system and to find gaps and bottlenecks that
can lead to new ideas for innovations. We identified
hybrid simulation, consisting of the System Dynam-
ics and the Agent-Based Simulation, to be an appro-
priate modeling approach for large scale simulations.
This method enables to solve problems on a macro-
scopic level, e.g. disease dynamics in a global con-
text, as well as on a detailed, behavioral microscopic
level. A further benefit of this approach within the
scope of ProHTA is the possibility to build models
top-down, beginning from high abstractions and go-
ing more in detail to frame-out individual workflows.
To make models capable for reuse and to master com-
Figure 8: Example of a cost-effectiveness-analysis (CEA).
[y-axis: costs per one life quality point, x-axis: time].
SIMULTECH2012-2ndInternationalConferenceonSimulationandModelingMethodologies,Technologiesand
Applications
364

plexity, we designed a modular and generic environ-
ment that is also eligible for flexible model changes.
As an effective co-working of interdisciplinary ex-
perts is crucial to get useful results, a conceptual mod-
eling process was developed. The main benefits are in
particular well-defined areas of activity for all experts
and the capability to proceed in a structured way.
To evaluate our methods, an exemplary use-
case scenario of an innovative stroke treatment ap-
proach, represented by Mobile Stroke Units within
a Metropolitan Scenario, had been implemented, us-
ing the simulation software AnyLogic (XJ Technolo-
gies Company Ltd., 2012). This tool is predestinated
for multi-method simulation paradigms. The project
procedure strictly followed the CMP and an overall
expert-credibility has been achieved.
There are still many challenges to master in the fu-
ture. Real data from the Stroke Register of Erlangen
(ESPro) will be used to validate the model using other
stroke use-cases and to asses interventions whose ef-
fects are already attestable by evidence data. A fur-
ther complex task will be the application of our hy-
brid simulation approach to other diseases, especially
within the domain of personalized medicine. As the
ProHTA research group includes oncology experts,
cancer diseases will be the focus of further work.
Some technical challenges are also still remaining.
Some of them are simulation performance, scalabil-
ity of models, requesting data (semi-)automated from
the data management component and further hybrid
simulation research for combination of SD and ABS
models.
ACKNOWLEDGEMENTS
Prospective Health Technology Assessment (Pro-
HTA) is funded by the German Federal Ministry of
Education and Research (BMBF) as part of the Na-
tional Cluster of Excellence Medical Technology -
Medical Valley EMN (Project grant No. 01EX1013).
REFERENCES
Amt f
¨
ur Statistik Berlin-Brandenburg (2010). Die kleine
Berlin–Statistik 2010.
Baumg
¨
artel, P. and Lenz, R. (2012). Towards data and
data quality management for large scale healthcare
simulations. In Conchon, E., Correia, C., Fred, A.,
and Gamboa, H., editors, Proceedings of the Interna-
tional Conference on Health Informatics, pages 275–
280. SciTePress - Science and Technology Publica-
tions. ISBN: 978-989-8425-88-1.
Brailsford, S. C. (2008). System Dynamics: What’s in it for
Healthcare Simulation Modelers. In Proceedings of
the 2008 Winter Simulation Conference, pages 1478–
1483. Winter Simulation Conference 2008.
Brailsford, S. C., Desai, S. M., and Viana, J. (2010). To-
wards the holy grail: Combining system dynamics and
discrete-event simulation in healthcare. In Proceed-
ings of the 2010 Winter Simulation Conference, pages
2293–2303. Winter Simulation Conference 2010.
Chahal, K. and Eldabi, T. (2008). Applicability of hybrid
simulation to different modes of governance in UK
healthcare. In Proceedings of the 2008 Winter Sim-
ulation Conference, pages 1469–1477. Winter Simu-
lation Conference 2008.
Ebinger, M., Rozanski, M., Waldschmidt, C., Weber, J.,
Wendt, M., Winter, B., Kellner, P., Baumann, A.,
Malzahn, U., Heuschmann, P., Fiebach, J., Endres,
M., and Audebert, H. (2012). PHANTOM-S: the pre-
hospital acute neurological therapy and optimization
of medical care in stroke patients – study. Interna-
tional Journal of Stroke. Feb 2.
Fassbender, K., Walter, S., Liu, Y., Muehlhauser, F.,
Ragoschke, A., Kuehl, S., and Mielke, O. (2003).
”Mobile Stroke Unit” for Hyperacute Stroke Treat-
ment. Stroke, 34(6):44e–44.
Forrester, J. W. (1999). Industrial Dynamics. Pegasus Com-
munications, Waltham and MA.
Geiger-Gritsch, S. (2008). Horizon Scanning in Oncology:
Concept Development for the Preparation of a Hori-
zon Scanning System in Austria. Ludwig Boltzmann
Institute for Health Technology Assessment.
Goodman, C. S. (2004). HTA 101: Introduction to Health
Technology Assessment. National Information Center
on Health Services Research and Health Care Tech-
nology (NICHSR). The Lewin Group.
Heath, S. K., Brailsford, S. C., Buss, A., and Macal, C. M.
(2011). Cross-paradigm simulation modeling: chal-
lenges and successes. In Proceedings of the 2011 Win-
ter Simulation Conference, pages 2788–2802. Winter
Simulation Conference 2011.
Heuschmann, P., Busse, O., Wagner, M., Endres, M., Vill-
ringer, A., R
¨
other, J., Kolominsky-Rabas, P., and
Berger, K. (2010). Frequency and Care of Stroke in
Germany. Aktuelle Neurologie, 37(07):333–340.
Kjellstr
¨
om, T., Norrving, B., and Shatchkute, A. (2007).
Helsingborg Declaration 2006 on European Stroke
Strategies. Cerebrovascular Diseases, 23(2-3):229–
241.
Kolominsky-Rabas, P. L., Heuschmann, P., Marschall, D.,
Emmert, M., Baltzer, N., Neundoerfer, B., Sch
¨
offski,
O., and Krobot K.J. (2006). Lifetime Cost of Ischemic
Stroke in Germany: Results and National Projections
From a Population-Based Stroke Registry: The Erlan-
gen Stroke Project. Stroke, 37(5):1179–1183.
Kotiadis, K. and Robinson, S. (2008). Conceptual mod-
elling: Knowledge acquisition and model abstraction.
In Proceedings of the 2008 Winter Simulation Confer-
ence, pages 951–958. Winter Simulation Conference
2008.
HybridSimulationApproachforProspectiveAssessmentofMobileStrokeUnits
365

Kuehn, A. and Grunwald, I. (2011). Das Konzept der Mo-
bilen Stroke Unit (MSU). Der Radiologe, 51(4):261–
262.
Pietzsch, J. B. and Pat
´
e-Cornell, M. E. (2008). Early tech-
nology assessment of new medical devices. Inter-
national Journal of Technology Assessment in Health
Care, 24(01):36–44.
Purrucker, J. and Veltkamp, R. (2011). Thrombolysis Be-
yond the 3-h Time Window. Aktuelle Neurologie,
38(09):494–504.
Robinson, S. (2011). Choosing the right model: Con-
ceptual modeling for simulation. In Proceedings of
the 2011 Winter Simulation Conference, pages 1428–
1440. Winter Simulation Conference 2011.
Walter, S., Kostpopoulos, P., Haass, A., Helwig, S., Keller,
I., Licina, T., Schlechtriemen, T., Roth, C., Pa-
panagiotou, P., Zimmer, A., Vierra, J., K
¨
orner, H.,
Schmidt, K., Romann, M.-S., Alexandrou, M., Yil-
maz, U., Grunwald, I., Kubulus, D., Lesmeister, M.,
Ziegeler, S., Pattar, A., Golinski, M., Liu, Y., Volk,
T., Bertsch, T., Reith, W., Fassbender, K., and Noor,
A. M. (2010). Bringing the Hospital to the Patient:
First Treatment of Stroke Patients at the Emergency
Site. PLoS ONE, 5(10):e13758.
XJ Technologies Company Ltd. (2012). AnyLogic -
www.xjtek.com.
SIMULTECH2012-2ndInternationalConferenceonSimulationandModelingMethodologies,Technologiesand
Applications
366
